Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Eltrombopag therapy in newly diagnosed steroid non-responsiveITP patients
Anil Kumar Tripathi • Ayush Shukla •
Sanjay Mishra • Yogendra Singh Yadav •
Deependra Kumar Yadav
Received: 30 October 2013 / Revised: 22 January 2014 / Accepted: 29 January 2014
� The Japanese Society of Hematology 2014
Abstract Primary immune thrombocytopenia (ITP) is an
autoimmune disorder characterised by isolated thrombo-
cytopenia (peripheral blood platelet count \100 9 109/L)
in the absence of other causes or disorders that may be
associated with thrombocytopenia. The upfront treatment
in newly diagnosed ITP patients is steroids; however, about
one-third patients do not respond, and require other treat-
ment, including IVIg, anti-D, or splenectomy. Previous
studies have shown decreased platelet production in some
ITP patients, aside from the evidence of enhanced platelet
destruction. Thrombopoietin receptor agonists (TPO-RA),
such as eltrombopag have been shown to provide good
response in steroid non-responsive chronic ITP patients.
We have studied response to eltrombopag in 25 newly
diagnosed steroid non-responsive ITP patients; 80 %
patients showed response at the end of 1 month, and 76 %
sustained response at the end of 3 months. The platelet
count rose from a mean value of 17.5 ± 3.6–152.5 ±
107.9 9 109/L at the end of 1 month. Our results suggest a
possible role of eltrombopag in newly diagnosed steroid
non-responsive ITP patients. However, our study is limited
in that it is a single-centre study, with a small sample size,
and lacks a long-term safety profile. Our findings highlight
the potential value of a larger prospective study on the
upfront use of TPO-RA in patients of ITP.
Keywords Primary ITP � ITP � TPO-RA � Eltrombopag
Introduction
Primary immune thrombocytopenia (ITP) is an autoim-
mune disorder characterised by isolated thrombocytopenia
(peripheral blood platelet count \100 9 109/L) in the
absence of other causes or disorders that may be associated
with thrombocytopenia [1]. The diagnosis of ITP remains
one of exclusion; no robust clinical or laboratory parame-
ters are currently available to establish its diagnosis with
accuracy. The main clinical problem of ITP is an increased
risk of bleeding, although bleeding symptoms may not
always be present. ITP is said to be ‘‘newly diagnosed’’ if
time of presentation from the diagnosis is within 3 months
and chronic if lasting for more than 12 months [1].
The disease is characterised by enhanced destruction of
antibody-coated platelets in the reticuloendothelial system.
In some patients, there is also an evidence of immune-
mediated megakaryocytic suppression/injury [2]. The main
aim of the treatment is to avoid bleeding by augmenting the
low platelet counts that may have caused bleeding.
As there is no consensus for etiology, similar is the
situation with treatment. Treatment strategies have focus-
sed on limiting the accelerated platelet destruction. Steroid
is the initial treatment choice but 1/3 patients do not
respond or need intolerable, larger doses [3]. The mecha-
nism by which steroid acts is not very clear, however, it is
supposed to be through its immunosuppressant effect on T
cells. In patients not responding to steroids, various treat-
ment options are splenectomy, anti-D, IV immunoglobulin,
Rituximab, danazol, vincristine, etc. [3].
Thrombopoietin receptor agonists (TPO-RA: oral el-
trombopag, subcutaneous romiplostim) have been tried in
patients with ITP on the basis that there is megakaryocytic
suppression/injury in some, if not all, patients of ITP.
Previous studies have shown that eltrombopag increases
A. K. Tripathi � A. Shukla (&) � S. Mishra �Y. S. Yadav � D. K. Yadav
Department of Clinical Hematology and Medical Oncology,
King George’s Medical University, Lucknow 226003,
U.P., India
e-mail: [email protected]
123
Int J Hematol
DOI 10.1007/s12185-014-1533-y

the platelet counts significantly in patients of chronic ITP
and reduces the morbidity and mortality associated with the
disease [4]. These studies have focussed on the role of
TPO-RA in patients of chronic ITP who failed steroid
therapy or other first-line treatment. However, there is a
paucity of published research work on the role of TPO-RA
in newly diagnosed (time of diagnosis within 3 months)
ITP patients who have failed steroid therapy. We hereby
prospectively studied the response to eltrombopag in newly
diagnosed ITP patients non-responsive to steroid and
sought to know the durability of response on TPO-RA.
Methods
This prospective cohort study comprised 27 patients of
primary ITP from the hematology clinic who fulfilled the
inclusion criteria such as:
1. ‘‘Newly diagnosed ITP’’ (time from diagnosis within
3 months).
2. Non-responsive to steroid at 2 weeks.
3. Could not opt for IVIg, anti-D or splenectomy as
further treatment.
The study was approved by the institutional ethical
committee and all patients had given a written informed
consent before enrolment. Non-responsiveness to steroid
was defined according to international working group
consensus [1].
Cases of ITP associated with secondary causes like HIV,
SLE, H. pylori, other cancer and pregnancy were excluded
from the study.
Cases underwent detailed clinical history, physical
examination and investigations. A complete hemogram
with thorough peripheral blood smear examination and
tests to exclude secondary causes of ITP including viral
profile (HIV, HBsAg, HCV), H. pylori, anti-thyroid, and
ANA and APLA were done.
Patients of newly diagnosed ITP who did not respond to
steroid therapy were given eltrombopag. Initial dose was
50 mg/day for 1 month which was tapered to 25 mg/day if
platelet count was sustained [150 9 109/L for a week.
Steroid was tapered in 2 weeks after eltrombopag was
started. Platelet count was done biweekly for first month,
and then monthly for 3 months. Decision to stop therapy
was taken if counts rose above 250 9 109/L in order to
reduce the thrombocytosis-associated risk. If there was no
response at 1 month or anytime later, patients were offered
choice of other modalities like splenectomy, anti-CD 20,
etc.
The primary end point was defined as a response to
eltrombopag that is platelet count more than 50 9 109/L at
the end of 1 and 3 months of treatment. The secondary end
points included safety and tolerability, affordability and
signs of bleeding. The incidence and severity of bleeding
were assessed at every visit according to WHO bleeding
scale.
The patients were followed fortnightly. The clinical
course including symptoms and side effects was recorded
on a regular follow-up.
Results
Out of newly diagnosed ITP patients (time from diagnosis
within 3 months) attending OPD/IPD clinics, only those
(n = 27) patients were included in the present study who
did not respond to steroid. Two patients were lost during
follow-up and there results are not included. The mean age
of patients (n = 25) was 27 ± 8.63 years. All patients
were 15 years old or above (range 15–55 years). Males
constituted 40 % (10/25) of the study population. The
mean platelet count at presentation was 13.7 ± 5.2 9 109/
L, median 12 9 109/L and the range was 20 9 109/L.
Clinical features included petechiae and purpura in 68 %,
ecchymosis in 40 % and mucosal bleeding in 60 % of
patients. All patients were newly diagnosed (time from
diagnosis within 3 months) cases of primary ITP and were
treatment-naive. All patients were treated in outpatient
clinic or day care centre. Indications for treatment were
bleeding in 76 %, platelet count B10 9 109/L in 8 %, and
both features in 16 %.
Patients who were included in the study had already
received prednisolone at a dose of 2 mg/kg/day for
2 weeks did not show response nor chose to go for sple-
nectomy or other therapy such as IVIg or anti-D. The mean
platelet count in these patients at the end of 2 weeks of
steroid treatment was 17.5 ± 3.6 9 109/L, median
18 9 109/L and the range was 16 9 109/L. These patients
were given 50 mg/day of eltrombopag, and steroid was
gradually tapered and discontinued within 2 weeks.
At 2 weeks of eltrombopag, the mean value of platelet
counts was 152 9 109/L (range 10–470 9 109/L). At
1 month of eltrombopag therapy, the primary end point, as
the response to eltrombopag, was seen in 80 % (20 out of
25) patients. Response was 70 % in males and 86.8 % in
females. Mean platelet count at 1 month of eltrombopag
therapy was 152.5 ± 107.9 9 109/L, median 150 9 109/L
and range (11–450 9 109/L) (Fig. 1). The durable response
at 3 months was seen in 76 % of the patients with a mean
platelet count of 141.8 ± 44.9 9 109/L, median
120 9 109/L and range (10–225 9 109/L) (Fig. 2). Twelve
of 25 patients had attained platelet counts [150 9 109/L
and their eltrombopag was reduced to 25 mg/day. We did
not stop eltrombopag even in those with good response
within 3 months, as previous studies have shown risk of
rebound thrombocytopenia on stopping it.
A. K. Tripathi et al.
123
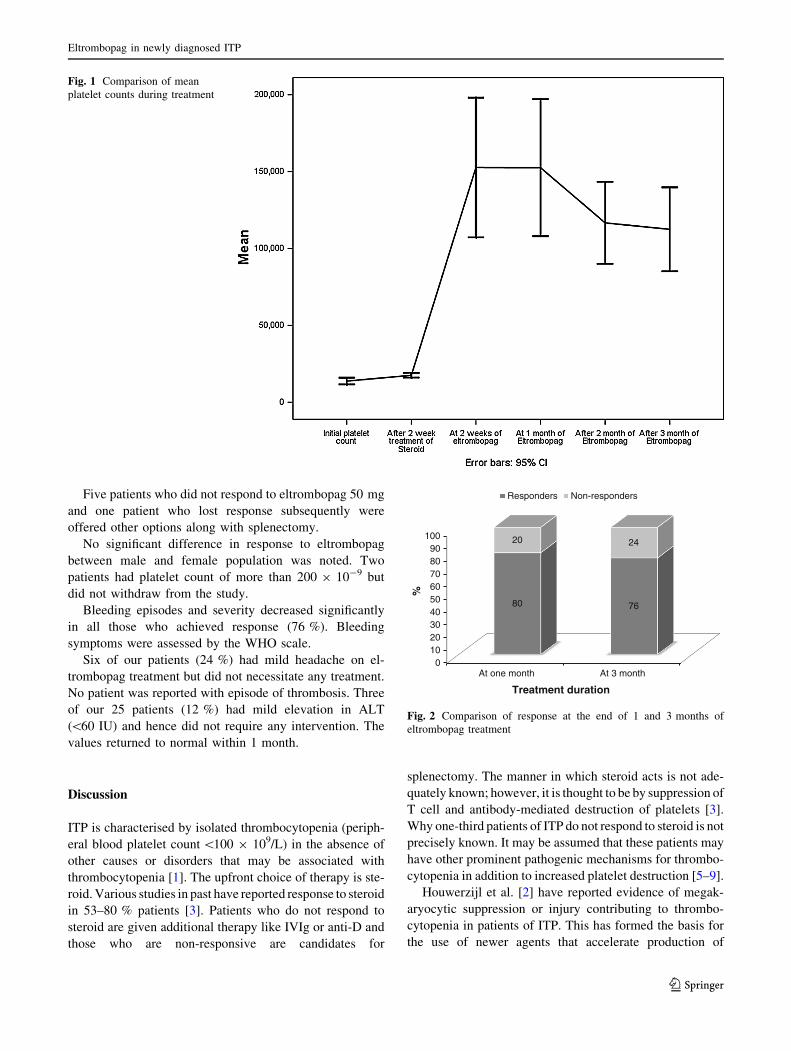
Five patients who did not respond to eltrombopag 50 mg
and one patient who lost response subsequently were
offered other options along with splenectomy.
No significant difference in response to eltrombopag
between male and female population was noted. Two
patients had platelet count of more than 200 9 10-9 but
did not withdraw from the study.
Bleeding episodes and severity decreased significantly
in all those who achieved response (76 %). Bleeding
symptoms were assessed by the WHO scale.
Six of our patients (24 %) had mild headache on el-
trombopag treatment but did not necessitate any treatment.
No patient was reported with episode of thrombosis. Three
of our 25 patients (12 %) had mild elevation in ALT
(\60 IU) and hence did not require any intervention. The
values returned to normal within 1 month.
Discussion
ITP is characterised by isolated thrombocytopenia (periph-
eral blood platelet count \100 9 109/L) in the absence of
other causes or disorders that may be associated with
thrombocytopenia [1]. The upfront choice of therapy is ste-
roid. Various studies in past have reported response to steroid
in 53–80 % patients [3]. Patients who do not respond to
steroid are given additional therapy like IVIg or anti-D and
those who are non-responsive are candidates for
splenectomy. The manner in which steroid acts is not ade-
quately known; however, it is thought to be by suppression of
T cell and antibody-mediated destruction of platelets [3].
Why one-third patients of ITP do not respond to steroid is not
precisely known. It may be assumed that these patients may
have other prominent pathogenic mechanisms for thrombo-
cytopenia in addition to increased platelet destruction [5–9].
Houwerzijl et al. [2] have reported evidence of megak-
aryocytic suppression or injury contributing to thrombo-
cytopenia in patients of ITP. This has formed the basis for
the use of newer agents that accelerate production of
Fig. 1 Comparison of mean
platelet counts during treatment
0102030405060708090
100
At one month At 3 month
80 76
20 24
%
Treatment duration
Responders Non-responders
Fig. 2 Comparison of response at the end of 1 and 3 months of
eltrombopag treatment
Eltrombopag in newly diagnosed ITP
123

platelets. TPO-RA such as eltrombopag and romiplostim
have been tried in patients with chronic ITP and phase II/III
trials have shown a good response with adequate safety and
efficacy [10–12]. Conventionally, in the steroid non-
responsive newly diagnosed patients, the choice is IVIg or
splenectomy. In our setup, most patients are either not able
to afford IVIg (average cost of therapy being $2500) or are
not willing to undergo splenectomy due to culturally
inherent fear of surgery. Also splenectomy has its own
limitations. It is effective only in 60–75 % of patients and
is associated with an increase in the risk to thrombosis.
Hence splenectomy in newly diagnosed ITP may be a hasty
decision. Moreover, few patients of adult ITP may attain
spontaneous remission once the effects of severe or
symptomatic thrombocytopenia are taken care of and
splenectomy can be avoided in them [3]. Eltrombopag has
previously been used effectively in chronic ITP patients
who were non-responsive to steroid or other agents [4, 10,
11]. However, its role in newly diagnosed ITP patients is
yet undefined. There is need for newer agents to be used in
newly diagnosed ITP patients who do not respond to ste-
roids. These agents should be able to increase the platelet
count within days in order to cover the period of bleeding
or severe thrombocytopenia. This justifies the use of TPO-
RA in newly diagnosed ITP patients. According to current
practice guideline, TPO-RA is not initial treatment of
choice in either naive, newly diagnosed patients or patients
non-responsive to steroid. Safety of TPO-RA in its short
term and to some extent long term uses is now established
by various studies. In addition, the response to eltrombopag
is visible within few days and the response is durable.
Hence, we sought to explore the role of eltrombopag in
newly diagnosed ITP patients (diagnosed within 3 months)
who were non-responsive to steroid. We used eltrombopag
as it has convenient oral dosing and is easily available.
We gave eltrombopag in 25 newly diagnosed patients of
ITP who did not show response after 2 weeks of steroid
therapy. The response to eltrombopag was observed in
80 % patients at 1 month. There was no effect of initial
platelet counts on the response to eltrombopag (Table 1).
There are no published studies on the effect of eltrombopag
in newly diagnosed ITP patients to the best of our
knowledge; however, when compared with a large study in
chronic ITP, where response was seen in 81 % patients,
response in our study was found to be comparable [4].
We tapered the dose of eltrombopag to 25 mg daily in
the responders and offered other options as splenectomy to
the non-responders. At the end of 3 months, response was
seen to be persisting in 76 % patients, which was higher
than the response seen in patients of chronic ITP as studied
by Cheng and Saleh [10, 11]. So the response to el-
trombopag in newly diagnosed patients can be considered
to be more durable than in patients of chronic ITP.
The mechanism by which TPO-RA increases platelet
count in patients not responding to steroid is a matter of
further studies. However, it is likely to be due to stimula-
tion of platelet production in such patients. In experimental
studies, TPO-RA was shown to stimulate production of
platelets in both the normal as well as injured bone marrow
[3, 13].
The pathogenetic mechanisms in ITP are heterogeneous
and the proposed mechanisms are (1) antibody-mediated
destruction, (2) T cell-mediated destruction, and (3)
megakaryocyte injury/suppression [5]. It is likely that one
or many mechanisms may operate in a single patient and the
response to therapy may depend upon the dominant
underlying mechanisms. We have previously shown that
patients who had evidence of bone marrow megakaryocytic
abnormality were less likely to respond to eltrombopag
[14]. Hence it can be assumed that the response to a par-
ticular agent may depend upon the predominant mechanism
underlying the pathogenesis of thrombocytopenia in ITP.
At present, the initial choice of therapy in newly diag-
nosed ITP patients is not individualised and steroid is
arbitrarily given to all patients of ITP who need treatment.
With addition of knowledge about different underlying
mechanisms of thrombocytopenia in ITP, it is imperative to
use other agents alone or in combination with steroids in
order to target different pathogenetic mechanisms. While
the specific ideal initial treatment is a matter of future
endeavours, combination therapy including steroid with
eltrombopag may be chosen as initial treatment in newly
diagnosed ITP patients, or eltrombopag may promptly be
chosen as agent of choice in case patients do not respond to
steroid within 2 weeks. Study population is biased because
it did not include other non-responders who opted for other
choices.
Our study has demerits in that it is a single-centre study,
has small sample size and lacks long-term safety profile.
This manuscript is intended to present our findings that
Table 1 Effect of initial
platelet count on response to
treatment with eltrombopag
Initial platelet count No. of patients At 1 month treatment At 3 months treatment
B10000 6 189000.00 ± 144391.10 133666.70 ± 74395.34
[10000 19 141052.60 ± 95715.71 105736.80 ± 63978.16
p value 0.35 0.37
A. K. Tripathi et al.
123

there is a possible role of eltrombopag in a subgroup of
newly diagnosed ITP patients and in no way it recommends
the use of eltrombopag in all newly diagnosed ITP patients.
However, the response to eltrombopag in newly diagnosed
steroid non-responsive ITP patients in the present study
sets a platform for a longer study on a larger number of
patients to substantiate the role of eltrombopag in these
patients.
Conflict of interest None.
References
1. Rodeghiero F, Roberto S, Terry GM, et al. Standardization of
terminology, definitions and outcome criteria in immune throm-
bocytopenic purpura of adults and children: report from an
international working group. Blood. 2009;113:2386–93.
2. Houwerzijl EJ, Blom NR, Van der Want JJL, et al. Ultrastructural
study shows morphologic features of apoptosis and para-apop-
tosis in megakaryocytes from patients with idiopathic thrombo-
cytopenic purpura. Blood. 2004;103:500–6.
3. Stasi R, Provan D. Management of immune thrombocytopenia in
adults. Mayo Clin Proc. 2004;79:504–22.
4. Bussel JB, Cheng G, Saleh MN, et al. Eltrombopag for the
treatment of chronic idiopathic thrombocytopenic purpura.
N Engl J Med. 2007;357:2237–47.
5. McMillan R. The pathogenesis of chronic immune thrombocy-
topenic purpura. Semin Hematol. 2007;44(4 Suppl 5):S3–11.
6. Olsson B, Anderson PO, Jemas M, et al. T cell mediated cyto-
toxicity toward platelets in chronic idiopathic thrombocytopenic
purpura. Nat Med. 2003;9(9):1123–4.
7. Chow L, Aslam R, Speck ER, et al. A murine model of severe
thrombocytopenia is induced by antibody and CD 8? T cell
mediated responses that are differentially sensitive to therapy.
Blood. 2010;115(6):1247–53.
8. Sakakura M, Wada H, Tawara I, et al. Reduced CD4? CD25- T
cells in patients with idiopathic thrombocytopenic purpura.
Thromb Res. 2007;120(2):187–93.
9. Ballem PJ, Segal GM, Stratton JR, et al. Mechanism of throm-
bocytopenia in chronic autoimmune thrombocytopenic purpura.
Evidence of both impaired platelet production and increased
platelet clearance. J Clin Invest. 1987;80(1):33–40.
10. Cheng G, Saleh MN, Marcher C, et al. Eltrombopag for man-
agement of chronic immune thrombocytopenia (RAISE): a
6-month, randomized, phase 3 study. Lancet. 2011;377(9763):
393–402.
11. Saleh MN, Bussel JB, Cheng G, et al. EXTEND Study Group.
Safety and efficacy of eltrombopag for treatment of chronic
immune thrombocytopenia: results of the long-term, open-label
EXTEND study. Blood. 2013;121(3):537–45.
12. Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard
of care in patients with immune thrombocytopenia. NEJM.
2010;363(20):1889–961.
13. Erickson-Miller CL, Delorme E, Tian SS, et al. Preclinical
activity of eltrombopag (SB-497115), an oral, nonpeptide
thrombopoietin receptor agonist. Stem Cells. 2009;27(2):424–30.
14. Tripathi A, Mishra S, Yadav D et al. Megakaryocyte morphology
and its impact in predicting response to steroid in immune
thrombocytopenia. Platelets 2013 (in press).
Eltrombopag in newly diagnosed ITP
123