Electromyography (EMG). Mark David S. Basco, PTRP Faculty Department of Physical Therapy College of Allied Medical Professions University of the Philippines Manila. Objectives. At the end of the session, you should be able to: Discuss the principles of EMG - PowerPoint PPT Presentation
Electromyography (EMG)
Electromyography (EMG)Mark David S. Basco, PTRPFacultyDepartment
of Physical TherapyCollege of Allied Medical ProfessionsUniversity
of the Philippines ManilaObjectivesAt the end of the session, you
should be able to:Discuss the principles of EMGDescribe the
characteristics of normal EMGDescribe the characteristics of
abnormal EMGDefinitionStudy of muscle function through the
examination of electrical signalsElectro electricMyo muscleGraphy
to graph / to measureWhy use EMG?In vivo examination of muscle
activityQuantifies muscle activitiesClinical vs. Kinesiological
History1791Luiggi Galvani, depolarized frog legs with metal
rods1838Carlo Matteucci, proved electrical currents originated in
mm1849Du Bois-Reymond, designed a galvanometer, reduced impedance
by popping blistersHistory
Principles
Involves detecting, amplifying, and displaying electrical
changes that occur during mm contraction
Electrical events are amplified electronically, visualized on a
tv-like monitor or even transformed into soundTV like monitor:
Oscilloscope6Principles
TV like monitor: Oscilloscope7How can we detect electrical
signals?ElectrodesTransducer; device converting one form of energy
to anotherDifferent typesSurface electrodesFine wire indwelling
electrodesNeedle electrodesElectrodesSurface ElectrodesApplied on
the surface of the skinMeasures signals from large muscles that lie
close to the skinOften silver/silver chloride, coated with a
suitable conducting gel, and can be taped on the skin
Refer to Sullivan for pictures10ElectrodesFine-wire Indwelling
ElectrodesTwo strands of 100micro-meter wires inserted into the
muscle bellyUsed for monitoring activity from deep mm, small mm, or
narrow mmMay not be useful for large mm ElectrodesNeedle
ElectrodesUsed to record motor unit potentials from different parts
of the muscleFine needles with electrodes inserted into the
muscleThe bare tip of the needle serves as the recording electrode
ElectrodesRecording / Detection ElectrodeEither surface, needle, or
fine-wireGround ElectrodeProvides a mechanism for cancelling out
the interference effect from external noiseSurface
electrodeAttached near the recording electrode
Electrodes
Electrodes
15Electrodes
16Myoelectric SignalVariables that may affect MUAPProximity of
electrodes to the fibers that are firingNumber and size of fibers
in the motor unitDistance between the fibersSize of the
electrodesDistance between the electrodes
MUAP Motor Unit Action Potential17Myoelectric SignalCross
talkElectrical overflowElectrical activity from nearby contracting
muscles reaches the electrodesControlled by:Careful electrode
placement, spacing, choice of size and type of electrode
MUAP Motor Unit Action Potential18Myoelectric
SignalArtifactsUnwanted electrical activityArises outside of the
tissues beinng examinedMay distort output signals
markedlySourcesMovementPower lineECG
MUAP Motor Unit Action Potential19Myoelectric SignalMovement
ArtifactSkinElectrodeContracting muscleElectrode cablesProduces
high voltage, high frequency artifactsControlled by:Firm fixation
of electrodes, firmly taping cables, skin preparation
Movement of skin, movement of electrode or pressure on
electrodes, and movement of electrodes within contracting muscles
usually produces artifacts below 20Hz causing minimal interference
can easily be controlled.20Myoelectric SignalPower line
InterferenceHuman body attracts electromagnetic energy from power
linesLoose electrode attachments, broken or frayed electrodes,
broken electrode wiresDiathermy, ES, cellphones, radios,
vibrators
21Myoelectric SignalECGcan occur if electrodes are placed on the
trunk, upper arm, or upper thighHow to reduce this artifact?Correct
application of ground electrodeUse of amplifier with appropriate
characteristics22AmplifierSignals (microvolts) recorded have to be
amplified about a thousand times for them to be displayed on an
oscilloscope and be heard through speakers or be recorded on a
chart
AmplifierThe electrical potential recorded by the electrodes is
composed of EMG signal from mm contraction and unwanted noise EMGs
use differential amplifiersGround electrode and active electrode
supply input to the amplifierDifference between the signals will be
amplified and recordedIf two electrodes receive equal signals, no
activity is recorded 24Amplifier
25Amplifier
26AmplifierCommon Mode Rejection RatioMeasure of how much the
desired signal is amplified relative to the unwanted signalThe
higher the value, the betterA good differential amplifier should
have a CMRR exceeding 100,000:1AmplifierSignal-to-noise
RatioReflects the ability of the amplifier to limit noise relative
to amplified signalRatio of wanted to unwanted signalNoise
generated fromInternal electrical componentsAmplifierGainRefers to
amplifiers ability to amplify signalsRatio of output signal to
input signal level
AmplifierInput ImpedanceResistive property observed in AC
circuitsReduced by:Larger electrodesSkin preparation
NORMAL EMG Insertional activityCaused by the needle breaking
through muscle fiber membranesAlso seen during needle
repositioningNormally stops when the needle stops moving.May be
described as NormalReducedProlongedReducedabsence; electrode not on
excitable tissue / fibrotic mm tissue
Prolonged- Hyperexcitable mm / during denervation / mm
inflammation32Electrical Silence(-) electrical activityIf needle is
at the NMJ/motor end plate, very small spontaneous potentials may
be observedAny other activity observed indicates pathology
Interference PatternNormally seen with strong muscular
contractionIndividual potentials are summated with increasing
number of motor units firing at higher frequencies
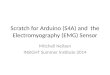
Abnormal EMGFibrillation PotentialsRepresents spontaneous,
repetitive depolarization of a single mm fiberNOT visibleMay result
fromDenervationMetabolic dysfunctionInflammatory diseases
(polio)TraumaIndicative of LMN lesions
Fibrillation Potentials
Positive sharp wavesRepresents asynchronous discharge of a
number of denervated mm fibersReflects an altered membrane
excitabilityUsually accompanied by fibrillation potentials
Fasciculation PotentialRepresent spontaneous discharges from a
group of mmOften visible; small mm twitchesSeen with irritation or
degeneration of ant horn cell, chronic pni, nerve root compression,
cramps or spasmsFasciculation PotentialMay be seen in NORMAL
individualsPathological significance if seen with fibrillation and
positive sharp waves
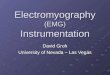
Myotonic / Complex Repetitive DischargeSeen with lesions of the
anterior horn cell and peripheral nerves, myopathiesDive-bomber
sound that occurs on needle insertion, voluntary
contractionProbably triggered by movement of needle electrode
within unstable mm fibers Myotonic / Complex Repetitive
Discharge
Nerve Conduction Velocity (NCV)Mark David S. Basco,
PTRPFacultyDepartment of Physical TherapyCollege of Allied Medical
ProfessionsUniversity of the Philippines ManilaObjectivesAt the end
of the session, you should be able to:Discuss the principles of
NCVDescribe motor NCV testingDescribe sensory NCV testing
PrinciplesInvolves direct stimulation to initiate an impulse in
motor or sensory nerves (evoked potential)The conduction time is
measured to determine the presence or absence of a lesionIt
provides data on the ability of the nerve to transmit impulses
Stimulating electrodeBipolar electrode with anode and
cathodePulse duration: 0.1 msecFrequency: 1HzContraindicated in
patients withIndwelling cardiac catheterCentral venous pressure
line
Contains a trigger mechanism that corresponds to a sweep on the
screenCathode stimulating electrode (black)Anode inactive electrode
(red)46Stimulating electrode
47Stimulating electrode
48MOTOR NCV testingStimulation and RecordingEvoked potential
recorded from a distal muscle innervated by the nerve under
studySmall surface electrodes are used to record the evoked
potential from musclesStimulation and Recording Recording
electrodePlaced over the belly of test muscleReference
electrodeOver the tendon of the mm; distal to the active
electrodeGround electrodePlaced over a neutral area between the
electrodes and the stimulation siteStimulation and Recording
Stimulation and Recording
Stimulation and Recording Stimulus starts low and is slowly
increasedIntensity is increased until the evoked response no longer
increases in sizeSupramaximal stimulusM-waveM-waveMAP (motor action
potential) CMAP (compund motor action potential) Represents the
summated activity of all motor units in the muscle that responded
to the stimulation54Stimulation and Recording Conduction
velocityDetermined by dividing the distance between the two points
by the difference between the two latenciesMeters/secondProximal
latencyDistal LatencyLatency time elapsed from the initial
propagation of nerve impulse to the depolarization of mm fibers
55Stimulation and Recording For example:Proximal latency:
7msecDistal latency: 2 msecConduction distance: 300 mm or 30 cmCV =
30 cm / (7msec 2 msec) = 30 cm / 5 msec = 60 m/s Latency time
elapsed from the initial propagation of nerve impulse to the
depolarization of mm fibers 56Stimulation and Recording How to
interpret?Upper Extremity: 50 70 m/s [60 m/s]Lower Extremity: 60
m/s57Sensory ncv testingStimulation and Recording Ring
electrodes
Stimulation and RecordingTechniquesOrthodromic
conductionAntidromic conductionStimulation and RecordingOrthodromic
conductionNormal way physiologic responses travel
Stimulation and RecordingAntidromic conductionStimulus applied
to proximal sites and is recorded at the index or long finger
Stimulation and RecordingHow to interpret?Normal sensory NCV40
75 m/sSensory NCVs have been found to be faster compared with the
motor NCVs Factors that may affect motor and sensory
conductionIncrease in body temperature5% increase in conduction
velocity per degreeReduced latenciesUE faster than LEProximal
segments faster than distal segmentsOTHERSH ReflexHoffman
ReflexMeasures the integrity of both motor and sensory fibersFor
exampleSubmaximal stimulus to the tibial n. in the popliteal
fossaMotor response recorded from the medial soleus (rich in mm
spindles) Norm: 29.8 msecF WaveElicited bySupramaximal stimulation
of a peripheral nerve in a distal site resulting in both
orthodromic and antidromic conduction.Antidromic conduction extends
to the spinal cordMost helpful in conditions where the most
proximal portion of the nerve is affectedUE: 30 secondsLE: less
than 60 seconds