Embed Size (px)
Citation preview

Electrolyte Emergencies and Acute Renal Failure inPediatric Critical CareElizabeth Galloway, MD, Lesley Doughty, MD
176
Electrolyte emergencies and acute renal failure are common problems in pediatric criticalcare. With improved understanding of electrolyte disturbances and more pediatric specifictreatment available for acute renal failure, this field is constantly changing. The initialemergency management and ongoing care of these problems require special considerationand often individualized treatment. This article addresses the pathophysiology andtreatment of electrolyte emergencies and acute renal failure. Special circumstances seenin the pediatric critical care setting are reviewed in greater detail with disease-specifictreatment considerations. In addition, a review of renal replacement therapy and its use inacute renal failure is given. This article will provide a review of, and treatment strategy for,the variety of electrolyte emergencies and causes of acute renal failure facing the criticalcare patient.Clin Ped Emerg Med 8:176-189 C 2007 Published by Elsevier Inc.
KEYWORDS electrolyte emergencies, acute renal failure, pediatric critical care
A15-year-old male (50 kg) with developmental delaypresents with a new onset tonic-clonic seizure and
a 3-day history of decreased responsiveness. Initialphysical examination revealed an unresponsive, hypoxe-mic male requiring bag-mask ventilation. The patienthad cool extremities and a heart rate of 180, a meanarterial pressure of 50, and a capillary refill time longerthan 4 seconds. Early treatment consisted of endotra-cheal intubation, volume resuscitation, and a dopamineinfusion. The patient's initial laboratory results wereas follows:
Sodium (Na)
150 mmol/L Potassium (K) 5.8 mmol/L Chloride (Cl) 88 mg/dL Bicarbonate 15 mmol/L BUN 104 mg/dL Creatinine (Cr) 3.4 mg/dLDivision of Critical Care Medicine, Department of Pediatrics, Cincinnati
Glucose 1235 mg/dL Hemoglobin 14.3 g/dL Children's Hospital Medical Center, University of Cincinnati, iCalcium 0.84 mmol/L Corrected Na 170 mmol/L Cincinnati, OH.Reprint requests and correspondence: Lesley Doughty, MD, Division of
Serum osm 406 mosm/L Serum ketones NegativeCritical Care Medicine, Cincinnati Children's Hospital Medical
C1urine 97 mmol/L Naurine 6 mmol/LCenter, OH 45229. (E-mail: [email protected])
VBG: pH 7.08; pCO2 35; pO2 35; Base Excess -25.The patient's final diagnosis was hyperglycemic non-ketotic syndrome. The presentation was complicated byhypovolemic shock secondary to dehydration. Withaggressive resuscitation and careful hemodynamic support,his shock improved. Over the next 3 days, his hypergly-cemia, hypernatremia, and metabolic acidosis improved.
This case demonstrates the complexity of electrolytedisturbances and renal failure in critically ill children. Thelaboratory data above will be used to demonstrate formulasand calculations necessary for the treatment of electrolytedisturbances and renal failure.
1522-8401/$ - see front matter C 2007 Published by Elsevier Inc.
doi:10.1016/j.cpem.2007.08.012

177Electrolyte emergencies and acute renal failure
Electrolyte DisturbancesElectrolyte imbalances are common occurrences in pedia-tric critical illness. They can be the hallmark of a particulardisease, an early warning of problems to come, oriatrogenic. Whether iatrogenic or pathologic, electrolyteimbalances can be the key to diagnosis and often requiredisease-specific treatment. This section will reviewsodium, potassium, calcium, magnesium, and phosphatedisturbances and the common associated diseases, treat-ments, and special circumstances seen in the pediatriccritical care setting.
SodiumUnder normal conditions, sodium (Na) is tightly regulatedbetween 135 and 145 mEq/L. Levels are consideredcritically low when below 125 mEq/L and critically highwhen above 150 mEq/L. As seen in the following formula,Na is the primary regulator of extracellular fluid volumeand serum osmolality (Osm):
Serum Osm ðmOsm=kg H20Þ¼ð2�serum NaÞþðglucose=18Þþðblood urea nitrogen=2:8Þ
Example from case:ð2�150Þþð1235=18Þþð104=2:8Þ¼406ðmOsm=kg H20Þ
Na homeostasis is maintained primarily throughhormonal control from the central nervous system andkidneys. Centrally, antidiuretic hormone (ADH) issecreted by the hypothalamus in response to increasedplasma osmolality, hypovolemia, and/or hypotension.The result is retention of free water, lowering of plasmaosmolality, and preservation of intravascular volume. Nais also regulated by its excretion or reabsorption by thekidney under the influence of atrial natriuretic factorand aldosterone. These hormones are secreted inresponse to such stimuli as sympathetic activation,decreased cardiac output, or alteration of intravascularvolume [1]. Abnormalities in sodium homeostasis occurfrom a multitude of causes including inappropriate Naloss or reabsorption through the kidneys, excess orinadequate free water, excess osmolar substances, orneurohormonal dysregulation.
Hyponatremia
Hyponatremia is most significant when the symptomaticstate has been reached rapidly. Symptoms include nausea,vomiting, headache, lethargy, seizures, and coma. Symp-toms are not often seen until the serum Na is less than125 mEq/L. Treatment depends on the presence ofhemodynamic compromise, the severity of the hypona-tremia, rapidity of onset, and osmolality. Initial fluidreplacement in a hemodynamically unstable patient isalways done with isotonic fluid regardless of the serumNa. Once hemodynamic stability is achieved, thencorrection of the serum Na perturbation should begin.
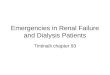
Acute severe hyponatremia (b48-hour duration, b125mEq/L) with neurologic symptoms (seizures, coma) is amedical emergency, and correction should be aimed atrapid but slight correction of serum Na. The goal is toraise the serum Na just enough to see improvement inneurologic symptoms such as cessation of seizures.Generally it is expected that 1 mL/kg of 3% normalsaline will raise the serum sodium by approximately1 mEq/L, and as such, treating initially with 2 to 3 mL/kgshould raise the serum Na sufficiently to stop seizureactivity. A repeat dose may be necessary with carefulmonitoring of serum Na to prevent overcorrection in thisrapid phase. Depending on the etiology of hyponatremia,therapy may be aimed at restriction of free water(excessive ADH secretion) or replenishment of totalbody Na (cerebral salt wasting [CSW]). Subsequentcorrection at a rate of 0.5 mEq/L per hour up to a levelof 135 mEq/L is recommended. If hyponatremia is achronic state, correction to normal Na can be detrimental.An even slower rate of correction (b0.5 mEq/L) isrecommended up to low-normal levels [2]. A rarecomplication of rapid correction is central pontinemyelinolysis. The proposed mechanism is a disruptionof the blood-brain barrier and an osmotic demyeliniza-tion. Central pontine and extrapontine myelinolysis hasbeen reported in children with symptoms ranging fromobtundation, seizures, coma, quadriplegia, and bulbardysfunction. Figure 1 depicts the causes of hyponatremiarelative to volume status and Na.
Hyponatremia Special Circumstances
Symptomatic hyponatremia can result from neurologicinjury. This phenomenon is seen in a variety of neurologic/neurosurgical situations including postoperative cranio-tomies, traumatic brain injury, intracranial hemorrhage,brain tumors, as well as many other forms of neurologicinjury. Commonly, it is thought that this results fromeither free water retention driven by excess ADH release(syndrome of inappropriate ADH [SIADH]) or from excessurinary NaCl loss (CSW) [2,3]. Controversy still remainsregarding these 2 conditions. Osmolar therapies forintracranial hypertension can complicate this diagnosis.The data listed in Table 1 provide a guide to differencesbetween the 2 entities.
The SIADH results in concentrated urine output (UOP)and free water retention. Several approaches are used totreat hyponatremia from this cause. One strategy focuseson restriction of the free water component of main-tenance. Reduce fluids by approximately 35% to allowunmatched insensible losses, which will result in a slowincrease in serum Na. For example, the use of 0.45%normal saline at a maintenance rate of 2/3 is a commonstrategy. Others advocate the use of normal saline at amaintenance fluid rate to minimize administration of freewater. The key issue is close monitoring of serum Na toavoid rapid correction.

Figure 1 Causes of hyponatremia. TBW, total body water; TBNa, total body Na; SIADH, syndrome of inappropriate ADH; DDAVP,
desmopressin; GI, gastroinstestinal.
178 E. Galloway, L. Doughty
Cerebral salt wasting is a poorly understood conditionresulting in excessive sodium loss in the urine. The highurine sodium content pulls free water with it, resulting in afree water deficit. Na losses, however, are in excess of freewater. Urine sodium levels can be higher than serum Na inthis condition. Careful volume and sodium correction withhypertonic fluids is necessary to maintain total bodysodium concentrations [2-5]. In this case, a carefullytitrated 3% normal saline infusion or enteral normal salinemay be necessary in addition to isotonic fluids to maintainserum Na in an acceptable range.
Iatrogenic hyponatremia is unfortunately common andlife-threatening. Hypotonic infusions particularly inpatients receiving enteral feeds may inhibit the inherentability of the body to control total body water (TBW).Special care should always be taken to limit intravenous(IV) fluids in patients receiving enteral feeds.
Hypernatremia
Thirst and ADH release are the primary defenses againsthypernatremia. When one or both of these defenses areinhibited, hypernatremia (Na N145) can result. Clinicalmanifestations of hypernatremia typically include symp-toms of dehydration as well as restlessness, progressing toirritability, stupor, and coma. Hypernatremia can presentwith or without intravascular volume derangementand with or without increases in total body sodium (seeFigure 2). If hypernatremia presents in the setting of severedehydration and hemodynamic instability, as always,isotonic fluid should be used to restore hemodynamic
Table 1 Syndrome of inappropriate ADH vs CSW.
SerumNa
UrineNa
UrineOutput
IntravascularVolume
UrineOsmolality
SIADH A z A Normal to z zCSW A zz zz Normal to A zz
adequacy. Once this is assured, then correction of theserum Na can begin. Treatment of hypernatremia isdirected at restoring TBW. Total body water and waterdeficit are calculated as follows:
TBW in children¼½0:6 L�weight ðkgÞ�Water deficit¼ð0:6�kgÞ
�½1�ðdesired sodium=serum sodiumÞ�Example from case: weight; 50 kg;
corrected serum Na; 170 mEq=L
ð0:6 L=kg�50 kgÞ�½1�ð145 mEq=L�170 mEq=LÞ�¼4:5 L
The total water deficit should be replaced over 48 to72 hours depending on the degree of dehydration. Goals oftreatment are to decrease Osm slowly. Serum Na shoulddecrease by less than 0.5 mEq/L per hour and not morethan 12 mEq/L per 24 hours [6]. This can usually beaccomplished using 0.45% normal saline at 125% ofmaintenance fluid rate [7]. The primary concern duringcorrection of hypernatremia is the development of cerebraledema. If hypernatremia has been evolving over manyhours, the intracellular and extracellular osmolar balance isreestablished by the creation of increased intracellularosmolar particles from such things as cleavage of aminoacids (often dubbed idiogenic osmoles). When serum Na iscorrected quickly, the extracellular osmolality decreasesfaster than that in the intracellular compartment, resultingin flux of free water into the cell and cerebral edema [7].
Hypernatremia Special Circumstances
Diabetic ketoacidosis and other metabolic conditions canhave profound effects on body water and sodium home-ostasis. In diabetes, elevated intravascular glucose inducesan osmotic diuresis. Prolonged polyuria can cause severefree water deficits as well as the loss of other electrolytes.

Figure 2 Causes of hypernatremia. TBW, total body water; TBNa, total body Na; SIADH, syndrome of inappropriate ADH; DDAVP,
desmopressin; GI, gastroinstestinal.
179Electrolyte emergencies and acute renal failure
On presentation, serum Na may be severely deranged.Serum Na must be evaluated in the context of the serumglucose at that time. Hyperglycemia can facticiously lowerserum Na, and in combination with Na losses frompolyuria, presenting Na can be low, normal, or high. Thefollowing formula is used to calculate the corrected serumNa [8]:
Measured Naþ½0:016�serum glucose ðmg=dLÞ�¼Corrected serum Na
Example from case: 150þð:016�1235Þ¼170
Hypernatremia in this setting is a reflection of thedegree of dehydration, and in combination with theserum glucose, leads to severe hyperosmolarity. In suchcases, slow correction of the total hyperosmolarity mustbe considered for the reasons listed above. One approachis to correct the glucose slowly, as is indicated in diabeticketoacidosis management with limited free water intro-duction, followed by slow correction of the free waterdeficit and serum Na. In this way, total Osm can belowered safely.Diabetes insipidus (DI) is another cause of hyperna-
tremia and must be identified because its treatmentrequires the more typical correction of hypernatremicdehydration. Central DI is a disturbance in Na and waterbalance as a result of ADH deficiency. It is commonly seenin the setting of congenital anomalies associated withmalformation of central brain structures, brain tumors, andsevere brain injury. Correction of hypernatremia in thissetting begins with achieving hemodynamic stability withisotonic fluids, followed by free water replacement. With-out ADH, UOP continues to be strikingly high, andmatching these losses can be extremely difficult. Hormonal
replacement with vasopressin in addition to fluid replace-ment is necessary.
Nephrogenic DI results from tubular resistance toendogenous vasopressin and requires careful Na restrictionand free water replacement [9]. The etiology of thissyndrome can be either genetic or acquired. The geneticform usually presents in infancy, and the acquired form canbe caused by numerous medications (eg, lithium, ampho-tericin, diuretics) and other systemic illness such as sicklecell disease, hypercalcemia, and significant potassiumdepletion [10]. Treatment of this problem mainly focuseson assuring adequate free water intake and NaCl restric-tion. Thiazide diuretics, amiloride, and indomethicin mayimprove concentrating ability and reduce polyuria [7].
Potassium (K)K levels in the body are carefully regulated by multiplemechanisms. Greater than 98% of total body K isintracellular; however, the most clinically relevant is theextracellular K. Extracellular K is kept within a narrowrange by the active and passive transport of K across thecell membrane. Active transport of K into the cell (againstthe concentration gradient) is accomplished via Na-K–adenosine triphosphatase pump. K can also enter the cellpassively via the Na-K-Cl channel along the sodiumgradient. K movement out of the cell follows theconcentration gradient through multiple K channels [11].Multiple factors can affect K transport and excretionincluding insulin, β-agonists, aldosterone, and acid basestatus. Disorders of K homeostasis are particularly criticalbecause of the potential clinical manifestations of relativelysmall changes in serum K. Organ systems primarilyaffected are cardiovascular, skeletal muscle, gastrointest-inal, and renal [12].

180 E. Galloway, L. Doughty
Hypokalemia
SerumK levels can be normal despite total body K depletionbecause of the large intracellular stores. This is particularlytrue in acid base disorders [1]. Symptoms from mild tomoderate hypokalemia (N2.5b3.5) are often vague, includ-ing fatigue, muscle weakness and constipation. Severehypokalemia (b2.5) can be associated with rhabdomyoly-sis, myoglobinuria, paralysis (ascending), and respiratoryarrest [13]. Changes in the electrocardiogram (ECG)tracing can occur initially with flattening of the T wavesextending to the development of U waves as a late finding.In cases of severe hypokalemia, sudden death, likelyassociated with prolonged QT, has been seen [14,15].Hypokalemia during digoxin therapy can lead to digoxintoxicity via multiple mechanisms [16]. Aggressive treat-ment of hypokalemia should be considered in particularclinical settings such as digoxin treatment, underlyingcardiac disease, acid base abnormalities, and overt hypo-kalemic symptoms [17]. Special care should be taken whentreating patients with redistribution hypokalemia (acidbase abnormalities) to avoid overcorrection [18]. EnteralKCl is the preferred route of replacement and, in children,can be dosed 1 to 2 mEq/kg per dose, repeating as necessaryfor slow correction. In life-threatening situations or whenenteral K is not possible and the serum K is critically low(b2.5 mEq/L), IV replacement 0.3 to 1 mEq/kg (adultmaximum 20-40 mEq per dose) over 1 hour can be safelygiven [7]. Patients receiving K replacement should be oncontinuous ECG monitoring. Of note, patients withhypomagnesemia can be refractory to K replacement andshould be given magnesium replacement in addition to K.
Hypokalemia Special Circumstances
Iatrogenic hypokalemia is extremely common. Patients atparticular risk are those on long-term diuretic therapy(chronic lung disease, heart disease [19]) and renal tubulardysfunction (as seen with amphoterocin use) [20].
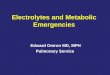
Figure 3 Treatment of
Redistribution hypokalemia is often seen during treatmentwith β-agonists (such as albuterol) and with severemetabolic acidosis [21]. For instance, in diabetic ketoaci-dosis, normal serum K levels do not represent total body K.During metabolic acidosis, K moves to the extracellularcompartment in exchange for protons moving intracellu-larly. As acidosis corrects and insulin therapy is begun, Kmoves back to the intracellular compartment effectivelylowering serum K.
Hyperkalemia
Hyperkalemia is defined as serum K greater than 5.5 mEq/L.The most severe consequences are cardiac, with malignantarrhythmias being the most deadly. Electrocardiographicchanges include peaked T waves, flattening of P waves,bundle-branch block, widening in the QRS, ventricularfibrillation, and asystole [22]. There are 3 arms in the usualtreatment of hyperkalemia: first, stabilize the myocardialmembrane; second, redistribute K intracellularly; and third,clearing K from the body. Treatment of hyperkalemiashould be dictated by patient symptoms and findings.Treatment order and components are described in Figure 3.
Hyperkalemia Special Circumstances
A variety of medications can cause hyperkalemiaespecially in the setting of preexisting renal impairment.Some of these medications are nonsteroidal anti-inflam-matory drugs (NSAIDs), angiotensin-converting enzyme(ACE) inhibitors, K sparing diuretics, pentamidine,cyclosporin, tacrolimus, β-blockers, digoxin, heparin,succinylcholine, and many nutritional/herbal supple-ments. Medication induced hyperkalemia can result frommultiple mechanisms: changes in renal blood flow,abnormal aldosterone synthesis and control, changes inNa and K channels, and decreased Na-K–adenosinetriphosphatase activity [23]. The special situationscreated by transplantation and critical illness necessitatethe use of many of these medications, often in
hyperkalemia.

181Electrolyte emergencies and acute renal failure
combination. Careful monitoring of K levels is para-mount to the safe care of these patients.Endogenous release of intracellular K from extensive
acute cell death can be seen in burns, trauma, heat stroke,rhabdomyolysis, tumor lysis syndrome (TLS), and massivehemolysis. Treatment approaches need to be 2-fold.Initially, it should be directed at lowering serum K andstabilization of any myocardial effects. Further planningfor continued K management needs to be institutedpromptly because continued K release may persist.
Calcium (Ca), Phosphorous (P), andMagnesium (Mg)Ca, Mg, and phosphorous homeostasis are dependentupon multiple factors: bone health, hormonal interac-tions, renal excretion/reabsorption, and intestinal absorp-tion. Ca and P are stored primarily in the bone. Releaseand absorption are controlled by parathyroid hormone(PTH), calcitonin, and vitamin D. Increased PTHstimulates the kidney, bone, and intestine to increasecirculating Ca and P. Mg is absorbed through thegastrointestinal tract; it is found in almost all foodsources. Mg absorption is also hormonally controlled,similar to Ca and P. Ca, phosphate, and Mg are involvedin all body systems as part of enzymes, energy produc-tion, and cell signaling. Deficiencies and excesses oftenpresent with vague symptoms but are vital to correct.
Hypocalcemia
Signs and symptoms of hypocalcemia (ionized Ca b0.8mmol/L) include anxiety, numbness, paresthesias, weak-ness, muscle cramps (tetany), laryngeal spasm, seizures,and arrhythmias (primarily prolonged QT). Symptomatichypocalcemia is a reflection of alteration in the ionizedCa fraction. As such, acid base disturbances and proteinbinding can alter Ca homeostasis. Causes of total Cadeficiency include vitamin D deficiency/impaired meta-bolism, reduced PTH production or end organ sensitivity,and impaired renal function [24]. Treatment of hypo-calcemia should be directed at the cause. Replacement ofCa alone is often not adequate especially in the setting ofvitamin D deficiency or hypoparathyroidism. In thesetting of life-threatening hypocalcemia (severe symp-toms or ionized Ca b0.7 mmol/L), IV replacement withCa (CaCl2 10–20 mg/kg up to 1 g IV or Ca gluconate 50-100 mg/kg IV over 5-10 minutes) is indicated and mustbe administered through verified and stable IV access.Special considerations should be taken in patients ondigoxin because rapid infusion of Ca can increase digoxintoxicity. Hypomagnesemia can cause refractory hypocal-cemia because of diminished secretion and action ofPTH [1].
Hypercalcemia
Hypercalcemia (Ca N12 mg/dL) is often asymptomatic;however, when severe, fatigue, weakness, hypotonia,
hypertension, vomiting, abdominal pain, constipation,and cognitive dysfunction can occur. Most cases ofhypercalcemia are caused from malignancy or hyperpar-athyroidism, and in rare cases, genetic diseases can be thecause. Treatment of hypercalcemia is directed at hydration,and increasing renal excretion with loop diuretics is ofteneffective [1]. Thiazide diuretics should be avoided. Inpatients with persistent, critically elevated Ca, hemodia-lysis (HD) can be considered.
Hypophosphatemia
P has many roles in metabolism as an integral part ofcellular signaling, adenosine triphosphate, and nucleicacids. In critically ill children, low phosphate can occurfrom many common situations such as diuretic therapy,malnutrition, and inadequate intestinal absorption. Mostcommon symptoms are fatigue and irritability. In severecases, acute respiratory insufficiency, arrhythmia, weak-ness, and altered mental status can occur [25]. Treatmentof hypophosphatemia should be focused on the cause. Incritical situations, IV replacement with K phosphate or Naphosphate over 6 hours has been described. For serumphosphate less than 0.5 mg/dL, phosphate can be dosedat 0.15 to 0.33 mmol/kg of phosphate and, for serumlevels 0.5 to 1 mg/dL, a dose of 0.05 to 0.25 mmol/kg over6 hours [10,26]. For mild asymptomatic hypophosphate-mia, supplemental phosphate can be administered orallyor in maintenance IV fluids. Enteral replacement iseffective; however, diarrhea/poor absorption may precludethis route.
Hyperphosphatemia
Hyperphosphatemia is most often caused from decreasedexcretion in the setting of renal failure. In the critical caresetting, chronic respiratory acidosis can lead to hyperpho-sphatemia, likely because of redistribution. Hypocalcemiacommonly occurs in conjunction with hyperphosphate-mia, often accounting for symptoms such as cardiacarrhythmias. Of note, many cases of hyperphosphatemiahave been seen after the use of phosphate containingenemas in infants and children. Treatment includeshydration; dietary restriction; enteral phosphate binders;and in critical situations, hemodialysis (HD).
Hypomagnesemia
Mg deficiency can present in many different ways, andmost commonly, symptoms are from associated Ca and Kdeficiencies, which can be caused by hypomagnesemia.Chronic diarrhea, chronic renal loss, and poor dietaryintake especially during chronic illness can lead tohypomagnesemia. In severe hypomagnesemia, neuromus-cular hyperexcitability and cardiac arrhythmias can occur.In chronic states of depletion, carbohydrate intolerance,hyperinsulinemia, hypertriglyceridemia, hypercholestero-lemia, and osteoporosis can be observed. Oral treatment ispreferred; however, when necessary, IV replacement (Mg

182 E. Galloway, L. Doughty
sulfate 25-50 mg/kg per dose [0.2-0.4 mEq/kg per dose];maximum single dose: 2000 mg [16 mEq]) can be given[27]. Of note, with refractory hypokalemia and hypocalce-mia, even despite a normal Mg level, giving Mg may helpcorrection of those electrolytes [28].
Hypermagnesemia
Excess Mg occurs from 2 etiologies, excess parental intakeand impaired renal excretion. Symptoms include initialhypotension, nausea, vomiting, flushing, urinary retention,and ileus. Severe hypermagnesemia can cause skeletalmuscle paralysis, hyporeflexia, bradycardia, respiratorydepression, coma, and cardiac arrest. Treatment includesdiscontinuation of Mg supplements. In the setting of renalfailure, dialysis is often the only option for clearance. Inemergencies, Ca can be given to temporarily relieve thesymptoms [11,29].
Ca, Phosphate, and Mg Special Circumstances
Tumor lysis syndrome is the combination of hyperurice-mia, hyperkalemia, and hyperphosphatemia. This is causedwhen a large amount of cytolysis occurs and cellularcontents are released into the blood stream [30]. Patientsmost at risk for this are those with rapidly growing tumorsthat outgrow their blood supply or at the initiation ofchemotherapy/radiation. Treatment is focused on prevent-ing renal failure and hyperkalemic arrhythmias. Treat-ments include urine alkalinization to keep uric acidsoluble, hydration, and administration of allopurinol orrasburicase. Hypocalcemia may also be seen primarilybecause of hyperphosphatemia. Treatment with Ca infu-sions can create Ca-P precipitation and should be avoidedin asymptomatic patients [10].
Refeeding syndrome occurs in children with malnutri-tion who abruptly restart enteral or IV nutrition. Pertinentclinical situations include any disease states with chronicmalnutrition. Of note, anorexia nervosa is a commondisease involving significant risk for refeeding syndrome.The primary electrolyte disturbances are hypophosphate-mia due to the rapid uptake of phosphate to supportanabolic metabolism, hypomagnesemia, and hypokalemia.This begins once high carbohydrate feeding is introduced.In addition to the electrolyte abnormalities, the body alsoretains extracellular water, adding stress and increasedworkload to the cardiac and pulmonary systems. The rapiddecrease in phosphate and increased body stresses can leadto life-threatening complications such as respiratory fail-ure, cardiac failure, arrhythmias, rhabdomyolysis, seizures,and coma.
As described above, there are many electrolyte abnorm-alities that warrant careful attention and specializedtreatment. Some situations, as described above, can occurdespite normal renal function; however, many such casesare seen in the setting of acute renal failure. The nextsection will review situations in which renal failure occursin critically ill pediatric patients.
Illustrative Case ContinuedAfter admission to the intensive care unit (ICU), thepatient was mechanically ventilated; dopamine andmilrinone were used for persistent shock; and insulintherapy and nutrition were begun. Klebsiella bacteremiawas noted on an initial blood culture. The patient wastreated with piperacillin/tazobactam, gentamicin, andvancomycin with discontinuation of the vancomycinafter the bacteria was identified. His hemodynamicsimproved and inotrope/vasopressor support was discon-tinued. Acute respiratory distress syndrome evolved, andcontinued ventilatory support was required. He becameoliguric and hypervolemic; diuretics were attempted;however, continuous venovenous hemofiltration (CVVH)was necessary for adequate fluid removal. Gradually, acuterespiratory distress syndrome resolved, and CVVH wastransitioned to intermittent HD. Ultimately, renal replace-ment therapy was no longer needed despite that renalfunction had not yet returned to normal. Renal functionindices upon discharge from the ICU were:
Blood urea nitrogen
38 mg/dL Naurine 110 mmol/L Crurine 2.5 mg/dL Naplasma 143 mmol/L Crurine 75 mg/dL 24-h UOP 1.23 mL/minThis patient had many risk factors for developing renalfailure such as hypovolemia, septic shock, and nephrotoxicdrugs. Initially prerenal insults were present, and whenshock was corrected, it was clear that intrinsic renal failurewas also present requiring renal replacement therapy. Inaddition, the use of nephrotoxic antibiotics may havecontributed to the intrinsic renal dysfunction. In the nextsection, these issues and many other renal failure issuesaffecting critically ill patients will be discussed.
Acute Renal FailureAcute renal failure is the loss of renal capacity for filtrationand tubular reabsorption. Renal failure becomes clinicallyapparent when UOP is reduced, leading to the retention ofnitrogenous wastes, electrolytes, and excess body fluid[10]. Acute renal failure in pediatric critical care iscommon; in one study, 4.5% of children admitted to thepediatric ICU had acute renal failure on presentation [31].The most common causes of pediatric acute renal failureare hypovolemic states, septic shock, cardiogenic shock,hemolytic uremic syndrome, hematological-oncologicalcomplications, postcardiac surgery, and burns [32].
Pathophysiology
Renal function is a product of filtration and reabsorption.Glomerular filtration rate (GFR) is a measure of renal

183Electrolyte emergencies and acute renal failure
function and represents the sum of the filtration rates ofthe functioning nephrons. As such, it provides a measureof filtration of plasma components into the renal tubules. Itdoes not account for reabsorptive function. The GFR canbe experimentally measured by giving an exogenoussubstance such as insulin that is freely filtered but notreabsorbed, secreted, or metabolized by the kidney and canbe quantified in the urine. More practically, GFR can beestimated by the clearance of creatinine (Cr). Creatinineclearance (CrCl) can be calculated from a 24-hour urinecollection (formula A) or estimated using a constant basedon sex and age (formula B):
Formula A:
Creatinine clearance ðmL=minÞ¼½Crurine� 24�hour urine output ðmL=minÞ�=Crplasma
Formula B:
Estimated CrCl ¼ k length ðcmÞ=Crplasma
k ¼ 0:45 for infants up to 1 year
k ¼ 0:55 for children > 1 year and adolescent girls
k ¼ 0:7 for adolescent boys
Example from case:
Formula A: CrCl¼ð75�1:23Þ=2:5¼37:5 mL=min
Formula B: CrCl¼ð0:7�150Þ=2:5¼42 mL=min
CrCl values below 50 mL/min require dose adjustmentof medications cleared by the kidney, and values below25 mL/min are consistent with renal failure [33].The GFR is maintained via 3 complex systems; first,
neural and hormonal messages sent to the kidney, whichinclude the renin-angiotension system, efferent sympa-thetic nervous system, vasopressin, and natriuretic pep-tides. Second, paracrine mechanisms including localintrarenal renin-angiotensin system, nitric oxide, endothe-lin, and eicosaniods are potent regulators of GFR. Lastly,blood pressure directly affects GFR through autoregulationachieved by changes in renal vascular resistance mediatedby the myogenic reflex and the tubuloglomerular feedback[34]. Myogenic reflex is the fast and pressure-sensitivereflex, and the tubuloglomerular feedback is the slowerNaCl concentration–dependent feedback loop. Changes inNaCl concentration are sensed by the macula densa of thejuxtaglomerular apparatus, which signals a change in theafferent arteriolar resistance [35,36].Renal failure ensues when these regulatory mechanisms
are unable to compensate for extreme hemodynamicconditions, toxins, and disease states. Renal failure iscommonly separated into prerenal azotemia, intrinsic renal
failure, and postrenal obstruction, as demonstrated inTable 2 [7,37].
Despite the use of many severity scores, kidney injuryhas been difficult to consistently classify. Recently, aninternational consensus classification has been developed,termed the RIFLE criteria. RIFLE criteria defines 5 gradesof severity: risk (R) injury (I), failure (F), loss (L), and end-stage renal disease (E) [38]. These criteria were developedfor adults but have been modified for pediatrics (pRIFLE).The pRIFLE criteria are depicted in Table 3. These criteriaare tools for the examination of epidemiology and potentialtherapies for acute kidney injury [39].
Prerenal FailurePrerenal failure is caused from intravascular volumedepletion, decreased cardiac output, renal vasoconstric-tion, and pharmacologic agents that impair intrarenalautoregulation. In prerenal failure, the integrity of the renalparenchyma and GFR will return to normal uponrestoration of renal blood flow. If renal blood flow is notrestored, acute tubular necrosis (ATN) can evolve. Manymechanisms work to restore adequate renal perfusion.Baroreceptors activate the sympathetic nervous system, therenin-angiotensin-aldosterone system, and release of ADH.This stimulates restoration of renal perfusion pressure byvasoconstriction and increases intravascular volume viaretention of salt and water. Intrarenal myogenic reflexessense a decrease in transmural pressure during hypoten-sive states and dilate the afferent arterioles improving renalblood flow. Synthesis of prostaglandin I2 is increased toenhance vasodilation [40]. Despite this complex system ofrenal autoregulation, many other substances/conditionscounteract these mechanisms. Exaggerated renal vasocon-striction can also occur in the setting of liver failure,cardiac failure, and septic shock.
Prerenal failure can be distinguished from intrinsic renalfailure in the acute setting by calculation of the fractionalexcretion of sodium (FENa):
FENa¼ðurine Na = plasma NaÞ= ðurine Cr = plasma CrÞ�100
Example from case:
@ Admission: FENa¼ð6=170Þ = ð105=3:4Þ�100¼0:1%
@ Discharge: FENa¼ð110 = 143Þ = ð75 = 2:5Þ�100
¼2:5%
Values below 0.1% suggest prerenal failure, and valuesabove 0.1% indicate intrinsic disease. It is important to note,however, that many conditions and medications can effectthe excretion of Na and render this tool ineffective.
Management of prerenal failure should be directed at thecause. Prerenal failure, when caused by hypovolemia,

Table 2 Causes of renal failure.
Prerenal Failure Intrinsic Renal Failure Postrenal Obstruction
Hypovolemia Glomerulonephritis Obstructive uropathyDehydration Postinfectious/poststreptococcal Posterior urethral valvesHemorrhage Lupus erythematosus Ureteropelvic junctionDiabetes insipidus Wegener’s granulomatosis Ureterovesicular junctionDiabetes mellitus Henoch-Schonlein purpura UreteroceleBurns Membranoproliferative TumorRelative hypovolemia Antiglomerular basement membrane Blood clotsSeptic shock Intravascular coagulation Obstructed bladder catheterHypoproteinemia Hemolytic-uremic syndrome StrictureAnaphylaxis Renal vein thrombosis Trauma/surgeryHypoperfusion DIC UrolithiasisCardiac failure Acute tubular necrosis Neurogenic bladderTamponade Shock Vesicoureteral reflux
Drugs and toxinsRadiocontrast agentsOrganic solventsHeavy metalsAntibioticsAminoglycosides, amphotericinChemotherapyNSAIDsACE inhibitorsEndogenous toxinsMyoglobinHemoglobinUric acid
Cortical necrosisAcute interstitial nephritisTumor infiltrationInfectionHypertensionCongenital renal diseases
ACE, angiotensin converting enzyme; DIC, disseminated intravascular coagulation; NSAIDs, nonsteroidal anti-inflammatory agents.
184 E. Galloway, L. Doughty
responds to isotonic fluid resuscitation. Special care shouldbe taken during volume resuscitation in the setting ofimpaired renal function because electrolyte disorders andvolume overload can occur. When poor cardiac output isthe cause of prerenal failure, excess fluid administrationcan further destabilize the disease process. Treatment ofthe underlying cardiac disease with diuretics, inotropicagents, and mechanical aids such as ventricular assistdevices can be beneficial [11]. Medications such asNSAIDs, ACE inhibitors, and angiotensin II receptor
Table 3 Pediatric RIFLE criteria.
pRIFLE Criteria eCCL UOP
Early R (risk) A25% b0.5 mL/kg/h � 8 hI (injury) A50% b0.5 mL/kg/h � 12 hF (failure) A75% b0.5 mL/kg/h � 24 h
or anuriaLate L (loss) Renal failure N4 wk
E (end stage) Renal failure N3 mo
eCCL, estimated creatinine clearance; UOP, urine output.
antagonists disrupt the autoregulatory mechanisms, caus-ing further decompensation of renal perfusion [41].
Prerenal Failure Special Circumstances
Abdominal compartment syndrome (ACS) can be a causeof prerenal failure in the critically ill. Intra-abdominalhypertension can be caused by anasarca, ascites, organo-megaly, or a combination thereof. When severe, it can leadto renal dysfunction, at which point the diagnosis of ACS ismade [42]. ACS decreases renal blood flow leading toprerenal failure. Treatment of ACS-induced renal dysfunc-tion should be directed at reducing intra-abdominalpressure via diuresis, paracentesis, and/or surgical inter-vention when appropriate. Some advocate providing ahigher mean arterial blood pressure to provide a betterperfusion pressure across the abdomen [43].
Intrinsic Renal FailureIntrinsic renal disease can be separated into large-vesseldisease, glomerular and microvascular disease, and dis-eases of the tubulointerstitium, including acute tubularnecrosis (ATN) from ischemia-/toxin-induced injury.

185Electrolyte emergencies and acute renal failure
Common causes in pediatric patients include ATN,hemolytic uremic syndrome (HUS), glomerulonephritis,and congenital anomalies [44]. ATN is associated with thehighest mortality [45,46].Large-vessel diseases include conditions such as auto-
immune vasculitis, thrombosis, and stenosis affecting therenal arteries and veins. These conditions are rare causes ofclinical renal failure except in the setting of underlyingchronic renal disease or a solitary kidney. Commonsettings include hypercoagulable syndromes such ashypertonic dehydration and antiphospholipid syndrome.Inflammatory changes in the arterial wall leading tothrombosis can occur in Takayasu's arteritis. In addition,stenosis at the anastomoses of the renal vessels can occurafter renal transplant [47].Microvascular and glomerular injury can be caused by
inflammatory (glomerulonephritides and vasculitis) andnoninflammatory (hypertension) vessel injury, thromboticmicroangiopathies, and hyperviscosity syndromes [11].Glomerulonephritides manifest clinically with hematuria,proteinuria, hypertension, edema, and azotemia. Hema-turia of glomerular origin presents with dysmorphic redblood cells (from osmotic and shear stress) and red bloodcell casts. Proteinuria (N2 g/d) and dark “coca cola”–colored urine is typical; however, urine sediment is ofteninconclusive, and renal biopsy is necessary to identify thespecific type of kidney disease. Common etiologies of acuteglomerulonephritis and vasculitis include poststreptococ-cal glomerulonephritis, membranoproliferative glomerulo-nephritis, rapidly progressive glomerulonephritis, minimalchange disease, systemic lupus erythematosus, Henoch-Schönlein purpura, polyarteritis nodosum, and IgAnephropathy [11]. Nephrotic syndrome is defined essen-tially as high-grade proteinuria (N3.5 g/d) withoutsignificant hematuria. It is also characterized by edema,hypoproteinemia, hyperlipidemia, and Na retention. Thissyndrome can be idiopathic or associated with many othersystemic illnesses [11].Tubulointerstitial diseases can be caused by inflamma-
tion of the renal interstitium and tubular injury. Causesinclude drugs, infection, and systemic illnesses such assystemic lupus erythematosis, leukemia/lymphoma, andcandidiasis. This category has been referred to as acutetubulointerstitial nephritis and can be precipitated bydrugs such as penicillins, amphotericin, and NSAIDs[10]. Depending on the tubular site of injury, differentfunctional abnormalities can occur. Proximal renaltubular acidosis is characterized by glucose, bicarbonate,phosphate, uric acid and amino acid wasting in the urine.Distal renal tubular acidosis is characterized by decreasedsecretion of K and hydrogen ions (H+) and decreasedreabsorption of Na. Medullary damage leads to impairedconcentration and decreased reabsorption of Na, such asthat seen in nephrogenic DI [10]. Acute tubulointerstitialnephritis can also be caused by severe infections, allograftrejection, and infiltrative disorders.
The term ATN is often used broadly to refer to allacute intrinsic kidney injury; however, there are manyother causes. ATN specifically refers to acute renal injuryin the absence of arterial or glomerular lesions [7]. Assuch, renal tubular cells are the primary site of injury inischemia or toxin-induced renal damage. Necrotictubular cells can detach and cause tubular obstructionleading to backleak of tubular contents and decreasedGFR [10]. ATN most commonly occurs in patients withsevere hypovolemic or septic shock and congestive heartfailure [44,48].
Toxin-induced ATN can come from endogenous orexogenous agents. Nephrotoxic agents cause injurythrough intrarenal vasoconstriction, direct tubular cellinjury, and tubular obstruction. Toxin-induced renal injuryis much more likely to occur during hypotension, sepsis, orchronic renal disease. The major categories of drugs thatcause renal injury are aminoglycosides, antivirals, organicsolvents, NSAIDs, immunosuppressives (cyclosporine),amphotericin, and radiocontrast. Endogenous agentssuch as myoglobin from rhabdomyolysis, hemoglobinduring hemolysis, and uric acid during TLS can alsocause ATN.
Intrinsic Renal Failure Special Circumstances
The incidence of renal failure in adults with septic shock is50% and is associated with a worse outcome. Whetherrenal failure causes a worse outcome or is simply anindication of the severity of illness is not clear. Multiplefactors contribute to renal failure in septic shock, includinghypoperfusion, vasoconstriction, inflammatory mediator-induced injury, disseminated intravascular coagulopathy,and drugs such as vasopressors and aminoglycosides.Treatment of renal failure in the setting of sepsis hasmarkedly changed with the improved modalities of renalreplacement therapy [49].
Contrast-induced ATN is most often seen in patientswith preexisting renal dysfunction, decreased intravascularvolume, low cardiac output, or when coadministered withother nephrotoxic agents. Most instances of contrast-induced nephropathy are mild with only a transient rise inserum Cr. One of the primary distinguishing features ofcontrast-induced nephropathy is the finding of low urinaryNa (b10 mEq/L). Another feature is the persistence of anephrogram 1 to 2 days after the contrast was administered[11]. Radiocontrast causes damage primarily to theproximal tubule. The exact mechanism of renal injury isstill elusive. Therapy to prevent contrast-induced nephro-pathy includes the judicious use of volume expansion. Useof diuretics to “flush” the kidney has shown no benefit and,in fact, may increase toxicity. Despite concern for renalinjury, contrast is often necessary in the care of criticallyill patients. The most important recommendations areto use the minimal amount of contrast necessary for theprocedure and to avoid concurrent intravascular volumedepletion [11].

186 E. Galloway, L. Doughty
Hemolytic uremic syndrome (HUS) consists of non-immune hemolytic anemia, low platelets, and renaldysfunction. The renal dysfunction is a combination ofthrombotic occlusion of capillary lumens, glomerularendothelial cell swelling, apoptosis of glomerular andtubular cells, and extensive cortical necrosis. Worldwide, itis the leading cause of renal failure in children [50]. Classicshiga-like toxin induced HUS from bacteria such asEscherichia coli O157:H7 usually presents with a bloodydiarrheal prodrome. Conversely, non–shiga-like toxin HUSis rarely associated with bloody diarrhea. Non–shiga-liketoxin HUS can be triggered by bacterial infections such asStreptococcus pneumoniae via the production of neurami-nidase, which promotes aggregation between erythrocytes,glomeruli, and platelets. Other causes include viralinfections, drugs, malignancies, transplantation, preg-nancy, or it can be familial. Prognosis is improving;however, renal failure occurs in 55% to 70% of shiga-liketoxin associated HUS. The prognosis of non–shiga-liketoxin–associated HUS is worse with a mortality rate of 25%[51]. Treatment of shiga-like toxin HUS is mainlysupportive. There is no clear benefit to antibiotics; infact, there are reports of worsening HUS after antibiotictreatment. Binding agents have been studied withoutbenefit. Treatment of non–shiga-like toxin HUS is con-troversial. Some have proposed treatment with eitherplasma infusions or plasma exchange until remission(resolution of thrombocytopenia) [51]. Other studies havenot shown benefit from this therapy.
Postobstructive Renal FailureObstruction to urinary output can occur at multiple levelsin the urinary tract. Luminal obstruction of the ureter canbe caused by renal calculi, thromboses, uric acid crystals,and fungal infections. Trauma to the ureter can induceswelling and obstruct the lumen. Congenital malforma-tions of the ureters and ureteropelvic junction account fora great deal of chronic renal disease in children [52]. In theurethra, congenital posterior urethral valves, phimosis,stricture, and iatrogenic urinary catheter obstruction andtrauma can also cause obstruction [53]. Regardless of thesite of obstruction, renal failure can ensue. Downstreamobstruction transmits increased pressure to the kidneycausing a fall in GFR. Management involves relief ofobstruction. If the obstruction is relieved early enough,resolution of renal injury is likely. However, in many cases,rapid relief of obstruction is impossible secondary to theneed for surgical intervention and/or delay in diagnosisleading to prolonged renal failure.
Chronic Renal DiseaseChronic renal disease is well beyond the scope of thisarticle; however, underlying chronic renal diseaseincreases the susceptibility to acute renal failure. Thehealthy kidney is able to compensate for a significantdegree of dysfunction before evidence of clinical failure. In
patients with chronic renal failure, a much smaller insult,be it toxin, hypoperfusion, or obstruction, can lead toclinical failure. Common settings in which subclinicalchronic renal disease can exist and be exacerbated by anacute process include patients with prolonged antibioticcourses, rheumatologic diseases, and the immunocompro-mised/transplant population. Patients with end-stage renaldisease need special attention during acute illness. Fluidmanagement, drug choices, and electrolyte correctionsrequire careful monitoring.
Renal Replacement TherapyAcute renal failure can be supported with renal replace-ment therapy. Criteria for beginning therapy includehyperkalemia greater than 7 mEq/L, volume overloadwith hypertension and pulmonary edema, severe acidosis,uremic encephalopathy, pericardial effusion, or bleeding.Additional indications include extreme electrolytederangements of Ca, P, and Na; severe azotemia (bloodurea nitrogen N150 mg/dL); toxidrome from a dialyzablesubstance; and to permit nutritional support/blood pro-duct administration in oliguric patients [54].
Renal replacement therapy can be performed in 2 majorforms; intermittent HD and continuous renal replacementtherapy (CRRT). Continuous renal replacement therapyencompasses peritoneal dialysis (PD), CVVH and manyothers. The trend over the past 10 years has been towardincreased use of CVVH instead of PD in critically illchildren [55] with the advent of improved technology.Early use of renal replacement therapy has become a trendin pediatric critical care for tighter fluid control and toprovide nutrition. Some propose that early high volumeCRRT may provide additional benefit from the removal ofseptic mediators [56]. Deciding when to start renalreplacement, what modality to use, and what dose ofdialysis is a difficult choice and is best made in conjunctionwith a pediatric nephrologist.
Peritoneal DialysisFor many years PD was the primary mode of CRRT forchildren. It continues to be an extremely practical mode ofCRRT primarily because anticoagulation and vascularaccess are unnecessary. Peritoneal dialysis is appropriatefor children and particularly useful in neonates in whichlarge bore catheters are impractical. It can be used inunstable patients; however, some hypotension can occurbecause of fluid flux into the peritoneum from the vascularspace [57]. Peritoneal dialysis use is limited in patientswho have sustained recent abdominal surgery, necrotizingentercolitis, or bowel perforation because of peritonealadhesions. Peritoneal dialysis solute clearance is slow, andin situations where significant or urgent clearance isnecessary, such as severe hyperkalemia or TLS, PD may notbe sufficient [37]. Peritoneal catheters can be placed in theoperating room or at the bedside percutaneously. Care

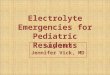
Figure 4 Schematic of ultrafiltration.
187Electrolyte emergencies and acute renal failure
should be taken to monitor for peritonitis. One of the mostcommon problems encountered is leakage around thecatheter site. Increasing the fill volume slowly will decreasethis risk. Once leakage has occurred, decreasing the fillvolumes, resuturing around a percutaneous catheter, andor placing fibrin glue into the catheter tunnel can help. Ofnote, neonates, because of their particular sensitivity toglucose, can be affected by the high concentration ofglucose in the dialysate fluid, leading to hyperglycemia.Although the use of PD is declining, there are still manysituations where it is the modality of choice for CRRT.
Continuous Venovenous HemofiltrationWhen considering extracorporeal CRRT, there are manyoptions: CVVH has mostly replaced continuous arteriove-nous hemofiltration because of the availability of pediatricsized venovenous catheters. In CVVH, the dialysis circuitrequires one large, stable, double-lumen central venouscatheter or, in neonates, 2 central access points. Once access
Figure 5 Schematic
is established, the goals of therapy must be determinedparticularly with regard to fluid and/or solute removal. Forultrafiltration (fluid removal), CVVH is excellent, but forrapid solute clearance, continuous venovenous HD may benecessary. CVVHDF provides both fluid removal andexcellent solute clearance [37]. Figures 4 and 5 are sche-matic representations of the concepts of ultrafiltration andHD. CVVH has become the therapy of choice because ofslow continuous fluid removal which is better tolerated inthe hemodynamically unstable patient. The primaryproblems with extracorporeal CRRT are access and antic-oagulation. To maintain filter patency, systemic (heparin)or local (citrate) anticoagulation is used. CVVH can also beconnected to an extracorporeal membrane oxygenationcircuit if dialysis/fluid removal is needed.
Intermittent HD
Although CRRT is increasing in use, HD continues to bethe mainstay of dialysis, as it is the most efficient way to
of dialysis.

188 E. Galloway, L. Doughty
clear solute and to remove fluid in the management ofchronic renal failure. Hemodynamic instability is usuallythe limiting factor in the use of HD because of the fluidshifts necessary to remove large amounts of fluid andsolute during a short treatment (2-3 hours). Hemodialysisis often very useful during recovery of renal function.Patients can transition from CVVH to HD, increasing theirfreedom of movement and decreasing the anticoagulantrisks. In patients with toxic metabolic conditions, such asinborn errors of metabolism and TLS, HD may providerapid one-time clearance; however, continued productionof toxins necessitates continuous removal. Removal ofexogenous dialyzable toxins such as after ingestions isoften best achieved by HD. For acute use, HD requiressimilar access to CVVH and anticoagulation althoughanticoagulation is only necessary during the treatment[58]. Fortunately, today, there are many options for renalreplacement therapy, making it possible to specificallytailor the therapy to the treatment requirements.
SummaryElectrolyte and renal function issues in critically illchildren are vast requiring many different approaches totreatment. Each disease state with its special considerationsand problems poses many challenges but fortunatelyimproved technologies have provided many treatmentoptions. Knowledge of the pathophysiology of renaldisease, its manifestations, and its treatment options isessential for optimizing care of the critically ill child.
References1. Weiss-Guillet EM, Takala J, Jakob SM. Diagnosis and management of
electrolyte emergencies. Best Pract Res Clin Endocrinol Metab 2003;17:623-51.
2. Adler SM, Verbalis JG. Disorders of body water homeostasis in criticalillness. Endocrinol Metab Clin North Am 2006;35:873-94.
3. Cole CD, Gottfried ON, Liu JK, et al. Hyponatremia in theneurosurgical patient: diagnosis and management. Neurosurg Focus2004;16:E9.
4. Jimenez R, Casado-Flores J, Nieto M, et al. Cerebral salt wastingsyndrome in children with acute central nervous system injury.Pediatr Neurol 2006;35:261-3.
5. Singh S, Bohn D, Carlotti AP, et al. Cerebral salt wasting:truths, fallacies, theories, and challenges. Crit Care Med 2002;30:2575-9.
6. Offenstadt G, Das V. Hyponatremia, hypernatremia: a physiologicalapproach. Minerva Anestesiol 2006;72:353-6.
7. Behrman R, Kliegman R. Jenson H, editors. Nelson textbook ofpediatrics. 16th ed.Philadelphia (Pa): W.B. Saunders Company; 2000.p. 196-222, 1758-68.
8. Rother KI, Schwenk WF. Effect of rehydration fluid with 75 mmol/Lof sodium on serum sodium concentration and serum osmolality inyoung patients with diabetic ketoacidosis. Mayo Clin Proc 1994;69:1149-53.
9. Kumar S, Berl T. Sodium. Lancet 1998;352:220-8.10. Fuhrman B, Zimmerman J, editors. Pediatric critical care. 2nd ed.
St. Louis (Mo): Mosby, Inc; 1998. p. 708-18, 741-66.11. Brenner B, Levine S, editors. Brenner and Rector's the kidney. 7th ed.
Philadelphia (Pa): W.B. Saunders Company; 2003.
12. Lin SH, Davids MR, Halperin ML. Hypokalaemia and paralysis. QJM2003;96:161-9.
13. Gennari FJ. Hypokalemia. N Engl J Med 1998;339:451-8.14. Cortesi C, Bettinelli A, Emma F, et al. Severe syncope and sudden
death in children with inborn salt-losing hypokalaemic tubulopathies.Nephrol Dial Transplant 2005;20:1981-3.
15. Zanolari-Calderari M, Vigier RO, Bettinelli A, et al. Electrocardio-graphic QT prolongation and sudden death in renal hypokalemicalkalosis. Nephron 2002;91:762-3.
16. McDonough AA, Wang J, Farley RA. Significance of sodium pumpisoforms in digitalis therapy. J Mole Cell Cardiol 1995;27:1001-9.
17. Cohn JN, Kowey PR,Whelton PK, et al. New guidelines for potassiumreplacement in clinical practice: a contemporary review by theNational Council on Potassium in Clinical Practice. Arch Intern Med2000;160:2429-36.
18. Schaefer M, Link J, Hannemann L, et al. Excessive hypokalemia andhyperkalemia following head injury. Intensive Care Med 1995;21:235-7.
19. Schaefer TJ, Wolford RW. Disorders of potassium. Emerg Med ClinNorth Am 2005;23:723-47.
20. Albengres E, Le Louet H, Tillement JP. Systemic antifungalagents. Drug interactions of clinical significance. Drug Saf 1998;18:83-97.
21. Rakhmanina NY, Kearns GL, Farrar HC. Hypokalemia in an asthmaticchild from abuse of albuterol metered dose inhaler. Pediatr EmergCare 1998;14:145-7.
22. Mattu A, Brady WJ, Robinson DA. Electrocardiographic manifesta-tions of hyperkalemia. Am J Emerg Med 2000;18:721-9.
23. Perazella MA. Drug-induced hyperkalemia: old culprits and newoffenders. Am J Med 2000;109:307-14.
24. Singh J, Moghal N, Pearce SH, et al. The investigation ofhypocalcaemia and rickets. Arch Dis Child 2003;88:403-7.
25. de Menezes FS, Leite HP, Fernandez J, et al. Hypophosphatemia incritically ill children. Rev Hosp Clin Fac Med Sao Paulo 2004;59:306-11.
26. Rogers M, Helfaer M, editors. Handbook of pediatric intensive care.3rd ed. Baltimore (Md): Williams and Wilkins; 1999. p. 719.
27. Abbott LG, Rude RK. Clinical manifestations of magnesiumdeficiency. Miner Electrolyte Metab 1993;19:314-22.
28. al-Ghamdi SM, Cameron EC, Sutton RA. Magnesium deficiency:pathophysiologic and clinical overview. Am J Kidney Dis 1994;24:737-52.
29. Baker SB, Worthley LI. The essentials of calcium, magnesium andphosphate metabolism: part II. Disorders. Crit Care Resusc 2002;4:307-15.
30. Haut C. Oncological emergencies in the pediatric intensive care unit.AACN Clin Issues 2005;16:232-45.
31. Bailey D, Phan V, Litalien C, et al. Risk factors of acute renal failure incritically ill children: a prospective descriptive epidemiological study.Pediatr Crit Care Med 2007;8:29-35.
32. Williams DM, Sreedhar SS, Mickell JJ, et al. Acute kidney failure: apediatric experience over 20 years. Arch Pediatr Adolesc Med 2002;156:893-900.
33. St. Peter WC. Pharmacologic approach in patients with renalfailure. In: Chernow B, editor. The pharmacologic approach to thecritically ill patient. Baltimore (Md): Williams and Wilkins; 1994.p. 41-79.
34. Cupples WA, Braam B. Assessment of renal autoregulation. Am JPhysiol Renal Physiol 2007;292:1105-23.
35. Koeppen B, Stanton B. Renal physiology. St. Louis (Mo): MosbyPhysiology Monograph Series; 2007. p. 39-42.
36. Just A. Mechanisms of renal blood flow autoregulation: dynamics andcontributions. Am J Physiol Regul Integr Comp Physiol 2007;292:R1-17.
37. Barletta GM, Bunchman TE. Acute renal failure in children andinfants. Curr Opin Crit Care 2004;10:499-504.

189Electrolyte emergencies and acute renal failure
38. Hoste EA, Clermont G, Kersten A, et al. RIFLE criteria for acutekidney injury are associated with hospital mortality in critically illpatients: a cohort analysis. Crit Care 2006;10:R73.
39. Akcan-Arikan A, Clermont G, Kersten A, et al. Modified RIFLEcriteria in critically ill children with acute kidney injury. Kidney Int2007;71:1028-35.
40. Yared A, Kon V, Ichikawa I. Mechanism of preservation of glomerularperfusion and filtration during acute extracellular fluid volumedepletion. Importance of intrarenal vasopressin-prostaglandin inter-action for protecting kidneys from constrictor action of vasopressin.J Clin Invest 1985;75:1477-87.
41. Taber SS, Mueller BA. Drug-associated renal dysfunction. Crit CareClin 2006;22:357-74.
42. Shibagaki Y, Tai C, Nayak A, et al. Intra-abdominal hypertension is anunder-appreciated cause of acute renal failure. Nephrol DialTransplant 2006;21:3567-70.
43. de Cleva R, Silva FP, Zilberstein B, et al. Acute renal failure dueto abdominal compartment syndrome: report on four cases andliterature review. Rev Hosp Clin Fac Med Sao Paulo 2001;56:123-30.
44. Filler G. Acute renal failure in children: aetiology and management.Paediatr Drugs 2001;3:783-92.
45. Otukesh H, Hoseni R, Hooman N, et al. Prognosis of acute renalfailure in children. Pediatr Nephrol 2006;21:1873-8.
46. Prakash J, Sen D, Kumar NS, et al. Acute renal failure due to intrinsicrenal diseases: review of 1122 cases. Ren Fail 2003;25:225-33.
47. Tsugawa K, Tanaka H, Kudo M, et al. Renal artery thrombosis in apediatric case of systemic lupus erythematosus without antipho-spholipid antibodies. Pediatr Nephrol 2005;20:1648-50.
48. Gill N, Nally JV, Fatica RA. Renal failure secondary to acute tubularnecrosis: epidemiology, diagnosis, and management. Chest 2005;128:2847-63.
49. Klenzak J, Himmelfarb J. Sepsis and the kidney. Crit Care Clin 2005;21:211-22.
50. Garg AX, Suri RS, Barrowman N, et al. Long-term renal prognosis ofdiarrhea-associated hemolytic uremic syndrome: a systematic review,meta-analysis, and meta-regression. JAMA 2003;290:1360-70.
51. Noris M, Remuzzi G. Hemolytic uremic syndrome. J Am Soc Nephrol2005;16:1035-50.
52. Warady BA, Chadha V. Chronic kidney disease in children: the globalperspective. Pediatr Nephrol (in press).
53. O'Brien WJ, Ryckman FC. Catheter-induced urinary bladderrupture presenting with pneumoperitoneum. J Pediatr Surg 1994;29:1397-8.
54. Levin DM, editor. Essentials of pediatric intensive care. St. Louis(Mo): Quality Medical Publishing Inc; 1990. p. 119.
55. Warady BA, Bunchman T. Dialysis therapy for children with acuterenal failure: survey results. Pediatr Nephrol 2000;15:11-3.
56. Fortenberry JD, Paden ML. Extracorporeal therapies in the treatmentof sepsis: experience and promise. Semin Pediatr Infect Dis 2006;17:72-9.
57. Flynn JT, Kershaw DB, Smoyer WE, et al. Peritoneal dialysis formanagement of pediatric acute renal failure. Perit Dial Int 2001;21:390-4.
58. Strazdins V, Watson AR, Harvey B. Renal replacement therapy foracute renal failure in children: European guidelines. Pediatr Nephrol2004;19:199-207.