-
7/29/2019 Electrolyte and Fluid Balance
1/25
ELECTROLYTEAND FLUIDBALANCEIons capable of carrying an electric
charge
Classified as cations and anions
-
7/29/2019 Electrolyte and Fluid Balance
2/25
-
7/29/2019 Electrolyte and Fluid Balance
3/25
WATER
Content varies 40-755 of the total body weight
Women have lower content than men
Water is the solvent for all processes in the human
body It transports nutrients to cells, determines cell
volume by its transport into and out of cells,
removes waste products by way of urine, and acts
as the bodys coolant by way of sweating
-
7/29/2019 Electrolyte and Fluid Balance
4/25
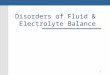
WATER
Intracellular fluid (ICF) is the fluid inside the cells
and accounts for about two thirds of total body
water.
Extracellular fluid (ECF) accounts for the other
one third of total body water and can be subdivided
into :
- intravascular extracellular fluid (plasma)
- interstitial cell fluid that surrounds the cells in the
tissue.
-
7/29/2019 Electrolyte and Fluid Balance
5/25
-
7/29/2019 Electrolyte and Fluid Balance
6/25
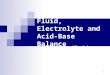
MAINTENANCEOF IONINTHEPLASMA
Active transport is a mechanism that requiresenergy to move ions
across cellular
membranes.
For example, maintaining a high intracellular concentration of
K
and a high extracellular (plasma) concentration of Na
requires
use of energy from ATP in ATPase-dependent ion pumps.
Diffusion is the passive movement of ions across a
membrane. It depends on the size and charge of
the ion being transported and on the nature of the
membrane through which it is passing. The rate ofdiffusion of
various ions also may be altered by
physiologic and hormonal processes.
-
7/29/2019 Electrolyte and Fluid Balance
7/25
-
7/29/2019 Electrolyte and Fluid Balance
8/25
CLINICAL SIGNIFICANCEOF OSMOLALITY
Osmolality in plasma is important because it is theparameter to
which the hypothalamus responds
Regulation of osmolality also affects the Na
concentration in plasma, largely because Na and its
associated anions account for approximately 90% of the
osmotic activity in plasma.
normal plasma osmolality (275 295 mOsm/kg of
plasma H2O)
-
7/29/2019 Electrolyte and Fluid Balance
9/25
CLINICAL SIGNIFICANCEOF OSMOLALITY
osmoreceptors in the hypothalamus respond quickly tosmall
changes in osmolality.
1%2% increase in osmolality causes a fourfold
increase in the circulating concentration of AVP
AVP acts by increasing the reabsorption of water in thecortical
and medullary collecting tubules.
AVP has a half lifein the circulation of only 15 to 20
minutes.
Renal water excretion is more important in controllingwater
excess, whereas thirst is more important in
preventing water deficit or dehydration.
-
7/29/2019 Electrolyte and Fluid Balance
10/25
-
7/29/2019 Electrolyte and Fluid Balance
11/25
REGULATIONOF BLOOD VOLUME
Changes in blood pressure are detected in this areas --
Cardiopulmonary circulation, carotid sinus, aortic arch,
andglomerular arterioles.
Adequate blood volume is essential to maintain bloodpressure and
ensure good perfusion to all tissue and organs.
Regulation of both Na and water are interrelated in
controllingblood volume.
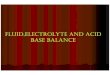
The renin-angiotensinaldosterone system responds primarilyto a
decreased blood volume.
Renin is secreted near the renal glomeruli in response
todecreased renal blood flow (decreased blood volume or
bloodpressure).
Renin converts angiotensinogen to angiotensin I, which
thenbecomes angiotensin II.
Angiotensin II causes vasoconstriction, which quicklyincreases
blood pressure, and secretion of aldosterone, whichincreases
retention of Na and the water that accompanies theNa.
-
7/29/2019 Electrolyte and Fluid Balance
12/25
-
7/29/2019 Electrolyte and Fluid Balance
13/25
FOUROTHERFACTORSAFFECTBLOODVOLUME:
(1) atrial natriuretic peptide (ANP), released from
themyocardial atria in response to volume expansion,promotes Na
excretion in the kidney (B-type natriureticpeptide [BNP] and ANP
act together in regulating bloodpressure and fluid balance)
(2) volume receptors independent of osmolality stimulate
the release of AVP, which conserves water by
renalreabsorption;
(3) glomerular filtration rate (GFR) increases with
volumeexpansion and decreases with volume depletion; and
(4) all other things equal, an increased plasma Na will
increase urinary Na excretion and vice versa. Thenormal
reabsorption of 98% to 99% of filtered Na by thetubules conserves
nearly all of the 150 L of glomerularfiltrate produced daily.
-
7/29/2019 Electrolyte and Fluid Balance
14/25
URINEOSMOLALITY
decreased in diabetes insipidus (inadequate AVP)
and polydipsia (excessive H2O intake) and
increased in conditions such as the syndrome of
inappropriate ADH (AVP) secretion (SIADH) and
hypovolemia (although urinary Na is usually
decreased).
-
7/29/2019 Electrolyte and Fluid Balance
15/25
DETERMINATIONOF OSMOLALITY
Specimen: serum or urine
Methods: determining osmolality are based on
properties of a solution that are related to the
number of molecules of solute per kilogram of
solvent.- An increase in osmolality decreases the freezing
point temperature and the vapor pressure.
Measurement of freezing point depression and
vapor pressure decrease (actually, the dew point)are the two
most frequently used methods of
analysis.
-
7/29/2019 Electrolyte and Fluid Balance
16/25
DETERMINATIONOF OSMOLALITY
Osmometers :- that operate by freezing point depression are
standardized using sodium chloride reference solutions.
- After calibration, the appropriate amount of sample ispipetted
into the required cuvet or sample cup and
placed in the analyzer.- The sample is then supercooled to 7C
and seeded to
initiate the freezing process. When temperatureequilibrium has
been reached, the freezing point ismeasured, with results for serum
and urine osmolalityreported as milliosmoles per kilogram.
- Calculation of osmolality has some usefulness either asan
estimate of the true osmolality or to determine theosmolal gap,
which is the difference between themeasuredosmolality and the
calculated osmolality.
-
7/29/2019 Electrolyte and Fluid Balance
17/25
OSMOLAL GAP
indirectly indicates the presence of osmotically
active substances other than Na, urea, or glucose,
such as ethanol, methanol, ethylene glycol, lactate,
orhydroxybutyrate
-
7/29/2019 Electrolyte and Fluid Balance
18/25
-
7/29/2019 Electrolyte and Fluid Balance
19/25
THE ELECTROLYTES
-
7/29/2019 Electrolyte and Fluid Balance
20/25
SODIUM
Na is the most abundant cation in the ECF,
representing
largely determines the osmolality of the plasma.
Na concentration in the ECF is much larger than
inside the cells.
Because a small amount of Na can diffuse through
the cell membrane, the two sides would eventually
reach equilibrium.
Active transport systems, such as ATPase ion
pumps, are present in all cells
The Na,K-ATPase ion pump moves three Na ions
out of the cell in exchange for two K ions moving
into the cell as ATP is converted to ADP.
-
7/29/2019 Electrolyte and Fluid Balance
21/25
SODIUM
The plasma Na concentration depends greatly on
the intake and excretion of water and, to asomewhat lesser
degree, the renal regulation of Na.
Three processes are of primary importance:
(1) the intake of water in response to thirst, as
stimulated or suppressed by plasma osmolality;
(2) the excretion of water, largely affected by AVP
release in response to changes in either blood
volume or osmolality;
(3) the blood volume status, which affects Na
excretion through aldosterone, angiotensin II, and
ANP (atrial natriuretic peptide).
-
7/29/2019 Electrolyte and Fluid Balance
22/25
CLINICAL APPLICATIONS
Hyponatremia
- a serum/plasma level less than 135 mmol/L.4
- most common electrolyte disorders in hospitalized
and nonhospitalized patients.
- Levels below 130 mmol/L are clinically significant.
- assessed by the cause for the decrease or with the
osmolality level.
- Decreased levels may be caused by increased Na
loss, increased water retention, or water imbalance
-
7/29/2019 Electrolyte and Fluid Balance
23/25
CLINICAL APPLICATIONS
Hyponatremia
- Increased Na loss in the urine can occurwith
decreasedaldosterone production, certain diuretics (thiazides),
withketonuria (Na lost with ketones), or a salt-losingnephropathy
(with some renal tubular disorders).
- K deficiency also causes Na loss because of theinverse
relationship of the two ions in the renal tubules.
When serum K levels are low, the tubules will conserveK and
excrete Na in exchange
- . Each disorder results in an increased urine Na level(20 mmol
per day), which exceeds the amount of waterloss.
- Prolonged vomiting or diarrhea or severe burns canresult in Na
loss.
- Urine Na levels are usually less than 20 mmol per day inthese
disorders, which can be used to differentiateamong causes for
urinary loss.
-
7/29/2019 Electrolyte and Fluid Balance
24/25
CLINICAL APPLICATIONS
Hyponatremia
- Water imbalance can occur as a result of excesswater
intake,which must be chronic
- In a normal individual, excess intake will not affect
Na levels. Syndrome of inappropriate AVP secretion
(SIADH) causes an increase in water retentionbecause of
increased AVP (ADH) production
-
7/29/2019 Electrolyte and Fluid Balance
25/25
CLINICAL APPLICATIONS