Embed Size (px)
Citation preview

ElectrophysioloIll?
and Pharmacologyof utilide
Gerald V. Naccarelli, MD, Kai S. Lee, Phi), John K, Gibson, PhD,and James Vanderktgt, PhD
lbutilidefumarateisa newclassIll introven~santiar-rhythmicagentindicatedfor theacuteterminationofatrialfibrillationandflutter.Ibutilideprolongsmpalari-zationintheatriaandventriclebyenhancingtheinwarddepolarizing,slowsodiumcurrent,a uniquemechanismofact@nfora classIllagent.Atrialrefmctorinessispro-1T
withnoevidenceofreverseusedependence.lbu-tili may alsoblackthe,delayedrectifiercurrent,butthisdoesnotappeartobeclinicallyrelevant.Invitroand
‘at highdoses,ibutilidemayshortenactionpotentialdu-ration,althoughthiseffecthasnotbeennotedclinically.hutilidecancausetorsadesdepointesina rabbitmodelof proarrhythmiadependenton theformationof earlyokdepdarizations. However,it causeslessproar-rhythmiathansotalol,dofetilide,or,sematilidein thismodel.Thepharmacokineticsof ibutilideare linear,itse~scukm distributionismpidandextensive,whileitssystemicclearanceishigh(eliminationhalf-life3-6hours).Eightmetabolizesatefarmedby theliver,only
oneof whichisslightlyactive.QT prolongationisdosedependent,is maximalat theendof theinfusion,andreturnstobaselinewithin2-4 hoursfallowinginfusion.Thepharmacokineticand electrophysiologiccharacter.isticsof ibutilidearecomplementaryin thatany riskofproarrhythmiaismademanageablebya shorthaif-lik.Aimostall repmiedcasesof drug-inducedtarsadesdepaintesventricularluchycardiaassociatedwithibutilidehaveoccurredwithin40 minutesofstasiingtheinfusion.Neve~eless,cliniciansusingibutilidecanfwfherreducethechanceofWsadesdepointesbybeingveryfamiliarwiththecriieriafar patientselection,andby beingpre-paredto We@ it shouldit occur.When usedwithfullknowledgeof itspotentialrisks,ibutilideisa ve~ effec-tiveintravenousagentfortheacuteterminationofatrialfibrillationandMter and is likelyto becomea signifi-canttreatmentoptionforthesearrhythmias.
(AmJCardioi1996;78(suppl8A):12-16)
Ibutilide fumarate is a newly available intrave.nous agent useful in the termination of atrial fib-
rillation and flutter. Based on its ability to prolongrepolarization, ibutilide is a class III antiar-rhythmic agent.l This article will review the elec-trophy siologic and pharmacokinetic effects ofibutilide and correlate these effects with its mech-anism of action, its efficacy, and its proarrhythmicpotential.
#
BASIC ELECTROPHYSIOLOGYOFIBUTILIDE
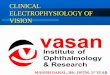
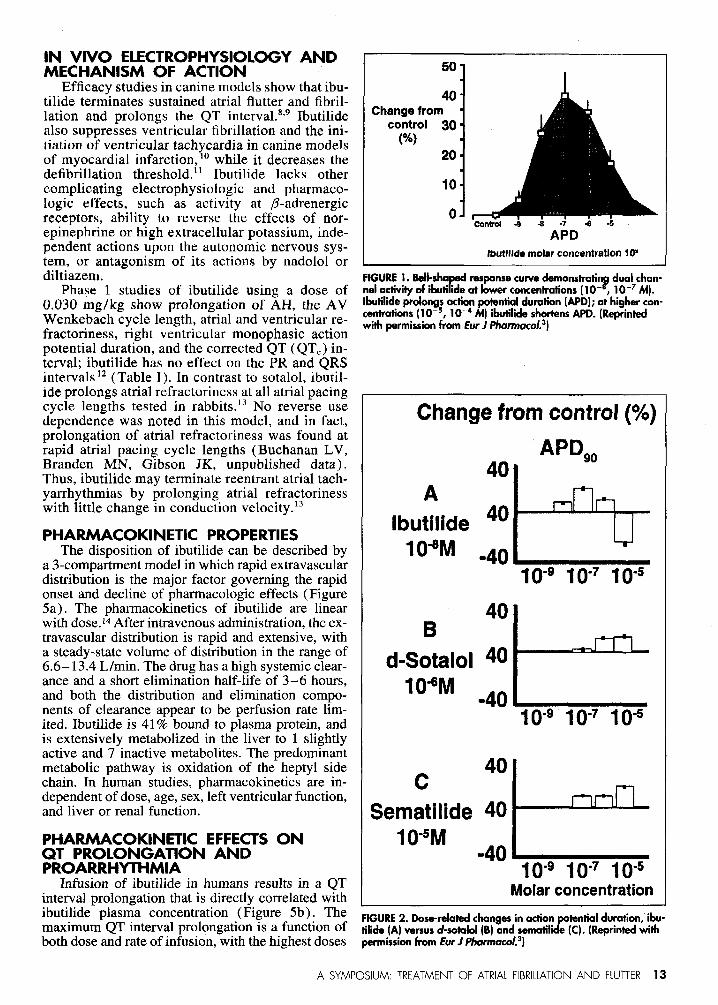
In vitro studies demonstrated that ibutilide in-creases the effective refractory period in rabbitventricular tissue in a dose-dependent manner2.Lee et a13demonstrated that ibutilide prolongs ac-tion potential duration in isolated guinea pig ven-tricular cells starting at concentration of 10-9 M.4This same study demonstrated a bell-shaped dose-response curve (Figure 1) with high concen-trations (10 ‘6– 10 M) of ibutilide actually short-ening the action potential duration. This bell-
From thePennState Cardiavoscular Center, PennState University Col-Iege of Medicine, Hershey, Pennsylvania (G.V.N.), and Pharmacia& Upjohn, Kalamazoo, Michi an (K.S,l., J.K.G, J.V.L).
YAddress for reprints: Gera d V. Naccarelli, MD, Penn State Car-diovascular Center, Penn State University College of Medicine, TheMilton S. Hershey Medical Center, PO. Box 850, Hershey, Penn-sylvania 17033.
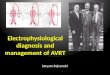
shaped response was different from dose-relatedincreases in action potential duration noted withsotalol and sematilide (Figure 2). Also, high dosesof ibutilide reversed the prolonged action potentialduration caused by drugs such as sematilide. Thisdual channel activity appears to be due to ibutilideincreasing the outward K + currents at high con-centrations, which was not seen with other classIII drugs tested.
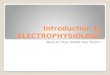
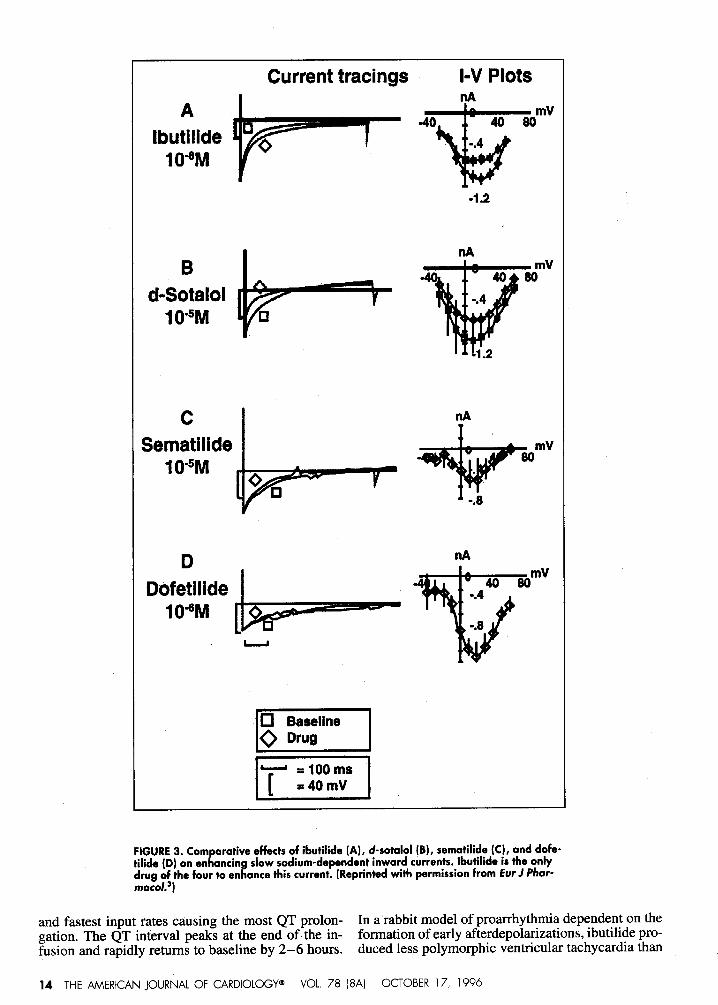
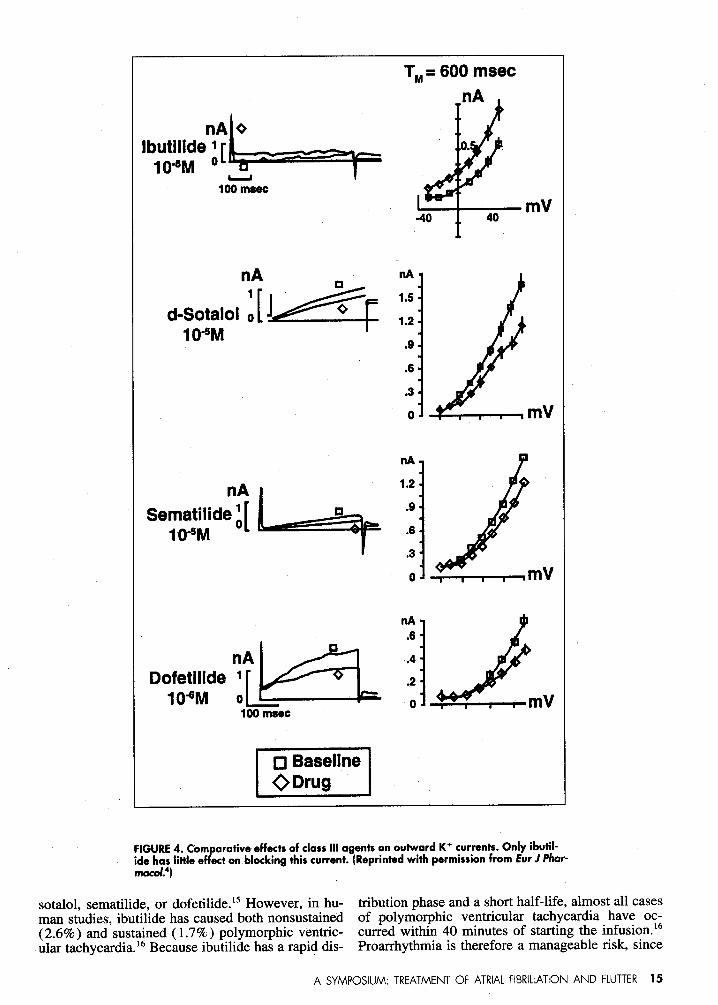
Considering the possible mechanisms bywhich a drug could prolong repolarization,5 ibu-tilide may act by blocking depolarizing K+ cur-rents as other class III agents do, by increasinginward Ca+2 current at plateau potentials, or byenhancing the slow inward depolarizing Na+ cur-rent in the plateau phase, Ibutilide’s predominantelectrophysiologic effect appears to be by the lat-ter action. Lee4 documented that ibutilide has thiseffect in guinea pig ventricular cells at pharma-cologic concentrations, wbile d-sotalol, sematil-ide, and dofetilide had no comparable effect (Fig-ure 3). Other studies by these same investigatorsdemonstrated that low doses of ibutilide ( <10-7M) had no effects on the 1~current (Figure 4) orL-type calcium plateau currents. At higher con-centrations, the effects of ibutilide became morecomplicated by affecting several outward K+ cur-rents. Furthermore, Yang et al’ showed that ibu-tilide blocks the delayed rectifier current (IK,) inAT-1 tumor cells.
12 01996 by Excerpta Medico, Inc.All rights reserved.
0002-9149/96/$ 15.00Pll S0002-9149(96)005607
IN VIVO ELECTROPHYSIOLOGYANDMECHANISM OF ACTION
Efficacy studies in canine models show that ibu-tilide terminates sustained atrial flutter and fibril-lation and prolongs the QT interval.8’9 Ibutilidealso suppresses ventricular fibrillation and the ini-tiation of ventricular tachycardia in canine modelsof myocardial infarction, 10while it decreases thedefibrillation threshold.ll Ibutilide lacks othercomplicating electrophysiologic and pharmaco-logic effects, such as activity at fl-adrenergicreceptors, ability to reverse the effects of nor-epinephrine or high extracellular potassium, inde-pendent actions upon the autonomic nervous sys-tem, or antagonism of its actions by nadolol ordiltiazem.
Phase 1 studies of ibutilide using ii dose of0.030 mg/kg show prolongation of AH, the AVWenkebach cycle length, atrial and ventricular re-fractoriness, right ventricular monophasic actionpotential duration, and the corrected QT (QTC) in-terval; ibutilide has no effect on the PR and QRSintervals 12(Table I). In contrast to SOtdOl, ibUtil-
ide prolongs atrial refractoriness at all atrial pacingcycle lengths tested in rabbits.13 No reverse usedependence was noted in this model, and in fact,prolongation of atrial refractoriness was found atrapid atrial pacing cycle lengths (Buchanan LV,13randen MN, Gibson JK, unpublished data).Thus, ibutilide may terminate reentrant atrial tach-yarrhythmias by prolonging atrial refractorinesswith little change in conduction velocity .13
PHARMACOKINETIC PROPERTIESThe disposition of ibutilide can be described by
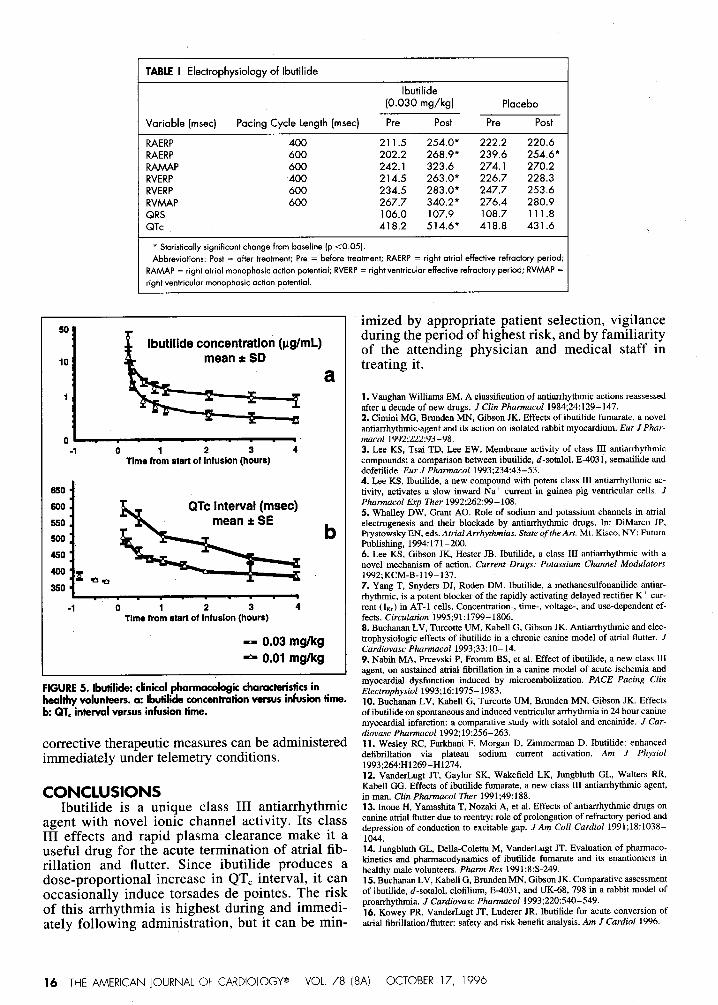
a 3-compartment model in which rapid extravasculardistribution is the major factor governing the rapidonset and decline of pharmacologic effects (Figure5a). The pharrnacokinetics of ibutilide are linearwith dose.14After intravenous administration, the ex-travascular distribution is rapid and extensive, witha steady-state volume of distribution in the range of6.6– 13.4 L/rein. The drug has a high systemic clear-ance and a short elimination half-life of 3–6 hours,and both the distribution and elimination compo-nents of clearance appear to be perfusion rate lim-ited. Ibutilide is 41$%bound to plasma protein, andis extensively metabolized in the liver to 1 slightlyactive and 7 inactive metabolizes. The predominantmetabolic pathway is oxidation of the heptyl sidechain. In human studies, pharmacokinetics are in-dependent of dose, age, sex, left ventricular function,and liver or renal function.
PHARMACOKINETIC EFFECTSONQT PROLONGATION ANDPROARRHYTHMIA
Infusion of ibutilide in humans results in a QTinterval prolongation that is directly correlated withibutilide plasma concentration (Figure 5b). Themaximum QT interval prolongation is a function ofboth dose and rate of infusion, with the highest doses
50“
40-Changefrom
control 30.(%)
20“
10“
o-COntrOl -S -8 -7 4 -6
APDIbutlllde molarconcentration1OX
FtGURE1.Bd-5hIaP
response curve demonstitindualchan-I?nelactivityof ibutiideatlowerconcentrations(10- , 10-7M).
lbutilideprolongsactionpokmtialduration(APD);athighercon-cenlratians(10-5,10-4M) ibutdideshortensAPD.(ReprintedwithpermissionhamEurJP/rmnxrco/.3)
Changefromcontrol(%)
APD9040
Ibu;ide 40104M .40 b
10-9 10-710-5
40B
d-Sotalol 40
’04M -40 b10-910-710-5
c40
Sematilide4010-5M
-40 e10-910-7 10-5
Molarconcentration
FIGURE2. Dose-relatedchangesinactionrknfia’dum’On’~b”-tilide(A)versusd-satahd(B)andsemahhe (C).(Reprintedwith
permissionhornEurJPharmaco/.3)
A SYMPOSIUM: TREATMENT OF ATRIAL FIBRIL4TION AND FIUTTER 13
AIbutilide
104M
l-vPlotsnA
Currenttracings
[
~%
mV-40 4080
0 -.4
-1.2
c I nAT
10-5M~~*”mvSematiiide
,~:d:otts ,
FIGURE3. Cornarativeeffectsof ibutilide(A), d-sotalol(B),semcrtilide(C),anddofe.tili&(D]onen~ntin~ slowsodium-dep*ndentin~ard~u~ren+s.ibutilideistfwonlydrlr:o~~thefourtoeh ancethiscurrent.(ReprintedwithpermissionfromEur J f%ar-
.
and fastest input rates causing the most QT prolon- In a’rabbit model of proarrhythrnia dependent on thegation. The QT interval peaks at the end of the in- formation of early afterdepolarizations, ibutilide pro-fusioh and rapidly returns to baseline by 2–6 hours. duced less polymo~hic ventricular tachycardia than
14 THE AMERICAN JOURNAL OF Cardiology@ VOL 78 (8A) OCTOBER 17, 1996
TM=600 msec
L
Ioonmec
‘;L+d-SotaJolo10.5M
nA
&
o.
-40 40
nA*
1.5-
1.2.
.9.
.6.
63.
0-
*I
mV
)’
I ODrug I
FIGURE4. Cornarativeeffectsaf classIllagentsanoutwardK+currents.Only ibutil-Jidehaslittlee ectonblockingthiscurrent.(ReprintedwithpermissionfromEur J Phar-
macy.’)
sotalol, sematilide, or dofetilide.15However, in hu- tribution phase and a short half-life, almost all casesman studies, ibutilide has caused both nonsustaine”d of polymorphic ventricular tachycardia have oc-(2.6%) and sustained (1.7%) polymorphic ventric- curred within 40 minutes of starting the infusion.lGular tachycardia.16Because ibutilide has a rapid dis- Proarrhythrnia is therefore a manageable risk, since
A SYMPOSIUM: TREATMENT OF ATRIA1 FIBRIL4TION AND FLUTTER 15
I TABLEI Electrophysiology crfIbutilide
Ibutilide(O.O3Omg/kg) Placebo
Variable (msec) Pacing Cycle Length (msec) Pre Past Pre Post
RAERPRAERPRAMAPRVERPRVERPRVMAPQRSQTc
400 211.5600 202.2600 242.1400 214.5600 234.5600 267.7
106.0418.2
254,0’ 222.2 220.6268,9* 239.6 254.6*323.6 274.1 270.2263,0’ 226.7 228.3283.0’ 247.7 253.6
340.2’ 276.4 280.9107.9 108.7 111.8514.6’ 418.8 431.6
* Statistically significant change from baseline (p <0.05].Abbreviations: Post = after treatment; Pre = before treatment; RAERP = right crtrialeffective refractory period;
RAMAP = right atrial monophasicaction potential; RVERP = right ventricular effectiverefractory period; RVMAP =right ventricular monophasicaction potential.
50
10
1 LIbutilideconcentration(pg/mL)mean* SD
a
o~-1 0 1 2 3 4
Time from startof Infusion(hOUr6)
530II
F d
-1 0 1 2 3 4Time from sfsrt of infusion(hours)
-0.03 mgkg-0.01 mgkg
FIGURE5. Wwtilide:clinicalpharmacologicchoroctwisficsinhealthvvolunteers.o: lbufilideconcentrationversusinfusionfime.b:QT.”infewaiversusinfusionfime.
corrective therapeutic measures can be administeredimmediately under telemetry conditions.
CONCLUSIONSIbutilide is a unique class III antiarrhythmic
agent with novel ionic channel activity. Its classIII effects and rapid plasma clearance make it auseful drug for the acute termination of atrial fib-rillation and flutter. Since ibutilide produces adose-proportional increase in QT. interval, it canoccasionally induce torsades de pointes. The riskof this arrhythmia is highest during and immedi-ately following administration, but it can be min-
imized by appropriate patient selection, vigilanceduring the period of highest risk, and by familiarityof the attending physician and medical staff intreating it.
1. Vaughan Williams EM. A classification of nntiarrhyfhmic actions reassessedafter a decade of new drugs. J C/in Pbmacol 1984;24:129–147.2. Cimini MG, Brnnden MN, Gibson JK. Effects of ibutilide fumarate, a novelantiamhythmic.agent and its action on isolated rabbit myacardium. Eur JPhar-7i+.5C01 1992;222:93-98.3. Lee KS, Tsai TD, Lee EW. Membrune, activity of class III antian’hythmiccompounds; a comparison between ibutilidc, d-sotalol, E-4031, sematilide anddofetilide. Eur J Phmtkzcol 1993;234:43-53.4. Lee KS. Ibutilide, a new compound with potent class 111antiarrbythmic ac-tivity, activates a slow inward Na+ current in guinea pig ventricular cells. JPharmacol Ezp Ther 1992;262:99-108.5. Whulley DW, Gmot AO. Role of sndium and potassium channels in atrialelectrogenesis and their blockade by antiarrbythmic drugs. In: DiMarco JP,Prystowsky EN, eds. AtrialArrhythmias. State of theArt. Mt. Kisco, NY: FuturaPublishing, 1994:171-200.6. Lee KS, Gibson JK, Hester JB. Ibutilide, a class III aatiarrhythmic with anovel mechanism of action. Current Drugs: Potassium Channel Modulators1992;KCM-B-119–137.7. Yang T, Snyders DJ, Roden DM. fbutilide, a methanesulfonanilide antiar-rhythnric, is a potent blocker of the rapidly activating delayed rectifier K+ cur-rent (1~) in AT-1 cells. Concentration-, time-, voltage-, and use-dependent ef-fects. Circulation 1995;91:1799-1806.8. Buchunaa LV, Turcotte UM, Kabell G, Gibson JK. Antiarrhythmic and elec-trophysiologic effects of ibutilide in a chronic canine model of atrial flutter. JCardiovasc Pharrnacol 1993;33:10–14.9. Nabih MA, Prcevski P, Fromm BS, et al. Effect of ibutilide, a new class IIIagent, on sustained atrial fibrillation in a canine model of acute ischemia andmyocardial dysfunction induced by microembolization. PACE Pacing ClinElecmophysiol 1993;16:1975-1983.10. Buchanan LV, Kabell G, Turcotte UM, Bmnden MN, Gibson JK. Effectsofibutilide on spontaneous and induced ventricular amhythmiain 24 hour caninemyocardial infarction: a comparative study with sotzdol and encainide. J Car-diovasc Phatrnacol 1992;19:256-263.11.Wesley RC, Farkhurri F, Morgan D, Zimmermun D. Jbutilide: enhanceddefibrillation via plateau sodium current activation. Am J Physio~1993;264:H1269-H1274.12. VanderLugt JT, Gaylor SK, Wakefield LK, Jungbluth GL, Walters RR,Kahell GO. Effects of ibutilide fumarate, a new class 111antiarrhytbmic agent,in man. C/in Pharmacol Ther 1991;49:188.13. Inoue H, Yamashita T, Nozaki A, et al. Effects of antiarrhythnric dregs oncanine atriat flutter due to reentry: role of prolongation of refractory period anddepression of conduction to excitable gap. JAm Coil Cardiol 1991;18:1038-1044.14. Jungbluth GL, Della-Coletta M, VanderLugt JT. Evaluation of phurmaco-kinetics and pharmacndyssamics of ibutilide fumarate and its enantiomers inhealthy mule volunteers. Pharm Res 1991:8:S-249.15. Buchanan LV, Kabell G, Bmnden MN, Gibson JK. Comparative assessmentof ibutilide, d-sotalol, clofilium, E-4031, and UK-68, 798 in a rabbit model ofprourrhytbsnia. J Cardiovasc Pharmacol 1993;220:540–549.16. Kowey PR, VanderLugt JT, Luderer JR. Ibutilide for acute conversion ofatriul fibrillation/ffutter: safety and risk benefit analysis. Am J Cardiol 1996.
16 THE AMERICAN JOURNAL OF CARDIOLOGY” VOL 78 (8A] OCTOBER 17, 1996