Embed Size (px)
Citation preview

April 1950 -I. Modern Aspects of the Electrical Responses of Muscle 225
2 Electromyography as an Aidto DiagnosisBy A. T. RICHARDSON, M.B., B.S., D.PIYS.MED.Registrar, Depattment of Physical Medicine, St. Thomas's
Hospital
Electromyography is a diagnostic procedure bywhich the electrical activity (action potentials) ofvoluntary muscle can be studied either at rest orduring contraction. The alterations in these actionpotentials, which occur in association with lesionsof the lower motor neurones or of the musclefibres themselves, are readily detectable by themodern electromyograph. Its use is therefore avaluable adjunct in the clinical diagnosis of diseasesof the neuromuscular system.
Recent technical developments in the field ofelectronics have made available clinical electro-myographic equipment which is simple and yetaccurate (Fig. I). The apparatus consists of twotypes of detection electrodes (surface and needle),a high gain amplifier and a display unit. Thedisplay unit contains a meter measuring theaverage voltage of the detected muscle actionpotentials and a cathode ray tube to enable visualinterpretation or photography of them. Theouput from the amplifier is also applied to a loudspeaker to allow recognition of the potentials bysound. It is expedient to use apparatus incor-porating a nerve stimulator and allowing estima-tion of the duration of the muscle action potentials,conveniently, by comparison with a standardcalibration wave.
Electromyography with the use of surface (skin)electrodes allows estimation of the integratedelectrical activity derived from the ill-defined massof muscle underlying the electrodes. By placingthese electrodes in comparable positions on sus-pected and normal contralateral muscles andmeasuring the electrical activity on maximalvoluntary contraction, supramaximal nerve trunkstimulation and tendon jerk response, an index ofthe number of intact motor units in the suspectedmuscle can be obtained. Serial measurements ofmotor unit activity on nerve trunk stimulation maybe used to follow recovery in peripheral nerve in-juries (Hodes, et al., 1948). Similarly the pro-gressive decline in muscle electrical activity on re-peated stimulation of the nerve in myastheniagravis offers a quantitative measurement of theeffects of the disease and of any response totreatment (Fig. 2). Electrical activity accompany-ing spontaneous muscle action such as that oc-curring in motor neurone disease (fasciculation)and in motor nerve irritation by prolapsed inter-vertebral discs, etc., is detectable by surface elec-
trodes but is more accurately investigated by theuse of needle electrodes.Of more value in diagnosis is the detection,
localization and analysis of individual muscleelectrical potentials by means of needle electrodes.Of the several varieties of needle electrodes avail-able the coaxial or concentric hypodermic needleelectrode is very suitable for general use. Thisneedle with its limited detection range, allowslocalization of the potentials and consequentaccurate localization of any pathological lesions.When using needle electrodes in the analysis ofaction potential wave form characteristics, careshould be taken to move the needle into a positionwhich detects the potential changes maximally.This minimizes distortion of the wave by passagethrough the tissues before pick-up. Care shouldalso be taken to analyse only repetitive potentialsand thus avoid the analysis of complex wave formsproduced by fortuitous interference by two ormore simple potentials. Because the individualpotentials constituting the complex wave formsgenerally have different frequencies they soonpass out of phase and the interference complexwave form is not repeated (Fig. 3).The action potentials which may be detected in
muscle are conveniently divided into thoseoccurring on voluntary effort and those occurringspontaneously or on mechanical stimulation of themuscle, e.g. by movement of the needle electrodein the muscle.
·Tiii?
...iiii~iii~ ~~~iii!i~?.*...:... *:. ~...,,...j
.!ii....!**[0....
..~.:?·:,
.·l IE;~
FIG. i.-A modem double-channel electromyograph.(Photograph by permission of Stanley Cox Ltd.)
copyright. on 30 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.294.225 on 1 A
pril 1950. Dow
nloaded from

226 POSTGRADUATE MEDICAL JOURNAL April 1950
Ei ., L
l.ii'1"?·;: *;·r. 1L'
izr,a ," 1.;e ··r.,
U: ' i r...IP.I )rse · .-·1I.!'."P.""..tJp.-.b.': .'S. S 3 H
E II:!:P*:U.: 1::·· 1. 8:CI$.Y·::..:.: ; %5'*) r%;··.·r' HBP! c:6.?i4·f'':·! f'"':': :;BPSs.I: .
:i· ·f··g.r.Q?·.j ;·I·a-:.
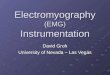
Fig. 2.-Muscle potential curves ob-tained on supramaximal stimula-tion of the nerve trunk in myas-thenia gravis at the start of con-traction and after I min. (stimula-tion rate, o per sec.).
Fig. 3.-Complex wave form (X)produced by simultaneous detec-tion of fibrillation potential (Y)and motor unit potential (Z).
Fig. 4.-The normal interferencepattern detected by needle elec-trode on maximal voluntary con-traction of a normal brachio-radialis muscle (milliseconds timescale).
Volitional Muscle Action Potentials(a) Normal Motor Unit Action Potentials
In normal muscle in full relaxation no electricalactivity is detectable electromyographically by astationary needle electrode. Insertion of theneedle electrode into normal muscle provokes anoutburst of motor unit potentials; these have beencalled, by Weddell, motor unit insertion potentials.On voluntary contraction repetitive normal motorunit action potentials occur at increasing fre-quencies up to an average maximum of 2o per sec.(Weddell, I944), and in increasing numbers withdeveloping tension. On full voluntary contractionthe many asynchronously contracting motor unitpotentials form the normal interference pattern.This is characterized by a low rumbling sound inthe loud speaker and a completely disturbed baseline on the cathode ray tube screen (Fig. 4). Theindividual motor unit potential has a duration inthe average limb muscle of 5 to io milliseconds,and an amplitude of Ioo microvolts to i millivolt(Weddell, I944). As detected by a coaxial needleelectrode the motor unit potentials are generallydiphasic or triphasic in form (Fig. 5a, b). Tri-phasic forms when detected at a distance appearmonophasic on account of failure to differentiatethe small first and third phases from the base lineat low amplitudes. The normal polyphasic motorunit action potentials (Fig. 5c) are detected in-frequently in limb muscles but more frequently inthe facial muscles. The formation of normal motorunit action potentials is apparently due to thepolarization changes accompanying the almostsynchronous contraction of the muscle fibres ofone motor unit (i.e. all the muscle fibres suppliedby one lower motor neurone).
Failure to obtain the normal interference patternon maximum volition almost always indicates amyelopathic (cord) or neuropathic (peripheralnerve and root) lesion. These are in contrast withmyopathic lesions which are confined to the musclefibres themselves in which, although the individualmotor unit action potentials may be reduced induration and there is an increased incidence ofpolyphasic potentials, an interference pattern isobtainable except in the late stages of the disease(Kugelburg, I949; Buchthal, I941). The de-tection of volitional motor unit action potentialsafter peripheral nerve injuries, indicating an in-complete nerve lesion, is of obvious importance indiagnosis and prognosis.
In neuropathic lesions the failure to obtain aninterference pattern may be due to disturbance ofnerve conduction (neuropraxia) or to degenerationof the nerve. Lower motor neurone degenerationgives rise to spontaneous muscle fibre activitywhich is detected electromyographically as' fibrillation action potentials' (vide infra).(b) ' Spike' and Complex Volitional Potentials
Regeneration of a lower motor neurone is oftendetectable electromyographically long beforeclinical signs of recovery are apparent. Inneuronal regeneration the muscle fibrillationpotentials indicative of denervation become re-duced in number, and highly polyphasic (complex)potentials may be detected on attempted voluntarycontraction (Weddell, I944) (Fig. 6). These com-plex volitional potentials are often of long durationand produce a characteristic rough sound in theloudspeaker by which they are readily dis-tinguished. As well as complex potentials, short
copyright. on 30 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.294.225 on 1 A
pril 1950. Dow
nloaded from

April 1950 Modern Aspects of the Electrical Responses of Mus,le 227
i.
Fig. 5.-Normal motor unit action potentials. (a) Diphasic. (b) Triphasic. (c) Polyphasic. (Milliseconds time scale.)
duration (i to 2 milliseconds) ' spike ' potentialsmay also be detected on attempted voluntarycontraction.
Spike and complex potentials detectable onvoluntary contraction during regeneration of nerveare due to the contraction of the recently re-innervated motor units. The complexities andtemporal dispersion are probably due to variationsin the conduction rate of the pre-terminal fibres ofthe recovering axon or variations in the trans-mission at the myoneural junctions (Weddell).
Loss of muscle fibre activity within a motorunit, such as may occur in myopathic lesions andon fatigue in myasthenia gravis, is responsible forthe higher incidence of polyphasic motor unitpotentials in these conditions (Fig. 7).Spontaneous Muscle Action Potentials(a) Fibrillation PotentialsThese small (amplitude less than o00 micro-
volts) potentials of I to 2 milliseconds durationmay be detected in muscle about three weeks afterdenervation (Fig. 8). They occur spontaneouslywhen they are heard as regular ' clicking' soundsat a frequency of 2 to 20 per sec., or in showerson insertion of the needle electrode into the de-nervated muscle (Weddell, I944). They are mostnumerous when the muscle is warmed, after theinjection of prostigmine and during active physio-therapeutic treatment (e.g. interrupted galvanism).They are detectable for long periods after denerva-tion and their detection, denoting as it does de-nervated muscle tissue with contractile elementsstill present, is a most valuable sign. Fibrillationpotentials are considered to be due to the spon-taneous contraction of individual muscle fibres.
(b) Spontaneous Motor Unit ActivityThe spontaneous muscle fasciculations of motor
neurone disease (amyotrophic lateral sclerosis andprogressive muscular atrophy) result in electricaldisturbances characteristic of motor unit twitches.The activity is apparently due to spontaneous im-pulses in abnormal motor units (Denny-Brown,I938), and there is evidence to indicate a peri-pheral origin for these impulses.
Irritation of nerve roots or nerve trunks bycervical ribs, etc., may give rise to spontaneousmotor unit activity. This finding is, however, in-constant even in the presence of marked neuro-logical signs. In the cervical region, particularly,it may be of value in localizing the point ofirritation.
(c) Trains of OscillationsTrains of high frequency potentials may be
obtained on insertion of the needle electrode intoaffected muscles in dystrophia myotonica, lesscommonly in motor neurone disease and rarely inother conditions. The duration of the potentialsis variable; in dystrophia myotonica some are ofthe duration of motor unit potentials; others aremuch shorter. These electrical discharges are re-markable for their change in pitch which causesthem to sound like a diving aeroplane, their fre-quency may be o00 to 150 per sec., dropping to20 per sec. (Buchthal, I941). In dystrophia myo-tonica they have been obtained after curare hasbeen given to block neuro-muscular transmission;their origin is unknown. In dystrophia myotonica,in addition to these trains of potentials, voluntarycontraction is followed by a fibrillary after-discharge. Spontaneous fibrillation which occurs
copyright. on 30 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.294.225 on 1 A
pril 1950. Dow
nloaded from

228 POSTGRADUATE MEDICAL JOURNAL April 1950
i I
.r ;;: ii. .. I'i'i r.·:
IPlrl."r.l"l+r.lpe.-r.llPIFig. 6.-Complex motor unit poten-
tial. Associated with reinnervation(facial palsy) (milliseconds time(scale).
b'ig. 7.-Motor units in myastheniagravis after fatigue (millisecondstime scale).
Fig. 8.-Fibrillation action poten-tials (milliseconds time scale).
in motor neurone disease, etc., is not detectable indystrophia myotonica.Synchronization of Motor Unit Activity
In normally innervated muscle the contractionof motor units is asynchronous, thus providing forthe smooth contraction of voluntary muscle. Thusif two needle electrodes of a double channelelectromyograph with differential amplifiers areinserted into two different motor units the timingof the motor unit potentials appears out of phase.In myelopathic lesions (notably acute anteriorpoliomyelitis) Buchthal and Clemmesen (I943) de-scribed synchronous activity of motor units de-tectable by three needle electrodes. This, theysuggested, was due to the spread of nervous im-pulses to contiguous neurones. An alternativeexplanation has been suggested by Denny-Brown('944), who has suggested that apparent syn-chronization is due to the detection by two or moreneedle electrodes of the same, often large, motorunit due to uncovering of this unit by loss of thesmall motor units. Whatever may be the ex-planation the occurrence of ' synchronization ' inmyelopathic lesions and its rarity in normalmuscles or in peripheral nerve lesions is un-doubted.To sum up, therefore, clinical electromyo-
graphy, although in its infancy, is of proven valuein peripheral nerve lesions in that it can provideevidence of nerve damage, recovery and retentionof any function before these phenomena can beestimated clinically. Although less is known aboutthe electromyographic appearance in otherdiseases, the detection and recognition of potentialsand their relative preponderance yields informa-tion unobtainable by other methods. It is usefully
combined with the use of intensity-duration curvesdescribed elsewhere in this issue.
I wish to thank Dr. P. Bauwens, physician incharge of the Department of Physical Medicine,St. Thomas's Hospital, for permission to publishthe pictures of muscle potentials illustrating thisarticle, which were taken from departmental re-cords. They were obtained by photographingcathode ray tube traces of the muscle potentialsafter recording on magnetic tape.
BIBLIOGRAPHY
BUCHTHAL, F., and CLEMMESEN, S. (I94I), Acta. Psychiat.Kbh., x6, I43.
BUCHTHAL, F., and CLEMMESEN, S. (I94I), Acta. Psychiat.Kbh., I6, 389.
BUCHTHAL, F., and CLEMMESEN, S. (1943), Acta. Psychiat.Kbh., I8, 377.
DENNY-BROWN, D., and PENNYBACKER, J. (1938), Brain,61, 311.
DENNY-BROWN, D. (I944), Arch. Neurol. and Psychiat., Chicago,61, 99.
HODES, R., LARRABEE, M. G., and GERMAN, W. (1948),Ibid., 60, 340.
KUGELBURG, E. (I949), J. Neurol. Neurosurg. Psychiat., 12, 129.WEDDELL, G., FEINSTEIN, B., and PATTLE, R. E. (I944),Brain, 67, 178.
3. Case Report. '
Facial Nerve PalsyBy B. 1. EAMES, M.B., CH.B., D.L.O.
Royal National Throat, Nose and Ear Hospital,Golden Square
A man, aged 6I, was first seen in May 1948,giving a history of discharge from both ears since1917, when he was torpedoed, with recent pain inthe right ear, unsteadiness and a right facial palsyin the lower half of the face which had been present
copyright. on 30 M
ay 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.294.225 on 1 A
pril 1950. Dow
nloaded from