Embed Size (px)
Citation preview

PAIN MEDICINE
Volume 7
•
Number S1
•
2006
© American Academy of Pain Medicine 1526-2375/06/$15.00/S35 S35–S46
Blackwell Publishing IncMalden, USAPMEPain Medicine1526-2375American Academy of Pain Medicine20067S1S35S46Original Article
Pre-Operative WorkupVillavicencio and Burneikiene
Reprint requests to:
Alan T. Villavicencio, MD, BoulderNeurosurgical Associates, 1155 Alpine Avenue, Suite 320,Boulder, CO 80304, USA. Tel: 303-998-0004; Fax: 303-998-0007; E-mail: [email protected].
Elements of the Pre-Operative Workup, Case Examples
Alan T. Villavicencio, MD, and Sigita Burneikiene, MD
A B S T R A C T
Boulder Neurosurgical Associates, Boulder, Colorado, USA
ABSTRACT
Spinal cord stimulation (SCS) is a well-recognized method of treating a variety of chronic neuro-pathic conditions that are refractory to conservative management. One of the most challengingaspects of this technique is proper patient selection. In this study we reviewed available knowledge,differential diagnosis, and strategies utilized for the management of patients who were consideredfor a neurostimulation procedure. Clinical and neurological evaluation, complete diagnosticworkup, a behavioral assessment, and a screening trial are all essential to determine a patient’ssuitability for SCS implantation. A correct diagnosis and proper indications will help to achieveoptimal treatment results and improve quality of life for a considerable number of patients sufferingfrom intractable pain.
Key Words.
Spinal Cord Stimulation; Neuromodulation; Patient Selection; Pre-Operative Workup
pinal cord stimulation (SCS) is a well-recognized method of managing a variety of
chronic neuropathic conditions that are refractoryto conservative management. One of the mostchallenging aspects of this technique is properpatient selection. Poor patient selection is thoughtto be the main reason for many of the suboptimallong-term results reported in the 1970s [1,2].In addition to technical improvements in theimplanted hardware, improved methods of evalu-ating patient psychological problems (such as drugdependence and secondary gain issues) have led tobetter rates of long-term efficacy ranging from60% to 80% [1,3]. Indications for spinal cord neu-romodulation include peripheral deafferentationpain or chronic nonmalignant pain of neuropathicorigin [4] that is amendable to stimulation cover-age. Failed back surgery syndrome (FBSS), arach-noiditis, complex regional pain syndrome (CRPS),radiculopathy, phantom limb syndrome, andperipheral neuropathy are the most frequentlytreated conditions in the United States with thistechnique [5,6]. The underlying etiology of the
S
pain disorder should be established prior to deviceimplantation. Central deafferentation pain syn-dromes that are associated with a lesion of thecentral nervous system (e.g., stroke, spinal cordinjury) do not tend to respond as well to SCS.Patients suffering from nociceptive or somaticpain (e.g., cancer pain) that results from nerveirritation, pain in multiple sites, or pain withchanging patterns, sometimes respond better tointrathecal drug administration.
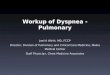
Permanent implantation of spinal cord stimula-tor leads is considered only after multidisciplinaryconservative therapies have failed and further neu-ral decompressive surgeries are not indicated. Thetreating physician should critically evaluate theunderlying diagnosis. A detailed history and com-prehensive physical examination is essential.Patients are asked to describe the nature andseverity of their pain and indicate its onset andduration. Neuropathic pain can be described usinga wide variety of terms, which include burning,constrictive, tearing, shooting, or tingling type ofpain. Individual pain evaluation remains subjec-tive. Various pain assessment tools (visual ornumeric) are used to rate pain. These include theMcGill-Melzack Pain Questionnaire (Figure 1),various pain assessment maps (Figure 2), a five-point pain scale (Figure 3), or the Visual AnalogScale (VAS) (Figure 2). Radiating pain tends to be
S36
Villavicencio and Burneikiene
Figure 1
McGill-Melzack Pain Questionnaire.

Pre-Operative Workup
S37
more effectively treated with neurostimulation asapposed to trunk, lateral, and midline pain com-ponents. Neurostimulation has had limited successin alleviating very severe excruciating pain (80–90on VAS), evoked, paroxysmal or shooting pain,and pain related to posture changes [7]. Neuro-stimulation is more effective if the disease progres-sion is static. Spatial characteristics of pain anddistribution patterns dictate the level at which theSCS lead(s) should be placed.
It is essential to correlate clinical features of thepain syndrome with the neurological status. Adetailed neurological examination is performedwith sensory and motor system assessment, payingparticular attention to the sensory system. A sen-sory examination for patients with neuropathicpain is performed to establish whether a stimulusis perceived as normal, hypoesthesia, or hyperes-thesia. Major hypoesthesia may indicate a loss oflarge-fiber dorsal column (DC) functions. Hyper-esthesia is often observed in patients sufferingfrom neuropathic pain with the typical sensation
disturbances being allodynia (painful reaction tousually nonpainful stimulus) and hyperalgesia(exaggerated pain response). These symptoms areconsidered to be diagnostic for a dysfunctionalsensory nervous system [8]. Neurostimulation ismore effective if a patient has a single unilateral ormononeuropathic—radicular pain site. In addi-tion, a motor system examination could revealweakness, apraxia, or neglect symptoms.
Neurostimulation should not be considered fora symptomatic treatment of a patient with a sur-gically treatable lesion. Likewise, candidates for
Figure 2
Pain assessment map anddiagram used in the clinic to allow forpatients to color in their symptomsonto the relevant area of their body.Also included is a visual analog scaleto allow patients to grade their pain ona scale from 0 to 10.
Figure 3
Five-point scale that allows patients to grade theirpain.

S38
Villavicencio and Burneikiene
neurostimulation should not demonstrate pro-gressive neurological dysfunction (e.g., weakness,bladder, or bowel dysfunction) related to a struc-tural lesion. Patients presenting with such symp-tomatology should be thoroughly investigated forother underlying causes of their problems.
Diagnosis of CRPS is almost exclusively basedon neurological examination and very distinctsymptoms reported by the patient. Patients oftencomplain of deep, sharp, sensitive, and/or hot paintypically located in a distal part of the upper orlower extremity accompanied by edema, sweating,and skin temperature and color changes [9]. Sen-sory symptoms also include hyperalgesia and/orallodynia on clinical examination. Motor dysfunc-tion is frequently described as weakness or adecreased range of motion. Although someauthors suggest using various diagnostic tests tomake a diagnosis such as plain radiographs, bonescintigraphy, or thermography, none of these havebeen found to be of any consistent proven value.This is with the exception of electrophysiologicstudies. Electromyography (EMG) can sometimesconfirm the presence of large-fiber peripheralnerve injury for the diagnosis of CRPS type II.Peripheral nerve conduction and EMG studiescan also be utilized to distinguish different typesof more common peripheral mono- or poly-neuropathies. As mentioned, this is especiallyuseful in assessing large-fiber DC function, as itspreservation is one of the prerequisites for induc-ing paresthesias [7].
Imaging studies are critical in identifying ana-tomic abnormalities or conditions that could becorrected surgically instead of or in addition toSCS placement (case examples 1, 2). Surgicallyamenable painful spinal deformities such as sagit-tal plane abnormalities should be ruled out, asshould spinal instability by assessing plain filmswith flexion–extension views (case examples 3, 4).Conventional magnetic resonance imaging (MRI)is usually the ideal study utilized to rule out discextrusion or sequestration, spinal canal or neuro-foraminal stenosis during preoperative screening.If spinal canal stenosis or cauda equina compres-sion is present, decompressive laminectomy orlaminoplasty is indicated, which could alleviatepain caused by a neural impingement. Percu-taneous placement of an epidural stimulationelectrode can also be more difficult and dangerousin patients with symptoms of spinal stenosis. Inpatients who clearly have neuropathic pain incombination with a structural lesion (e.g., spinalstenosis or deformity), the placement of a laminec-
tomy style electrode during the decompres-sion and/or stabilization procedure should beconsidered.
Case Example 1
A 47-year-old man presented with severe leftL4 radicular pain, numbness, and a history of pre-vious microdiscectomy at L4/L5. MRI study(Figure 4A,B) demonstrated a huge free fragmentdisc herniation at L3/4 and severe bilateral L4 andL5 root compression with severe spinal stenosis.The patient underwent left posterior microsurgi-cal L3-L4 hemilaminectomy and discectomy withremoval of the massive free fragment (Figure 4C).His symptoms completely resolved after thesurgery.
Case Example 2
A 49-year-old man presented with T9/10 radicularsymptoms, progressive paraplegia, and spasticity.MRI demonstrated a large (approximately2
×
3 cm) intradural extramedullary schwannomaat T9 with severe spinal cord compression(Figure 5A,B). The patient was taken to the oper-ating room, where he underwent a T9, T10, andpartial T11 laminectomy, and the tumor wasremoved. The intraoperative photograph demon-strates the tumor, which occupied the entire widthof the canal being removed (Figure 5C). Thepatient was seen at our clinic 2 weeks after thesurgery, and he reported that all of his previoussymptoms were resolved.
Case Example 3
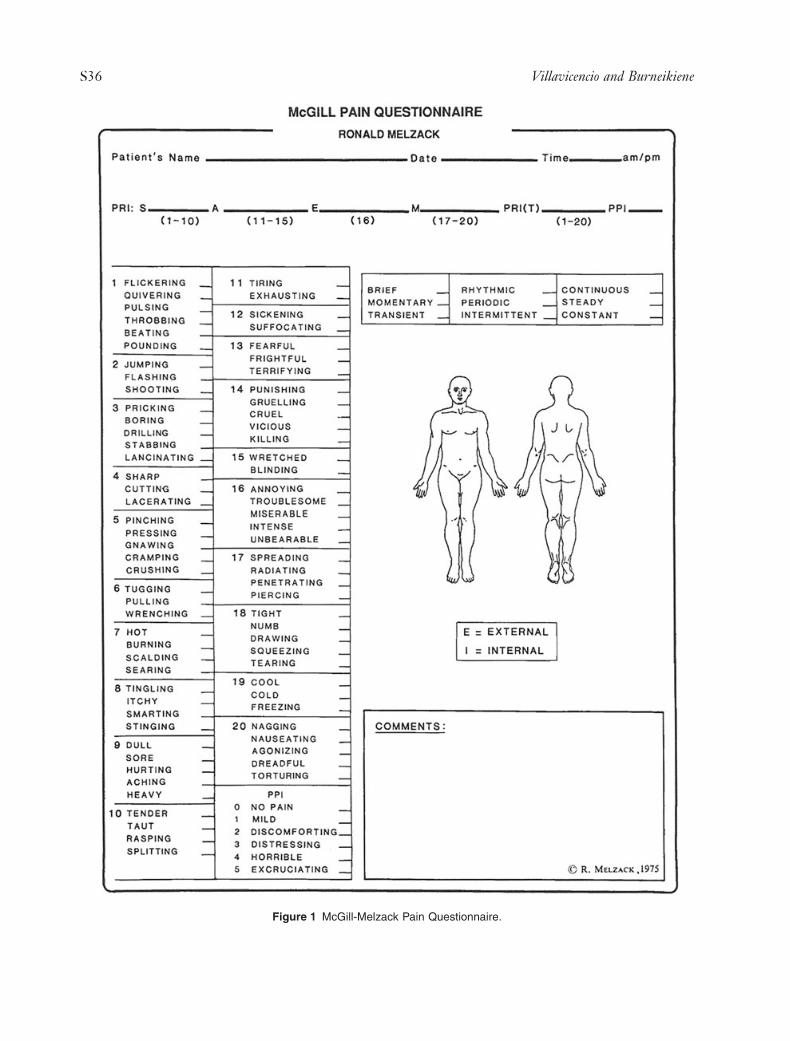
A 26-year-old man presented with a long and com-plex history of medical and surgical issues relatedto Klippel–Feil syndrome. Autofusion of all cervi-cal interspaces, except C2/3 and C4/5, wasdetected on lateral radiographs (Figure 6A) andthree-dimensional computed tomography (CT)reconstruction (Figure 6B). The patient hasundergone previous multilevel laminectomies forspinal cord stimulator lead placement with result-ant postsurgical kyphosis and chronic neck pain inaddition to his original neuropathic symptoms.There has been a progressive loss of spinal cordstimulator efficacy as a result of lead migration inassociation with a worsening structural deformity.He had a 5-year history of neck pain radiatingdown both arms and into his thoracic spine. Thepatient described his pain as “deep” and “tense”

Pre-Operative Workup
S39
and noted nocturnal numbness and tingling ofupper extremities. There was no evidence of cordcompression on the CT myelograms, but plainfilms with flexion/extension views demonstratedinstability at C4/5. The decision was made to pro-ceed with anterior cervical discectomy, fusion, andplating at C4/5 and C2 to C5 posterior fusion,instrumentation, and revision of spinal cord stim-ulator. A significant decrease in the kyphotic angu-lation was achieved (Figure 6C), the patientreported that his previous discomfort in the neckand arms improved considerably, and he reportedabout 50% pain relief at 6-month follow-up.
Case Example 4
A 47-year-old man with a history of cervical insta-bility underwent a C1-C3 fusion with sublaminarwires at another institution before he was seen atour clinic. The patient developed progressively
worsening neck pain and spastic quadriparesis inassociation with burning dysesthesias into bothupper extremities. He had been set up to undergoplacement of percutaneous spinal cord stimulatorleads by another physician. The patient was seek-ing a second opinion at our clinic and was foundto have a pseudoarthrosis with broken wires andgross spinal instability (Figure 7A,B) in associationwith multilevel spinal stenosis and cord compres-sion (Figure 7C). After undergoing a multilevelanterior posterior decompression and fusion(Figure 7D,E), his neck pain and burning dyses-thesias resolved with no change in spasticparaparesis.
Most clinicians find psychological or psychiat-ric assessment to be a valuable component forappropriate patient selection for SCS [10–13].Patients with active psychosis, major personalitydisorders, serious cognitive deficits, secondarygain issues, or serious drug/alcohol addictions are
Figure 4
Sagittal (A) and axial (B) T2-weighted magnetic resonance imagesdemonstrating free fragment disc her-niation at L3/4. Intraoperative photo-graph of removed free fragment (C).
A
C
B

S40
Villavicencio and Burneikiene
routinely screened out for nonsurgical therapies.Significant psychological issues have a strong neg-ative predictive value for outcome. Mild psycho-logical disturbances such as reactive depressionand somatization are common for this patient pop-ulation and are not necessarily contraindicationsfor implantation. However, the majority of psy-chological factors can be successfully managedwith psychological intervention, thus allowingthose patients to undergo SCS implantation.
Test Stimulation
The introduction of percutaneously placed epidu-ral electrodes allows a therapeutic trial stimulationafter longitudinal mapping of the epidural spacefor optimal electrode positioning [14]. It is fre-quently required by insurance companies that painrelief be demonstrated before a patient can beselected for permanent implantation of a stimula-
tor. Patients with a mixed pain syndrome in whomneuropathic symptoms coexist with nociceptivepain generators (e.g., tumor-related neural com-pression) may respond to either neurostimulationor intraspinal morphine administration. There-fore, performing temporary implantation in suchcases is very important. Although test stimulationhelps to exclude patients in whom the topograph-ical appropriateness of stimulation cannot beaccomplished for neuropathological or anatomicalreasons [15], it cannot be considered to be a reli-able predictor of success. In one study, only a 52–59% success rate was reported for the patientswho underwent test stimulation before permanentdevice implantation [16,17]. In this study, multi-polar systems have significantly improved clinicalreliability over unipolar systems. The use of per-cutaneous versus plate electrodes could be par-tially responsible for such suboptimal outcomes[18,19].
Figure 5
Magnetic resonance imag-ing T2-weighted image with sagittal(A) and axial (B) view demonstratinga large intradural, extramedullaryschwannoma at T9. Schwannoma,intraoperative image (C).
A
C
B
Pre-Operative Workup
S41
Tolerance of paresthesias, greater than 50%pain relief, and overall patient satisfaction shouldbe demonstrated in order for test stimulationresults to be considered positive. Other relativerequirements include improved functional level,reduced usage of pain medications, and reducedreliance on the healthcare system [2]. If trial ther-apy provides sufficient relief from pain, thepatient can be scheduled for another procedureand receive permanent implants. The authors’preferred method of trialing patients is to place alaminectomy-style lead in an awake patient undermonitored anesthesia care (MAC) anesthesia withintraoperative mapping of the coverage. Thepatient is then sent home for a week or two withan external control device. This is followed byeither removal of the leads (unsuccessful trial) orplacement of an implantable pulse generator(IPG) that gets connected to the alreadyimplanted leads that have been secured to thedura and spinous processes in order to minimizethe potential for lead migration. In the case of an
unsuccessful trial, other treatment options areexplored.
Failed Back Surgery Syndrome
Inappropriate or inadequate surgery is the mostcommon cause of FBSS [20]. Other conditionsthat can be responsible for FBSS include perma-nent neural injury, arachnoiditis, epidural fibrosis,radiculitis, microinstablity of the lumbar struc-tures, and recurrent disc herniation. Patients typ-ically complain of greater radicular discomfortthan axial back pain. Neurological evaluation maydemonstrate deficits related to a history of priorsurgery and should be correlated with the patient’scurrent complaints. Although imaging studies areoften obscured by metal hardware artifacts, theycan be helpful in establishing a diagnosis. CTmyelography with water-soluble contrast cansometimes be helpful in identifying problemsamendable to reoperation (case example 5). Ifrepeated surgery fails to adequately address a
Figure 6
Lateral (A) cervical spineplain X-ray and sagittal three-dimen-sional computed tomography recon-struction (B) demonstrating multiplefused levels consistent with diagnosisof Klippel–Feil syndrome. Intraopera-tive fluoroscopic images (C) demon-strating a significant decrease in thekyphotic angulation after the surgery.
A
C
B

S42
Villavicencio and Burneikiene
patient’s condition, SCS alone or in combinationwith reconstructive surgery should be considered(case examples 6 and 7). Contrast-enhanced MRIstudies could help to distinguish between recur-rent disc herniation and postoperative scarring.Radiographic studies (plain films with flexion/extension) are performed to rule out instability.Assessment of fusion is performed with CT usingthree-dimensional reconstruction. Provocativediscography can be performed to determinewhether anatomical abnormalities identified atcertain levels on imaging studies are clinically sig-nificant and the individual patient’s characteristicpain can be reproduced during the procedure.Unless there are clear indications, further surger-ies should be performed after very careful consid-erations. North et al. [21,22] evaluated the efficacyof reoperation versus SCS for FBSS in a prospec-tive, randomized study. The frequency of cross-over to the alternative procedure was used as anoutcome measure. They demonstrated that SCSwas more successful than reoperation, as patients
initially randomized to SCS were significantly lesslikely to crossover, and patients randomized toreoperation required increased opiate analgesicuse considerably more often than those random-ized to SCS.
Case Example 5
An 81-year-old man with a long history of lowback pain and lower extremity radicular symp-toms, who previously underwent three surgerieson his lumbar spine, was diagnosed with FBSS.Imaging studies of the lumbosacral spine demon-strated severe multilevel degenerative changeswith degenerative scoliosis. Lumbar spine mye-lography (Figure 8A,B) with CT myelogram(Figure 8C) identified a possible cause of patient’ssymptoms. Severe central neural canal stenosis wasfound at T12/L1 and moderate stenosis at L1/L2.The patient underwent T12 through S1 lumbardecompression, instrumentation, and fusion withbone morphogenetic protein. The patient has
Figure 7
Lateral cervical spine plain X-ray flexion view (A) demonstrating approximately 3 mm of anterolisthesis of C1 onC2. Extended view in the same patient demonstrates 2 mm of retrolisthesis (B). Magnetic resonance imaging (C) demon-strating moderate central canal stenosis at C4/5 and critical central canal stenosis at C5/6 with associated inflammationand cord edema, and severe central canal stenosis at C6/7. Postoperative radiographs: lateral (D) and AP (E) viewsdemonstrating posterior fusion construct with dual rods and transpedicular screws extending through C1 to C7.
A B
D E
C

Pre-Operative Workup
S43
been doing well at 1-year follow-up, and he hasbeen able to significantly decrease his use of nar-cotic pain medication.
Case Example 6
A 56-year-old patient presented with a more than15-year history of progressively worsening bilat-eral lower extremity and low back dysesthetic neu-ropathic pain. Five years ago, he underwent an L4-S1 decompression with posterior instrumentationand fusion procedure to alleviate his symptoms.Unfortunately, the patient reported no significantrelief. Subsequent conservative therapies consist-ing of physical therapy, various epidural and nerveroot injections, and medications provided no sus-tained benefit. He was diagnosed with FBSS, dor-sal nerve root injury at L5, and since that time wasgradually increasing his narcotic pain medications.
The patient was undergoing preoperative eval-uation for a neurostimulation device implantation.He described his back pain as constant achingthat is exacerbated with certain types of motion.Plain radiographs were performed with flexion–extension views, then a broken sacral screw andpseudoarthrosis at L5/S1 (Figure 9A,B) with amoderate level of instability were found. In addi-tion, his bilateral lower extremity discomfort wasvery constant and described as “jabs of electricalpain and walking on bare bones” with radiationtoward his ankles and calves. MRI studies demon-strated no central canal or nerve root impinge-
ment (Figure 9C). Neurological examinationrevealed weakness in his left foot and decreasedsensation to pinprick below the knee bilaterallywith bilateral patchy areas of hyperpathia in theL5 distribution.
The patient was felt to have neuropathic painas a result of multilevel root stretch injuries andunderwent a combined redo instrumentation andfusion with individually placed root stimulators(Figure 9D,E). At 6-month follow-up, the patientreported that the previous pain in his back andlower extremities decreased by 80%, and he wasable to significantly decrease his pain medications.
Case Example 7
A 79-year-old woman underwent a series of backsurgeries (laminectomy in 2001, fusion in 2002,and redo fusion in 2003) to treat her low back pain.She developed chronic debilitating low back painand right lower extremity radicular symptoms andrequired complete assistance with her daily living.Physical therapy, functional rehabilitation, anti-inflammatory agents, and narcotic medicationsfailed to provide relief. She was unable to stand formore than a minute and could not walk. Her painbecame exacerbated with standing and any type ofmotion and was described as a burning and stab-bing discomfort located in her lower back, groin,anterior thigh, and right leg. She had kyphoticspinal deformity with intense paraspinal musclespasm. Neurological examination revealed three
Figure 8
AP (A) and lateral (B) plain film myelography with confirmatory computed tomography myelography (C) demon-strating severe (T12/L1) and moderate (L1/L2) central neural canal stenosis.
A CB

S44
Villavicencio and Burneikiene
out of five motor strength in the right iliopsoasand quadriceps, and hypersensitivity in the rightL2 distribution with decrease reflexes.
A CT myelogram demonstrated extensive post-operative changes of L3/L5 laminectomy and pos-terior fusion with no signs of central or foraminalstenosis. Overall good positioning of the hardwarewas found with the exception of the right L2pedicle screw, which appeared to be violating thepedicle and irritating the nerve root.
The patient subsequently underwent removalof the right L2 pedicle screw and a portion of therod. She felt initial relief of her symptoms,improved overall mobility as well as the functionalcapacity in her leg, but unfortunately, her symp-toms slowly began to return within 6 months.
Electromyography and nerve conduction stud-ies demonstrated L4 radiculopathy. An L4 trans-foraminal epidural steroid injection wasperformed, which had no effect on her symptoms.
SCS therapy was then considered. Patient under-went extensive psychological evaluation, andalthough it revealed mild symptoms of depression,it was determined that she was an appropriate can-didate for test stimulation implantation. SCS trialimplantation (Figure 10) demonstrated good par-esthesia coverage with about 50% pain reductionin her right lower extremity. It was decided toproceed with permanent device implantation. At6-month follow-up, the patient reported that herdiscomfort in the right thigh and leg remainedreduced by about 50%, and she was able to returnto a more active life style.
Conclusions
Clinical and neurological evaluation, completediagnostic workup, behavioral assessment, and ascreening trial are all essential to determine apatient’s suitability for SCS implantation. A cor-
Figure 9
AP (A) and lateral (B) plain films demonstrating a previous L4-S1 instrumented fusion with pseudoarthrosis atL5/S1 and broken right S1 screw. Magnetic resonance imaging demonstrating no central canal or nerve root impingement(C). Intraoperative fluoroscopic images, lateral (D) and AP (E) with individually placed root stimulators.
A B
D E
C

Pre-Operative Workup
S45
rect diagnosis and appropriate indications willhelp to achieve optimal treatment results andimprove quality of life for a considerable numberof patients suffering from intractable pain.
References
1 Cameron T. Safety and efficacy of spinal cord stim-ulation for the treatment of chronic pain: A 20-yearliterature review. J Neurosurg 2004;100(3 supplSpine):254–67.
2 Windsor RE, Falco FJ, Pinzon EG. Spinal cordstimulation in chronic pain. In: Lennard TE, ed.Pain Procedures in Clinical Practice, 2nd edition.Philadelphia, PA: Hanley & Belfus; 2000:377–94.
3 Krames E. Implantable devices for pain control:Spinal cord stimulation and intrathecal therapies.Best Pract Res Clin Anaesthesiol 2002;16(4):619–49.
4 Simpson BA. Spinal cord stimulation in 60 cases ofintractable pain. J Neurol Neurosurg Psychiatry1991;54(3):196–9.
5 Alo KM, Holsheimer J. New trends in neuromodu-lation for the management of neuropathic pain.Neurosurgery 2002;50(4):690–703; discussion 703–4.
6 Lang P. The treatment of chronic pain by epiduralspinal cord stimulation—A 15 year follow up;present status. Axone 1997;18(4):71–3.
7 Meyerson BA, Linderoth B. Spinal cord stimulation.In: Loeser JD, ed. Bonica’s Management of Pain.Philadelphia, PA: Lippincott Williams & Wilkins;2001:1856–76.
8 Backonja MM. Painful neuropathies. In: Loeser JD,ed. Bonica’s Management of Pain, 3rd edition. Phil-adelphia, PA: Lippincott Williams & Wilkins;2001:371–88.
9 Galer BS, Jensen MP. Development and prelimi-nary validation of a pain measure specific to neuro-pathic pain: The Neuropathic Pain Scale.Neurology 1997;48(2):332–8.
10 Block AR, Ohnmeiss DD, Guyer RD, RashbaumRF, Hochschuler SH. The use of presurgical psy-chological screening to predict the outcome of spinesurgery. Spine J 2001;1(4):274–82.
11 Burchiel KJ, Anderson VC, Wilson BJ, et al. Prog-nostic factors of spinal cord stimulation for chronicback and leg pain. Neurosurgery 1995;36(6):1101–10; discussion 1110–1.
12 Kupers RC, Van den Oever R, Van Houdenhove B,et al. Spinal cord stimulation in Belgium: A nation-wide survey on the incidence, indications andtherapeutic efficacy by the health insurer. Pain1994;56(2):211–6.
13 North RB, Kidd DH, Wimberly RL, Edwin D.Prognostic value of psychological testing in patientsundergoing spinal cord stimulation: A prospectivestudy. Neurosurgery 1996;39(2):301–10; discussion310–1.
14 North R. Spinal cord stimulation for the failedback surgery syndrome. In: Gildenberg PL, TaskerR, eds. Textbook of Stereotactic and FunctionalNeurosurgery. New York: McGraw-Hill;1998:1611–20.
15 Simpson BA. Selection of patients and assessmentof outcome. In: Simpson BA, ed. Electrical Stimu-lation and the Relief of Pain, Vol. 15. Elsevier:Pain Research and Clinical Management;2003:237–49.
16 North RB, Kidd DH, Zahurak M, James CS, LongDM. Spinal cord stimulation for chronic, intractablepain: Experience over two decades. Neurosurgery1993;32(3):384–94; discussion 394–5.
17 Kumar K, Toth C, Nath RK, Laing P. Epiduralspinal cord stimulation for treatment of chronicpain—Some predictors of success. A 15-year expe-rience. Surg Neurol 1998;50(2):110–20; discussion120–1.
18 Villavicencio AT, Leveque JC, Rubin L, Bulsara K,Gorecki JP. Laminectomy versus percutaneouselectrode placement for spinal cord stimulation.Neurosurgery 2000;46(2):399–405; discussion 405–6.
19 North RB, Kidd DH, Petrucci L, Dorsi MJ. Spinalcord stimulation electrode design: A prospective,randomized, controlled trial comparing percutane-ous with laminectomy electrodes: Part II—Clinicaloutcome. Neurosurgery 2005;57(5):990–6.
Figure 10
Intraoperative fluoroscopic image, trial spinalcord stimulation placement.

S46
Villavicencio and Burneikiene
20 North RB, Campbell JN, James CS, et al. Failedback surgery syndrome: 5-year follow-up in 102patients undergoing repeated operation. Neurosur-gery 1991;28(5):685–90; discussion 690–1.
21 North RB, Kidd DH, Farrokhi F, Piantadosi SA.Spinal cord stimulation versus repeated lumbosacralspine surgery for chronic pain: A randomized, con-
trolled trial. Neurosurgery 2005;56(1):98–106;discussion 106–7.
22 North RB, Kidd DH, Piantadosi S. Spinal cordstimulation versus reoperation for failed back sur-gery syndrome: A prospective, randomized studydesign. Acta Neurochir Suppl 1995;64:106–8.