Embed Size (px)
Citation preview

E/M coding for Mental HealthPamela Pully CPC, CPMAProfessional Insurance Consultants.

Presenter Pamela Pully 30+ years billing/coding/auditing all specialties. CPC - Certified Professional Coder CPMA – Certified Professional Medical Auditor Member of American Academy of Professional
Coders (AAPC), Past officer of local chapter. National Alliance of Medical Auditing Specialist (NAMAS) member, and current officer of Michigan Association of Reimbursement Officers (MARO)

Disclaimer This information is accurate as of April 1,
2015 and is designed to offer basic information for coding and billing. All information is based on experience, training and has been researched, interpreted and carefully reviewed by this trainer. Medical compliance/coding and billing information changes quickly. This can become outdated quickly. This is intended to be an educational guide and should not be considered as legal or consulting opinion.
Disclaimer cont. CPT, HCPCS and ICD-9 books were used for
coding information. Rules used come from AMA, ICD-9,CMS, final
rule and others. HIPAA and PPACA laws. Any questions on information I am
presenting, please ask. I will give you the source document I used.
It is important to me to give the best and most up to date information I can.

Goals for Training Have a better understand of things you
should and should not do when documenting for Evaluation and Management (E/M) codes.
Be aware of what is needed and/or required for each level of E/M.
Learn what is required for the new Diagnostic Evaluation.
Understand when to use add on codes
What we are going to talk about today.
1) Evaluation and Management (E/M) codes. The replacement for Medication Review 90862.
2) 7 Elements of E/M3) 1997 Exam Rules4) What are differences between New patient and
established patients.5) Diagnostic evaluation.6) Add on code 907857) Documentation requirements.8) This is an aggressive schedule, we can do it.9) Ask questions as we go.
What we should not do Cross Walk codes-90862 to any one E/M. Use only time as factor for coding. Use of unspecified diagnostic codes for
services. Just minimal training in this area. Getting correct diagnosis especially ICD-10 is a different training.
Treat all carriers the same. Only use one carriers set of rules. This is
especially important for Medicaid.

Different codes different rules If you cross walk , the old medication review
to one E/M code you run the risk for not meeting the documentation requirements.
Using the same code for easy and difficult cases can lead to rejections and flag for audit.
Documentation ( sometimes carrier utilization rules) decides the code.
Keep in mind 1% errors is100% wrong.

Review of documentation requirements
90862
Must include the condition for which the medication is needed, type of medication, dosage, directions for use, any frequent side effects and the effect the medication is having on the patients symptoms/condition
99213
2 of 3 for established patient
Expanded problem focus history
Expanded problem focus exam
Low Medical Decision Making (MDM)

Evaluation and Management There are 7 components to E/M 3 key elements
and 3 contributory factors and time.1. History2. Exam3. Medical Decision Making4. Counseling5. Coordination of care6. Nature of Presenting Problem7. Time

E/M rules for time Time factor: You can only use time if
more than 50% of the visit is spent counseling and it is documented. More on this later.
You can have a higher level of E/M codes with less time.
Chief Complaint (CC) and Medical Decision Making (MDM) are the most important part of an E/M code.
Chief Complaint The Chief Complaint also known as CC, is
part of the medical history taking, and is a concise statement describing the symptom, problem, condition, diagnosis, physician recommended return, or other factors that are the reason for a medical encounter.
The patient's initial comments to a physician, nurse, or other health care professional help form the differential diagnosis.
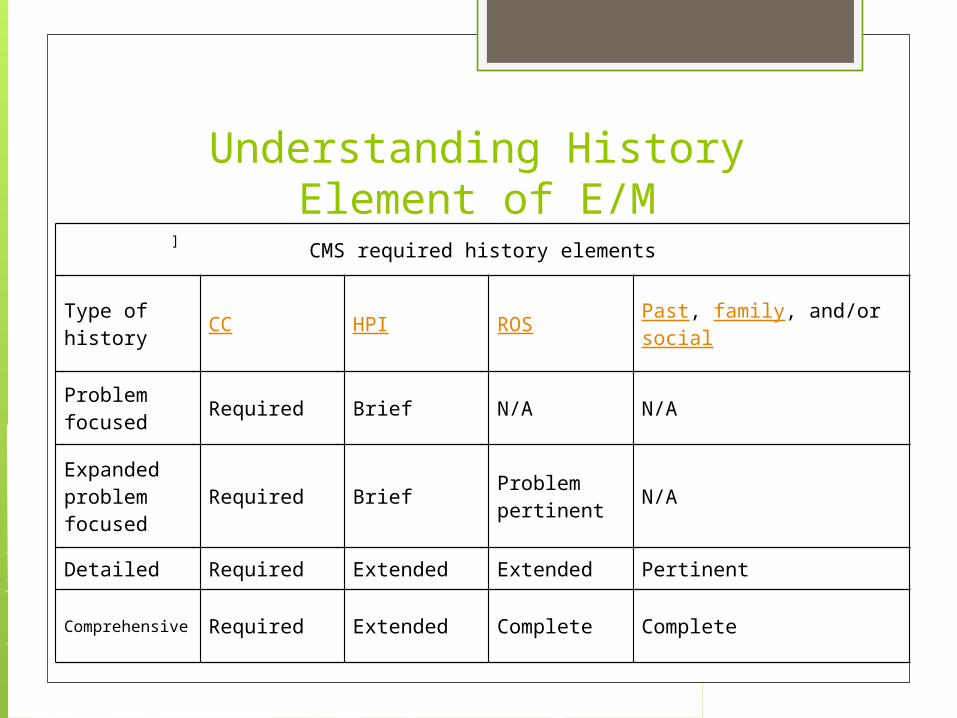
Understanding History Element of E/M
CMS required history elements
Type of history CC HPI ROS Past, family, and/or social
Problem focused Required Brief N/A N/A
Expanded problem focused
Required Brief Problem pertinent N/A
Detailed Required Extended Extended Pertinent
Comprehensive Required Extended Complete Complete
]

1995/1997 Exam rules Best advise decide what works best for
your practiced and use it. You can use 1995 for one claim and 1997
for another. Eliminate the potential risk from an audit.
Make decision to use 1995 or 1997. Write in policies and procedures. “We use
1997 exam rules for E/M” or “1995 rules”.
Understanding Exam Element of E/M
1995 rules are easy but usually for specialty physicians this is not the best rule to use.
1997 rules has bullet points within one area exam allowing you to get a better level.
1995/1997 Lets look at the 1997 exam for psych https://
www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/eval_mgmt_serv_guide-ICN006764.pdf
Understanding MDM Element of E/M
A-number of diagnosis or treatment options
B-Risk of Complications and/or Morbidity or Mortality
C-amount and/or complexity of data reviewed
Remove the lowest next lowest rules.
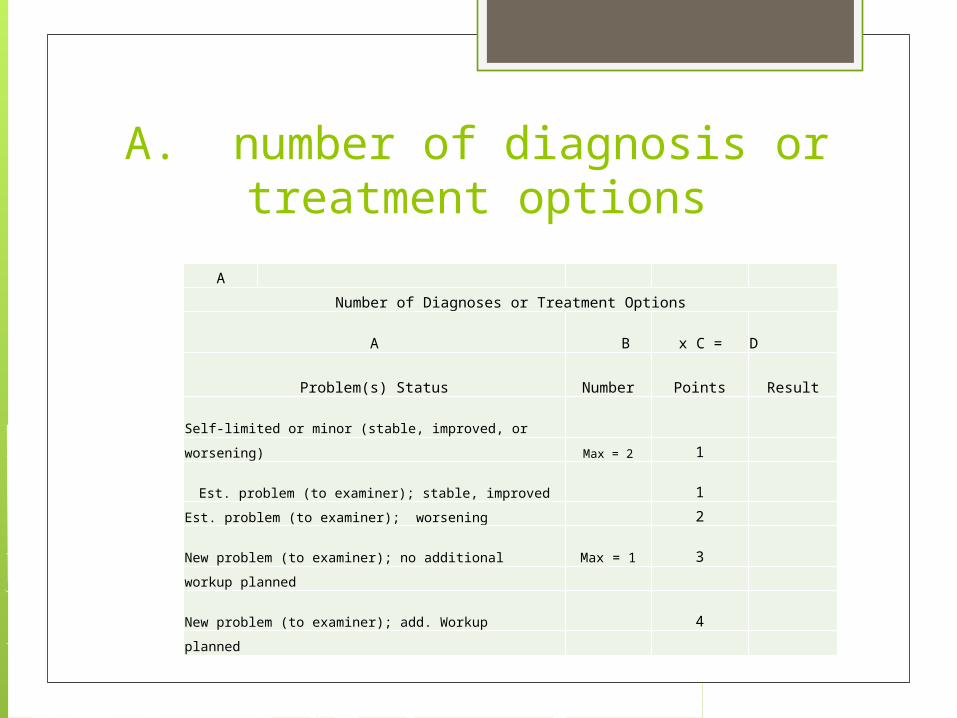
A. number of diagnosis or treatment options
A
Number of Diagnoses or Treatment Options
A B x C = D
Problem(s) Status Number Points Result
Self-limited or minor (stable, improved, or
worsening) Max = 2 1
Est. problem (to examiner); stable, improved 1
Est. problem (to examiner); worsening 2
New problem (to examiner); no additional Max = 1 3
workup planned
New problem (to examiner); add. Workup 4
planned

B. Risk of complications and/or morbidity or mortality
There is much information in this area.
It is found on the paper passed out with this power point.
Let review Important factor in using the high
level of toxic medicine.

Amount and/or complexity data reviewed
C
Amount and/or Complexity of Data Reviewed
Reviewed Data Points
Review and/or order of clinical lab tests 1
Review and/or order of tests in the radiology section of CPT 1
Review and/or order of tests in the medicine section of CPT 1 Discussion of test results with performing physician 1 Decision to obtain old records and/or obtain history from someone other than patient
Review and summarization of old records and/or obtaining history from someone other than patient and/or discussion of case with another health care provider.
1 Independent visualization of image, tracing or specimen itself (not simply review of report)
2
AIMS test adds to E/M Aims tests are not individually billable.
Usually done by non-physician provider.
If you review test positive or negative and document you reviewed this is, an additional point is added to review of test data. This is in the MDM section of the E/M code. Test data reviewed, one point.
Time for counseling/coordination of care
You must spend more than 50% of the visit on counseling or coordinating care.
It must be documented: Total time and the amount of time spent on counseling or coordinating care.
You do not have to use start stop time of counseling. You can think of time spent as part of the entire visit. Just make sure you document.
N.A.M.A.S. 5/9/2014 Documentation of Time with Evaluation and
Management Services: Time is built into the E/M codes so physicians are told
to base their E/M selection on the 3 components: History, Exam and Medical Decision Making. Times are listed in the CPT manual with each level of service as a guideline only.
If a provider spends more than 50% of a face-to-face visit counseling and/or coordinating patient's care, the provider can code the visit based on time spent even if the History, Exam and MDM elements are lacking.
N.A.M.A.S. 5/9/2014 Time must be documented as well as the
detailed description of the circumstance (counseling patient or coordinating care). For example: 55 minutes spent with patient, 30 minutes was spent in discussion with patient and family regarding care.
Prolonged service codes can be reported in addition to an E/M code when the length of time a provider spends with a patient in an outpatient setting exceeds greater than 30 minutes beyond the typical for the level of service selected.
Difference in New patient and Established patient
A new patient for a group practice is one that has not been seen by anyone in the group with the same discipline in the last 3 years.
CMS and AMA have different rules for “new” A new patient E/M code must meet 3 of 3 to
be coded at that level. An established patient only requires 2 of 3
to be coded at that level.
E/M codes for different place of service
AFC/Group home. There are two groups of codes. New and
Established. New 99324-99328 Established 99334-99337 Residential home POS 12 New 99341-99345 Established 99347-99350
90785 add on code for complicated cases
90785-This code can be used to add on to diagnostic evaluation and therapy codes not E/M when the follow is present.
Factors typically present1. Have other individuals legally
responsible for their care, such as minors or adults with guardians, or
New 90785 add on code for complicated casesFactors typically present
2. Request others to be involved in their care during the visit, such as adults accompanied by one or more participating family member or interpreter or language translator or
3. Require the involvement of another third parties, such as child welfare agencies, parole or probation officers or schools.

90785 maybe reported when at least one is present:
1. The need to manage maladaptive communication (related to, e.g.; high anxiety, high reactivity, repeated questions or disagreements ) among participants that complicates delivery of care.
2. Caregiver emotions or behavior that interferes with the caregivers understand and ability to assist in the implementation of the treatment plan.

90785 maybe reported when at least one is present:
3. Evidence or disclosure of a sentinel event and mandated report to third party (e.g., abuse neglect with report to state agency) with initiation of discussion of the sentinel event and/or report with patient and other visit participants.
90785 maybe reported when at least one is present:
4. Use of play equipment, other physical devices, interpreter, or translator to communicate with the patient to overcome barriers to therapeutic or diagnostic interaction between the physician or other qualified health care professional and a patient who…….next slide
90785 maybe reported when at least one is present:
a) Is not fluent in the same language as the physician or healthcare professional.
b) Has not developed or has lost, either the expressive language communication skills to explain his/her symptoms and response to treatment, or the receptive communication skills to understand the physician or healthcare professional.
99211 This is the most basic service done in
the office. Usually done by nurse when patients is
not being seen by doctor. You must document 2 elements,
Example vitals and what you did. This must be billed under the provider.
99211 This code is for the office setting only. If there is a nurse visit done in the home
you have to follow the rule: CPT code first HCPCS codes second.
There is no CPT code for nurse visit in the home so you look to HCPCS.
The best HCPCS code for a nurse visit in the home is T1002.
Do not use T1002 for in office visits.

DocumentationDocumentation Guidelinesa) They are in place and you need to
familiarize yourself with them. b) Medical necessity is the most weighted
elements in a E/M. There needs to be a reason for the visit. Chief Complaint.
c) There are different guidelines for different carriers when it come to billing.
Documentation rules for E/M We now know the parts of E/M. We need to be
reminded that documentation must be complete in these areas.
You can lose money or increase revenue with your documentation.
You must put down what you are doing and the calculations in your head must be documented.
One doctor I worked with put it like this. “Document what you did do and why did you do it. Explain your thought process.”

Timeliness requirement 3.3.2.5 - Late Entries in Medical Documentation (Rev. 377, Issued: 05-27-11, Effective: 06-28-11, Implementation:
06-28-11)
The MACs, CERT, Recovery Auditors, and ZPICs shall give less weight when making review determinations to documentation, including a provider’s internal query responses, created more than 30 calendar days following the date of service. If the MACs, CERT, or Recovery Auditors identify providers with patterns of making late (more than 30 calendar days past the date of service) entries in the medical documentation, including the query responses, the reviewers shall refer the cases to ZPIC and may consider referring to the RO(regional office) and State Agency.

Diagnostic Evaluation CPT90791 and 90792
Local Coverage Determination (LCD): Psychiatry and Psychology Services (L30489)
90791: A psychiatric diagnostic evaluation (90791 is an integrated assessment that includes history, mental status and recommendations. It may include communicating with the family and ordering further diagnostic studies. Use add-on code 90785 in conjunction with 90791 when the diagnostic evaluation includes interactive complexity services.
90792: A psychiatric diagnostic evaluation with medical services (90792) includes 90791 and a medical assessment. It may require a physical exam, communication with the family, prescription medications and ordering laboratory or other diagnostic studies. Use add-on code 90785 in conjunction with 90792 when the diagnostic evaluation includes Interactive Complexity services
Diagnoses The rule is to code to the highest
specificity . Should not use unspecified codes. Make sure to include all diagnoses that
you considered before setting the plan or prescribing medication.
ICD-9 has ordering rules. Final rule ICD-10 effective 10-01-2015

Medicaid provider qualifications requirements
90791--ok for N .P. or psychiatrist 90792 require a psychiatrist. There was much discussion in Lansing
with the state and changing this requirement. I finally happened 1/1/2015
The current mental health qualification chart has been changed.

Any questions?