Embed Size (px)
Citation preview

ELSAThe European Lacidipine Study on Atherosclerosis
Principal Results

Relationship of hypertension and atherosclerosis
Hypertension
Increased turbulent flow(particularly at
bifurcation points)
Increased risk of atherosclerotic
lesions
Mechanical stress of high blood pressure
Endothelial damage
Increased permeability for lipids and free radicals
Release of vasoconstrictive
factors (endothelin)
Zanchetti, 1992
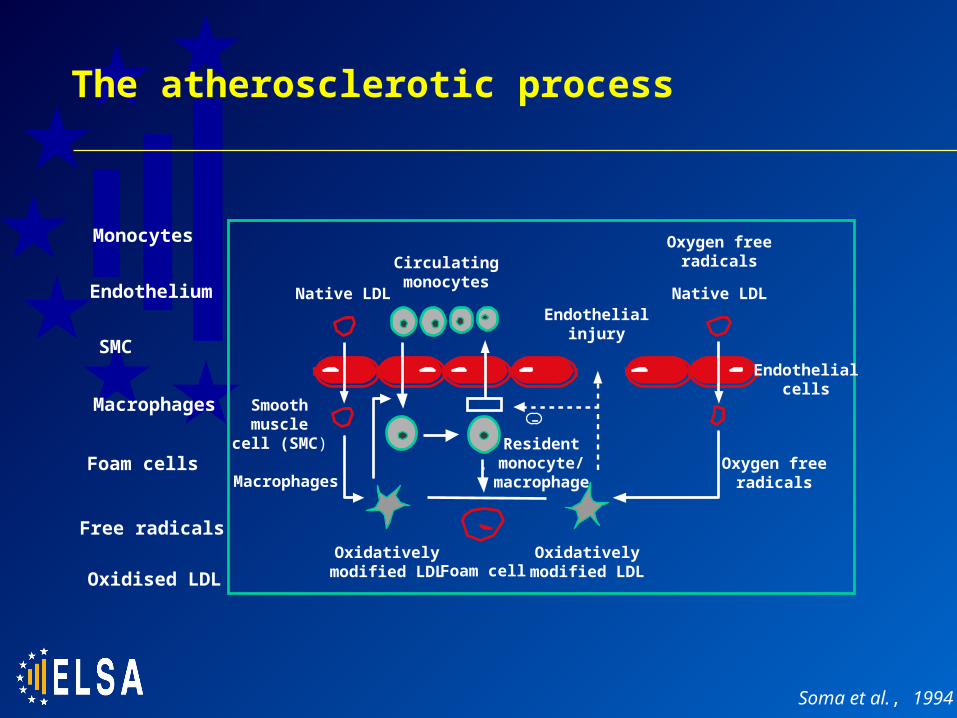
The atherosclerotic process
Monocytes
Endothelium
SMC
Macrophages
Foam cells
Free radicals
Oxidised LDL
-
Circulatingmonocytes
Native LDLEndothelial
injury
Oxygen freeradicals
Native LDL
Smoothmuscle
cell (SMC)
Macrophages
Residentmonocyte/
macrophage
Endothelialcells
Oxygen freeradicals
Oxidativelymodified LDL Foam cell
Oxidativelymodified LDL
Soma et al., 1994

Lacidipine: Dual action against atherosclerotic processes
Macrophage activation/foam cell formation
Oxidation ofLDL cholesterol
Vascular smooth muscle cell migration
Thrombocyte aggregation
Calciumantagonist
Antioxidant
Gaviraghi et al., 1998

Antiatherosclerotic properties of lacidipine: Pre-clinical data (1)
• The antiatherosclerotic activity of lacidipine has been extensively documented in pre-clinical studies, often at non-antihypertensive doses: Lacidipine (0.3, 1.0 and 10 mg/kg/day) completely prevented
arteriolar irregularities in the retina vessel of hypertensive Dahl-S rats; the highest dose was also antihypertensive1
Lacidipine (3 mg/kg/day) reduced carotid intima/media hyperplasia (induced by cuff injury) by approximately 50% in hypercholesterolaemic rabbits2
Lacidipine (0.3 mg/kg/day p.o.) inhibited fatty streak formation in hypercholesterolaemic Golden Syrian hamsters3
Lacidipine inhibited metalloproteinase-9 secretion by human macrophages in culture, an effect expected to stabilise atherosclerotic plaques in vivo4
1Cristofori et al., 1991; 2Soma et al.,1994; 3Cristofori et al., 2000; 4Bellosta et al., 2001

Lacidipine protects stroke-prone hypertensive rats against the impairment of endothelium-dependent vasodilation evoked by a salt-rich diet1
Lacidipine was the most effective of three dihydropyridines in reducing the expression of the endothelial cell adhesion molecules, ICAM-1, VCAM-1 and E-selectin, in response to TNF- stimulation2
Lacidipine (3.0 mg/kg/day) reduced atherosclerotic lesions in the aorta of transgenic apo-E-deficient mice by 50%3
Antiatherosclerotic properties of lacidipine: Pre-clinical data (2)
1Krenek et al., 2001; 2Cominacini et al., 1999; 3Cristofori et al., 2000

Potential antioxidant effects of lacidipine on endothelial function of hypertensive patients
• Several experiments suggest that endothelial dysfunction and reduced nitric oxide (NO)-dependent vasodilation play a key role in atherogenesis
• Essential hypertension reduces responsiveness to endothelium-dependent vasodilators and the suppression of vasodilation by NO synthesis inhibitors
• Lacidipine (4–6 mg/day) but not atenolol (50–100 mg/day) increased endothelium-dependent vasodilation and restored the response to NO synthesis inhibitors
• Markers of oxidative stress, including LDL hydroperoxidases and reactive oxygen species were also reduced by lacidipine
• The antioxidant activity of lacidipine may be a key factor in restoring NO availability and increasing endothelium-dependent vasodilation
Taddei et al., 2001

monocyte
damaged endothelium
macrophage foamcell
lipid
thrombocytes
plaque
oxidative stress
1
2
3
smooth muscle cells 4
5
Gaviraghi et al., 1998
Lacidipine: Summary of potential antiatherosclerotic mechanisms

ELSA: Inclusion and exclusion criteria
• Major inclusion criteria Aged 45–75 years Systolic and diastolic blood pressure of 150–210 mmHg and
95–115 mmHg, respectively Readable ultrasound carotid artery scan with maximum
intima-media thickness (IMT) < 4.0 mm
• Major exclusion criteria Fasting serum cholesterol > 320 mg/dL Insulin-dependent diabetes mellitus Myocardial infarction (within previous 12 months) Stroke (within previous 6 months) Previous carotid endarterectomy

Study design
0 1 2 3
Run-in Titration Maintenance
-1 0 1 3
4 5 6 7 8 9 10 11 Follow up
6 12 18 24 30 36 42 48 5–9 days
25mg
12.5mgHCTZ (if required)
6mg
4mg
50mg
100mg
12.5mg25mg
PlaceboAtenolol
Lacidipine
HCTZ (if required)
Clinical examination
Months
Visits
Medication
Measurements
Blood pressure
Trial phases
B-mode ultrasound & arterial blood pressure monitoring
Zanchetti, 1996

Zanchetti et al., 1998
Measurement of IMT and CBMmax
• The primary endpoint for IMT measurement in the ELSA trial is CBMmax. This is defined as the mean of the maximum IMT of the four far walls of the carotid bifurcation and distal common carotid artery
Externalcarotid
Commoncarotid
Bifurcation
Internalcarotid
Internal
Common
Thickening: 1.0, <1.3 mm
Plaque: 1.3 mm
Normal: <1.0 mm
Stratification Location

Advantages over other studies
• Large scale gives ELSA statistical power to detect small but clinically significant changes
• Standardisation of techniques for highly reproducible data
• Rigorous quality control for reliable quantification
1Zanchetti et al., 1998; 2Borhani et al., 1996; 3Mancini et al., 2000
ELSA1
MIDAS2
VHAS1
PREVENT3
Number of patients0 500 1000 1500 2000 2500

Study endpoints
• Primary objective Comparison of effects of lacidipine and atenolol on carotid IMT
• Primary efficacy outcome Change in CBMmax
• Secondary objective Comparison of the effects of lacidipine and atenolol on:
cardiovascular events blood pressure control progression/regression of atherosclerotic plaques
• Secondary efficacy outcomes Percentage of patients with increased/decreased number of carotid
plaques Incidence of fatal/non-fatal ‘major’ and ‘minor’ cardiovascular events,
and total mortality Change in mean maximum IMT (Mmax)

Patient populations
• Safety, N = 2,334All patients randomised and receiving at least one dose of DB treatment
• Intention to treat (ITT), N = 2,035Patients from the safety population having at least one baseline and one subsequent readable scan
• Per-Protocol 1 (PP1), N = 1,884Patients from the ITT population with no major protocol violations
• Per-Protocol 2 (PP2), N = 1,807Patients from the ITT population with no major protocol violations and with at least one scan after baseline taken under active treatment
• Completers, N = 1,519All PP patients having completed the 4-year DB treatment period

Baseline characteristics
Age (years)
Serum LDL-cholesterol (mmol/l)
Gender (% males)
Serum triglycerides (mmol/l)
Current smoking (%)
Clinic SBP (mmHg)
Body mass index (kg/m2)
CBMmax (mm)
IMT-common carotid (mm)
IMT-carotid bifurcation (mm)
Lacidipine AtenololVariable55.9 ± 7.5
3.73 ± 0.98
55.4
1.51 ± 0.77
18.4
163.1 ± 12.5
27.2 ± 3.6
1.1619 ± 0.2480
1.0173 ± 0.2152
1.3115 ± 0.3782
56.1 ± 7.5
3.70 ± 0.94
54.2
1.51 ± 0.71
22.6
163.9 ± 12.2
27.2 ± 3.9
1.1589 ± 0.2399
1.0090 ± 0.1980
1.3131 ± 0.3594
24-h ambulatory DBP (mmHg) 87.6 ± 9.388.2 ± 9.3
Total cholesterol (mmol/L)) 5.84 ± 1.015.80 ± 0.98
Clinic DBP (mmHg) 101.3 ± 4.9101.4 ± 5.3
Serum HDL-cholesterol (mmol/l) 1.34 ± 0.461.34 ± 0.43
24-h ambulatory SBP (mmHg) 140.4 ± 14.2141.4 ± 14.0

CBMmax progression – repeated measurements model
Atenolol
Estimated treatment effect (mm):
Lacidipine vs. atenolol
95% Confidence interval
ITT Completers
1006
PP1 PP2
926 901 764
Lacidipine 1022 942 906 765
-0.0227 -0.0276 -0.0293 -0.0281
-0.0330 -0.0381 -0.0399 -0.0394
-0.0124 -0.0171 -0.0187 -0.0167
Patient number:
Statistics (P) < 0.0001 < 0.0001 < 0.0001 < 0.0001

Treatment-related changes:Carotid wall CBMmax
CBMmax: Final vs. baseline scan
Ratio of mean changes (95% CI)
0.02
0.01
0
Mea
n c
han
ge
(mm
/yea
r)
0.06
0.05
0.04
0.03
ITT PP1 PP2 Completers
0.2 0.4 0.6 0.8 1 1.2 1.4
In favour of lacidipine In favour of atenolol
Lacidipine
Atenolol
ITTPP1
PP2
Completers

Treatment-related changes: Common carotid and carotid bifurcation IMT
ITT
PP1
PP2
Completers
Mmax changes in common carotid (CC) and carotid bifurcation (CB) with lacidipine compared with atenolol (repeated measurements model)
CCCB
-0.05 -0.04 -0.03 -0.02 -0.01 0 +0.01
P-values
Treatment Time Baseline Mmax
< 0.0001 < 0.0001 < 0.0001
< 0.0001
< 0.0001
< 0.0001 < 0.0001 < 0.0001
< 0.0001
< 0.0001
< 0.0001 < 0.0001 < 0.0001
< 0.0001 < 0.0001 < 0.0001
< 0.0001 < 0.0001
< 0.0001 < 0.0001
= 0.0085
= 0.0015
= 0.0004
= 0.0013
CCCB
CCCB
CCCB
Estimated lacidipine effect (mm)
Lacidipine better Atenolol better

Treatment-related changes: Carotid plaque prevalence
Changes in number of carotid plaques per patient from baseline to end of study with lacidipine and atenolol
Atenolol (N = 937)
Lacidipine (N = 947)
1
3
20
18
123
170
515
525
220
194
50
34
8
3
144
191
515
525
278
231
Lacidipine
Atenolol
Change in number of plaques
-3 -2 -1 0 +1 +2 +3 Less No change
More
% o
f p
atie
nts
60
50
40
30
20
10
0

Treatment-related changes:Blood pressure and heart rate
-12
-10
-8
-6
-4
-2
0
b/min
SBP DBP HR
-24
-20
-16
-12
-8
-4
0
mmHg
SBP DBP HR
-24
-20
-16
-12
-8
-4
0
mmHg
-12
-10
-8
-6
-4
-2
0
b/min
Blood pressure (SBP, DBP) and heart rate (HR) changes during randomised treatment (ITT)
Clinic values 24 h Ambulatory values
LacidipineAtenolol

Safety analysis
Myocardial infarction
Relative risk of adverse events in lacidipine- and atenolol-treated patients
Stroke
All death
Hospitalised angina
Other minor CV events
All serious AEs
Events (N)
LacidipineAtenolol
17
14
33
17
11
30
Major CV events
CV death 8
201
18
9
27
4
13
17
27
186
Lacidipine better Atenolol better
1.0
Relative risk (95% CI)
0.1 0.2 0.3 0.5 2.0 4.0

Confirmation of the antiatherosclerotic action of lacidipine
• The ELSA study provides conclusive evidence of the antiatherosclerotic activity of lacidipine
• Lacidipine was more effective than atenolol in slowing progression of carotid wall IMT
• Key features of ELSA that allowed these conclusions included: Measurement techniques Large study size Standardisation of protocol Rigorous quality control

ELSA in the context of previous studies
MIDAS1, VHAS2 and INSIGHT-IMT3
Intervention studies in hypertension All compared the effects of a calcium antagonist and diuretic on carotid IMT All found reductions in IMT with the calcium antagonist similar to those seen with
lacidipine in ELSA Results not as conclusive as in ELSA, because of the limited size of these
studies and the measurement methodology (readings not blind for time-sequence, and IMT measurements limited to the CC)
PREVENT4, BCAPS5 and SECURE6
Placebo-controlled studies in patients with vascular disease All found reductions in CBMmax with antihypertensive therapy
BCAPS demonstrated a reduction in carotid progression with metoprolol,5 suggesting that -blockers also may have a protective effect in preventing atherosclerosis and that the lacidipine effects in ELSA may be over and above those seen with atenolol
1Borhani et al., 1996; 2Zanchetti et al., 1998; 3Simon et al., 2001; 4Pitt et al., 2000; 5Hedblad et al., 2001; 6Lonn et al., 2001

Key findings from the ELSA study
• Compared with atenolol, lacidipine is significantly (P < 0.001) more effective in slowing increases in carotid IMT in hypertensive patients:
• reduced 4-year CBMmax progression by
0.0227 mm (ITT population) 0.0281 mm (Completers population)
• reduced yearly carotid IMT progression rate by 23–40% (40–60% in Completers and PP2)
• increased the proportion of patients with regression of pre-existing plaques by 31%

Implications of the ELSA results
• Lacidipine has a greater effect than atenolol in preventing alterations in the carotid wall, despite having a smaller effect on ambulatory blood pressure
• The greater reduction in IMT at the carotid bifurcation over the common carotid supports the antiatherosclerotic activity of lacidipine
• The ELSA results are consistent with the pre-clinical evidence indicating that lacidipine inhibits atherosclerosis at doses insufficient to lower blood pressure
• Therefore, the antiatherosclerotic action of lacidipine appears to be independent of its antihypertensive effects

Clinical significance of the ELSA results
1Hodis et al., 1998; 2Salonen & Salonen, 1993; 3Bots et al., 1997; 4Chambless et al., 2000
• The risk of coronary events or stroke increases progressively with increasing carotid IMT1–4;
• The presence of carotid plaques increases the 5-year risk of myocardial infarction three-fold1;
• The reduction in CBMmax progression seen with lacidipine in the ELSA : 0.009 mm/year difference vs atenolol 40–60% reduction of progression vs atenolol
could reduce the risk of cardiovascular events in the longer term. Increases in IMT progression rate in the same range of those observed with atenolol in ELSA compared to lacidipine have in fact been associated with a 60% greater risk of
myocardial infarction and coronary death1

The ELSA study:Summary
• 4-year, multi-centre study• Largest study of treatment effects on carotid IMT
to date• Careful design and implementation for highly
reliable results• Clear demonstration of benefits of lacidipine over
atenolol in slowing the progression of carotid IMT• Clinically significant treatment effect on IMT• Verifies pre-clinical evidence of antiatherosclerotic
properties of lacidipine• Supports antiatherosclerotic actions of lacidipine
independent of antihypertensive effects