Embed Size (px)
Citation preview

Nina Zimmermann, Peter Schneider
WHO Collaborating Centre forPharmaceutical Pricing and Reimbursement Policies, Vienna
Gesundheit Österreich / Austrian Public Health Institute
2nd Summer School Pharmaceutical Pricing and Reimbursement Policies28 August – 01 September 2017 | Vienna, Austria
Pharmaceutical Pricing

The information and data provided in this presentation was collected and analyzed by the WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies located at the PharmacoeconomicsDepartment of Gesundheit Österreich GmbH (GÖG).
The data do not have any legally binding value. This is not a presentation of WHO. The presenter is responsible for the views expressed in this presentation, and they do not necessarily represent the decisions and policies of the World Health Organization.
Credits go to:- PPRI team members & WHO Collaborating Centre staff at GÖG- The members of the PPRI network (= competent authorities for
pharmaceutical pricing and reimbursement)
Information used from this presentation has to be correctly quoted. Commercial exploitation is forbidden.
Disclaimer and acknowledgements
2© 2017 Vienna WHO Collaborating Centre
Outline
© 2017 Vienna WHO Collaborating Centre
Medicine pricing policies
Different pricing policies for different types of
medicines
Pharmaceutical distribution chain and
remuneration of pharmacies and wholesalers, taxes
© 2017 Vienna WHO Collaborating Centre
Timely and equitable access to pharmaceuticals for
patients
Reward for valuable innovation within a
competitive and dynamic market that
also encourages Research &
Development
Control of pharmaceutical
expenditure
Conflicting policy goals in medicines policy
Source: High Level Pharmaceutical Forum 2005- 2008. Conclusions and Recommendations. European Commission DG Health & Consumers. 2008.

» Collate and appraise the available evidence on policies for managing medicine prices
» Based on best evidence and practice and experience develop recommendations for medicine pricing policies in countries
» Publish and disseminate the policy guidelines and recommendations to countries and other stakeholders
» 3 overarching questions:
1) Should countries use price control measures to manage medicine prices?
2) Should countries adopt measures to control add-on costs in the supply chain?
3) Should countries promote the use of quality assured generic medicines as a strategy to manage medicine prices?
© 2017 Vienna WHO Collaborating Centre
WHO Guideline on Country Pharmaceutical Pricing Policies 2015
http://apps.who.int/medicinedocs/documents/s21016en/s21016en.pdf

WHO Guideline on Country Pharmaceutical Pricing Policies 2015
Key principles
» Combination: use a combination of different pharmaceutical pricing policies (based on the objective, context and health system) that address supply and demand issues
» Transparency: make pricing policies, processes, and decisions transparent
» Legal basis: implement appropriate legislative framework and governance and administrative structures, supported by technical capacity - regularly reviewed, monitored and evaluated and amended
» Effective implementation: If regulation of pharmaceutical prices is introduced, effective implementation will be required to ensure compliance (e.g. incentives, enforcement, price monitoring system, fines)
» Promotion of generics: adopt policies to promote the use of quality assured generic medicines in order to increase access and affordability
» Collaboration: Countries should collaborate to promote exchange of information about policies, their impacts, and pharmaceutical prices

© 2017 Vienna WHO Collaborating Centre
Price control Free pricing
Statutorypricing
Pricenegotiations
Price is seton the basis
of a law, enactment,
decree
Prices arenegotiatedbetween
manufacturerand payer
Medicine pricing policies
Public procurement / tendering
Formal andcompetitiveprocurement
procedure
By thegovernment /
authorities
Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies.Glossary of pharmaceutical terms. Update July 2016. Accessible athttp://whocc.goeg.at/Glossary
8
Medicine prices – subject to price control
» Price control in most of the European countries
» Majority of the countries price control is limited to
reimbursable medicines
» BUT: Linkage between pricing and reimbursement in DE and DK
» Most common price control policy = statutory pricing (i.e.
setting the price on a regulatory, unilateral basis); e.g. BE, BG,
CY, CZ, EL, ES, LT, LU, PT, SE
» Price negotiations are used in a few countries (e.g. FR, IT)
» Procurement in the hospital sector and/or for public function
» Mixture
» Statutory pricing after negotiations (EE, LV, PL)
» In case of failure of negotiations (e.g. FR) or non-availability of
data for comparison (e.g. IE)
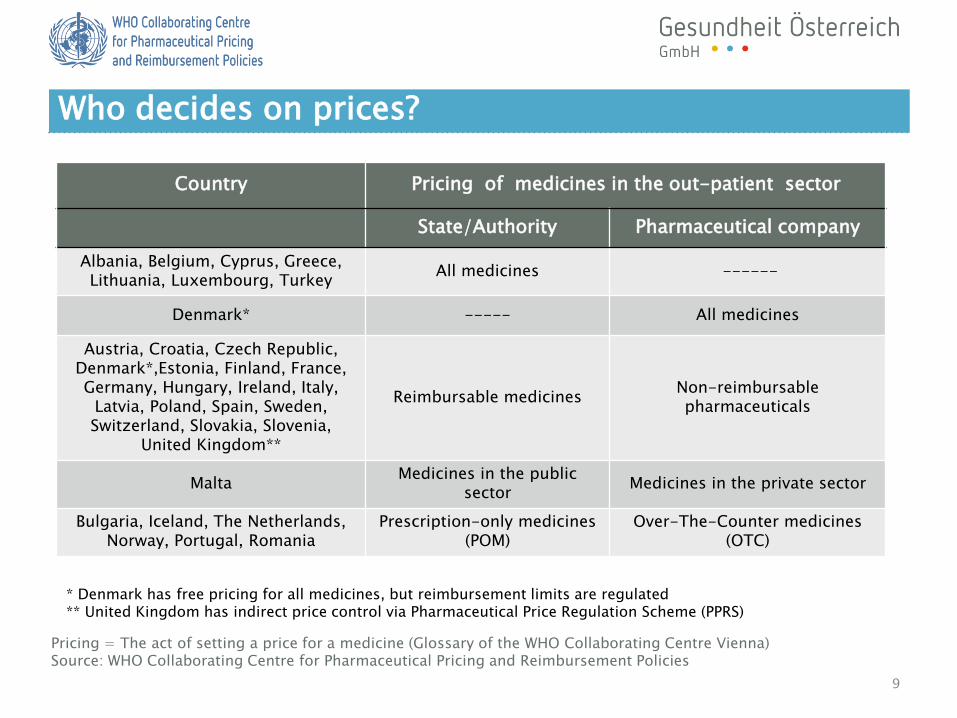
Pricing = The act of setting a price for a medicine (Glossary of the WHO Collaborating Centre Vienna)Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies
Country Pricing of medicines in the out-patient sector
State/Authority Pharmaceutical company
Albania, Belgium, Cyprus, Greece, Lithuania, Luxembourg, Turkey
All medicines ------
Denmark* ----- All medicines
Austria, Croatia, Czech Republic,Denmark*,Estonia, Finland, France, Germany, Hungary, Ireland, Italy,
Latvia, Poland, Spain, Sweden, Switzerland, Slovakia, Slovenia,
United Kingdom**
Reimbursable medicinesNon-reimbursablepharmaceuticals
MaltaMedicines in the public
sectorMedicines in the private sector
Bulgaria, Iceland, The Netherlands,Norway, Portugal, Romania
Prescription-only medicines(POM)
Over-The-Counter medicines(OTC)
9
* Denmark has free pricing for all medicines, but reimbursement limits are regulated** United Kingdom has indirect price control via Pharmaceutical Price Regulation Scheme (PPRS)
Who decides on prices?

» At the level of price types» Ex-factory price (manufacturer
price)
» Pharmacy purchasing price (wholesale price)
» Pharmacy retail price (gross / net)
» Different kind of medicines» Prescription-only medicines / Non-
prescription medicines
» Reimbursable / non-reimbursablemedicines
» On-patent / off-patent medicines
» Generics / biosimilar medicines
» Orphan drugs
» High-priced medicines / high-costmedicines
» For different sectors» Out-patient / in-patient sectors
» Public / private sectors
» From different perspectives» From industry perspective: ‘starting
price’, usually ex-factory price (sometimes also pharmacy purchasing price )
» From payer’s perspective: reimbursement price (actual price, tendering price in specific situations)
» From patient’s perspective: Pharmacy retail price / public price
© 2017 Vienna WHO Collaborating Centre
Medicine prices – dimensions of price control

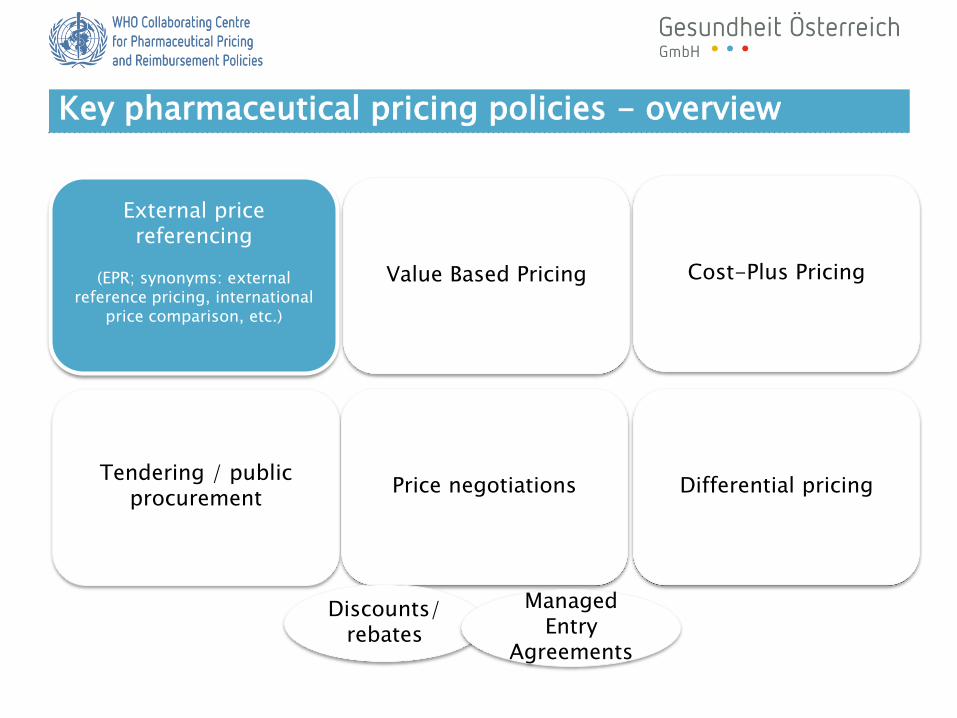
Key pharmaceutical pricing policies - overview
External pricereferencing
(EPR; synonyms: externalreference pricing, international
price comparison, etc.)
Value Based Pricing Cost-Plus Pricing
Tendering / publicprocurement
Price negotiations Differential pricing
Discounts/ rebates
ManagedEntry
Agreements
Key pharmaceutical pricing policies - overview
External pricereferencing
(EPR; synonyms: externalreference pricing, international
price comparison, etc.)
Value Based Pricing Cost-Plus Pricing
Tendering / publicprocurement
Price negotiations Differential pricing
Discounts/ rebates
ManagedEntry
Agreements

Definition:
the practice of using the price(s) of a pharmaceutical product in one or several countries in order to derive a benchmark or reference price for the purposes of setting or negotiating the price of the product in a given countrySource: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies. Glossary of pharmaceutical terms. Update July 2016. Accessible at http://whocc.goeg.at/Glossary
Coverage 2017
» EU Member States: 25/26 (DK in H) of 28 EU-MS
» different methodological approaches
13
External price referencing – definition and coverage

Notes: DK: EPR is used to set the price cap for new medicines in the hospital sector. In the out-patient sector the pharmaceutical manufacturer can freely set the price. DE: elements of EPR are – together with elements of free pricing and VBP - applied in the pricing process
Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Information, data collected with PPRI network
Use of EPR in European countries, 2017 (or latest available year)
Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Information, data collected with PPRI network
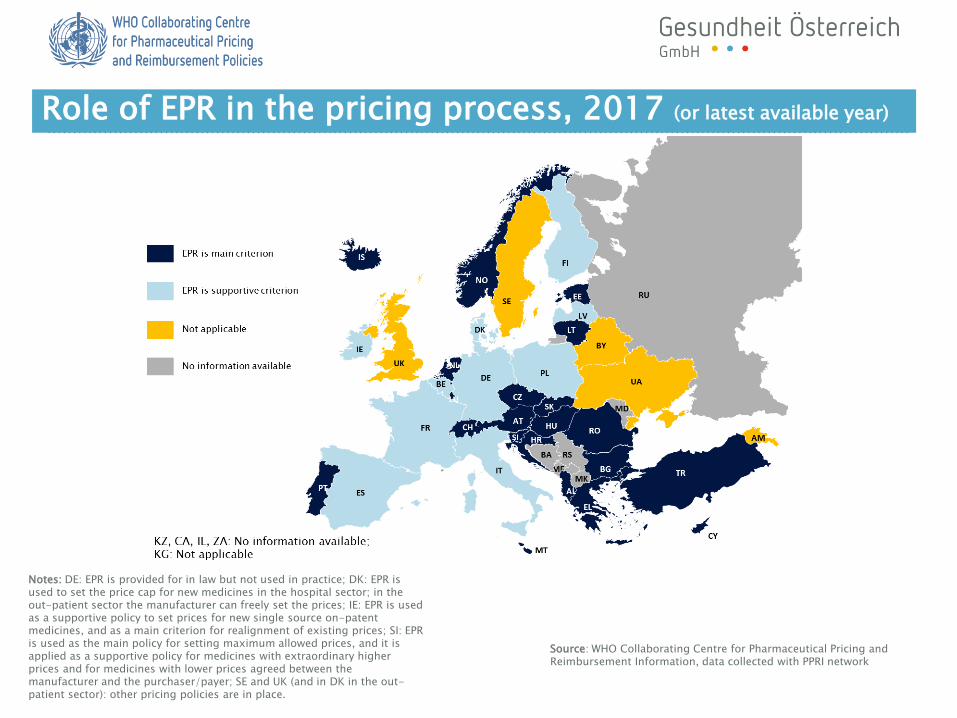
Notes: DE: EPR is provided for in law but not used in practice; DK: EPR is used to set the price cap for new medicines in the hospital sector; in the out-patient sector the manufacturer can freely set the prices; IE: EPR is used as a supportive policy to set prices for new single source on-patent medicines, and as a main criterion for realignment of existing prices; SI: EPR is used as the main policy for setting maximum allowed prices, and it is applied as a supportive policy for medicines with extraordinary higher prices and for medicines with lower prices agreed between the manufacturer and the purchaser/payer; SE and UK (and in DK in the out-patient sector): other pricing policies are in place.
Role of EPR in the pricing process, 2017 (or latest available year)

Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Information, data collected with PPRI network
Notes: ES: the number of countries has not been defined, mainly Euro zone countries are taken into account. IT: the countries are not defined, but prices from countries which participate in the Euripid database are considered. SE and UK (and in DK in the out-patient sector): other pricing policies are in place. DE: EPR is not applied in practice.
Number of countries in the basket, 2017 (or latest available year)
Major criteria for country baskets: geographic neighborhood or a comparable economic situation in the reference countries
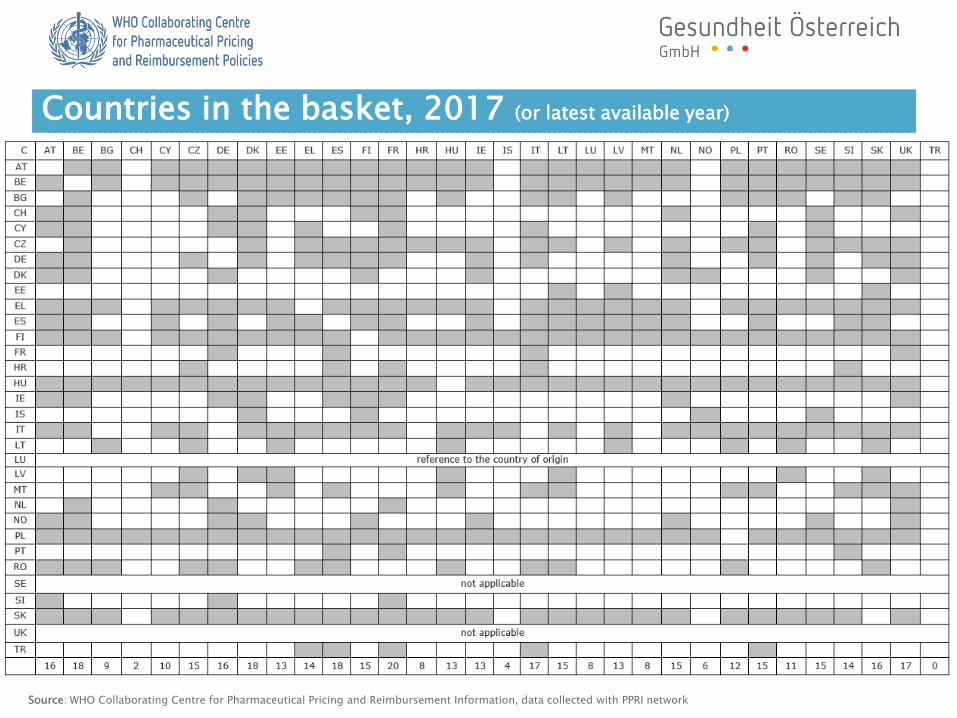
Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Information, data collected with PPRI network
Countries in the basket, 2017 (or latest available year)

Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Information, data collected with PPRI network
Notes: CZ, EL, NO & SK: Average of the three lowest prices of reference countries in the basket. EE: Prices cannot exceed the highest valid price in reference countries. FR: prices should be similar to those in the reference countries and should not be lower than the lowest price in one of the four reference countries. IL: Average of four countries (FR, BE, HU, ES). The lowest price between this average and the price in NL will be chosen. In case of no reference from all five countries the average price between DE and UK. IS: The average price of reference countries is used for out-patient medicines while the lowest price of reference countries is used for in-patient medicines. LT: The reference price shall not exceed 95% of the average price of reference countries. LV: The third lowest price in the country basket, but not higher than the price in LT & EE. SI: The lowest price is used for original medicines and the average price for generics. SE and UK (and in DK in the out-patient sector): other pricing policies are in place. DE: EPR is not applied in practice.
Methodology to determine the reference prices, 2017 (or latest available year)

Differences between countries with respect to
» scope of medicines e.g. originators, prescription-only
medicines, new innovative medicines
» price type considered e.g. ex-factory price, wholesale
price, list prices
» price revisions (regular and irregular intervals)
» price sources (mainly MAH)
» dealing with missing information
» exchange rates
19
Further results on EPR
» Savings:
» EPR can lead to substantial savings for public payers, but the effect seems to ‘fade-out’ in the course of time
» The authorities who recently introduced EPR considered the policy as effective, whereas authorities with longer-term experiences with EPR said that the benefits of the beginning have increasingly been foiled by limitations arising after some time
» Limitations:
» Incentivises manufacturers to first launch in high-priced countries and delay (or not launch) in lower-price countries availability problems
» Non-consideration of (even statutory) discounts lead to a distortion of prices, and public payers risk overpaying transparency concerns
» EPR is not a simple exercise but requires expertise and administrative efforts to establish and run an appropriate system
» Prices obtained by EPR do not reflect the value of a medicine in the given country and are influenced by the design of the system
» EPR is exposed to exchange rate-volatility when referenced prices are denominated in local currencies
20
Experiences with EPR according to a literature review

Countries which apply EPR have lower prices.
Price differences among countries that apply EPR.
Source: Leopold, C., Mantel-Teeuwisse, A.K., Seyfang, L., Vogler, S.,de Joncheere, K., Laing, R.O., Leufkens, H.G.M.: Impact of External Price Referencing on Medicine Prices – A Price Comparison Among 14 European Countries. In: Southern Med Review, 5(2): 34-41
21

» EPR as benchmark: Countries should consider using external reference pricing as a method for negotiating or benchmarking the price of a medicine.
» Part of overall strategy: Countries should consider using external reference pricing as part of an overall strategy, in combination with other methods, for setting the price of a medicine.
» Transparency: In developing an external reference pricing system, countries should define transparent methods and processes to be used.
» Comparability: Countries / payers should select comparator countries to use for ERP based on economic status, pharmaceutical pricing systems in place, the publication of actual versus negotiated or concealed prices, exact comparator products supplied, and similar burden of disease. 22
WHO Guideline: Use of External Price Referencing
http://apps.who.int/medicinedocs/documents/s21016en/s21016en.pdf

» A simple base scenario was constructed to highlight general features of EPR systems within Europe
» Inputs for the model were extracted from a survey
» Medicine prices for countries that stated not to re-evaluate their EPR prices stay constant over the years
» In other countries, prices drop at consecutive re-evaluation rounds
» The erosion of the average price over the years is at about 15%
Simulations of different scenarios
23
607
0809
0100
607
0809
0100
607
0809
0100
607
0809
0100
607
0809
0100
607
0809
0100
0 50 100 150 0 50 100 150 0 50 100 150 0 50 100 150 0 50 100 150
0 50 100 150
Austria Belgium Bulgaria Croatia Cyprus CzechRepublic
Denmark Estonia Finland France Germany Greece
Hungary Iceland Ireland Italy Latvia Lithuania
Luxembourg Malta Norway Poland Portugal Romania
Slovakia Slovenia Spain Sweden Switzerland TheNetherlands
UK
me
dic
ine p
rice a
t m
onth
=12
0
monthGraphs by country
0
10
20
30
40
50
60
70
80
90
100
110
DK
SE
UK
AT
BE
LU
CH IE DE IS NO SI
FR
NL FI
PT
MT
CY
PL
LT
HU
BG
CZ
EE
EL IT LV
SK
ES
RO
HR
Source: Vogler S, Lepuschütz L, Schneider P, Stühlinger V.: Study on enhanced cross-country coordination in the area of pharmaceuticalproduct pricing. Written by Gesundheit Österreich Forschungs- und Planungs GmbH, University for Health Sciences, Medical Informaticsand Technology (UMIT) and SOGETI. Funded by the Health Programme of the European Union, 2016, Viennahttps://ec.europa.eu/health//sites/health/files/systems_performance_assessment/docs/pharmaproductpricing_frep_en.pdf
Simulations of six scenarios
» In the simulations six scenarios were explored
» (1) Consideration of statutory discounts;
» (2) regular price revisions;
» (3) changes in country baskets with respect to size and income;
» (4) changes in the calculation method;
» (5) changes in choice of exchange rate; and
» (6) the consideration of the affordability-to-pay
24
Source: Vogler S, Lepuschütz L, Schneider P, Stühlinger V.: Study on enhanced cross-country coordination in the area of pharmaceutical product pricing. Written by Gesundheit Österreich Forschungs- und Planungs GmbH, University for Health Sciences, Medical Informatics and Technology (UMIT) and SOGETI. Funded by the Health Programme of theEuropean Union, 2016, Viennahttps://ec.europa.eu/health//sites/health/files/systems_performance_assessment/docs/pharmaproductpricing_frep_en.pdf
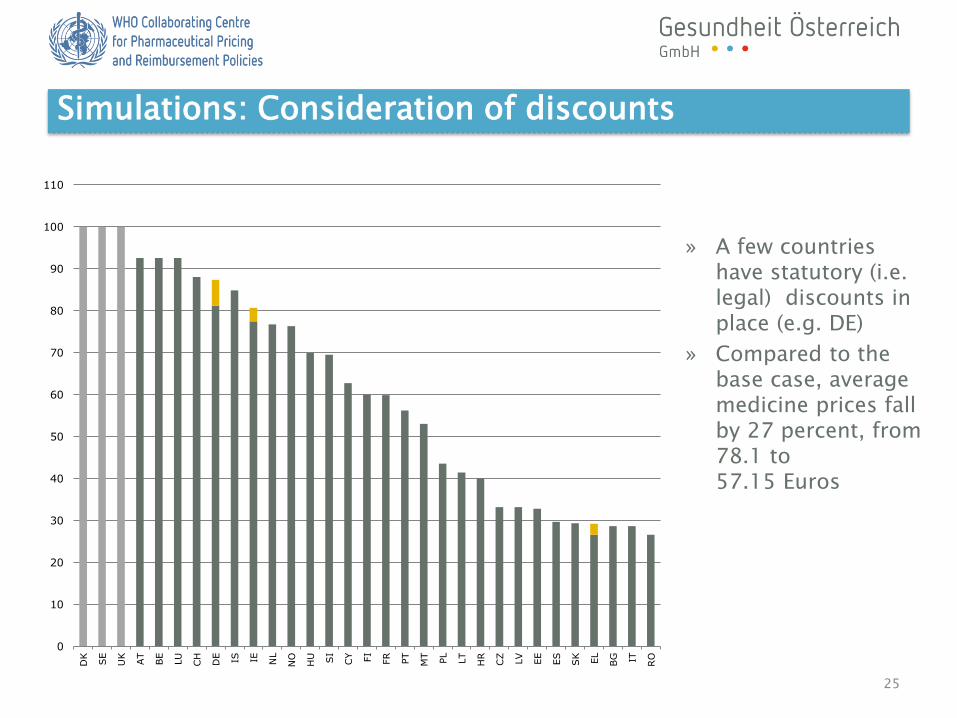
» A few countries have statutory (i.e. legal) discounts in place (e.g. DE)
» Compared to the base case, average medicine prices fall by 27 percent, from 78.1 to57.15 Euros
Simulations: Consideration of discounts
25
0
10
20
30
40
50
60
70
80
90
100
110
DK
SE
UK
AT
BE
LU
CH
DE IS IE NL
NO
HU SI
CY FI
FR
PT
MT
PL
LT
HR
CZ
LV
EE
ES
SK
EL
BG IT RO
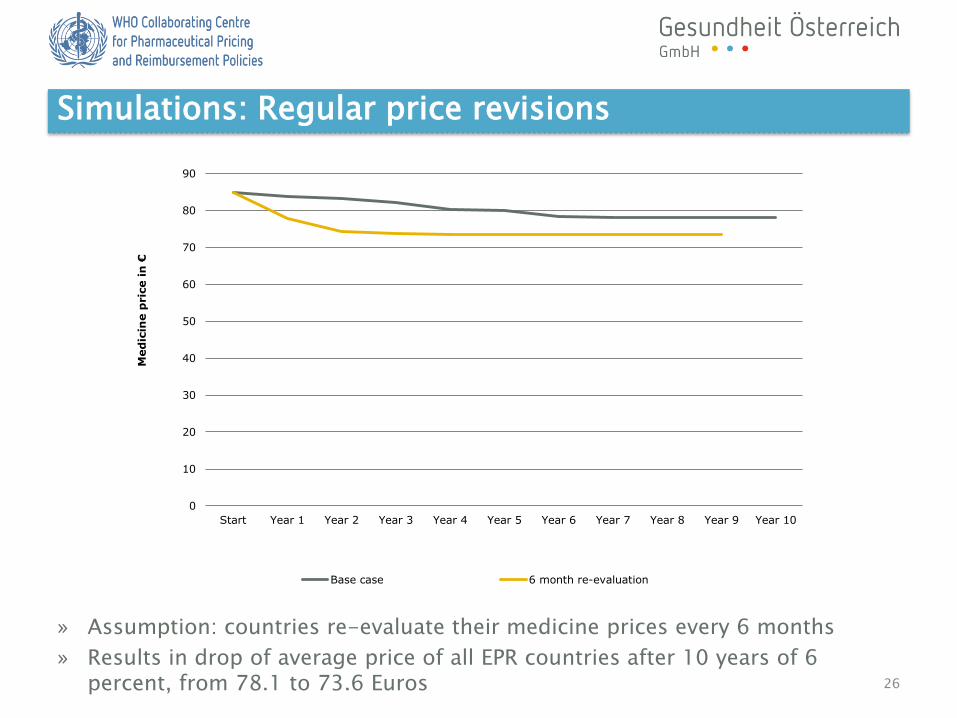
» Assumption: countries re-evaluate their medicine prices every 6 months
» Results in drop of average price of all EPR countries after 10 years of 6 percent, from 78.1 to 73.6 Euros
Simulations: Regular price revisions
26
0
10
20
30
40
50
60
70
80
90
Start Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7 Year 8 Year 9 Year 10
Med
icin
e p
ric
e i
n €
Base case 6 month re-evaluation

» Assumption: Countries agree not to reference to the least wealthy countries (lowest GDP quintile)
» Leads to a negligible, insignificantly small rise in EPR prices
Simulations: Changes in country baskets
27
0
10
20
30
40
50
60
70
80
90
100
DK SE UK AT BE LU CH IE DE IS NO SI FR NL FI PT MT CY PL LT HU BG CZ EE EL IT LV SK ES RO HR
Prices under base case Prices when excluding lowest-income quintile from reference baskets
Source: Vogler S, Lepuschütz L, Schneider P, Stühlinger V.: Study on enhanced cross-country coordination in the area of pharmaceuticalproduct pricing. Written by Gesundheit Österreich Forschungs- und Planungs GmbH, University for Health Sciences, Medical Informaticsand Technology (UMIT) and SOGETI. Funded by the Health Programme of the European Union, 2016, Viennahttps://ec.europa.eu/health//sites/health/files/systems_performance_assessment/docs/pharmaproductpricing_frep_en.pdf
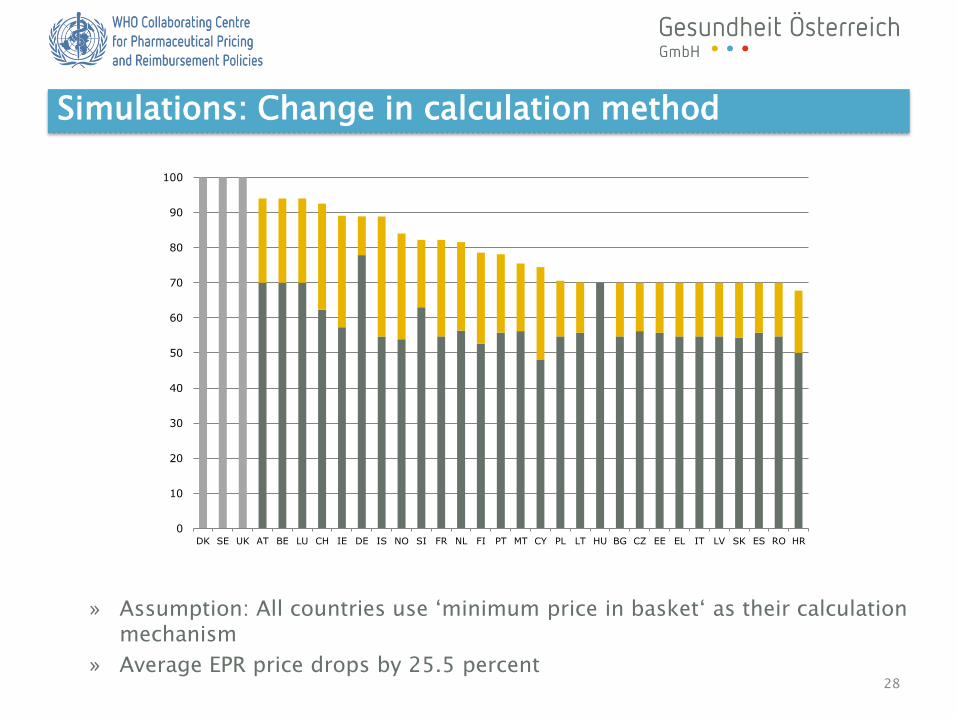
» Assumption: All countries use ‘minimum price in basket‘ as their calculation mechanism
» Average EPR price drops by 25.5 percent
Simulations: Change in calculation method
28
0
10
20
30
40
50
60
70
80
90
100
DK SE UK AT BE LU CH IE DE IS NO SI FR NL FI PT MT CY PL LT HU BG CZ EE EL IT LV SK ES RO HR

» Scenario of all countries using average monthly exchange rates compared toyearly exchange rates
» For BG, CZ, IT and NO the price changes by more than 7 percent
Simulations: Choice of exchange rate
29
0
10
20
30
40
50
60
70
80
90
100
110
UK SE DK IS CH AT BE LU IE FI FR SI DE NO NL PT CY MT PL HR RO LV IT LT EE CZ ES SK EL BG HU
using average yearly exchange rates using average monthly exchange rates

» Assumption: all countries include PPP-adjustments for their reference prices
» Prices in some wealthy countries increase, while they drop in some less wealthy countries such as BG, HU, PL, RO
Simulations: Purchasing Power Parity
30
0
20
40
60
80
100
120
140
DK SE UK AT BE LU CH IE DE IS NO SI FR NL FI PT MT CY PL LT HU BG CZ EE EL IT LV SK ES RO HR
Base scenario All countries applying PPP adjustments

Key take-aways from the simulations
» Choices in the design of EPR mechanisms (e.g. basket,
re-evaluation period, calculation method, exchange rate
used) matter
» Referring to actual prices paid might reduce prices by
allowing countries with low negotiation power to benefit
from discounts
» Regular re-evaluations tend to lead to faster price drops
and lower average prices
» Coordinating to adapt EPR formulae, such as adjusting
for purchasing power parity, might reduce medicine
prices in lower-income countries in relation to wealthier
countries
31

32
Suggestions for improvements EPR
» Clear methodology
» Well-chosen basket of countries (issue of work-load for large basket)?
» Consider the economic situation of reference countries (choice of reference countries, weighting by PPP)
» Regular monitoring and price revisions (key part of the market)
» Consideration of discounts, at least published mandatory discounts;in the longer run transparency related to discounts, cost elements of the prices
» Policy mix and ‘new’ policies beyond the pricing scope
» Collaborative approaches
Country example - Norway
» Current system of EPR – implemented in 2002
» The maximum price for prescription-only-medicines is set due to external reference pricing
» The Market Authorisation Holder (MAH) has to apply for a maximum price (pharmacy purchasing price PPP) before entering the market
» NoMA revises the price of the 250 top-selling active ingredients on a yearly basis
» Maximum prices are based on the average of the three lowest PPP in Sweden, Finland, Denmark, Germany, United Kingdom, the Netherlands, Austria, Belgium and Ireland
» Comparison is mainly be drawn with the same product in the reference countries (incl. different brand names
» Mean exchange rate of the last six whole months, as presented by the Central Bank of Norway, is used for the conversion
© 2017 Vienna WHO Collaborating Centre
Key pharmaceutical pricing policies - overview
External pricereferencing
(EPR; synonyms: externalreference pricing, international
price comparison, etc.)
Value Based Pricing Cost-Plus Pricing
Tendering / publicprocurement
Price negotiations Differential pricing
Discounts/ rebates
ManagedEntry
Agreements

Definition:
... it is meant for countries to set prices for new medicines and/or decide on reimbursement based on the therapeutic value that the medicine offers, usually assessed through health technology assessment (HTA) or economic evaluation.Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies. Glossary of pharmaceutical terms. Update July 2016. Accessible at http://whocc.goeg.at/Glossary
Narrow definition: integrated in the pricing and reimbursement system: link payments for medicines to evidence-based assessments of value for patients (+ their relatives and the society as a whole)
» Countries with narrower definition: SE (UK – planned, not implemented); AUS, NZ
» Countries with broader definition: nearly all EU MS35
Value Based Pricing – Definition and Coverage

» Introduced in 2002
» Pricing processes are completely integrated
» National competent authority (the Dental and Pharmaceutical Benefits Board (TLV)) will communicate a joint reimbursement and pricing decision
» Added value is assessed for all new medicines and where higher prices are granted to medicines that demonstrate higher added value
» Cost-effectiveness is analysed from a broad societal perspective (but hesistant with including productivity effects), also important: severity, uncertainty
» Value based pricing: price in relation to value for society, extensive use of HTA
36
Value Based Pricing – Example Sweden

37
Source: TLV
Value Based Pricing – Example Sweden

» No incentives for manufacturers to price below threshold
» Relatively large differences in the definition of what should be included in ‘value’ and what excluded, across countries
» Value assessments cannot be ‘exported’ to countries which apply EPR since the extent of ‘value’ is country- and system-specific
» Capacity-building
38
Value Based Pricing – Impact and limitations

Key pharmaceutical pricing policies - overview
External pricereferencing
(EPR; synonyms: externalreference pricing, international
price comparison, etc.)
Value Based Pricing Cost-Plus Pricing
Tendering / publicprocurement
Price negotiations Differential pricing
Discounts/ rebates
ManagedEntry
Agreements

Definition:
Pricing procedure which calculates a ’reasonable’ price for a product based on the production costs, promotional expenses, research & development, administration costs, overheads and profitSource: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies. Glossary of pharmaceutical terms. Update July 2016. Accessible at http://whocc.goeg.at/Glossary
Cost-plus pricing is not used in EU Member States
» Country examples: » Bangladesh, China, Islamic Republic of Iran, Pakistan,…
40
Cost-Plus Pricing – Definition and Coverage

» Not as sole policy: Countries generally should not use a cost-plus method as an overall pharmaceutical pricing policy
» Change to another policy: Countries using a cost-plus method as an overall policy that wish to change their strategy should consider replacing or complementing the cost-plus approach with other policies, including EPR etc.
41
WHO Guideline: Application of cost-plus pricing formulae for pharmaceutical price setting
http://apps.who.int/medicinedocs/documents/s21016en/s21016en.pdf
Key pharmaceutical pricing policies - overview
External pricereferencing
(EPR; synonyms: externalreference pricing, international
price comparison, etc.)
Value Based Pricing Cost-Plus Pricing
Tendering / publicprocurement
Price negotiations Differential pricing
Discounts/ rebates
ManagedEntry
Agreements

Procurement - Definition: Pharmaceutical procurement is a complex process that involves many steps and many stakeholders. It is also conducted within national and institutional policies, rules, regulations, and structures that may hinder or support the overall efficiency of the procurement process. An effective procurement process at any level must ensure that four strategic objectives are achieved:
- the procurement of the most cost effective medicines in the right qualities,
- the selection of reliable suppliers of high-quality products,
- procurement and distribution systems that ensure timely and undisturbed deliveries,
- processes that ensure the lowest possible total costs.
Tendering - Definition:Any formal and competitive procurement procedure through which tenders (offers) are requested, received and evaluated for the procurement of goods, works or services, and as a consequence of which an award is made to the tenderer whose tender/offer is the most advantageous. For specific medicines for which equivalents (e.g. generics) exist, public payers ask (generic) manufacturers for bids, and the best tender will be awarded a contract for a specific time.
Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies. Glossary of pharmaceutical terms. Update July 2016. Accessible at http://whocc.goeg.at/Glossary
43
Tendering / Public procurement – Definition
No centraltendering/procurement in EU
In-patient sector: majorpricing policy
Out-patient sector: fewEuropean countries

44
» Few examples from different European countries (preferential pricing policy – NL, DK, BE/once, CY, MT..)
» Highly competitive measures
» Impact on prices
» Requires flexibility from pharmacists (stock-keeping, e.g. change every two weeks / DK)
» Short-term savings
» Medicines shortages?
Competition vs. regulation ?
Tendering in the out-patient sector

» 2007/2008: ‘Kiwi light model’ (higher R rate for winner)
» 2 tenders (simvastatin & amlodipine), supply problems,
discontinued
» Increased utilization of further publicly funded, not
tendered statins in the year of the first tender neutralized
savings of € 14.6 mio. made on the simvastatin tender
45
» Companies are obliged to report their planned PPP for next
two weeks to the Danish Medicines Agency (IT system)
» All reimbursable out-patient medicines
» Decrease in public pharmaceutical expenditure and at the
same time increase in medicine consumption
» ‘Preference price policy’: 2005-2008 collectively, since 2008 by
individual sickness funds, similar models by some health insurers
» Large savings (€ 352 million in 2009, € 654 million in 2012 and
€ 679 million in 2014), temporary increase in the dispensing fee
» Large-scale shortages for tendered and non-tendered medicines
ResultsResults
Source: Vogler S, Gombocz M, Zimmermann N.: Tendering for off-patent outpatient medicines: lessons learned from experiences in Belgium, Denmark and the Netherlands. In: Journal of Pharmaceutical Health Services Research, 2017
» Robust legal framework
» Strategic design of tender (e.g. winner-
takes-it-all principle?, contract duration)
» Strategies to address medicines shortages
» Stakeholder management
» Demand-side measures to promote generic
uptake
46
Discussion & conclusion: key prerequisitesTendering in the out-patient sector - prerequisites

Tender NO
SE
FI
DK
DE
FR
ESPT
CH
IT
MT
CY
ATHU
SI
SKCZ
PL
EE
LV
LT
IE
EL
BG
RO
BA
HR
AL
MKME
RS
LU
BE
NL
Not scope of the survey and/orno information available
UK
IS
Source: PHIS Hospital Pharma, based on PHIS Hospital Pharma reports and further surveys; 27 countries (EU MS excl. EL & LU; NO + TR)
TR
IS
47
Tender & Negotiation
Procuring strategies in hospitals
Key pharmaceutical pricing policies - overview
External pricereferencing
(EPR; synonyms: externalreference pricing, international
price comparison, etc.)
Value Based Pricing Cost-Plus Pricing
Tendering / publicprocurement
Price negotiations (Differential pricing)
Discounts/ rebates
ManagedEntry
Agreements

Definition:
A pricing procedure, where medicine prices are discussed/ negotiated (e.g. between manufacturer and public payer).
Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies. Glossary of pharmaceutical terms. Update July 2016. Accessible at http://whocc.goeg.at/Glossary
» Results of the price negotiations are lower prices than the list prices and often kept confidential
» Confidential prices distort price comparisons
49
Price negotiations – Definition and Coverage

Discounts and rebates to public payers, 2011
Only discounts and rebates by pharmaceutical industry
Vogler S, Zimmermann N, Habl C, Piessnegger J, Bucsics A.: Discounts and rebates granted to public payers for medicines in European countries. In: Southern Med Review 2012, 5(1): 38-46http://whocc.goeg.at/Literaturliste/Dokumente/Articles/Vogler_Discounts_Rebates_SMR_2012_5_1.pdf
50

Discounts and rebates on medicines
Study results 2016 within a sample of high-income countries:
» Most frequent discount received was between 20% and 29% of official list prices;
» 6 participants reported: 60% or more of the list prices;
» On average: confidential discounts were more common, complex, and significant for specialty pharmaceuticals than for primary care pharmaceuticals;
» Participants had a more favorable view of the impact of confidential discount schemes on their health systems than on the global marketplace
© 2017 Vienna WHO Collaborating Centre
Source: Morgan S, Vogler S, Wagner A.: Payers’ experiences with confidential pharmaceutical Price discounts: A survey of public and statutory health systems in North America, Europe, and Australasia. In: Health Policy, 121, Issue 4: 354-362, April 2017, http://dx.doi.org/10.1016/j.healthpol.2017.02.002
Key pharmaceutical pricing policies - overview
External pricereferencing
(EPR; synonyms: externalreference pricing, international
price comparison, etc.)
Value Based Pricing Cost-Plus Pricing
Tendering / publicprocurement
Price negotiations Differential pricing
Discounts/ rebates
ManagedEntry
Agreements

Definition:
» Different prices for different groups of customers
» ‘Equity pricing’ vs. ‘discriminant monopolist’
» Systematic use of DP has been limited to vaccines,
contraceptives and ARVs mostly in LMIC; wide-
spread use of EPR and parallel trade concept limit
application within EU
Differential pricing: Definition and coverage
53

Experiences with Differential Pricing (DP)
54
» Benefits
May ensure access to medicines that would
otherwise have been unaffordable for these countries
Under specific conditions: when competitive production is feasible,
rapid access and small quantities of medicines are required
Benefits for manufacturers: increased revenue
» Limitations
Not an instrument for savings
Generic competition is likely to be more effective in reducing
prices than DP
Not a ‘stand-alone’ policy
Reliance on industry
Not sustainable
» v
For example
» High priced medicines / high-cost medicines
» Generics / biosimilars
© 2017 Vienna WHO Collaborating Centre
Different policies for different types of medicines

» Definition? What is a high price?
© 2017 Vienna WHO Collaborating Centre
Pricing policies for high-priced medicines
Source: Results of a survey among PPRI network members, 2014 (27 countries replied)
WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies
http://whocc.goeg.at/Downloads/Conference2015/Presentations/MO/1545_strandIII_Zimmermann_new.pdf

Generic price link
Definition:
Practice of setting the price of a generic in relationship to the original product, usually at a certain percentage lower than the original medicine price. The design of this generic price link policy may vary, with different percentages for the different generics (first generic coming to the market, second generic, etc.), and in some cases the prices of orignal medicines might also be part of the policy, i.e. that they will also be required to decrease.
Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies. Glossary of pharmaceutical terms. Update July 2016. Accessible at http://whocc.goeg.at/Glossary
© 2017 Vienna WHO Collaborating Centre
Pricing policies for generics

58
Generic price link 2016
Source: WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Information, data collected with PPRI network 2016
Example Estonia:The first follower is required to be priced 30% below the originator. The next three followers need to be priced by at least 10% below of cheapest medicine in the group Similar
regulationsfor
biosimilars

The staged approachto price components
Source: WHO/HAI 2008: Measuringmedicine prices,availability,affordability and pricecomponents
Pharmaceutical distribution chain and remuneration of pharmacies and wholesalers
In EU Member States:
• Pharmacy andwholesale
remuneration• VAT

Reimbursable medicines
» Most countries regulate both wholesale and pharmacy remuneration
» Two (Switzerland, Czech Republic) out of 30 European countries (EU-28, Norway, Switzerland) have joint remuneration of wholesale and pharmacy markets
» In these countries both actors share the regulated regressive mark-up for distribution and dispensing.
» Three (Malta, Netherlands, Cyprus) countries do not
have binding, national remuneration regulation;
» In Malta and Cyprus the market is
segregated into public and private
sectors with remuneration regulation
only valid in the private sector.
» Netherlands liberalized
pharmacy remuneration in 2012 with
agreements being negotiated
by individual actors.
60
L
Pharmaceutical distribution chain and remuneration of pharmacies and wholesalers
Source: GÖG (2015)‚ Vergütung der Arzneimitteldistribution in den europäischen Ländern

» In eight countries wholesale remuneration is not regulated (e.g. Denmark, Finland, UK);
» In these countries manufacturers and wholesalers negotiate confidential wholesale margins.
» 22 countries regulate maximum wholesale
remuneration for the reimbursement
market; in 11 countries the
regulation applies to all
pharmaceuticals.
61
L
Wholesale remuneration for reimbursable medicines
Source: GÖG (2015)‚ Vergütung der Arzneimitteldistribution in den europäischen Ländern

» Wholesale remuneration in Europe tends to be related to the price of distributed pharmaceuticals (price-oriented remuneration)
» Most countries regulate maximum remuneration through a mark-up on the ex-factory price (exception: Italy)
» Regressive remuneration schemes, in which proportional remuneration decreases with the pharmaceutical price are more common than linear mark-ups.
» The regressive schemes used in
Europe include from 2 (eg. France)
to 16 (eg. Germany) categories often combining percentage-based components with a fixed fee.
62
IE
Wholesale remuneration for reimbursable medicines in detail
Source: GÖG (2015)‚ Vergütung der Arzneimitteldistribution in den europäischen Ländern

» In 16 countries, pharmacy remuneration depends exclusively on the price of disbursed pharmaceuticals (price-oriented remuneration).
» In 5 countries (e.g. UK, the Netherlands) remuneration is exclusively service-based(e.g. fixed fee per disbursed medicine).
» 7 countries (e.g. Belgium, Germany, Switzerland) have a mixed remuneration scheme.
» In most countries with a mixed scheme the price-oriented element appears to be given more weight (Exception: Switzerland).
63
SI
CY
UK
HU
CZ
ES
SK
CH
SE
RO
PT
PL
AT
NO
NL
MT
LU
LT
LV
HR
IT
IS
IE
EL
FR
FI
EE
DE
DK
BG
BE
Not relevant
Service-based
Mixed
Price-oriented
Source: GÖG (2015)‚ Vergütung der Arzneimitteldistribution in den europäischen Ländern
Pharmacy remuneration for reimbursable medicines

© 2017 Vienna WHO Collaborating Centre
For reimbursable and non-reimbursable medicines
Manufacturerprice
Max. wholesalemark up in %
Pharmacypurchase Price
max. wholesalemargin in %
Starting from to Starting from to
0,00 1,60 20% 0 1,92 16,7%
1,61 2,88 15% 1,85 3,31 13,0%2,89 6,39 10% 3,18 7,03 9,1%6,40 12,78 5% 6,72 13,42 4,8%
12,78 213,08 3% 13,16 219,47 2,9%
Maximum per package 6,39 213,08... 6,39
PharmacypurchasePrice % mark-up
Fixed mark up in Euro
PharmacyRetail Price net
max. Pharmacymargin
Starting from toStartingfrom to
0 0,64 0,38 0 0,64 0,38
0,65 1,28 40% 1,29 1,79 29%
1,29 1,92 35% 1,74 2,59 26%
1,93 2,56 30% 2,51 3,33 23%
2,57 3,2 25% 3,21 4,00 20%
3,21 6,39 20% 3,85 7,67 17%
6,4 44,74 15% 7,36 51,45 13%
44,74… 5,11 Euro 49,85... 5,11 Euro
Country example Estonia

65
CY
UK
HU
CZ
ES
SI
SK
CH
SE
RO
PT
PL
AT
NO
NL
MT
LU
LT
LV
HR
IT
IS
IE
EL
FR
FI
EE
DE
DK
BG
BE
Not relevant
No compulsory pharmacy discounts/clawbacks
Compulsory pharmacy discounts/clawbacks
Compulsory discounts and clawbacks to the public sector influence pharmacy remuneration in 15 countries
Pharmacy remuneration for reimbursable medicines –Discounts/Clawbacks
Source: GÖG (2015)‚ Vergütung der Arzneimitteldistribution in den europäischen Ländern

» Countries should consider regulating distribution chain mark-ups (i.e. regulation of distributors and wholesalers)
» Countries should consider regulating retail chain mark-ups and fees (i.e. regulation of pharmacies, dispensing doctors and dispensaries)
» If mark-ups are regulated, countries should consider regressive mark-ups (i.e. lower mark-up for higher-priced products) rather than fixed percentage mark-ups
» Incentive to dispense higher priced products because they receive a higher net margin
» Countries should consider using remuneration/mark-up regulation to provide incentives for supplying specific medicines (e.g. generics) or to protect specific patients or population groups (e.g. vulnerable groups, remote populations)
» In systems where rebates and discounts in the distribution chain occur, countries should consider regulation and should make them transparent 66
WHO Guideline: Regulation of mark-ups inthe pharmaceutical supply and distribution chain
http://apps.who.int/medicinedocs/documents/s21016en/s21016en.pdf

2021
19
21
19
25
20
23
21
24
20
25
27
22
17
21 21
18
21
23 23
20
25
22
20 20
10
6
20
5
109
6
4
10
2,1
5 5
23
3
5
12
0
6
89
0
9,5 10
0
10
25
12
10
0
5
10
15
20
25
30
AT BE BG CY CZ DE DK EE EL ES FI FR * HR* HU IE** IT LU LT * LV MT NL PL PT RO SE* SI SK UK*
standard VAT in %
VAT in % for reimbursable medicines (marked with an asterix) and for medicines (POM and OTC medicines) supplied on foot of a prescription (UK, SE)
VAT in % for non-reimbursable medicines (marked with an asterix) and for (non-prescription) medicines purchased without prescription
** In Ireland depends the VAT rate on the route of administration e.g. on oral medicines the VAT rate is 0% on external applications (creams,lotions,
ointments, injections, etc.) the rate is 23%; For a few products (low protein biscuits, hormonal contraception) 13,5% VAT is applied
Value-added tax in European countries

» Benefits of tax exemptions» Most likely to have an equity impact on the poor
» Downsides of tax exemptions» Loss of revenue for national governments
» Elimination or decrease of taxation revenue from medicines may have a negative impact on some aspects of the health care system
» Countries should consider exempting essential medicines from taxation
» Countries should ensure any reductions or exemptions from taxes on medicines have the effect to reducing costs to the patient/purchaser
68
WHO Guideline: Tax exemptions/reductions for pharmaceutical products
http://apps.who.int/medicinedocs/documents/s21016en/s21016en.pdf
Nina Zimmermann
Peter Schneider
Stubenring 6
1010 Vienna
T: +43 1 515 61 – 132 or 116
F: +43 1 513 84 72
Email:
www.goeg.at
http://whocc.goeg.at
Vienna WHO CC websitehttp://whocc.goeg.at
Contact
© 2016 Vienna WHO Collaborating Centre