Embed Size (px)
DESCRIPTION
Stable Angina: The best timing of coronary angiography and the role of further investigations on myocardial ischemia still need to be defined. Eliano Pio Navarese, MD, PhD Nicolaus Copernicus University, Poland SIRIO MEDICINE network. Very Early vs delayed PCI in NSTE-ACS. Background. - PowerPoint PPT Presentation
Citation preview

Stable Angina: The best Stable Angina: The best timing of coronary timing of coronary
angiography and the role angiography and the role of further investigations of further investigations onon myocardial ischemia myocardial ischemia still need to be defined still need to be defined
Eliano Pio Navarese, MD, PhDNicolaus Copernicus University, Poland
SIRIO MEDICINE network

Very Early vs delayed PCI in
NSTE-ACS
Navarese, Ann Intern Med 2013
In NSTE-ACS the superiority of coronary angiography/PCI vs a conservative medical treatment has been shown.
In NSTE-ACS a very early invasive approach (≤ 24 hours) is not proven to be superior to an delayed approach (>24 hour).
Trials showed no advantage of coronary angiography/PCI
vs medical therapy in stable
coronary artery disease (CAD).
Which is the best timing of angiography in stable CAD?
Background

PCI vs medical therapy Stepwise diagnostic approach to CAD

Guidelines require a Bayesian approach to diagnosis, which uses the results of diagnostic tests along with clinicians’ initial estimates of the disease, termed pre-test probability (PTP).
ESC guidelines, EHJ 2013

ESC guidelines, EHJ 2013

ESC guidelines, EHJ 2013

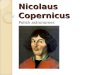
COURAGE trial: COURAGE trial: Survival Free of Death from Any Cause and Myocardial Infarction
Number at RiskMedical Therapy 1138 1017 959 834 638 408 192 30PCI 1149 1013 952 833 637 417 200 35
Years0 1 2 3 4 5 6
0.0
0.5
0.6
0.7
0.8
0.9
1.0
PCI + OMT
Optimal Medical Therapy (OMT)
Hazard ratio: 1.0595% CI (0.87-1.27)P = 0.62
7
Boden, et al. N Engl J Med 2007

Bangalore, Circulation 2012

Issues of the Courage trial
1) Selection bias (randomization after cardiac catheterization)
2) No sufficient threshold for ischemia (lower risk)
3) No use of contemporary techniques such as FFR and minimal use of DES
Rossini, Am J Cardiovasc Dis. 2013

Hachamovitch et al. Circ 1998;
Card
iac
Death
Rate
(%
)
0% 1-5% 5-10% 11-20% >20%*p < 0.0001 % Total Myocardium Ischemic†10,627 Consecutive patients followed 1.9 + 0.6 years.
*
§

Primary endpoint: % with ischemia reduction ≥ 5% myocardium (N=314)
19.8%
p=0.00433.3%
Isch
em
ia r
ed
ucti
on
≥ 5
%
COURAGE nuclear substudy IICOURAGE nuclear substudy II

FFR-guided
30 days2.9% 90 days
3.8% 180 days4.9% 360 days
5.3%
Angio-guided
absolute difference in MACE-free survival
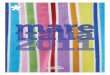
FAME study: Event-free Survival FAME study: Event-free Survival

FAME 2 : FFR-Guided PCI versus Medical Therapy in FAME 2 : FFR-Guided PCI versus Medical Therapy in Stable CADStable CAD
Primary Outcomes
0
5
10
15
20
25
30
Cu
mu
lati
ve in
cid
en
ce (
%)
166 156 145 133 117 106 93 74 64 52 41 25 13Registry447 414 388 351 308 277 243 212 175 155 117 92 53PCI+MT441 414 370 322 283 253 220 192 162 127 100 70 37MT
No. at risk
0 1 2 3 4 5 6 7 8 9 10 11 12Months after randomization
MT vs. Registry: HR 4.32 (1.75-10.7); p<0.001PCI+MT vs. Registry: HR 1.29 (0.49-3.39); p=0.61PCI+MT vs. MT: HR 0.32 (0.19-0.53); p<0.001

Weintraub N Engl J Med 2008.
PCI and Relief of Angina

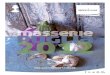
Event risk stratification

ESC guidelines, EHJ 2013

Granillo, EHJ 2013

ClinicalTrials.gov Identifier: NCT01471522

Optimal Timing = Optimal Patient
Navarese et al. unpublished

“Unicuique suum”?
Grazie!