Embed Size (px)
Citation preview
Emerging Challenges in Primary Care: 2016
Evolving Strategies of Care in Diabetes: The Role and Rationale of
Glucoretic Therapy
Faculty
• Richard S. Beaser, MDSenior Staff PhysicianChair, Continuing Medical Education Committee Joslin Diabetes CenterAssociate Clinical Professor of MedicineHarvard Medical SchoolBoston, MA
• Mark Stolar, MDAssociate Professor of MedicineFeinberg School of Medicine Northwestern UniversityChicago, IL
• Louis Kuritzky, MDClinical Faculty Family Medicine Residency ProgramPalms Medical GroupNorth Florida Regional Medical CenterClinical Assistant Professor Emeritus Department of Community Health and Family Medicine University of Florida Gainesville, FL
• Jeff Unger, MD, ABFM, FACEDirector, Unger Primary Care Medical GroupRancho Cucamonga, CA
2
Disclosures
§ Richard S. Beaser, MD has no relationships to disclose.
§ Louis Kuritzky, MD serves as a speaker and/or advisor and/or consultant for Boehringer Ingelheim, Sanofi Aventis, Salix, AbbVie, Allergan, Lilly, Lundbeck, Novo Nordisk and Janssen.
§ Mark Stolar, MD serves as a speaker for and/or on the advisory board for Takeda, Sanofi, and Astra Zeneca.
§ Jeff Unger, MD, ABFM, FACE serves as a speaker for Novo Nordisk, Teva and Janssen. Dr. Unger also serves as a stock owner, consultant and researcher for Novo Nordisk.
3
Learning Objectives
§ Describe the role of the kidney in glycemic control.
§ Review emerging data surrounding the effects of SGLT2 inhibitor therapy.
§ Recognize the incidence and risk of hypoglycemia in managing patients with diabetes.
§ Discuss approaches to individualizing the treatment of T2DM.
4
PRE-TEST QUESTIONS
5
Pre-test ARS Question 1
In normal physiologic situations, approximately how many grams of glucose are excreted in the urine each day?
1. 0 g
2. 70 g
3. 125 g
4. 180 g
6
Pre-test ARS Question 2
Which of the following adverse events has not been seen with SGLT-2 inhibitors?
1. Increased fracture risk
2. Acute reduction in eGFR
3. Normoglycemic ketoacidosis
4. Congestive Heart Failure
7
Pre-test ARS Question 3The patient is a 52-year-old obese African American man with a 7 year history of type 2 diabetes mellitus (HbA1c 8%) and CKD. The decision is made to add an SGLT-2 inhibitor and reinforce lifestyle modifications to control his blood glucose. How should you counsel the patient about his new medication?
1. Explain that his HbA1c will likely decrease 1.5 to 2 percentage points from his current value after beginning the SGLT-2 inhibitor
2. Advise the patient that the new medication may cause a small increase in his blood pressure
3. Warn the patient that the SGLT-2 inhibitor may cause weight gain
4. Counsel patient about the signs and symptoms of orthostatic hypotension which may occur secondary to volume depletion with SGLT-2 inhibitors
8

Pre-test ARS Question 4
According to studies using continuous glucose monitoring, approximately what proportion of patients with type 2 diabetes on treatment have unrecognized hypoglycemic episodes?
1. >15%
2. >30%
3. >45%
4. >70%
9
Pre-test ARS Question 5
Please rate your confidence in your ability to appropriately use SLGT-2 inhibitors in patients with type 2 diabetes:
1. Not at all confident
2. Slightly confident
3. Moderately confident
4. Pretty much confident
5. Very confident 10
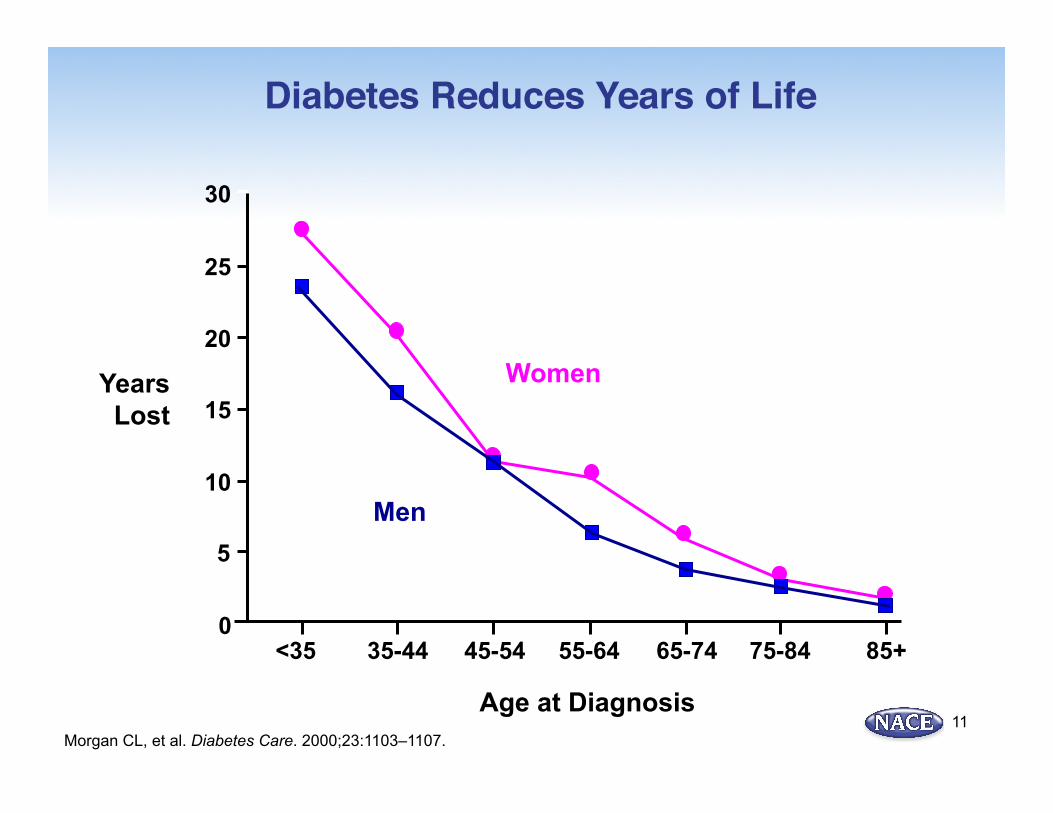
Diabetes Reduces Years of Life
Morgan CL, et al. Diabetes Care. 2000;23:1103–1107.
0
5
<35 35-44
10
15
20
25
30
Years Lost
45-54 55-64 65-74 75-84 85+
Age at Diagnosis
Women
Men
11
Patient Case 1: Edward B.§ Edward B.: 54-year-old obese black man
Ø Works as a long-haul truck driver Ø Diagnosed with T2D 10 years ago
§ Strong family history of T2D (maternal and paternal sides of his family and 2 siblings)
§ Despite counseling for intensive lifestyle modification (including nutritional counseling and physical activity), continues to gain weight Ø 15 lb this year
§ Poor compliance with current drug therapy regimen because of his job Ø Fears experiencing hypoglycemia while driving
§ Finds it difficult to adhere to a dietary regimen because he frequently eats “on the go”
14
Patient Case 1: Edward B. (cont.)
§ HbA1c is 9.2% § Fasting plasma glucose (FPG) level is 165 mg/dL § Has several additional risk factors for
cardiovascular disease including obesity, hypertension, and elevated cholesterol level • High blood pressure (140/95 mm Hg; medically
managed) • Elevated lipid levels (medically managed) • Body mass index (BMI) is 36 kg/m2
§ Reports episodes of low blood glucose levels • Most recent documented blood glucose level via finger
stick was 58 mg/dL
15
Patient Case 1: Edward B. (cont.)
§ Current medications • Metformin 1000 mg twice daily • Glimepiride 8 mg once daily • Basal insulin glargine • Enalapril/HCTZ 10 mg/25 mg once daily • Rosuvastatin 20 mg once daily
16
Edward B.: Clinical Data
§ Physical Exam: Pertinent positives
§ Acanthosis nigricans on neck
§ R carotid bruit
§ Decreased vibratory sense in feet
§ Labs: Abnormalities:
§ eGFR 52
§ Albumin/creat ratio 60mcg/mg (N <30)
17
Patient Case Edward B.: Question #1
How might his medication be changed to address his elevated HbA1c, continued weight gain and fear of hypoglycemia? 1. Discontinue glimepiride and add a GLP-1 receptor agonist 2. Discontinue glimepiride and add an SGLT-2 inhibitor 3. Discontinue metformin and increase the dose of glimepiride 4. Discontinue glimepiride and add a thiazolidinedione 5. Options 1 and 2
18
Clinical Rationale for changes
§ Severe insulin resistance not adequately addressed by metformin
§ Hypoglycemia from sulfonylurea despite lack of postprandial efficacy
§ Increased CV/CVA risk (see IRIS study/ EMPA-REG study)
§ Microalbuminuria
19
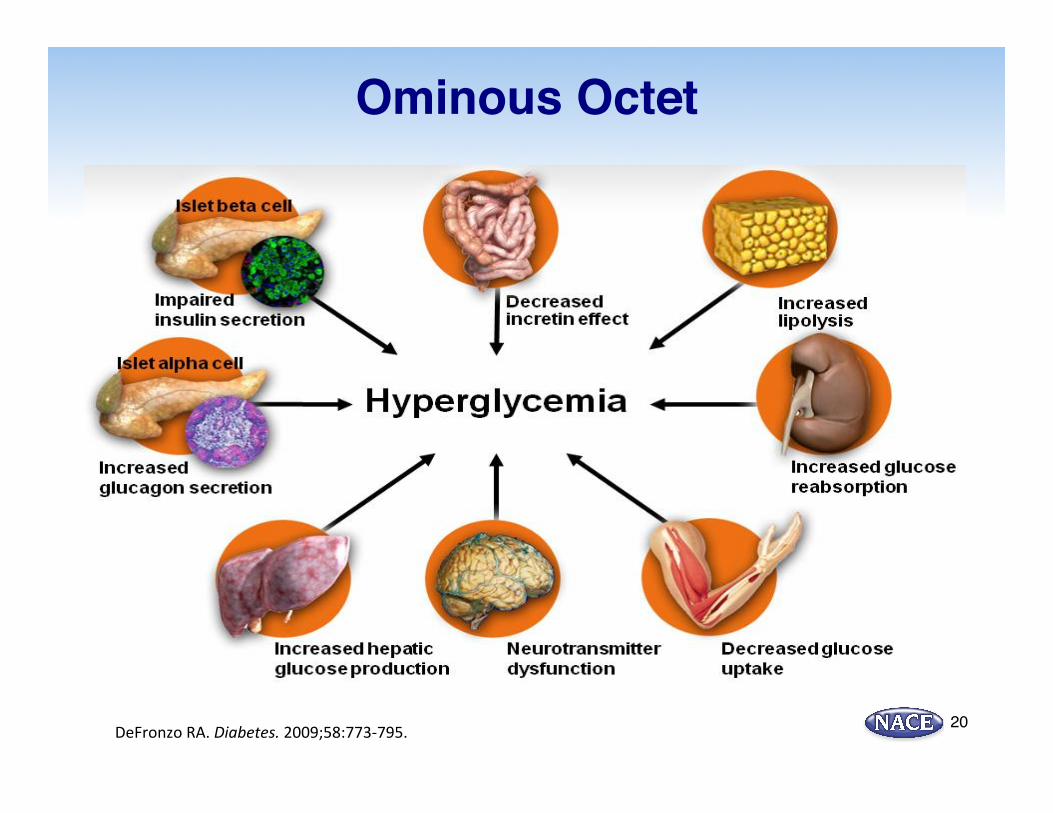
Ominous Octet
DeFronzo RA. Diabetes. 2009;58:773-‐795. 20
Normal Glucose Homeostasis Reflects a Balance of Glucose Production, Absorption, and Excretion
Ø Multiple pathways maintain constant glucose +/- 80-120 mg/dL Ø Insulin Ø Glucagon Ø Hepatic: gluconeogenesis, glycogenolysis Ø Renal: gluconeogenesis, glucose reabsorption,
glucose excretion
Chao E, et al. Nature Rev Drug Discov. 2010;9:551-559.
21
The Kidney Plays Key Roles in Maintaining Glucose Homeostasis: Production and Reabsorption of Glucose
§ Gluconeogenesis (Production) • Estimated to be responsible for up to 20% of total glucose release
§ Glucose filtration • Filters up to 180 g/day of glucose through the renal glomerulus
§ Glucose reabsorption • Expedites reabsorption of filtered glucose into plasma and excretion of excess
glucose in urine • At plasma glucose concentrations up to 180 to 200 mg/dL, essentially all glucose
is reabsorbed • At levels ~200 to 250 mg/dL or when the filtered glucose load exceeds
375 mg/min, excess glucose is excreted in urine: “transport maximum (Tmax)” • Renal absorption from the kidneys is via SGLT-1 and and SGLT-2 sodium co-
transporters
Chao E, et al. Nature Rev Drug Discov. 2010;9:551-559; DeFronzo RA, et al. Diabetes Obes Metab. 2012;14:5-14; Gerich JE. Diabet Med. 2010;27:136-142.
22
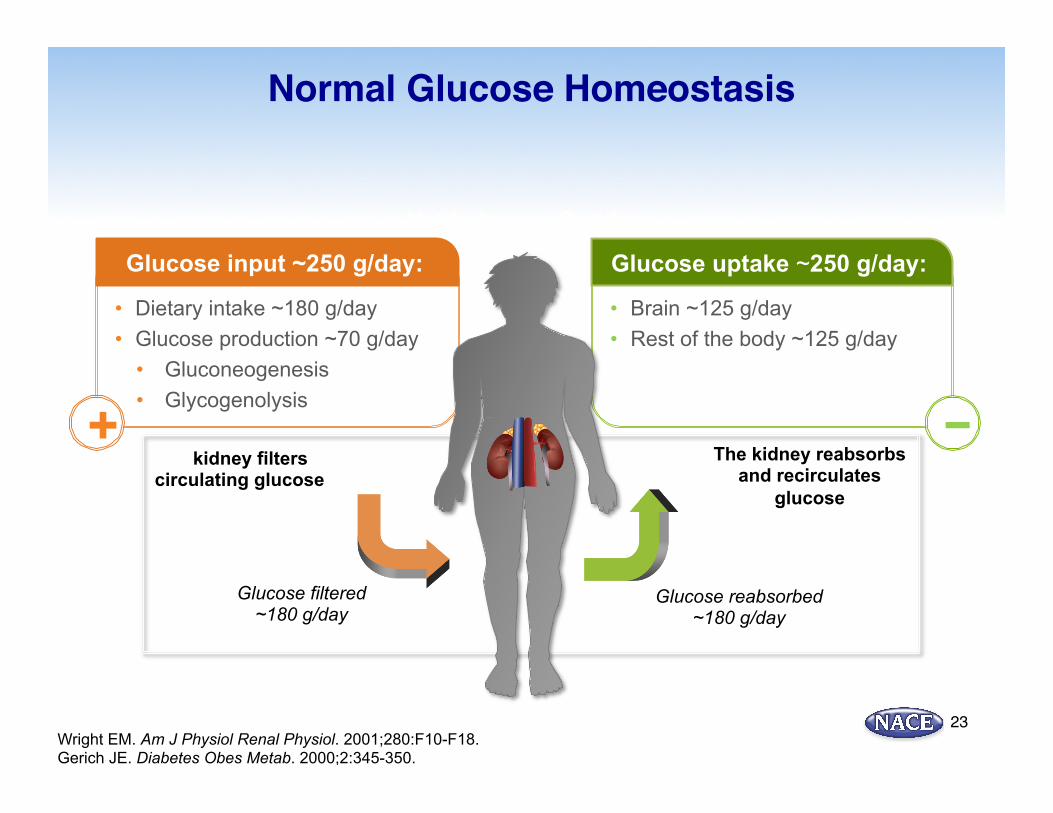
• Brain ~125 g/day • Rest of the body ~125 g/day
Glucose uptake ~250 g/day:
−
• Dietary intake ~180 g/day • Glucose production ~70 g/day
• Gluconeogenesis • Glycogenolysis
Normal Glucose Homeostasis
Wright EM. Am J Physiol Renal Physiol. 2001;280:F10-F18. Gerich JE. Diabetes Obes Metab. 2000;2:345-350.
+
Net balance ~0 g/day
Glucose input ~250 g/day:
The kidney filters circulating glucose
Glucose filtered ~180 g/day
Glucose reabsorbed ~180 g/day
The kidney reabsorbs and recirculates
glucose
23
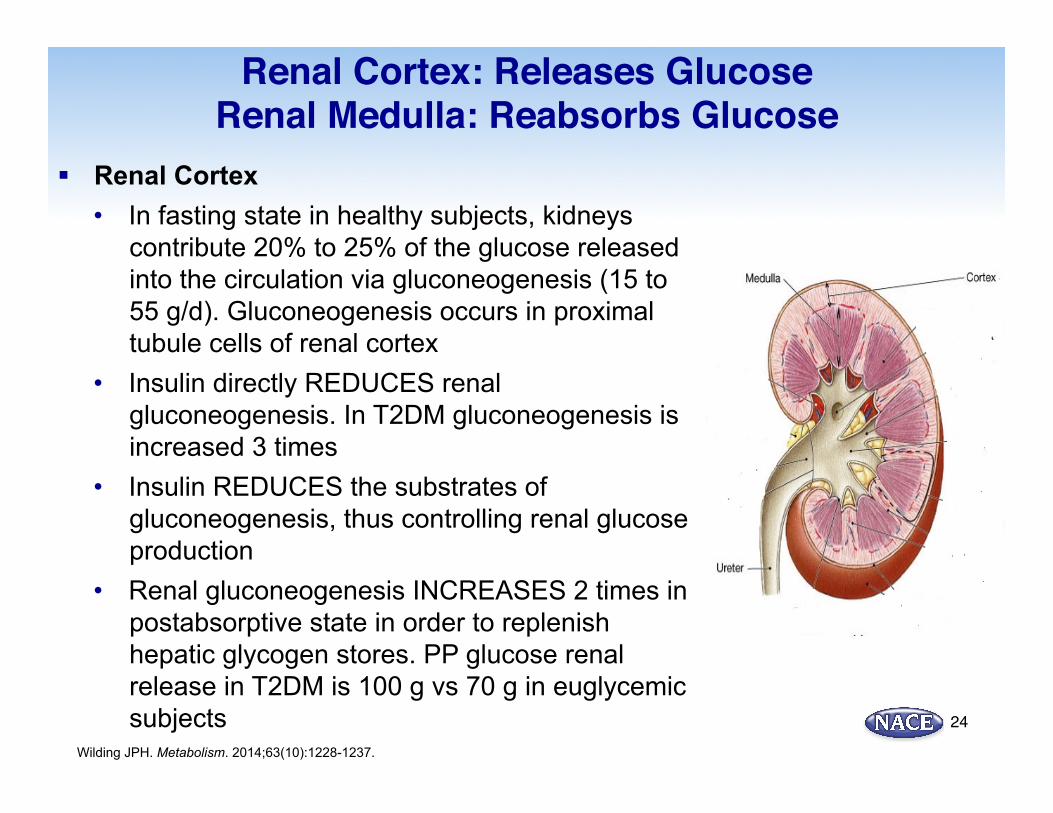
Renal Cortex: Releases Glucose Renal Medulla: Reabsorbs Glucose
§ Renal Cortex • In fasting state in healthy subjects, kidneys
contribute 20% to 25% of the glucose released into the circulation via gluconeogenesis (15 to 55 g/d). Gluconeogenesis occurs in proximal tubule cells of renal cortex
• Insulin directly REDUCES renal gluconeogenesis. In T2DM gluconeogenesis is increased 3 times
• Insulin REDUCES the substrates of gluconeogenesis, thus controlling renal glucose production
• Renal gluconeogenesis INCREASES 2 times in postabsorptive state in order to replenish hepatic glycogen stores. PP glucose renal release in T2DM is 100 g vs 70 g in euglycemic subjects
Wilding JPH. Metabolism. 2014;63(10):1228-1237.
24
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
SGLT2 GLUT2
Control T2DM
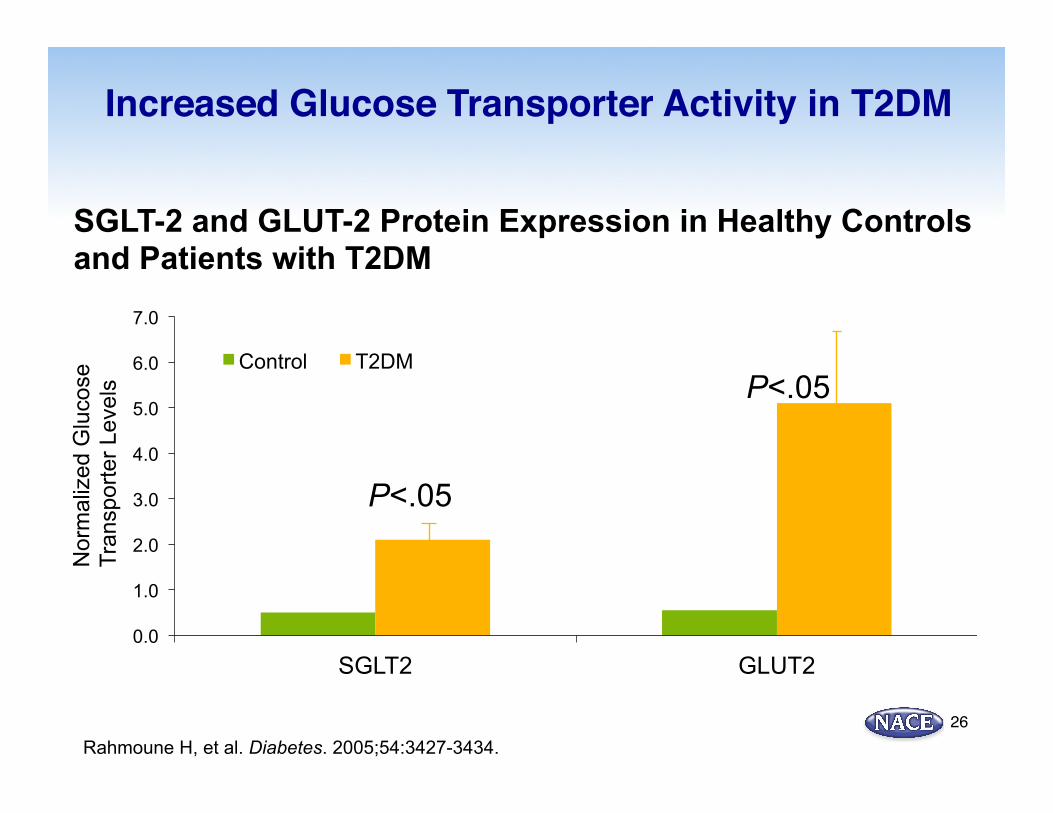
Increased Glucose Transporter Activity in T2DM
Rahmoune H, et al. Diabetes. 2005;54:3427-3434.
P<.05
P<.05
SGLT-2 and GLUT-2 Protein Expression in Healthy Controls and Patients with T2DM
Nor
mal
ized
Glu
cose
Tr
ansp
orte
r Lev
els
26
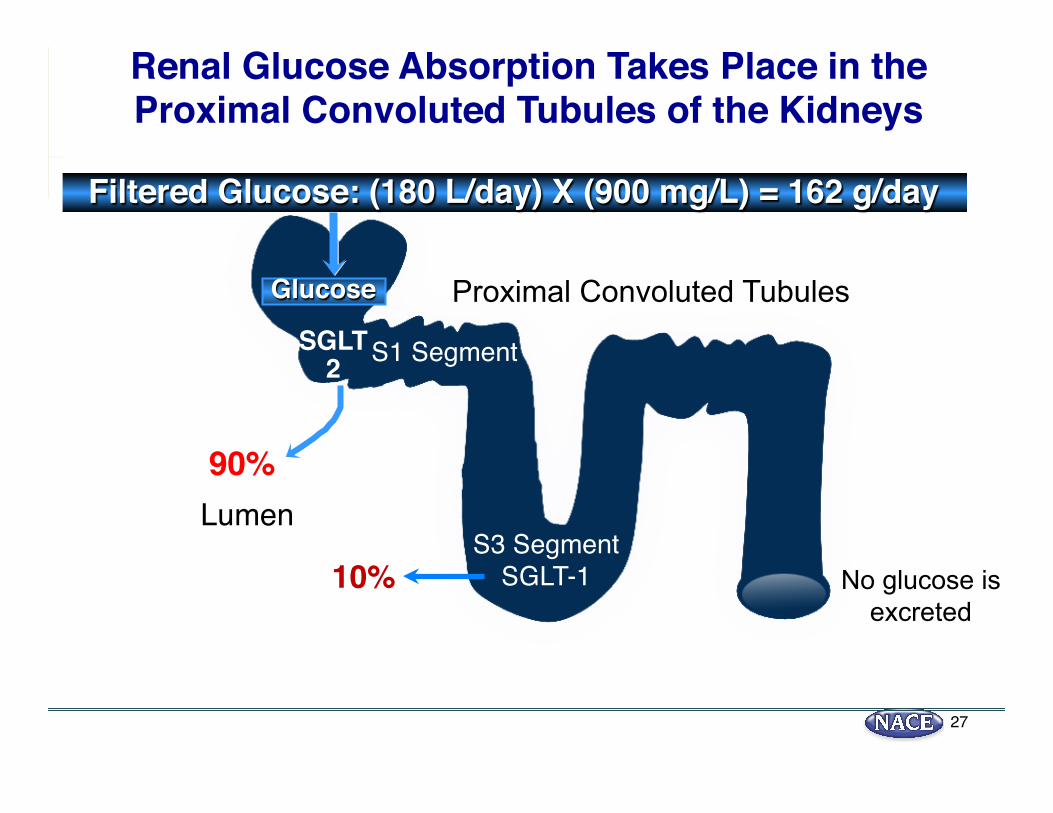
Glucose
SGLT2
90%
Renal Glucose Absorption Takes Place in the Proximal Convoluted Tubules of the Kidneys
SGLT-110%
Lumen
No glucose is excreted
Filtered Glucose: (180 L/day) X (900 mg/L) = 162 g/day
Proximal Convoluted Tubules
S3 Segment
S1 Segment
27
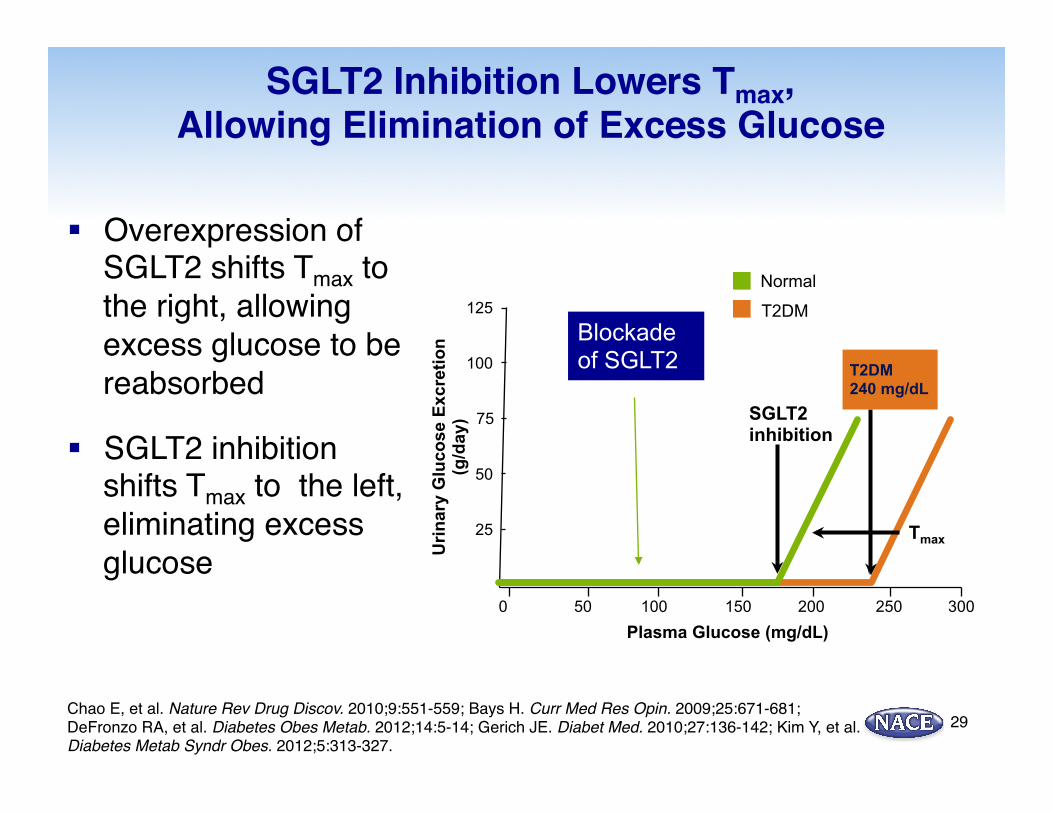
SGLT2 Inhibition Lowers Tmax, Allowing Elimination of Excess Glucose
§ Overexpression of SGLT2 shifts Tmax to the right, allowing excess glucose to be reabsorbed
§ SGLT2 inhibition shifts Tmax to the left, eliminating excess glucose
Chao E, et al. Nature Rev Drug Discov. 2010;9:551-559; Bays H. Curr Med Res Opin. 2009;25:671-681; DeFronzo RA, et al. Diabetes Obes Metab. 2012;14:5-14; Gerich JE. Diabet Med. 2010;27:136-142; Kim Y, et al. Diabetes Metab Syndr Obes. 2012;5:313-327.
300 250 200 150 100 50 0
25
50
75
100
125
Urin
ary
Glu
cose
Exc
retio
n
(g/d
ay)
Plasma Glucose (mg/dL)
Tmax
SGLT2 inhibition
Normal
T2DM 240 mg/dL
T2DM Blockade of SGLT2
29
Is Pharmacologic Blockade of SGLT2 Safe?Familial Renal Glycosuria (FRG)
§ An inherited renal tubular disorder characterized by persistent isolated glucosuria in the absence of hyperglycemia
§ Patients excrete >100 grams of glucose/day (normal glucose excretion = 0 g/d)
§ Caused by mutations in the SGLT2 coding gene, SLC5A2
§ Patients have normal renal function, are not overweight, and do not develop diabetes
§ Asymptomatic
§ Family members of FRG may show glycosuria when given a 50 grams of glucose tolerance test after 2 and 4 hours
Prie D. Diabetes Metab. 2014;40(6 Suppl 1):S12-16.Santer N, et al. Clin J Am Soc Nephrol. 2010;5:133-141.
30
The Benefits of SGLT2 Inhibitors Unique Mechanism of Action
Inhibition of SGLT2 results in:
Daily urinary excretion of excess glucose ~70 g, providing:1
§ Significant HbA1c reductions (-0.34% to -1.03%)2,3 § Additional benefits of weight reduction (-2.0 to -3.4 kg) and a reduction in
blood pressure (cardioprotective)2
§ Reduction of fasting and PPG levels
31
SGLT2 Inhibitors act independently of insulin mechanisms2
Works regardless of β-cell function
Complements insulin-dependent
mechanisms
Low propensity for hypoglycemia
1. List JF, et al. Diabetes Care 2009;32:650–657.2. Bailey CJ, et al. Lancet 2010;375:2223–2233.3. Bailey CJ, et al. Diabetes. 2011;60(Suppl. 1):71st ADA Scientific Sessions;San Diego, CA. June 24-28, 2011.Poster #988-P.
Clinical Attributes of SGLT2 Inhibitors: Glycemic End Points
§ Reduce A1C by approximately 0.5% to 1.0% as monotherapy1-4
§ Provide additional A1C reductions when added to:3,5-11
§ Metformin (~0.7%)§ Glimepiride (~0.63%)§ Pioglitazone (~0.82%-0.97%)§ DPP-4 inhibitor (~0.5%)§ Basal insulin (~0.6%-1.0%)
1. Stenlöf K, et al. Diabetes Obes Metab. 2013;15:372-382; 2. Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224; 3. Henry RR, et al. Int J Clin Pract. 2012;66:446-456; 4. List JF, et al. Diabetes Care. 2009;32:650-657; 5. Cefalu WT, et al. Lancet. 2013;382:941-950; 6. Bailey CJ, et al. Lancet. 2010;375:2223-2233; 7. Bailey CJ, et al. BMC Med. 2013;11:43; 8. Nauck MA, et al. Diabetes Care. 2011;34:2015-2022; 9. Rosenstock J, et al. Diabetes Care. 2012;35:1473-1478; 10. Jabbour SA, et al. Diabetes Care. 2014;37:740-750; 11. Strojek K, et al. Diabetes Obes Metab. 2011;13:928-938.
32
Clinical Attributes of SGLT2 Inhibitors: Low Hypoglycemia Risk and Weight Loss
§ Low risk of hypoglycemia1-8
§ SGLT2 inhibitors are not associated with hypoglycemia as monotherapy or in combination with metformin or DPP-4 inhibitors
§ May increase hypoglycemia when combined with insulin or insulin secretagogues; dose adjustments of those agents may be necessary
§ SGLT2 inhibitors promote clinically relevant weight loss1-4,6,9,10
§ Approximately 2.0 to 2.5 kg in clinical trial settings§ Significant weight loss versus placebo when added to metformin4,10
1. Bailey CJ, et al. BMC Med. 2013;11:43; 2. Bolinder J, et al. J Clin Endocrinol Metab. 2012;97:1020-1031; 3. Nauck MA, et al. Diabetes Care. 2011;34:2015-2022; 4. Rosenstock J, et al. Diabetes Care. 2012;35:1232-1238; 5. Schernthaner G, et al. Diabetes Care. 2013;36:2508-2515; 6. Stenlöf K, et al. Diabetes Obes Metab. 2013;15:372-382; 7. Strojek K, et al. Diabetes Obes Metab. 2011;13:928-938; 8. Wilding JP, et al. Diabetes Care. 2009;32:1656-1662; 9. Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224; 10. Bailey CJ, et al. Lancet. 2010;375:2223-2233.
33
15.9
11.5
19.5
9.5 10.0 10.2 10.1 9.0
4.8 4.3
0
5
10
15
20
25
Major Macrovascular
Event
Major Microvascular
Event
Death From Any Cause
CV Disease Non-CV Disease Perc
ent o
f pat
ient
s w
ith >
1 se
vere
hyp
ogly
cem
ic e
vent
Severe Hypoglycemia (n=231) No Severe Hypoglycemia (n=10,909)
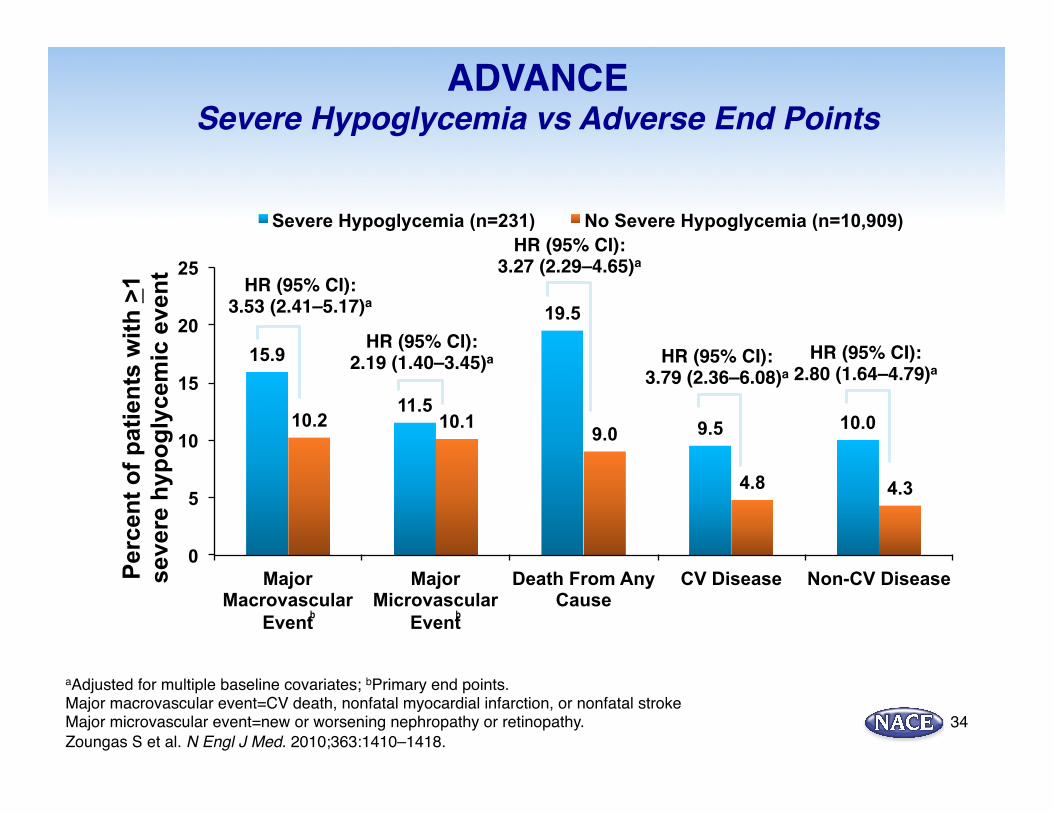
ADVANCESevere Hypoglycemia vs Adverse End Points
aAdjusted for multiple baseline covariates; bPrimary end points. Major macrovascular event=CV death, nonfatal myocardial infarction, or nonfatal strokeMajor microvascular event=new or worsening nephropathy or retinopathy.Zoungas S et al. N Engl J Med. 2010;363:1410–1418.
HR (95% CI):3.53 (2.41–5.17)a
HR (95% CI):2.19 (1.40–3.45)a
HR (95% CI):3.27 (2.29–4.65)a
HR (95% CI):3.79 (2.36–6.08)a
HR (95% CI):2.80 (1.64–4.79)a
b b
34
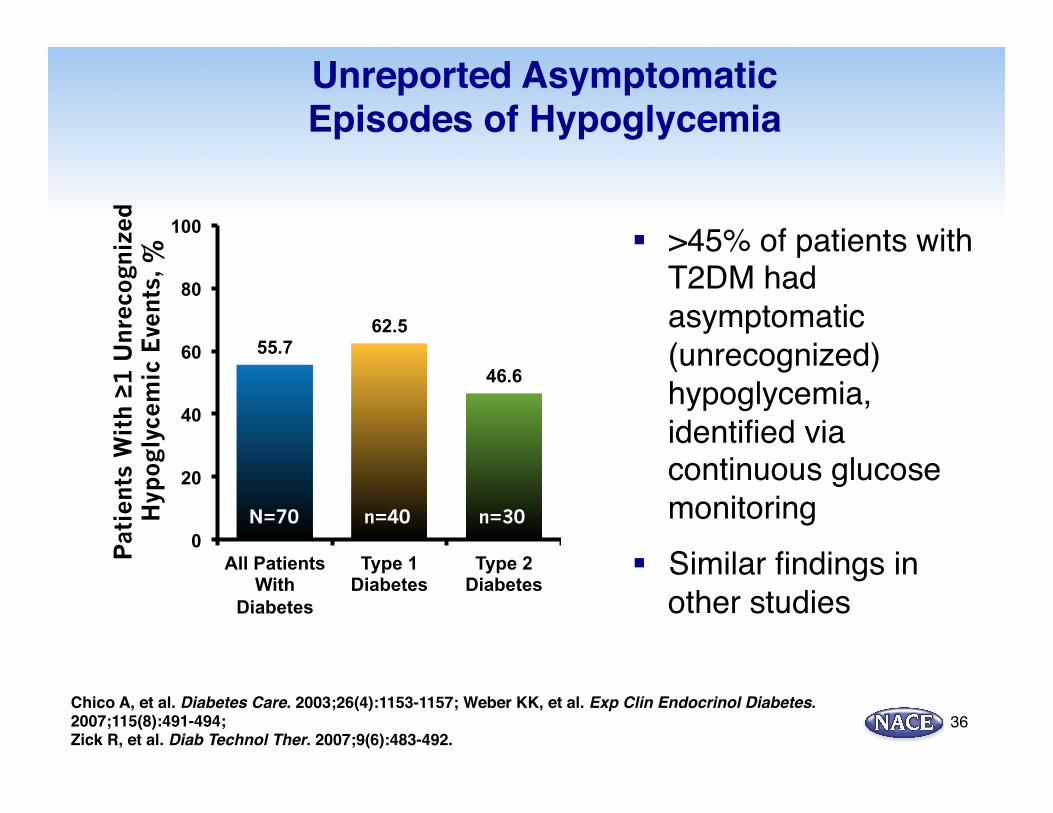
Unreported Asymptomatic Episodes of Hypoglycemia
§ >45% of patients with T2DM had asymptomatic (unrecognized) hypoglycemia, identified via continuous glucose monitoring
§ Similar findings in other studies
Chico A, et al. Diabetes Care. 2003;26(4):1153-1157; Weber KK, et al. Exp Clin Endocrinol Diabetes. 2007;115(8):491-494;Zick R, et al. Diab Technol Ther. 2007;9(6):483-492.
Pat
ient
s W
ith ≥1
Unr
ecog
nize
d
Hyp
ogly
cem
ic E
vent
s, %
55.7 62.5
46.6
0
20
40
60
80
100
All Patients With
Diabetes
Type 1 Diabetes
Type 2 Diabetes
N=70 n=40 n=30
36
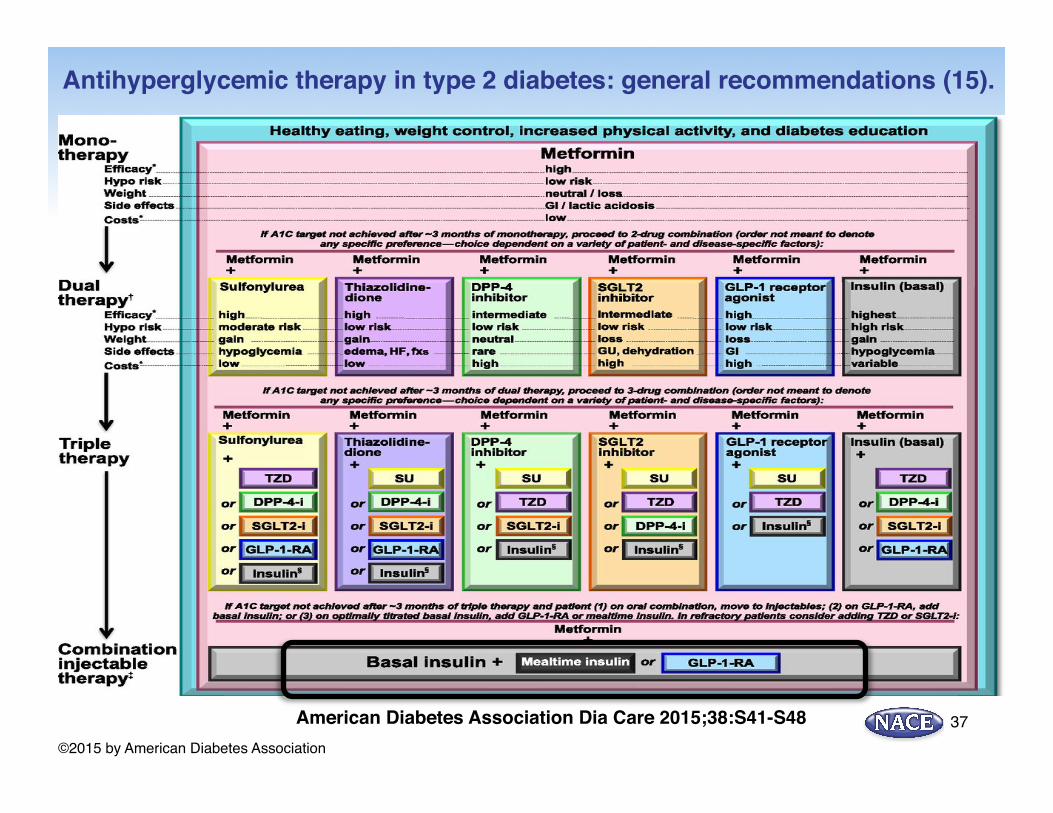
Antihyperglycemic therapy in type 2 diabetes: general recommendations (15).
American Diabetes Association Dia Care 2015;38:S41-S48©2015 by American Diabetes Association
37
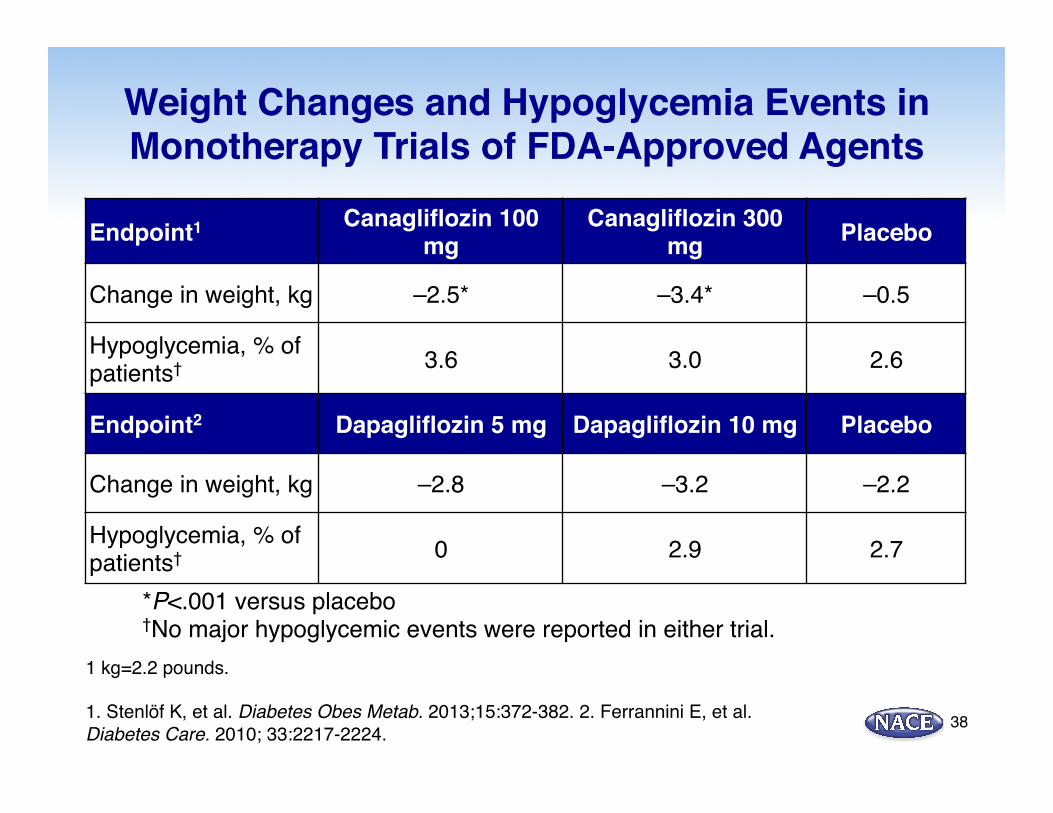
Weight Changes and Hypoglycemia Events in Monotherapy Trials of FDA-Approved Agents
Endpoint1 Canagliflozin 100 mg
Canagliflozin 300 mg Placebo
Change in weight, kg –2.5* –3.4* –0.5
Hypoglycemia, % of patients† 3.6 3.0 2.6
Endpoint2 Dapagliflozin 5 mg Dapagliflozin 10 mg Placebo
Change in weight, kg –2.8 –3.2 –2.2
Hypoglycemia, % of patients† 0 2.9 2.7
1 kg=2.2 pounds.
1. Stenlöf K, et al. Diabetes Obes Metab. 2013;15:372-382. 2. Ferrannini E, et al. Diabetes Care. 2010; 33:2217-2224.
*P<.001 versus placebo†No major hypoglycemic events were reported in either trial.
38
Clinical Attributes of SGLT2 Inhibitors: Metabolic Effects
§ Blood pressure: ↓ both SBP and DBP1-3
§ Lipids§ Small, generally non clinically relevant ↑ LDL-C4,5
§ Small ↓ TRG3
§ Small ↑ HDL3,5
§ Renal§ Small transient (1-4 weeks) ↓ eGFR returns to
baseline.
1. Clar C, et al. BMJ Open. 2012;2:e001007. 2. Stenlöf K, et al. Diabetes Obes Metab. 2013;15:372-382. 3. Bailey CJ, et al. Lancet. 2010;375:2223-2233. 4. Farxiga (dapagliflozin). Package insert. Princeton, NJ: Bristol-Myers Squibb; 2014. 5. Invokana (canagliflozin). Package insert. Titusville, NJ: Janssen Pharmaceuticals; 2013. Warner C, et al. NEJM. DOI: 10.1056/NEJMoa1515920
Clinical Attributes of SGLT2 Inhibitors: Cardiovascular Outcome Trial With Empagliflozin
Study Design
§ Multicenter, randomized, double blind, placebo controlled trial comparing the effect of CV outcomes between empagliflozin 10 & 25 mg with placebo
§ Background therapy was continued, but pts were randomized following a 2 week placebo run-in phase
§ Drug naiive pts had A1C > 7.0 to < 9.0 at screening
§ Subjects on background meds had A1C > 7.0 to < 10.0 at screening
§ Pts had to be high risk for CV events
§ Primary endpoint was first occurrence of CV death, non-fatal MI, or non-fatal stroke
Zinman B, et al. Cardiovasc Diabetol. 2014 ;13:102. Zinman B, et al. N Engl J Med. 2015 Sep 17. [Epub ahead of print]
EMPA-REG OUTCOME Trial
40
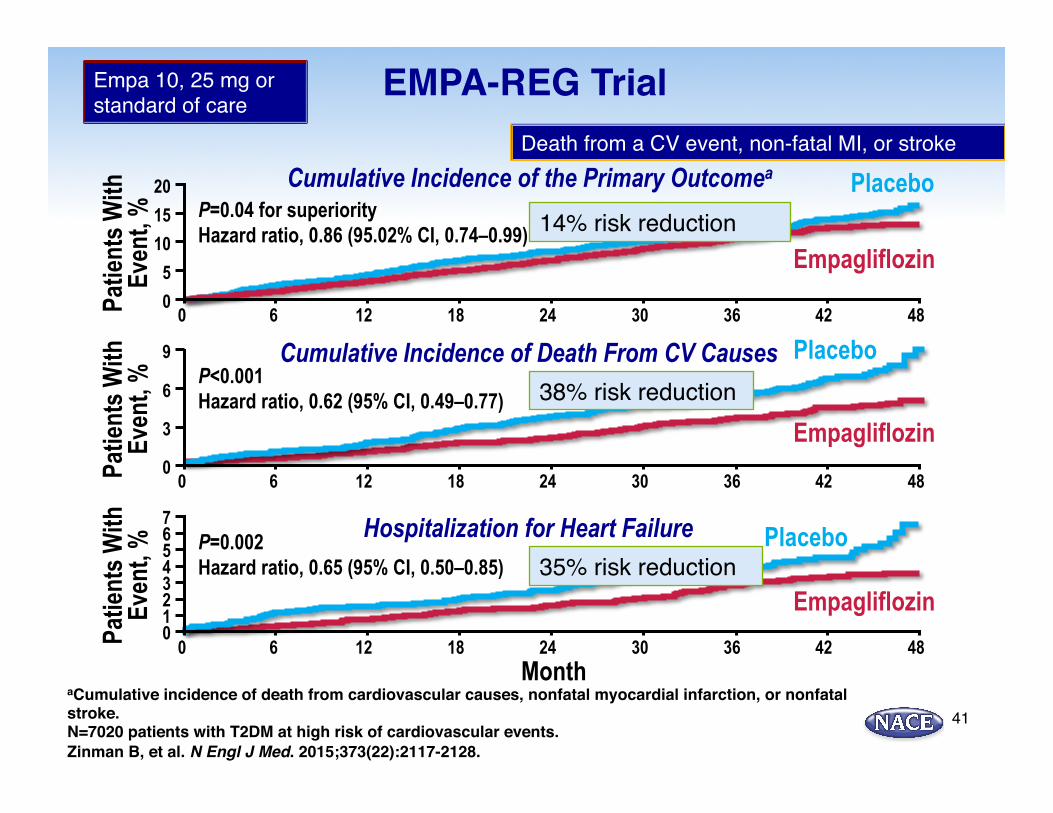
EMPA-REG Trial
aCumulative incidence of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke.N=7020 patients with T2DM at high risk of cardiovascular events.Zinman B, et al. N Engl J Med. 2015;373(22):2117-2128.
Patie
nts W
ith
Even
t, %
Empagliflozin
P=0.04 for superiority Hazard ratio, 0.86 (95.02% CI, 0.74–0.99)
Placebo 20 15
5 10
0 0 12 6 18 24 30 36 42 48
Cumulative Incidence of the Primary Outcomea
Patie
nts W
ith
Even
t, %
Empagliflozin
P<0.001 Hazard ratio, 0.62 (95% CI, 0.49–0.77)
Placebo 9
3
6
0 0 12 6 18 24 30 36 42 48
Cumulative Incidence of Death From CV Causes
Patie
nts W
ith
Even
t, %
Empagliflozin
P=0.002 Hazard ratio, 0.65 (95% CI, 0.50–0.85)
Placebo 7 6 4 5
0 0 12 6 18 24 30 36 42 48
Month
Hospitalization for Heart Failure
3 2 1
41
38% risk reduction
14% risk reduction
35% risk reduction
Death from a CV event, non-fatal MI, or stroke
Empa 10, 25 mg or standard of care
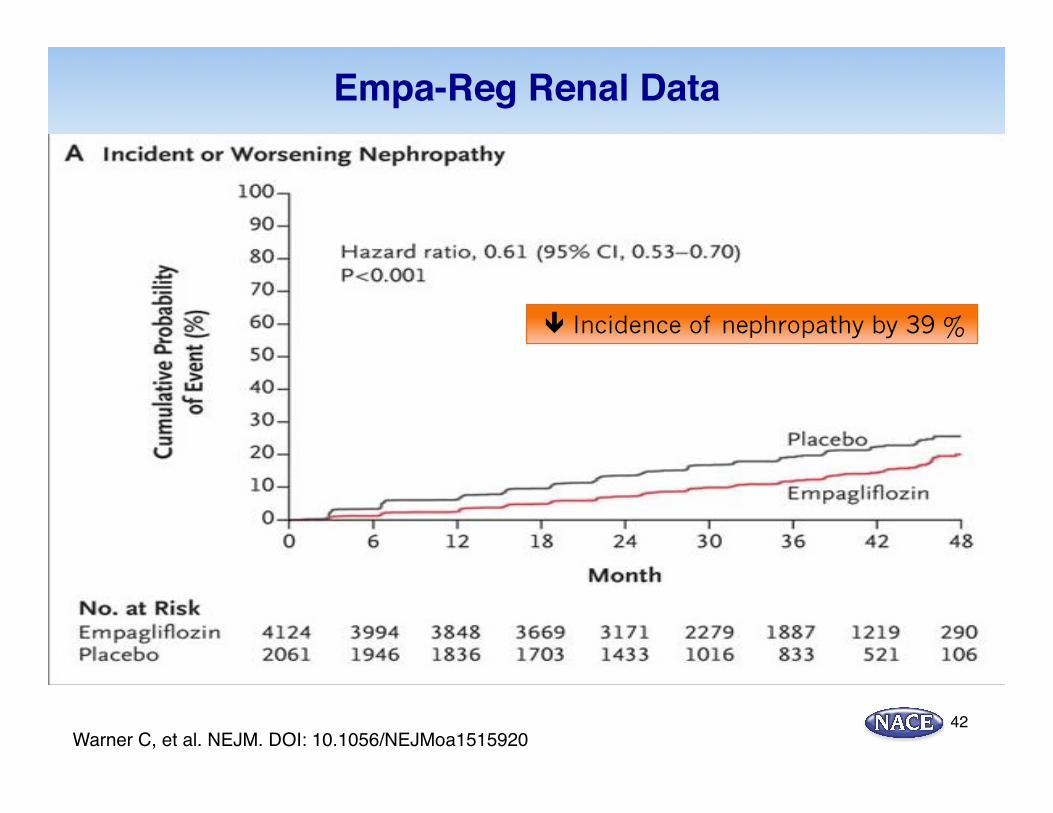
Empa-Reg Renal Data
Warner C, et al. NEJM. DOI: 10.1056/NEJMoa151592042
ê Incidence of nephropathy by 39 %
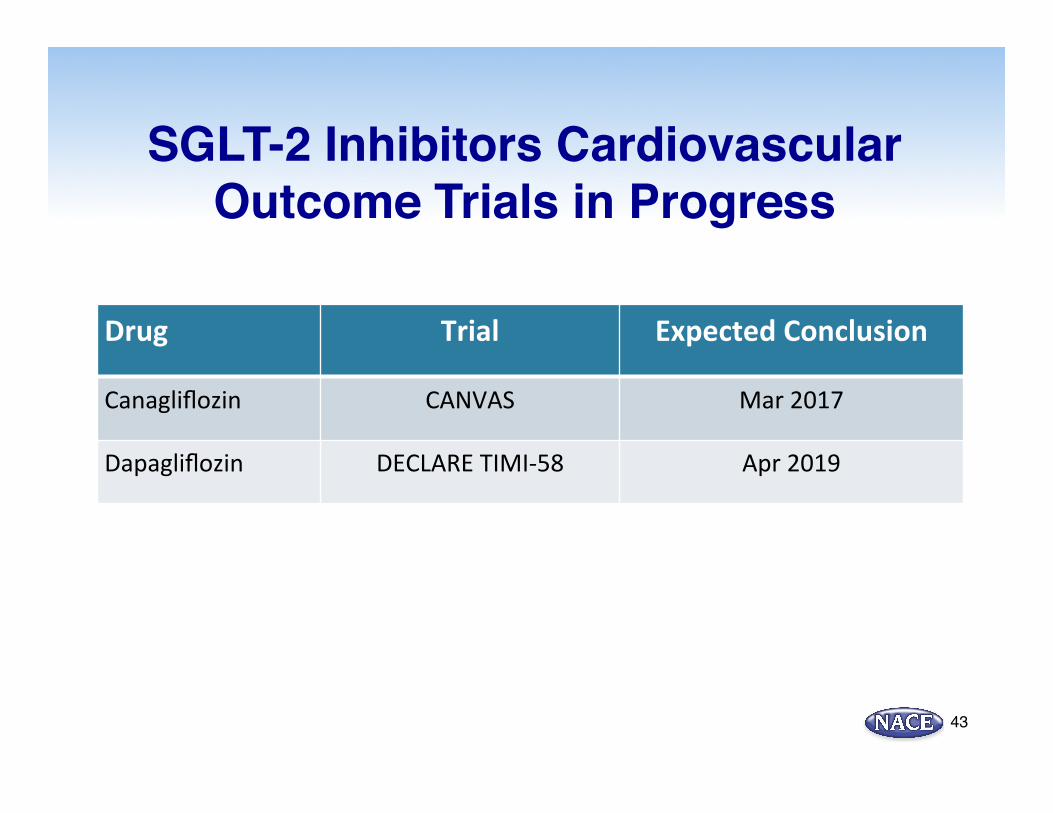
SGLT-2 Inhibitors Cardiovascular Outcome Trials in Progress
43
Drug Trial Expected Conclusion
Canagliflozin CANVAS Mar 2017
Dapagliflozin DECLARE TIMI-‐58 Apr 2019
LEADER CV Outcomes Trial§ Double-blind, placebo controlled randomized trial evaluating
the safety and efficacy of liraglutide vs. placebo (1:1) in pts with T2DM
§ A1C > 7 %
§ Inclusion criteria: > Age 50, at least 1 CV precondition (PVD, CKD stage 3 or greater, NYHA class II-III, microalbuminuria, LVH, ABI < 0.9, no prior usage of a GLP-1 RA.
§ 9340 randomized patients. Retention rate over 5 years was 99 %
§ Primary outcome was time to1st occurrence of death from CV causes, nonfatal MI, nonfatal stroke, coronary revascularization, unstable angina, new onset macroalbumiuria
44Marso SP, et al. NEJM. 6/13/16. DOI 10.1056NEJ Moa1603827
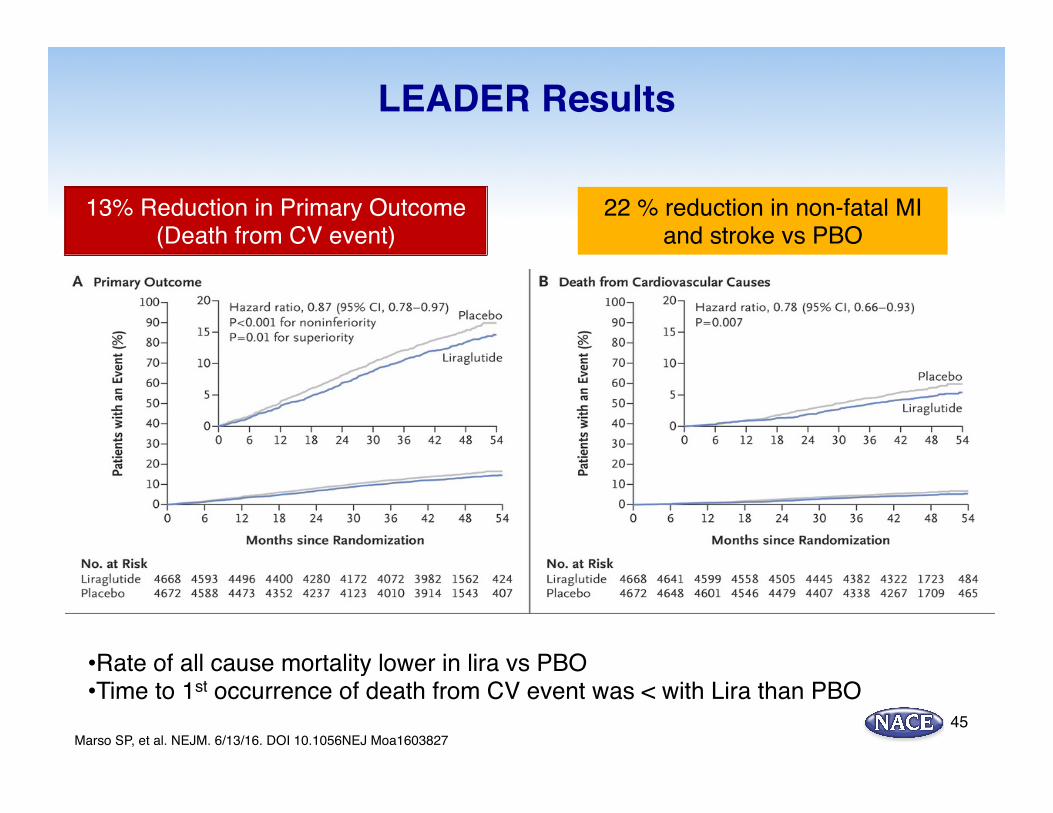
LEADER Results
45
• Rate of all cause mortality lower in lira vs PBO• Time to 1st occurrence of death from CV event was < with Lira than PBO
13% Reduction in Primary Outcome (Death from CV event)
Marso SP, et al. NEJM. 6/13/16. DOI 10.1056NEJ Moa1603827
22 % reduction in non-fatal MI and stroke vs PBO
Patient Case 2: Felicia - A Challenging Patient
§ Felicia is a 56 yo African American woman with a 5 year history of type 2 diabetes. She was initially well controlled on metformin alone, but since a hospitalization 3 years ago for acute systolic CHF (HFrEF) due to hypertensive urgency, her diabetes is difficult to control.
§ She is currently on metformin 1000 mg BID and detemir 70 units am
46
Felicia: A Challenging Patient
§ PMH : Fracture of left femur 2012
§ Hypertension
§ Idiopathic microhematuria
§ Pancreatitis 1998 felt due to cholelithiasis
§ Meds: Metformin 1000 mg bid, detemir 70u qam, metoprolol tartrate 100mg bid, losartan 100mg qam, furosemide 40mg BID, amlodipine 5mg qd, atorvastatin 20mg
47
Felicia: The Challenging Patient
§ PE: Height 5ft 6 in, wt 210lb BMI 33.9
§ BP 126/86 P 72
§ Physical exam is normal except for an S4 and trace peripheral edema.
§ Labs : HGB A1c 7.7% Creatinine 1.45 eGFR48 Albumin/creatinine 68 mcg/mg
48
Which of the following statements are false?
1. SGLT-2 inhibitors should not be used in a patient with history of fractures
2. Incretin based therapy would be a good option for postprandial control in this patient
3. Pioglitazone would be an effective add-on therapy in this patient
4. All of the above
49
ARS QUESTION
Which of the following complications of SGLT-2 therapy is the patient most at risk for?
1. Recurrent fracture
2. Ketoacidosis
3. Bladder Cancer
4. Orthostatic Hypotension
5. AKI (Acute kidney injury)
50
ARS QUESTION
Safety and Tolerability§ Common adverse events include slight increase versus placebo in rate of:
§ Urinary tract infections (~5% to 10%)1-8
§ Genital tract infections (~8% to 10%)1-8 § Generally not serious and easily managed
• Renal dosing considerations9,10,11
§ Dapagliflozin contraindicated for patients with eGFR <60 mL/min/1.73 m2
§ Canagliflozin: Limit dose to 100 mg in patients with eGFR 45 to <60 mL/min/1.73 m2 contraindicated at eGFR <45 mL/min/1.73 m2. Potential for hypovolemic events, particularly in elderly patients or patients with renal impairment
§ Empagliflozin should be discontinued in patients with a persistent eGFR less than 45 mL/min/1.73 m2
§ Should not be used for patients with active bladder cancer9
§ Safe/well-tolerated when added to existing therapy for patients aged >55 years12
1. Bailey CJ, et al. Lancet. 2010;375:2223-2233; 2. Bolinder J, et al. J Clin Endocrinol Metab. 2012;97:1020-1031; 3. Clar C, et al. BMJ Open. 2012;2:e001007; 4. List JF, et al. Diabetes Care. 2009;32:650-657; 5. Rosenstock J, et al. Diabetes Care. 2012;35:1232-1238; 6. Schernthaner G, et al. Diabetes Care. 2013;36:2508-2515; 7. Stenlöf K, et al. Diabetes Obes Metab. 2013;15:372-382; 8. Wilding JP, et al. Diabetes Care. 2009;32:1656-1662; 9. Farxiga (dapagliflozin) [package insert]. Princeton, NJ: Bristol-Myers Squibb; 2014; 10. Invokana (canagliflozin) [package insert]. Titusville, NJ: Janssen Pharmaceuticals; 2013; 11. Jardiance (empagliflozin) [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; 2014; 12. Bode B, et al. Hosp Pract (1995). 2013;41:72-84.
51
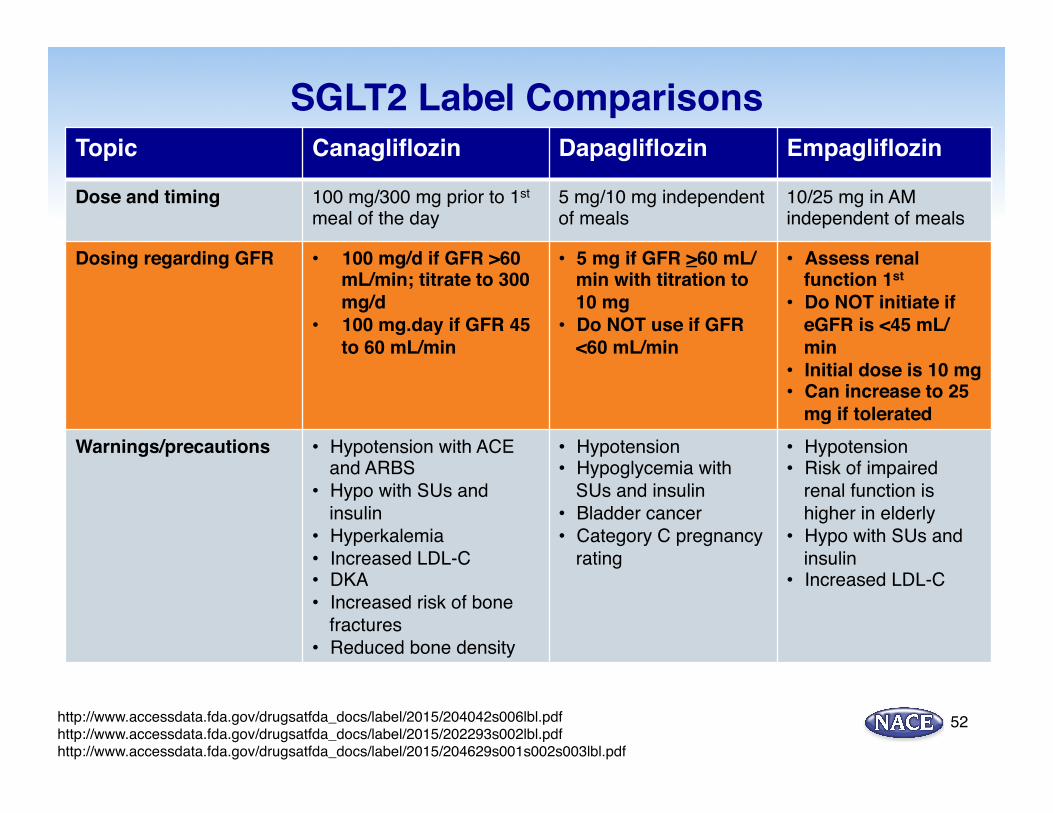
SGLT2 Label Comparisons
http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/204042s006lbl.pdfhttp://www.accessdata.fda.gov/drugsatfda_docs/label/2015/202293s002lbl.pdfhttp://www.accessdata.fda.gov/drugsatfda_docs/label/2015/204629s001s002s003lbl.pdf
Topic Canagliflozin Dapagliflozin Empagliflozin
Dose and timing 100 mg/300 mg prior to 1st meal of the day
5 mg/10 mg independent of meals
10/25 mg in AM independent of meals
Dosing regarding GFR • 100 mg/d if GFR >60 mL/min; titrate to 300 mg/d
• 100 mg.day if GFR 45 to 60 mL/min
• 5 mg if GFR >60 mL/min with titration to 10 mg
• Do NOT use if GFR <60 mL/min
• Assess renal function 1st
• Do NOT initiate if eGFR is <45 mL/min
• Initial dose is 10 mg• Can increase to 25
mg if toleratedWarnings/precautions • Hypotension with ACE
and ARBS• Hypo with SUs and
insulin• Hyperkalemia• Increased LDL-C• DKA• Increased risk of bone
fractures• Reduced bone density
• Hypotension• Hypoglycemia with
SUs and insulin• Bladder cancer• Category C pregnancy
rating
• Hypotension• Risk of impaired
renal function is higher in elderly
• Hypo with SUs and insulin
• Increased LDL-C
52
SGLT 2 Inhibitors and DKA Concerns & ? Mechanisms
Concerns§ 20 cases of DKA in T2DM reported to the FDA Adverse Events Reporting System
3/13-6/14 + 13 published case of euDKA in patients with T1DM and T2DM
§ Most were women
§ 9 cases in T1DM, 4 in T2DM
§ Most cases linked to reduced insulin doses
§ Possible link to increased activity, recent illness, alcohol use, decreased food intake
§ Some patients had no identifying cause
§ All patients responded to IV rehydration and insulin
§ All patients with T1DM should be counseled regarding off label use of SGLT2s
Taylor SI, et al. J Clini Enocrinol Metab. 2015;100 (8):2849-2852. Peters A, et al. Diabetes Care. 2015. doi: 10:2337/dc 15-0843.53
SGLT 2 Inhibitors and DKA Concerns & ? Mechanisms
Taylor SI, et al. J Clini Enocrinol Metab. 2015;100 (8):2849-2852. Peters A, et al. Diabetes Care. 2015. doi: 10:2337/dc 15-0843.
Potential MechanismsSGLT2 Inhibition
Ø Increases glucose renal clearance
Ø Decreases renal clearance of ketone bodies
Ø Endogenous/exogenous insulin levels reduced + dehydration or increased activity level
+Increased in alpha cell secretion of glucagon (mediated by SGLT2)
Ø Increase in lipolysisØ “EuDiabetic Ketoacidosis”
54
Patient Case 4: Christine M – A lean type 2 diabetic
§ Christine M is a 42 yo yoga instructor who developed developed diabetes 9 months after her last pregnancy - 15 years ago. Her mother and grandmother all have diabetes with onset in their early 40s, and both started on insulin in their late 50’s.
§ She was started on metformin 1000mg bid and sitagliptin 100mg qam but most recent A1c was 7.8%
56
Christine M: Clinical data
§ Height 5ft 7”
§ Weight 142 lb
§ BMI 22.2
§ BP 110/62
§ Laboratory data all normal
§ Physical exam normal
§ HGM shows average fasting of 120mg/dl.
57
What is next best step for Christine?
1. Add basal insulin
2. Add an SGLT-2 inhibitor
3. Change DPP-4 to a once weekly GLP-1 analogue
4. Discontinue metformin and add sulfonylurea for postprandial control
5. 2 and 3 and stop metformin58
ARS QUESTION

Rationale for changes in treatment
1) Patient is not insulin resistant. The need/mechanism for metformin isn’t essential
2) The patient’s hyperglycemia is mostly postprandial. Basal insulin may be useful in a relatively insulin deficient patient but not postprandially
3) GLP-1 more potent in beta cell effects than DPP-4 and glucagon suppression (may address NDKA risk)
59
Summary: SGLT2 Inhibitors§ Approved for use in patients with T2DM
§ Benefits§ Glucose control (FPG, PPG, and A1c)§ Weight reduction § BP reduction
§ Adverse effects: predominantly mild and transient§ Thirst, increase in urination frequency, UTI, mycotic infections§ Hypoglycemia risk heightened when used with SUFs or insulin§ Seniors: be vigilant for volume depletion and subsequent
orthostasis§ Monitor Renal Fx (no toxicity with CKD, but lack of efficacy)
§ Fx risk increased 60
POST-TEST QUESTIONS
61
Post-test ARS Question 1
In normal physiologic situations, approximately how many grams of glucose are excreted in the urine each day?
1. 0 g
2. 70 g
3. 125 g
4. 180 g
62
Post-test ARS Question 2
Which of the following adverse events has not been seen with SGLT-2 inhibitors?
1. Increased fracture risk
2. Acute reduction in eGFR
3. Normoglycemic ketoacidosis
4. Congestive Heart Failure
63
Post-test ARS Question 3The patient is a 52-year-old obese African American man with a 7 year history of type 2 diabetes mellitus (HbA1c 8%) and CKD. The decision is made to add an SGLT-2 inhibitor and reinforce lifestyle modifications to control his blood glucose. How should you counsel the patient about his new medication?
1. Explain that his HbA1c will likely decrease 1.5 to 2 percentage points from his current value after beginning the SGLT-2 inhibitor
2. Advise the patient that the new medication may cause a small increase in his blood pressure
3. Warn the patient that the SGLT-2 inhibitor may cause weight gain
4. Counsel patient about the signs and symptoms of orthostatic hypotension which may occur secondary to volume depletion with SGLT-2 inhibitors
64
Post-test ARS Question 4
According to studies using continuous glucose monitoring, approximately what proportion of patients with type 2 diabetes on treatment have unrecognized hypoglycemic episodes?
1. >15%
2. >30%
3. >45%
4. >70%
65
Post-test ARS Question 5
Please rate your confidence in your ability to appropriately use SLGT-2 inhibitors in patients with type 2 diabetes:
1. Not at all confident
2. Slightly confident
3. Moderately confident
4. Pretty much confident
5. Very confident 66
Post-test ARS Question 6
67
Which of the statements below describes your approach to the assessment and management of patients with Diabetes?
1. I do not participate in the assessment and management of patients with Diabetes, nor do I plan to this year.
2. I did not participate in the assessment and management of patients with Diabetes before this course, but as a result of attending this course I’m thinking of doing this now.
3. I do participate in the assessment and management of patients with Diabetes and I now plan to change my treatment methods based on completing this course.
4. I do participate in the assessment and management of patients with Diabetes and this course confirmed that I don’t need to change my methods.