Embed Size (px)
Citation preview

The Journal of Emergency Medicine, Vol. 43, No. 6, pp. 1167–1174, 2012Copyright � 2012 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/$ - see front matter
doi:10.1016/j.jemermed.2012.02.018
RECEIVED: 10 MACCEPTED: 14 F
BriefReports
EMERGENCY PHYSICIANS’ AND NURSES’ ATTITUDES TOWARDSALCOHOL-INTOXICATED PATIENTS
Otis U. Warren, MD,* Victoria Sena, RN,† Esther Choo, MD,* and Jason Machan, PHD†
*Warren Alpert School of Medicine of Brown University, Rhode Island Hospital, The Miriam Hospital, University Emergency MedicineFoundation, Providence, Rhode Island and †Lifespan Foundation, Rhode Island Hospital, Providence, Rhode Island
Reprint Address: Otis U. Warren, MD, Rhode Island Hospital, 593 Eddy Street, Claverick 2, Providence, RI 02903
, Abstract—Background: Emergency physicians andnurses are frequently dissatisfied professionally when treatingalcohol-intoxicated patients, and have negative attitudes to-wards this patient population and alcohol rehabilitation. StudyObjectives: The goal of this study is to examine differences inattitudes between emergency physicians and nurses towardsalcohol-intoxicated patients. Methods: This single-site surveystudy evaluated emergency physicians’ and nurses’: 1) atti-tudes of personal professional satisfaction and dissatisfactionwhen caring for intoxicated patients; 2) attitudes towards thedifficulty in caring for alcohol-intoxicated patients; 3) attitudestowards respect of the alcohol-intoxicated patient; 4) attitudestowards the adequacy of training in caring for intoxicated pa-tients; 5) attitudes towards rehabilitation and counseling ofalcohol-intoxicated patients. Results: Physicians were less sat-isfied and more dissatisfied than nurses when caring foralcohol-intoxicated patients. Physicians found treatingalcohol-intoxicated patients more difficult than nurses did.Physicians were more likely to agree that alcohol-intoxicatedpatients should be treated with respect. Physicians felt moreadequately trained than nurses in caring for alcohol-intoxicated patients. Nurses were more likely to believe thatalcohol-related rehabilitation is ineffective compared withphysicians. Both nurses and physicians refer alcohol-intoxicated patients to rehabilitation to a similar extent.Conclusions: Emergency physicians and nurses have similarattitudes but significant differences in the extent of theseattitudes towards the care of the alcohol-intoxicatedpatient. � 2012 Elsevier Inc.
, Keywords—alcohol; physician; nurse; attitude;emergency
ay 2011; FINAL SUBMISSION RECEIVED: 11 Octobebruary 2012
1167
INTRODUCTION
Alcohol intoxication is common among emergencydepartment (ED) patients. Estimates on the frequencyof intoxication in this population range from 2.5% to30% (1,2). Patients with substance abuse problems aremore likely to present to EDs than to primary caresettings (3,4). This patient population contributessubstantially to ED resource utilization and health careprovider time and effort. This is also a patientpopulation that is difficult to care for, for many reasons.Intoxicated patients can be belligerent, difficult toassess medically, and frequently have concomitantserious medical or traumatic conditions. These reasons,combined with limited alcohol abuse resources, cancontribute to health care provider frustration in caringfor the alcohol-intoxicated patient (5).
Literature supports the effectiveness of brief interven-tions and counseling related to substance abuse (6–8).Recommendations from multiple professional societies(the American Medical Association and the AmericanCollege of Emergency Physicians) advocate the routineuse of these screening tools and subsequent referral forsubstance abuse treatment. A survey of ED physicians in2006 found that 80% of ED physicians thought thattreatment for alcohol problems does not work (5). Addi-tionally, 70% felt angry dealing with patients with alcoholproblems (6). Many of these same attitudes are reflected insurveys of nurses caring for intoxicated patients (9,10).
er 2011;

1168 O. U. Warren et al.
These attitudesmay affect theway that intoxicated patientsare cared for during their stay, and may contribute to theineffectiveness of clinicians in identifying patients withsubstance use problems and referring them to appropriatecounseling (9,11,12). Overall, clinician responses tointoxication may represent a significant barrier to the careof these patients (11,13).
In caring for intoxicated patients, ED nurses and doc-tors have different but overlapping roles. ED nurses, whoperform triage and initial assessments, are often the pro-viders who initially recognize that a patient is intoxicatedand interact with the intoxicated patient. Nurses providemore hands-on care of intoxicated patients than do physi-cians. This often means cleaning, bathing, ensuringpatient comfort, and initial stabilization. In the belliger-ent patient, it is often the nurse’s responsibility tode-escalate the patient, which may result in verbal orphysical aggression directed towards the nurse. TheEmergency Physician, on the other hand, although usu-ally not directly involved with these patient care respon-sibilities, is ultimately responsible for the direction ofmedical care, recognition of underlying medical condi-tions, and bears the large burden of medical liability.Both physician and nurses share the responsibility inreferral for substance abuse counseling.
Multiple barriers to alcohol screening and interventionpractices have been studied (14). However, to our knowl-edge, no previous study has compared attitudes amongphysicians and nurses in the ED towards caring for intoxi-cated patients. Identifying differences in attitudes be-tween physicians and nurses would highlight importantdiscrepancies and allow for a more unified, focusedteam approach in the care of the intoxicated patient.
The goals of this investigation are to compare nurseand physician attitudes towards the care of alcohol-intoxicated patients, including professional satisfaction,difficulties in clinical care, respect towards the patients,preparation for caring for the patients, and referralpractices.
METHODS
Study Design
This was a cross-sectional study of ED physicians andnurses conducted using standardized written surveys.Surveys were administered over a 1-month period inJune of 2010. The research protocol was approved bythe hospital’s Institutional Review Board.
Study Setting and Population
The study was conducted at a high-volume (>100,000visits per year), urban hospital that is a Level I trauma
center and a tertiary referral center. The ED has a 4-yearresidency training program with 12 trainees per year.
Measurements
The survey instrument was based on themes used in priorvalidated surveys and our observations of the practice ofemergency physicians and nurses (15–17). The fullsurveys can be found in the Appendix. Questions weredesigned to assess eight themes regarding the care ofthe alcohol-intoxicated patient; 1) professional satisfac-tion, 2) professional dissatisfaction, 3) perceived diffi-culty of the clinical evaluation, 4) respect of thealcohol-intoxicated patient, 5) adequacy of training, 6)willingness to train, 7) rehabilitation referral practices,8) negative attitudes towards rehabilitation. All survey re-sponses were based on a five-point Likert scale witha score of 1 corresponding to ‘‘Strongly agree with thestatement,’’ 3 being ‘‘Neutral,’’ and 5 corresponding to‘‘Strongly disagree with the statement.’’
Surveys were administered during a sampling of day,evening, and overnight shifts. Surveys were distributedto all nurses in attendance at pre-shift clinical rounds.Physicians were approached on an individual basis byresearch staff either before or after the ED shift. Surveyrespondents were not aware that this survey would beused to compare responses between physicians andnurses. Surveys were not distributed to non-EmergencyMedicine residents or fellows rotating through the EDfrom other specialties. Research staff provided verbal in-formed consent. Upon completion, surveys were placedanonymously in a drop box. There was no compensationfor completing the surveys.
Data Analysis
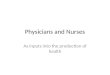
For analysis purposes, the Likert scale was treated asa continuous variable. A modified, multi-trait/multi-method matrix was constructed to assess correlationbetween questions within the same theme group(Figure 1). Responses from individual questions withintheme groups were combined to compare overall differ-ences between nurses’ and physicians’ responses in thesespecific themes; t-test analysis was performed on thesedata. Comparisons between nurses’ and physicians’ re-sponses to individual questions about the sedation ofthe alcohol-intoxicated patient were also made via t-testanalysis. Physicians’ and nurses’ data were combinedwhen analyzing questions related to the respect of thealcohol-intoxicated patient. Comparisons between ques-tions related to respect were made via t-test analysis ofthese combined (MD and RN) data.

Figure 1. Modified multi-trait/multi-method matrix.
MD and RN Attitudes towards Alcohol Patients 1169
RESULTS
General
Among the nurses, the response rate was 73% (58 of 80receiving the survey). Among physicians, the responserate was 65% (39 of 60 receiving the survey). Of the phy-sicians completing the survey, 59% were residents and41% were attendings. Of the nurses completing the sur-vey, 67% were full time and 33% were part time, witha median experience range of 5–8 years.
Attitudes towards Professional Satisfaction whenTreating Alcohol-intoxicated Patients (Table 1,Themes 1 and 2)
In Themes 1 and 2 (Table 1), physicians and nurses wereasked a series of questions related to their personal pro-fessional satisfaction or dissatisfaction when treatingalcohol-intoxicated patients. Agreement with the state-ments in Theme 1 reflected that they were generally sat-isfied professionally when treating alcohol-intoxicatedpatients. Agreement with the statements in Theme 2
reflected that participants were generally dissatisfied pro-fessionally when treating alcohol-intoxicated patients.Overall, both nurses and physicians disagreed with ques-tions asking if they were professionally satisfied whentreating alcohol-intoxicated patients. However, physi-cians disagreed significantly more than nurses (meanLikert scores: MD 3.57 [95% confidence interval (CI)3.45–3.75], RN 3.23 [95% CI 3.09–3.38]). Both nursesand physicians agreed with questions asking if theywere dissatisfied with treating alcohol-intoxicated pa-tients, with physicians agreeing significantly more thannurses (mean Likert scores: MD 2.44 [95% CI 2.27–2.61], RN 2.69 [95% CI 2.54–2.85]).
Attitudes towards the Difficulty of the Evaluation of theAlcohol-intoxicated Patient (Table 1, Theme 3)
In Theme 3, physicians and nurses were asked a series ofquestions that assessed their attitudes about whether thealcohol-intoxicated patient is difficult to evaluate. Bothnurses and doctors agreed that the alcohol-intoxicatedpatient is difficult to evaluate, with physicians agreeing

Table 1. Comparison of Physicians’ and Nurses’ Mean Likert Scores for Question Themes
MD RN
Mean Likert Score(95% CI)
Mean Likert Score(95% CI)
Theme 1 3.57 (3.45–3.70) 3.23 (3.09–3.28) Agreement reflects satisfaction treating ETOH patientsTheme 2 2.44 (2.27–2.61) 2.69 (2.54–2.85) Agreement reflects dissatisfaction treating ETOH patientsTheme 3 2.37 (2.22–2.51) 2.60 (2.46–2.75) Agreement reflects clinical difficulty in treating ETOH patientsTheme 4 1.62 (1.47–1.75) 1.99 (1.82–2.15) Agreement reflects a belief that ETOHpatients should be treatedwith
respectTheme 5 2.51 (2.29–2.37) 3.16 (2.96–3.35) Agreement reflects a belief that respondents have received adequate
training in treating ETOH patientsTheme 6 2.32 (2.14-2.51) 2.35 (2.29-2.60) Agreement reflects a belief that more trainingwould improve the care
of ETOH patientsTheme 7 2.41 (2.21-2.61) 2.59 (2.40-2.79) Agreement reflects frequent referral to ETOH rehabilitationTheme 8 3.50 (3.30-3.70) 3.16 (2.95-3.38) Agreement reflects a belief that ETOH rehabilitation does not work
CI = confidence interval; ETOH = alcohol.Theme numbers are located in column 1, with a description of what agreement with the theme reflects in column 4.Mean Likert scoreswith95% confidence interval are listed for each theme for physicians and nurses in columns 2 and 3, respectively.
1170 O. U. Warren et al.
non-significantly more so than nurses (mean Likertscores: MD 2.37 [95% CI 2.22–2.51], RN 2.60 [95% CI2.46–2.75]).
Attitudes towards Respect of the Alcohol-intoxicatedPatient (Table 1, Theme 4)
In Theme 4, physicians and nurses were asked a series ofquestions that assessed whether they felt that alcohol-intoxicated patients should be treated with respect.Overall, both physicians and nurses agreed with thesestatements, with physicians agreeing significantly moreso than nurses (mean Likert scores: MD 1.62 [95% CI1.47–1.75], RN 1.99 [95% CI 1.83–2.15]).
Although physicians and nurses generally agreed withstatements that alcohol-intoxicated patients deserve to betreated with respect, they disagreed with the statement,‘‘alcohol-intoxicated patients ARE treated with respect.’’The combined (RN and MD) mean Likert score for the firststatement (Question 17) was 1.70 (95% CI 1.57–1.83)versus the second statement, mean Likert score of 3.23(95% CI 3.05–3.41). Note that this survey question wasnot used in the thematic analysis for Theme 4 and was an-alyzed separately.
Attitudes on Training in the Care of theAlcohol-intoxicated Patient (Table 1, Themes 5 and 6)
In Theme 5, physicians and nurses were asked a series ofquestions that assessed whether they felt they receivedadequate training in the care of the alcohol-intoxicatedpatient. Physicians generally agreed with statementsthat they received adequate training, whereas nurseswere generally neutral (mean Likert scores: MD 2.51[95% CI 2.29–2.73], RN 3.16 [95% CI 2.96–3.35]). In
Theme 6, physicians and nurses both agreed to a similarextent with statements that more training would improvethe care of alcohol-intoxicated patients (mean Likertscores: MD 2.32 [95% CI 2.14–2.51], RN 2.35 [95% CI2.29–2.60]).
Attitudes and Practice towards Alcohol-relatedCounseling and Rehabilitation (Table 1, Themes 7 and 8)
In Theme 7, physicians and nurses were asked a series ofquestions related to the referral of alcohol-intoxicatedpatients to rehabilitation and counseling. Physicians andnurses generally refer patients to rehabilitation/counsel-ing to similar extents (mean Likert scores MD 2.41 [95%CI 2.21–2.61], RN 2.59 [95% CI 2.40–2.79]). When askedif they feel as if alcohol rehabilitation does not work(Theme 8), physicians tended to disagree and nurseswere generally neutral (mean Likert scores: MD 3.50[95% CI 3.30–3.70], RN 3.16 [95% CI 2.95–3.38]).
Attitudes towards the Sedation of Alcohol-intoxicatedPatients
When asked if they agreed with the statement, ‘‘I prefermy alcohol-intoxicated patients to be medically sedated,’’physicians and nurses had generally similar responses,with a trend toward disagreement with this statement(mean Likert scores: MD 3.51 [95% CI 3.86–3.17], RN
3.39 [95% CI 3.72–3.07]). When physicians and nurseswere asked if they felt that the other group preferred theirpatients to be sedated (i.e., nurses were asked if physi-cians preferred their patients to be sedated and physicianswere asked if nurses preferred their patients to be se-dated), physicians agreed with this statement and nursesdisagreed with this statement (mean Likert scores: MD

Table 2. Subgroup Comparison of Attendings’ and Residents’ Mean Likert Scores for Question Themes
Attending (n = 16) Resident (n = 23)
Mean Likert Score(95% CI)
Mean Likert Score(95% CI)
Theme 1 3.46 (3.25–3.67) 3.68 (3.53–3.84) Agreement reflects satisfaction treating ETOH patientsTheme 2 2.56 (2.28–2.83) 2.35 (2.14–2.56) Agreement reflects dissatisfaction treating ETOH patientsTheme 3 2.41 (2.17–2.64) 2.34 (2.15–2.52) Agreement reflects clinical difficulty in treating ETOH patientsTheme 4 1.69 (1.47–1.89) 1.56 (1.37–1.75) Agreement reflects a belief that ETOHpatients should be treatedwith
respectTheme 5 2.18 (1.80–2.56) 2.74 (2.50–2.98) Agreement reflects a belief that respondents have received adequate
training in treating ETOH patientsTheme 6 2.56 (2.25-2.88) 2.16 (1.94-2.38) Agreement reflects a belief that more trainingwould improve the care
of ETOH patientsTheme 7 2.28 (1.97-2.59) 2.50 (2.23-2.77) Agreement reflects frequent referral to ETOH rehabilitationTheme 8 3.53 (3.25-3.81) 3.48 (3.20-3.76) Agreement reflects a belief that ETOH rehabilitation does not work
CI = confidence interval; ETOH = alcohol.Theme numbers are located in column 1, with a description of what agreement with the theme reflects in column 4.Mean Likert scoreswith95% confidence interval for the Attendings and Residents are listed in columns 2 and 3, respectively.
MD and RN Attitudes towards Alcohol Patients 1171
2.46 [95% CI 2.78–2.14], RN 3.47 [95% CI 3.73–3.23].Said differently, physicians and nurses demonstrated sim-ilar attitudes towards the sedation of intoxicated patients.However, physicians perceived that nurses wanted theirpatients sedated more than nurses actually stated wantingtheir patients sedated.
Attitudes Based on Experience (Tables 2, 3)
In sub-group analysis, we found no statistical differencebetween the attitudes of residents and attendings sur-veyed. Theme 5, which asks whether respondents feltthey have received adequate training in the care ofalcohol-intoxicated patients, approached statistical sig-nificance (Table 2). Similarly, there were no significantdifferences between more experienced nurses (> 8 years)and less experienced nurses (# 8 years) (Table 3).
Table 3. Subgroup Comparison of More Experienced (>8 Years) wifor Question Themes
More Experienced(n = 25)
Less Experienced(n = 33)
Mean Likert Score(95% CI)
Mean Likert Score(95% CI)
Theme 1 3.52 (3.33–3.71) 3.62 (3.44–3.79) AgTheme 2 2.92 (2.67–3.17) 2.52 (2.33–2.71) AgTheme 3 2.82 (2.60–3.04) 2.44 (2.26–2.63) AgTheme 4 1.88 (1.68–2.12) 2.08 (1.86–2.29) Ag
rTheme 5 2.94 (2.63–3.25) 3.32 (3.07–3.57) Ag
tTheme 6 2.62 (2.36-2.88) 2.32 (2.13-2.52) Ag
oTheme 7 2.72 (2.42-3.02) 2.50 (2.23-2.77) AgTheme 8 3.36 (3.03-3.69) 3.02 (2.72-3.31) Ag
CI = confidence interval; ETOH = alcohol.Theme numbers are located in column 1, with a description of what agre95% confidence interval for the more experienced and less experience
DISCUSSION
In general, we found that nurses and physicians had sim-ilar attitudes in caring for alcohol-intoxicated patients.Most significant differences we identified between thegroups were more a matter of the degree of the attitude.These differences, although statistically different, likelydo not reflect a clinical difference. ED physicians andnurses expressed professional dissatisfaction when treat-ing alcohol-intoxicated patients, with physicians express-ing significantly more dissatisfaction. On average,providers felt that alcohol-intoxicated patients deserveto be treated with respect, but felt that these patientswere not, in actual practice, treated with respect.
We also found that physicians reported greater diffi-culty caring for the intoxicated patient than nurses. Thesedifferences were unexpected, given that nurses generally
th Less Experienced (#8 Years) Nurses’ Mean Likert Scores
reement reflects satisfaction treating ETOH patientsreement reflects dissatisfaction treating ETOH patientsreement reflects clinical difficulty in treating ETOH patientsreement reflects a belief that ETOHpatients should be treatedwithespectreement reflects a belief that respondents have received adequateraining in treating ETOH patientsreement reflects a belief that more trainingwould improve the caref ETOH patientsreement reflects frequent referral to ETOH rehabilitationreement reflects a belief that ETOH rehabilitation does not work
ement with the theme reflects in column 4.Mean Likert scoreswithd nurses are listed in columns 2 and 3, respectively.

1172 O. U. Warren et al.
have more face-to-face time with patients, thus will bearthe larger burden of de-escalating, cleaning, comfort care,and provider-directed verbal or physical abuse that can berelated with the care of intoxicated individuals. Given thelarge volume of alcohol-related ED visits, this may pro-vide a burden on the psyche of providers (18,19).
We found that although ED physicians and nurses bothagreed that alcohol-intoxicated patients should be treatedwith respect, both groups also agreed that these patientsare not treated with respect. This is a clear discrepancy be-tween what providers feel should be done and what pro-viders actually do. Interestingly, nurses and physiciansagreed with each other in regards to this discrepancy, andthe question remains:Whyare alcohol-intoxicated patientsnot treated with respect given that both nurses and physi-cians feel that they should be? This discrepancy indicatessomebreakdown of compassionate care of the patient. Fur-ther research is needed to examine specific components ofcare that may be lacking for alcohol-intoxicated patientsand associations between these attitudes and lack of inter-ventions and referral for alcohol abuse.
Prior work has demonstrated that ED physician atti-tudes towards their role in a brief intervention correlatedwith referral patterns (6). Here we find similar resultsamong physicians’ attitudes towards the effectiveness ofalcohol rehabilitation, in that, physicians tended to dis-agree with statements about the ineffectiveness of alcoholrehabilitation. Nurses, however, were more neutral on theeffectiveness of alcohol rehabilitation. This difference inattitude may represent a barrier for screening and brief in-tervention practices. During an ED visit, an alcohol-intoxicated patient will likely be seen by at least one nurseand one physician. Our data suggest that there will likelybe differing attitudes within that single ED visit. One po-tential solution to this problem is to implement departmen-tal standardized screening and referral policies, which areestimated to exist currently in only 15% of EDs (14).
We wished to test the perception that nurses prefer thealcoholic patient to be medically sedated and that physi-cians were reluctant to provide the sedation. If true, thistension could represent a barrier to the collaborativecare of the alcohol-intoxicated patient between nursesand physicians. However, we found that physicians andnurses have similar attitudes regarding sedation and thatphysicians were largely mistaken in believing that thenurses would prefer their patients sedated.
Limitations
This study was conducted at a single site, which limits thegeneralizability of the results. Being a single-center studyensures, however, that differences in attitudes are not re-lated to differing populations of patients. Additionally,the themes of the questions asked are similar to themes
used in prior research on provider attitudes in treatingalcohol-intoxicated patients (5,9,11,13,15–17).
Response rate was low among surveys distributed tophysicians. This has the potential to increase selectionbias compared with the higher response rate of the nurses.In addition, 59% of the physician surveys were completedby residents, which could limit this study’s generalizabil-ity to other non-teaching practices. However, there wereno significant differences between the attending and res-ident responses (Table 2).
When analyzing the data, the survey questions weregrouped according to themes, as opposed to individualquestions. Although the questions within each theme gen-erally had better correlation with each other than withother themes, there was also correlation of questionsfrom different theme groups (Figure 1). This is likelydue to the interrelated nature of many of the themes.For instance, it is logical that a correlation exists betweennegative attitudes about professional satisfaction and per-ceived difficulty in caring for intoxicated patients.
CONCLUSIONS
ED nurses and physicians have many similar attitudes inregards to the care of alcohol-intoxicated patients in theED, although they differ as to the extent of these attitudes.These specific areas where differences in attitudes existcould represent a barrier to the collaborative care of thealcohol-intoxicated patient in the ED. Recognizing theextent of the similarities of physicians’ and nurses’ atti-tudes and identifying the few areas where there is a signif-icant difference may be an important step in improvingthe ED care of the alcohol-intoxicated patient.
REFERENCES
1. Person PH Jr. The Drug Abuse Warning Network: a statistical per-spective. Public Health Rep 1976;91:395–402.
2. Li G, Keyl PM, Rothman R, ChanmugamA, Kelen GD. Epidemiol-ogy of alcohol-related emergency department visits. Acad EmergMed 1998;5:788–95.
3. Cherpitel CJ. Drinking patterns and problems: a comparison of pri-mary care with the emergency room. Subst Abus 1999;20:85–95.
4. Cherpitel CJ. Emergency room and primary care services utilizationand associated alcohol and drug use in the United States generalpopulation. Alcohol Alcohol 1999;34:581–9.
5. O’Rourke M, Richardson LD, Wilets I, D’Onofrio G. Alcohol-re-lated problems: emergency physicians’ current practice and atti-tudes. J Emerg Med 2006;30:263–8.
6. D’OnofrioG,DegutisLC.Preventivecare in theemergencydepartment:screening and brief intervention for alcohol problems in the emergencydepartment: a systematic review. Acad Emerg Med 2002;9:627–38.
7. Babor TF, McRee BG, Kassebaum PA, Grimaldi PL, Ahmed K,Bray J. Screening, brief intervention, and referral to treatment(SBIRT): toward a public health approach to the management ofsubstance abuse. Subst Abus 2007;28:7–30.
8. MadrasBK,ComptonWM,AvulaD, StegbauerT, Stein JB,ClarkHW.Screening, brief interventions, referral to treatment (SBIRT) for illicitdrug and alcohol use at multiple healthcare sites: comparison atintake and 6 months later. Drug Alcohol Depend 2009;99:280–95.

*Note: On surveys distributed to physicians, question 28 askedabout nurses and vice-versa on surveys distributed to nurses.
MD and RN Attitudes towards Alcohol Patients 1173
9. Lappalainen-Lehto R, Seppa K, Nordback I. Cutting down sub-stance abuse—present state and visions among surgeons and nurses.Addict Behav 2005;30:1013–8.
10. Lock CA, Kaner E, Lamont S, Bond S. A qualitative study ofnurses’ attitudes and practices regarding brief alcohol interventionin primary health care. J Adv Nurs 2002;39:333–42.
11. Chappel JN, Schnoll SH. Physician attitudes. Effect on the treat-ment of chemically dependent patients. JAMA 1977;237:2318–9.
12. Siegfried N, Ferguson J, Cleary M, Walter G, Rey JM. Experience,knowledgeandattitudesofmental health staff regardingpatients’ prob-lematic drug and alcohol use. Aust N Z J Psychiatry 1999;33:267–73.
13. Lindberg M, Vergara C, Wild-Wesley R, Gruman C. Physicians-in-training attitudes toward caring for and working with patients withalcohol and drug abuse diagnoses. South Med J 2006;99:28–35.
14. Cunningham RM, Harrison SR, McKay MP, Mello MJ, Sochor M.National survey of emergency department alcohol screening and in-tervention practices. Ann Emerg Med 2010;55:556–62.
15. Chappel JN, Veach TL,KrugRS. The substance abuse attitude survey:an instrument for measuring attitudes. J Stud Alcohol 1985;46:48–52.
16. Tolor A, Tamerin JS. The attitudes toward alcoholism instrument:a measure of attitudes toward alcoholics and the nature and causesof alcoholism. Br J Addict Alcohol Other Drugs 1975;70:223–31.
17. Pillon S, Laranjeira R, Dunn J. Nurses’ attitudes towards alcohol-ism: factor analysis of three commonly used scales. Sao PauloMed J 1998;116:1661–6.
18. Lloyd S, Streiner D, Shannon S. Predictive validity of the emer-gency physician and global job satisfaction instruments. AcadEmerg Med 1998;5:234–41.
19. Goldberg R, Boss RW, Chan L, et al. Burnout and its correlates inemergency physicians: four years’ experience with a wellnessbooth. Acad Emerg Med 1996;3:1156–64.
APPENDIX: SURVEY QUESTIONS
Theme 1: Professional Satisfaction1) I enjoy treating alcohol-intoxicated patients.2) Alcohol-intoxicated patients receive quality care in
the ED.3) I make a difference in the life of alcohol-
intoxicated patient when I care for them in the ED.4) I treat alcohol-intoxicated patients in the ED be-
cause I enjoy working with them.5) I treat alcohol-intoxicated patients in the ED be-
cause I believe I can make a difference in their life.
Theme 2: Professional Dissatisfaction6) The evaluation of an alcohol-intoxicated patient is
more difficult than an equivalent patient who is notintoxicated.
7) I am frustrated by the number of alcohol-intoxicated patients I treat.
8) I would be more satisfied in my career if I treatedless alcohol-intoxicated patients.
9) Alcohol-intoxicated patients are a drain on healthcare resources.
10) I treat alcohol-intoxicated patients in the ED be-cause my job requires me to do so.
Theme 3: Clinical Evaluation11) Bad outcomes happen more frequently to alcohol-
intoxicated patients compared with similar non-intoxicated patients.
12) Alcohol-intoxicated patients receive more diag-nostic tests compared with non-alcohol-intoxicated patients with similar issues.
13) Caring for alcohol-intoxicated patients often dis-tracts from the care of other patients.
14) Alcohol-intoxicated patients receive unnecessaryworkup in the ED.
15) Alcohol-intoxicated patients are verbally andphysically disruptive.
Theme 4: Respect16) Alcohol-intoxicated patients deserve the same
treatment as non-intoxicated patients.17) Alcohol-intoxicated patients deserve to be treated
with respect.Alcohol-intoxicated patients ARE treated withrespect.(This question was not used in the thematic anal-ysis)
Theme 5: Training18) I feel I received adequate training in treating
alcohol-intoxicated patients.19) I feel I am well qualified to treat alcohol-
intoxicated patients.
Theme 6: Willingness to Train20) I am interested in learning new techniques and re-
ceiving more training on how to treat and care foralcohol-intoxicated patients in the ED.
21) Iwould bemorewilling to treat alcohol-intoxicatedpatients in the ED if I had more training.
22) I would be more competent in treating alcohol-intoxicated patients if I received more training.
Theme 7: Rehabilitation Referral Practice23) I refer patients to rehabilitation programs.24) I counsel patients about their drinking habits.
Theme 8: Negative Rehabilitation Attitude25) Counseling alcohol-intoxicated patients in the ED
is a waste of time.26) Referral to rehabilitation programs is a waste of
time for the alcohol-intoxicated patient.
Sedation Questions (See note below)27) I prefer alcohol-intoxicated patients be medically
sedated.28) * (Nurses or Doctors) prefer alcohol-intoxicated
patients to be medically sedated.

1174 O. U. Warren et al.
ARTICLE SUMMARY
1. Why is this topic important?Alcohol-intoxicated patients make up a significant
percentage of patients seen in emergency departments.Physicians and nurses have different roles in caring forthese patients and might have different attitudes towardsthe care of these patients.2. What does this study attempt to show?
This study attempts to show differences and similaritiesbetween physicians’ and nurses’ attitudes towardsalcohol-intoxicated patients.3. What are the key findings?
Physicians and nurses generally have similar attitudestowards alcohol-intoxicated patients in regards to profes-sional satisfaction, respect of the alcohol-intoxicatedpatient, attitudes of alcohol rehabilitation, and adequacyof personal professional training. However, physiciansand nurses differ significantly to the extent of these atti-tudes in several areas. Physicians also overestimatenurses’ desire for sedation of the alcohol-intoxicatedpatient.4. How is patient care impacted?
Patient care can be improved by the recognition of theseattitudes by physician and nurses. This recognition canlead to a more coordinated, focused, team approach in car-ing for the alcohol-intoxicated patient.