Embed Size (px)
Citation preview
Emerging risk factors and markers of CKD progression
Florian KronenbergInnsbruck Medical University, Division of Genetic Epidemiology
CKD: Relevance of the problem
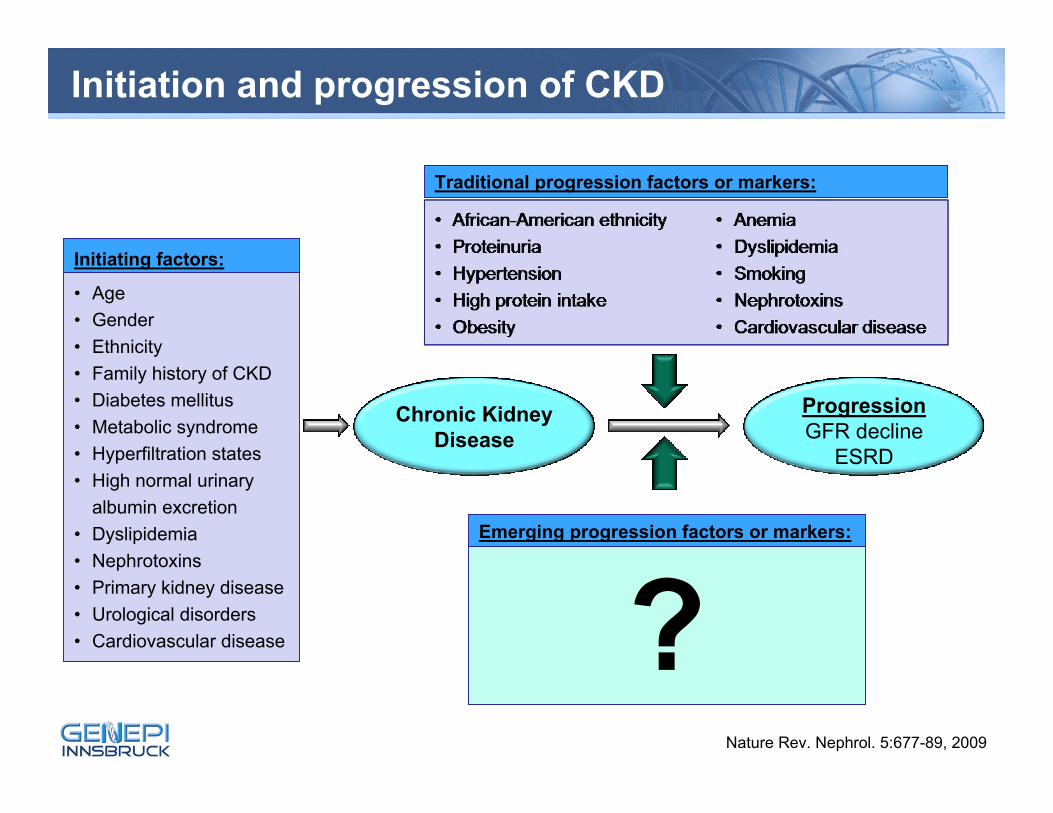
Initiation and progression of CKD
Chronic KidneyDisease
ProgressionGFR decline
ESRD
Traditional progression factors or markers:
• Age• Gender• Ethnicity• Family history of CKD• Diabetes mellitus• Metabolic syndrome• Hyperfiltration states• High normal urinary
albumin excretion• Dyslipidemia• Nephrotoxins• Primary kidney disease• Urological disorders• Cardiovascular disease
Initiating factors:
?Emerging progression factors or markers:
Nature Rev. Nephrol. 5:677-89, 2009
Definition of CKD progression
■ Surrogates of GFR slope ► Doubling of baseline serum creatinine level► Need of renal replacement therapy (dialysis and/or transplantation)► Particular relative increase from baseline serum creatinine level► Yearly or monthly decline in GFR► GFR reduction to 50% of baseline► Graft loss
■ Indices of renal damage► Worsening of proteinuria► Appearance of albuminuria in patients with diabetes
Mild to Moderate Kidney Disease Study
■ 227 patients with primary non-diabetic CKD
■ Patients with nephrotic syndrome excluded
■ Recruited 1996/97
■ Age 46 ± 13 years
■ Iohexol clearance at baseline: average GFR 64 ± 39 ml/min
■ Followed for 7 years
■ Endpoint: doubling of serum creatinine and/or ESRD
■ 177 completed follow-up
■ 65 reached endpoint (36 Crea-doubling, 29 ESRD)
ADMA: Asymetric Dimethylarginine
■ Potent and long-lasting endogenous inhibitor of NO synthase → less NO production
■ NO is a potent vasodilatator and regulator of the vascular tone and blood flow
■ Kidney is the main site of ADMA removal
■ ADMA markedly increased in renal patients
■ High ADMA levels related to atherosclerotic complications
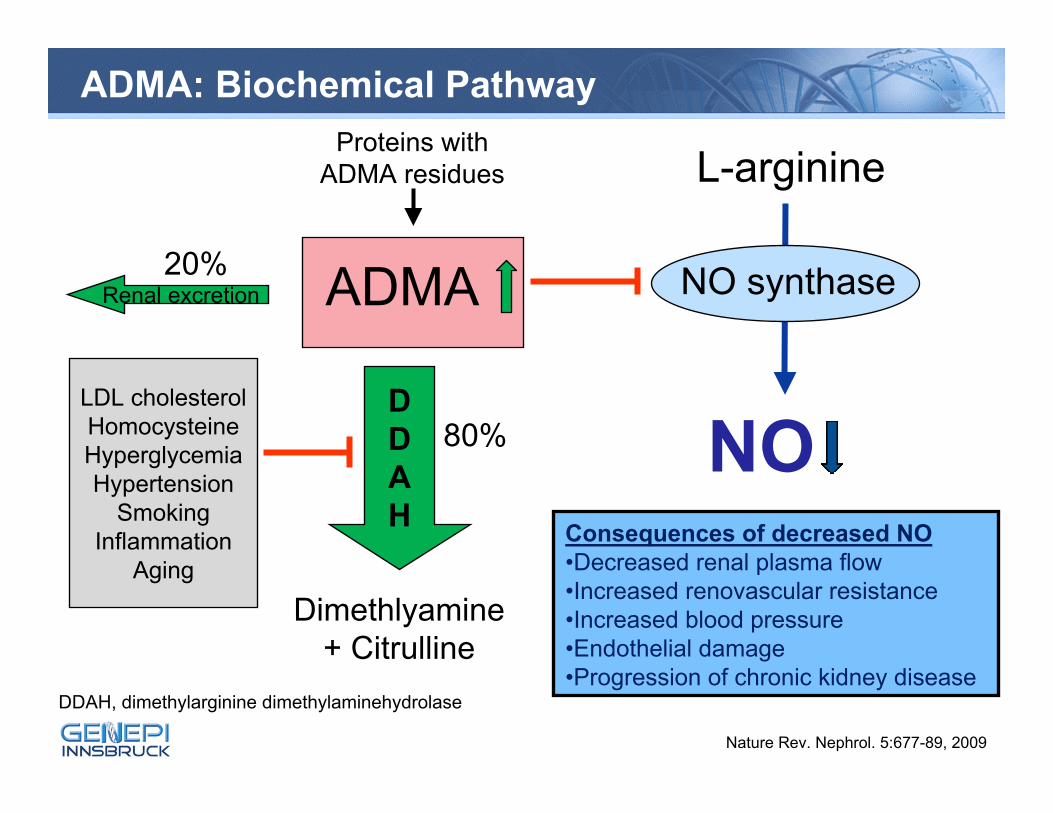
ADMA
L-arginine
NO
NO synthase
DDAH
Dimethlyamine + Citrulline
Renal excretion
LDL cholesterolHomocysteineHyperglycemiaHypertension
SmokingInflammation
Aging
Proteins with ADMA residues
Consequences of decreased NO•Decreased renal plasma flow•Increased renovascular resistance•Increased blood pressure•Endothelial damage•Progression of chronic kidney disease
80%
20%
ADMA: Biochemical Pathway
DDAH, dimethylarginine dimethylaminehydrolase
Nature Rev. Nephrol. 5:677-89, 2009
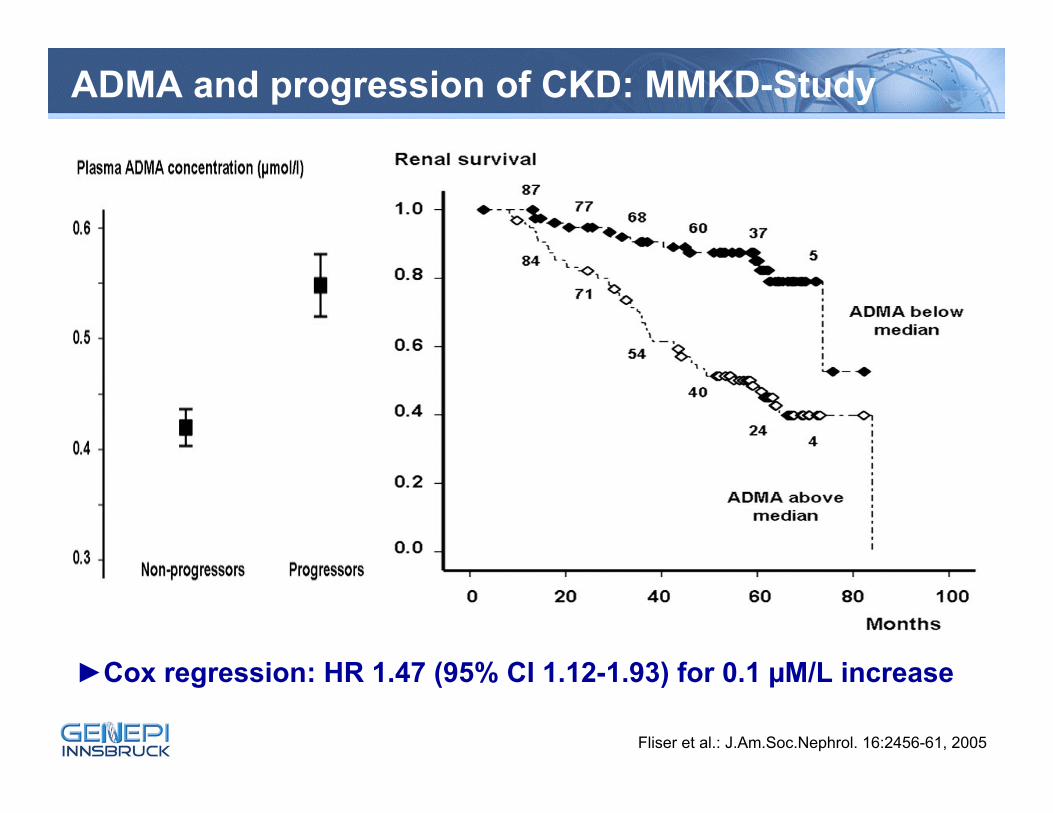
ADMA and progression of CKD: MMKD-Study
►Cox regression: HR 1.47 (95% CI 1.12-1.93) for 0.1 µM/L increase
Fliser et al.: J.Am.Soc.Nephrol. 16:2456-61, 2005
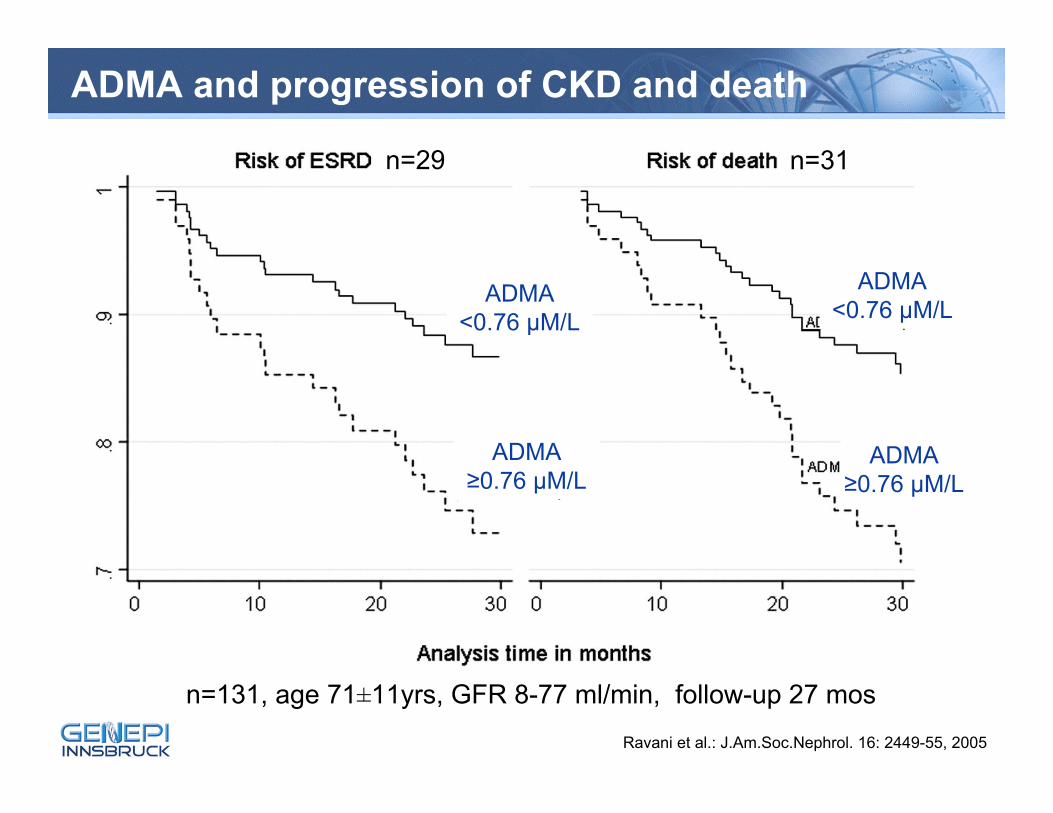
ADMA and progression of CKD and death
Ravani et al.: J.Am.Soc.Nephrol. 16: 2449-55, 2005
ADMA<0.76 µM/L
ADMA≥0.76 µM/L
ADMA<0.76 µM/L
ADMA≥0.76 µM/L
n=131, age 71±11yrs, GFR 8-77 ml/min, follow-up 27 mos
n=29 n=31
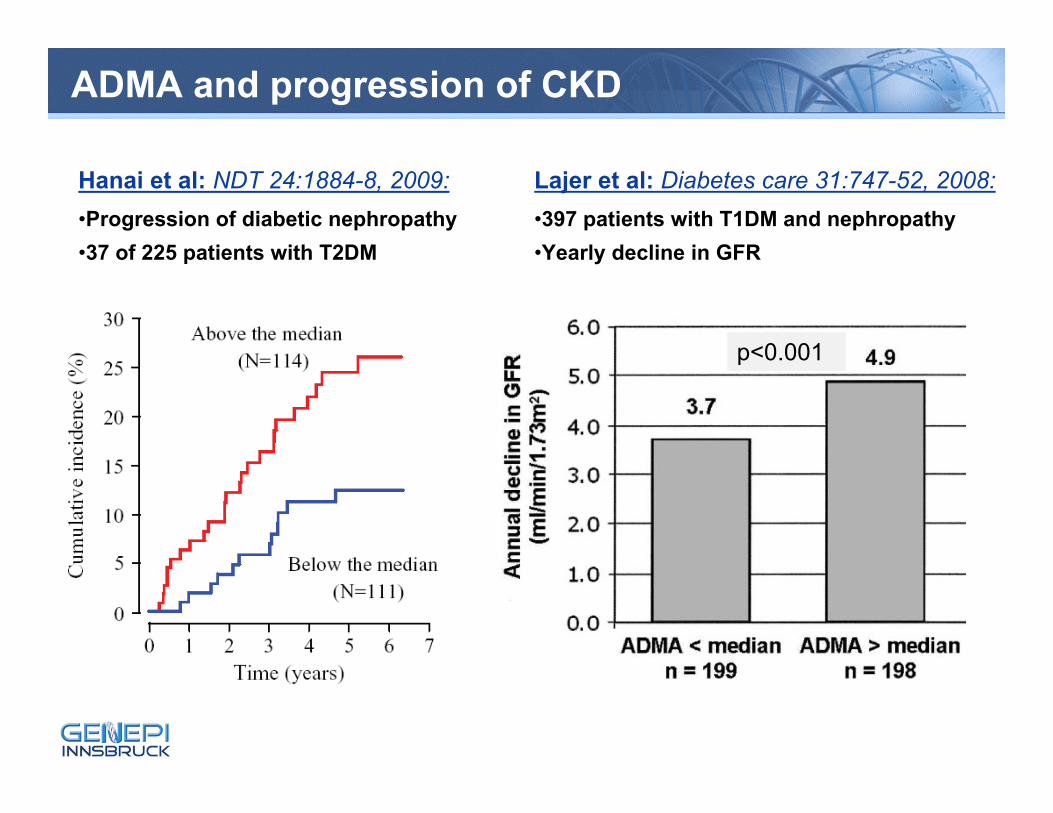
ADMA and progression of CKD
Hanai et al: NDT 24:1884-8, 2009:•Progression of diabetic nephropathy•37 of 225 patients with T2DM
p<0.001
Lajer et al: Diabetes care 31:747-52, 2008:•397 patients with T1DM and nephropathy•Yearly decline in GFR
Calcium-phosphate metabolism
■ Progression of CKD in animal models:► High phosphate► High PTH► Lack of active vitamin D
■ Ca-Ph metabolism and progression of CKD in humans:► High phosphate (5 of 5 studies) and high Ca*Ph (3 of 4 studies)► High PTH levels (2 of 2 studies)
■ Fibroblast Growth Factor 23 (FGF23):► Recently identified “phosphatonin”► Regulator of phosphate balance► Under physiological conditions: high phosphate load results in
increased FGF23 secretion and phosphaturia
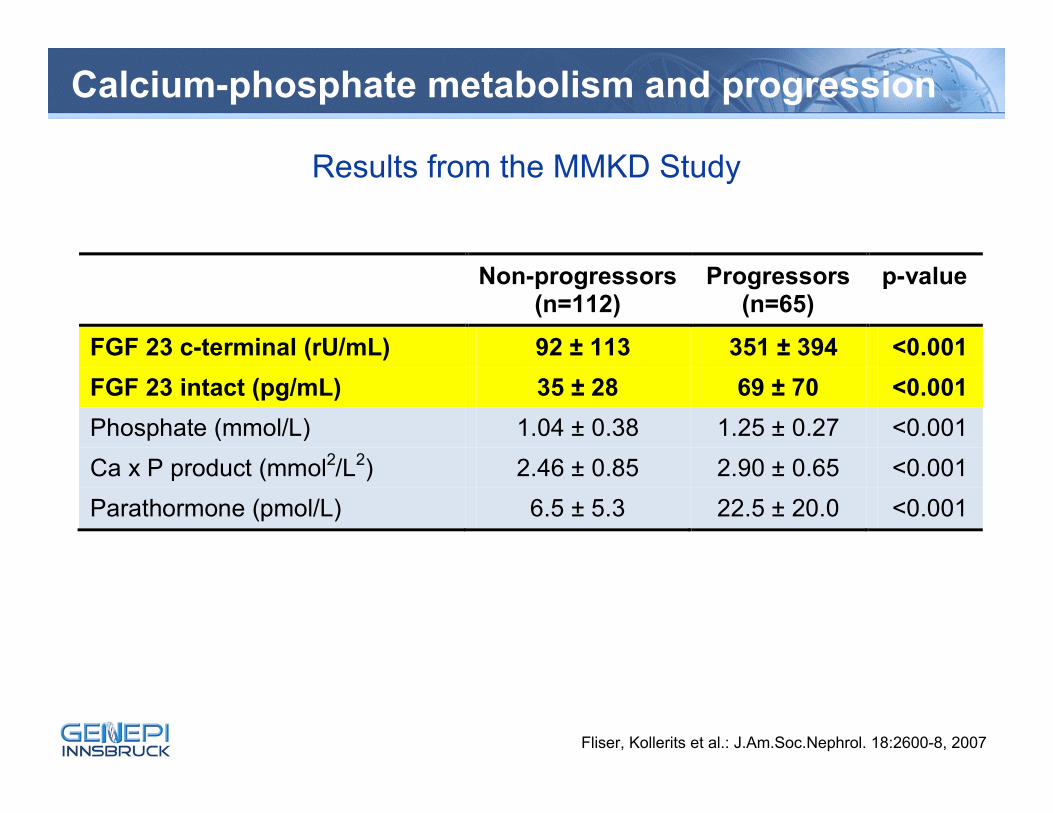
Calcium-phosphate metabolism and progression
Non-progressors(n=112)
Progressors (n=65)
p-value
FGF 23 c-terminal (rU/mL) 92 ± 113 351 ± 394 <0.001 FGF 23 intact (pg/mL) 35 ± 28 69 ± 70 <0.001 Phosphate (mmol/L) 1.04 ± 0.38 1.25 ± 0.27 <0.001 Ca x P product (mmol2/L2) 2.46 ± 0.85 2.90 ± 0.65 <0.001 Parathormone (pmol/L) 6.5 ± 5.3 22.5 ± 20.0 <0.001
Fliser, Kollerits et al.: J.Am.Soc.Nephrol. 18:2600-8, 2007
Results from the MMKD Study
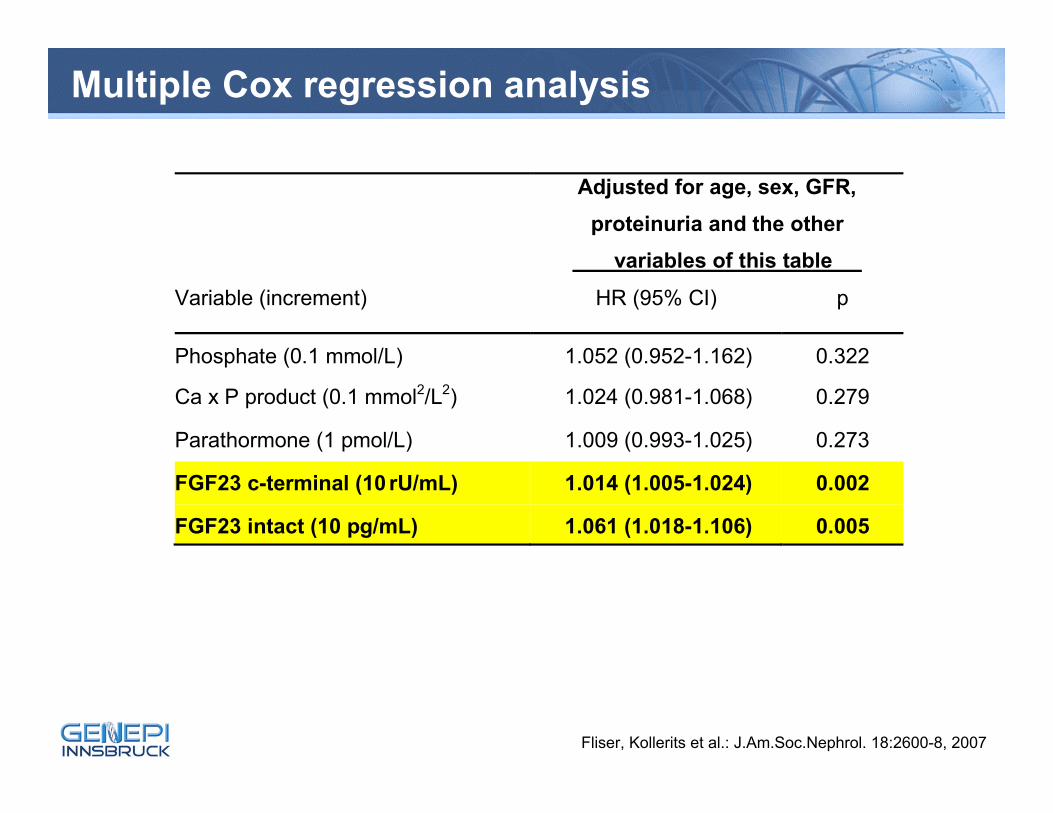
Multiple Cox regression analysis
Fliser, Kollerits et al.: J.Am.Soc.Nephrol. 18:2600-8, 2007
Adjusted for age, sex, GFR, proteinuria and the other
variables of this table
Variable (increment) HR (95% CI) p
Phosphate (0.1 mmol/L) 1.052 (0.952-1.162) 0.322
Ca x P product (0.1 mmol2/L2) 1.024 (0.981-1.068) 0.279
Parathormone (1 pmol/L) 1.009 (0.993-1.025) 0.273
FGF23 c-terminal (10 rU/mL) 1.014 (1.005-1.024) 0.002
FGF23 intact (10 pg/mL) 1.061 (1.018-1.106) 0.005
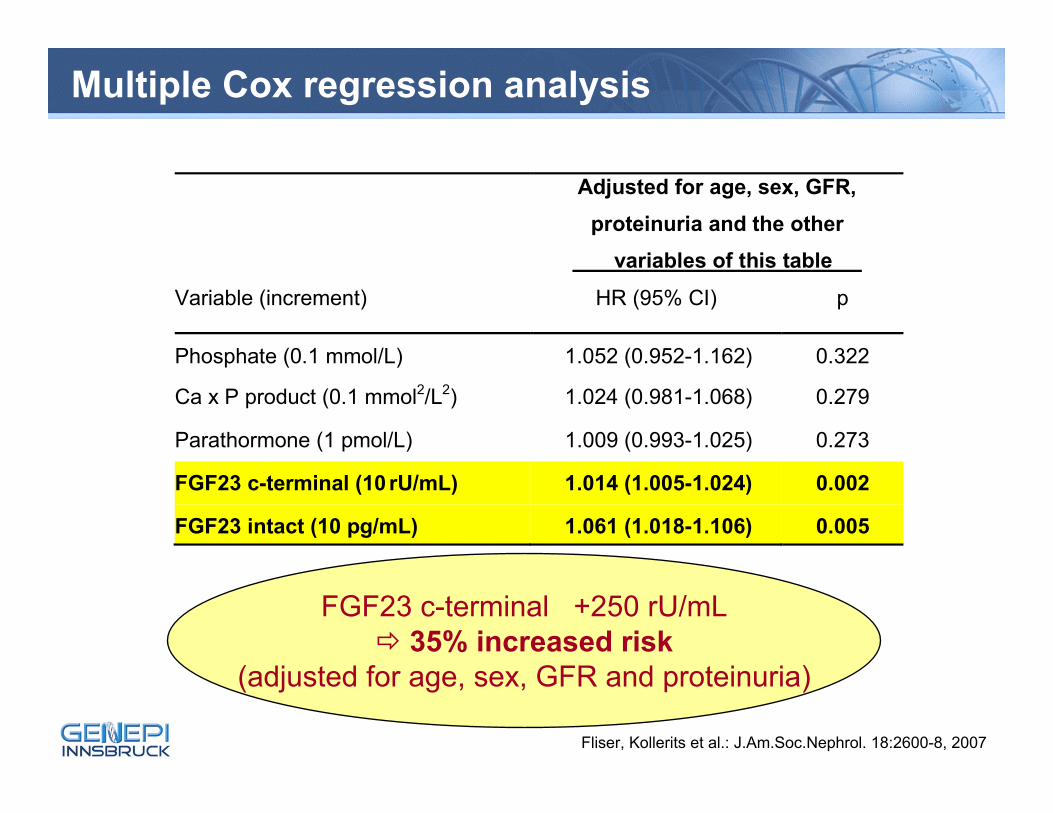
Multiple Cox regression analysis
Fliser, Kollerits et al.: J.Am.Soc.Nephrol. 18:2600-8, 2007
Adjusted for age, sex, GFR, proteinuria and the other
variables of this table
Variable (increment) HR (95% CI) p
Phosphate (0.1 mmol/L) 1.052 (0.952-1.162) 0.322
Ca x P product (0.1 mmol2/L2) 1.024 (0.981-1.068) 0.279
Parathormone (1 pmol/L) 1.009 (0.993-1.025) 0.273
FGF23 c-terminal (10 rU/mL) 1.014 (1.005-1.024) 0.002
FGF23 intact (10 pg/mL) 1.061 (1.018-1.106) 0.005
FGF23 c-terminal +250 rU/mL35% increased risk
(adjusted for age, sex, GFR and proteinuria)
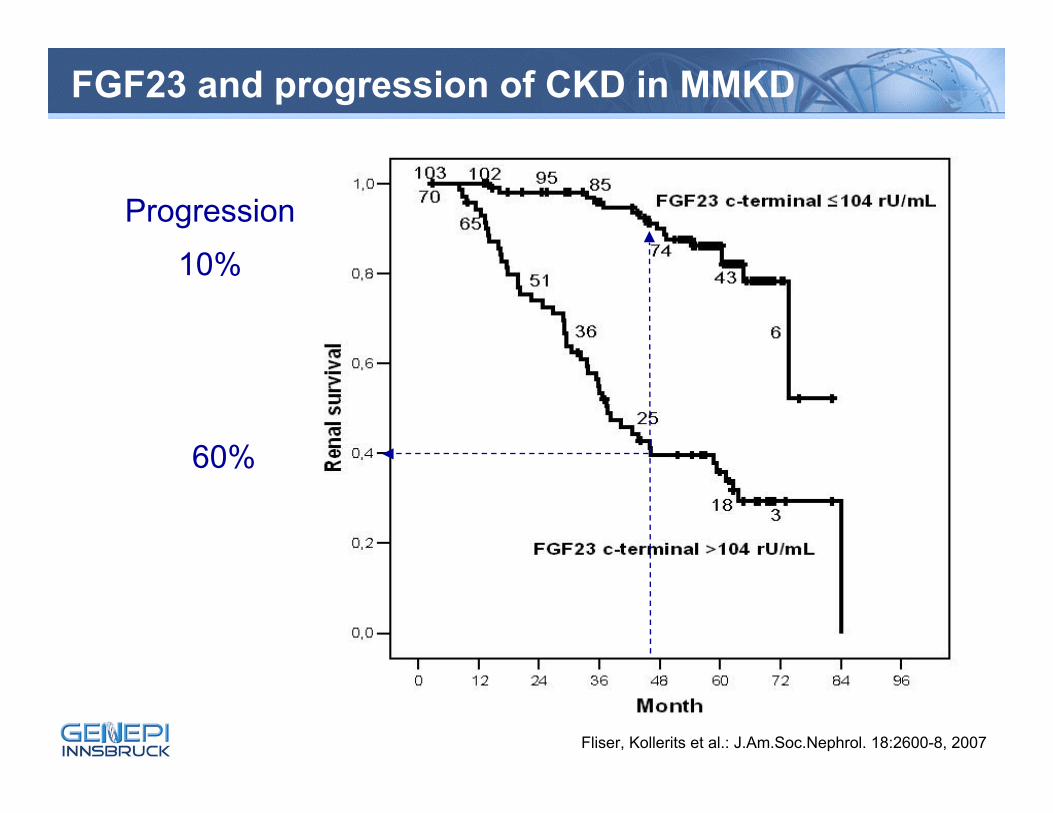
FGF23 and progression of CKD in MMKD
Fliser, Kollerits et al.: J.Am.Soc.Nephrol. 18:2600-8, 2007
Progression
10%
60%
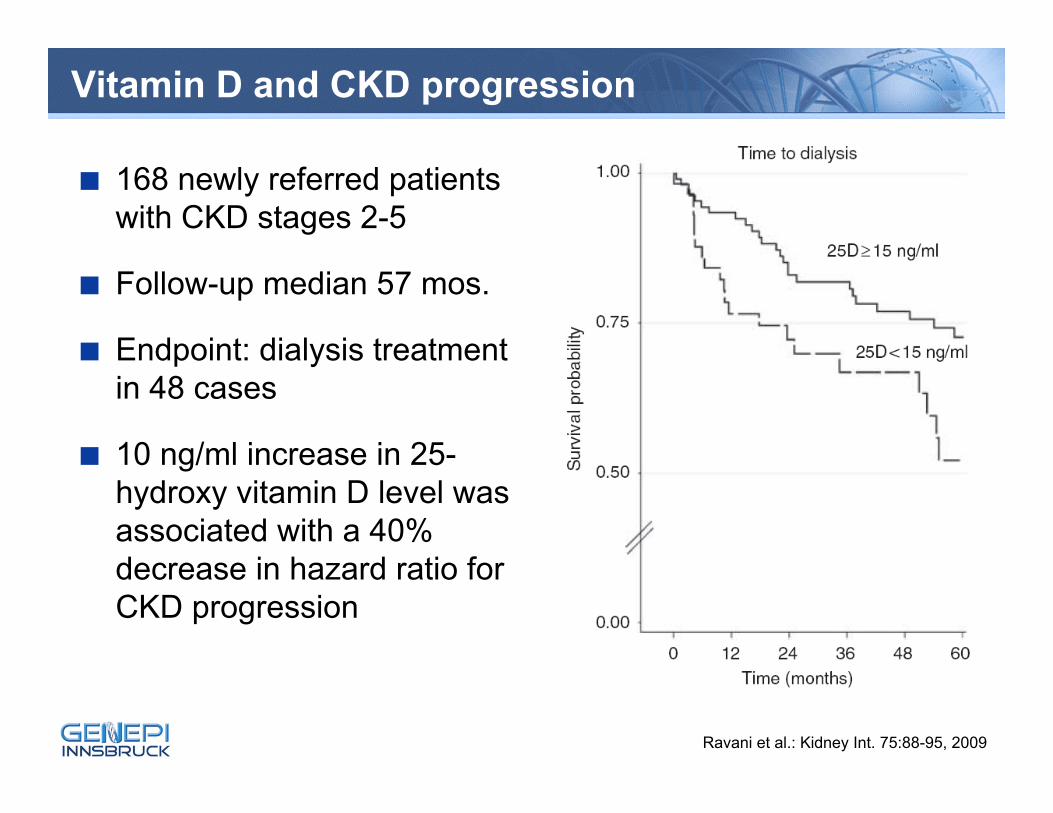
Vitamin D and CKD progression
■ 168 newly referred patients with CKD stages 2-5
■ Follow-up median 57 mos.
■ Endpoint: dialysis treatment in 48 cases
■ 10 ng/ml increase in 25-hydroxy vitamin D level was associated with a 40% decrease in hazard ratio for CKD progression
Ravani et al.: Kidney Int. 75:88-95, 2009
Adiponectin
■ Produced in adipocytes
■ Central role in glucose and lipid metabolism (insulin sensitizer)
■ An anti-inflammatory, anti-atherosclerotic and vasculo-protective cytokine
■ A large number of studies showed an association between low adiponectin levels and negative outcomes
■ Adiponectin is elevated in patients with kidney impairment
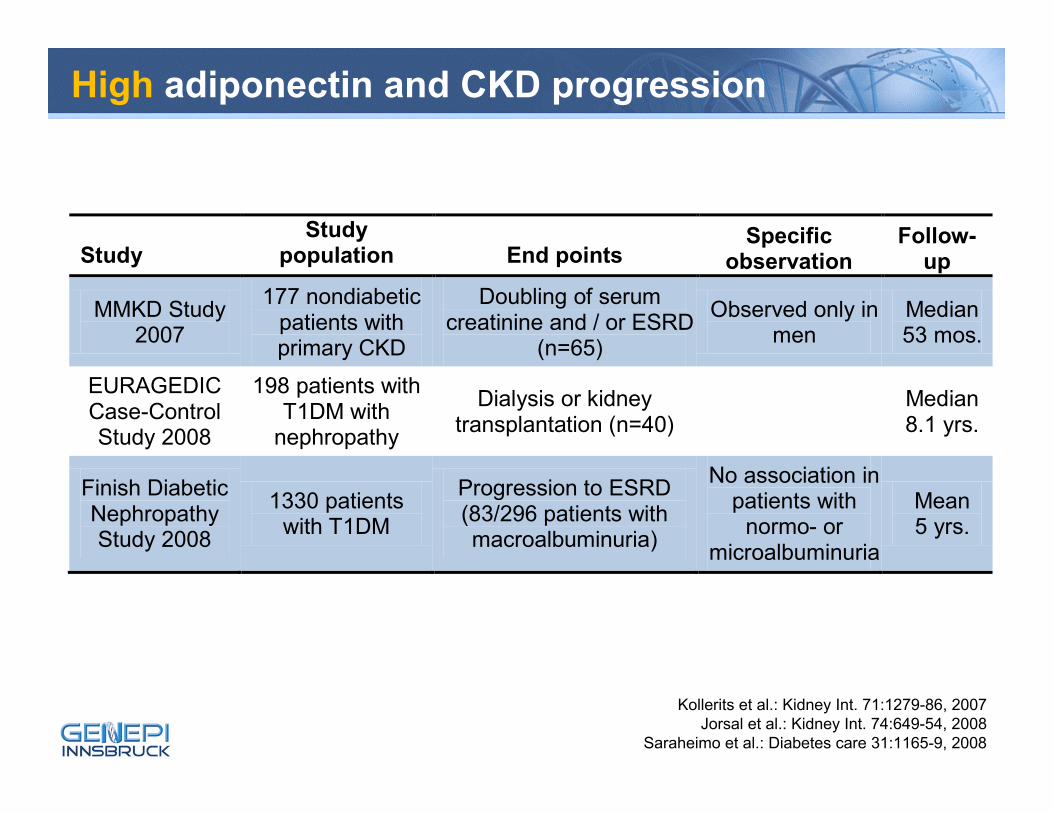
High adiponectin and CKD progression
Study Study
population End points Specific
observation Follow-
up
MMKD Study 2007
177 nondiabetic patients with primary CKD
Doubling of serum creatinine and / or ESRD
(n=65)
Observed only in men
Median 53 mos.
EURAGEDIC Case-Control Study 2008
198 patients with T1DM with
nephropathy
Dialysis or kidney transplantation (n=40) Median
8.1 yrs.
Finish Diabetic Nephropathy Study 2008
1330 patients with T1DM
Progression to ESRD (83/296 patients with macroalbuminuria)
No association in patients with
normo- or microalbuminuria
Mean 5 yrs.
Kollerits et al.: Kidney Int. 71:1279-86, 2007Jorsal et al.: Kidney Int. 74:649-54, 2008
Saraheimo et al.: Diabetes care 31:1165-9, 2008
Adiponectin association "reshaped"
■ High adiponectin in other studies predicted …► lower risk for cardiovascular events in ESRD (Zoccali et al. 2002)► mortality in CKD 3 and 4 in the MDRD Study (Menon et al. 2006)► mortality in patients with CHF (Kistorp et al. 2005)► all-cause and CVD mortality in CAD patients (Pilz et al. 2006)► and several other studies
Adiponectin association "reshaped"
■ High adiponectin in other studies predicted …► lower risk for cardiovascular events in ESRD (Zoccali et al. 2002)► mortality in CKD 3 and 4 in the MDRD Study (Menon et al. 2006)► mortality in patients with CHF (Kistorp et al. 2005)► all-cause and CVD mortality in CAD patients (Pilz et al. 2006)► and several other studies
The association of adiponectin might turn in the opposite direction in the presence of severe disease conditions
A compensatory attempt to attenutae endothelial and vascular damage?
Adiponectin resistance?
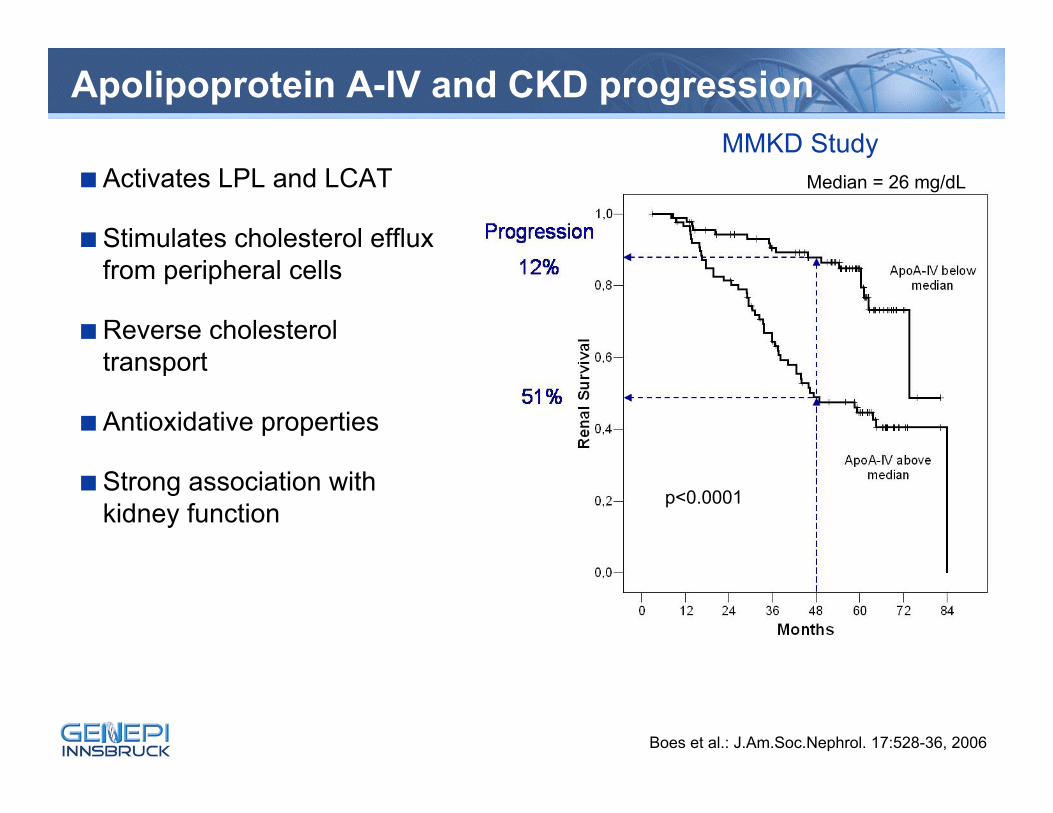
Apolipoprotein A-IV and CKD progression
■Activates LPL and LCAT
■Stimulates cholesterol efflux from peripheral cells
■Reverse cholesterol transport
■Antioxidative properties
■Strong association with kidney function
Boes et al.: J.Am.Soc.Nephrol. 17:528-36, 2006
Median = 26 mg/dL
p<0.0001
MMKD Study
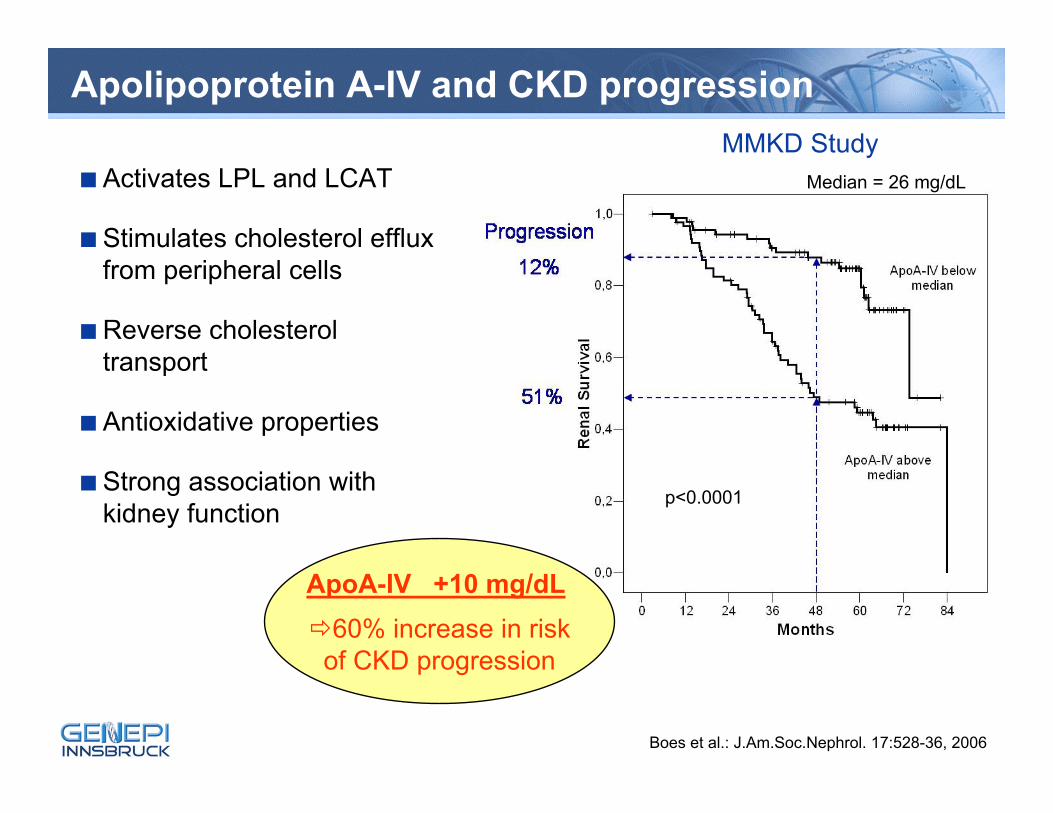
Apolipoprotein A-IV and CKD progression
■Activates LPL and LCAT
■Stimulates cholesterol efflux from peripheral cells
■Reverse cholesterol transport
■Antioxidative properties
■Strong association with kidney function
Boes et al.: J.Am.Soc.Nephrol. 17:528-36, 2006
Median = 26 mg/dL
p<0.0001
MMKD Study
ApoA-IV +10 mg/dL 60% increase in risk
of CKD progression
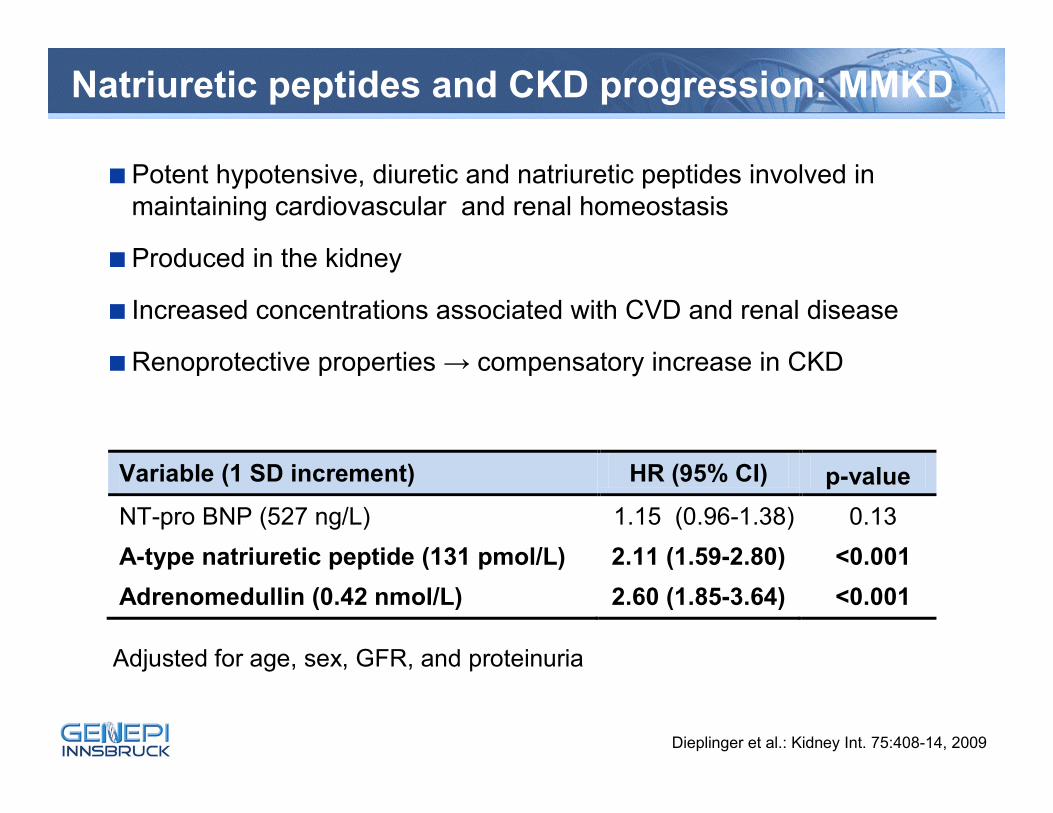
Natriuretic peptides and CKD progression: MMKD
■Potent hypotensive, diuretic and natriuretic peptides involved in maintaining cardiovascular and renal homeostasis
■Produced in the kidney
■ Increased concentrations associated with CVD and renal disease
■Renoprotective properties → compensatory increase in CKD
Dieplinger et al.: Kidney Int. 75:408-14, 2009
Variable (1 SD increment) HR (95% CI) p-value NT-pro BNP (527 ng/L) 1.15 (0.96-1.38) 0.13 A-type natriuretic peptide (131 pmol/L) 2.11 (1.59-2.80) <0.001 Adrenomedullin (0.42 nmol/L) 2.60 (1.85-3.64) <0.001
Adjusted for age, sex, GFR, and proteinuria
Calculating the gain in information
ADMA
FGF23
ANP
Adrenomedullin
NT-proBNP
ApoA-IV
GFR
Proteinuria
Problem of correlation of variables (multicollinearity)
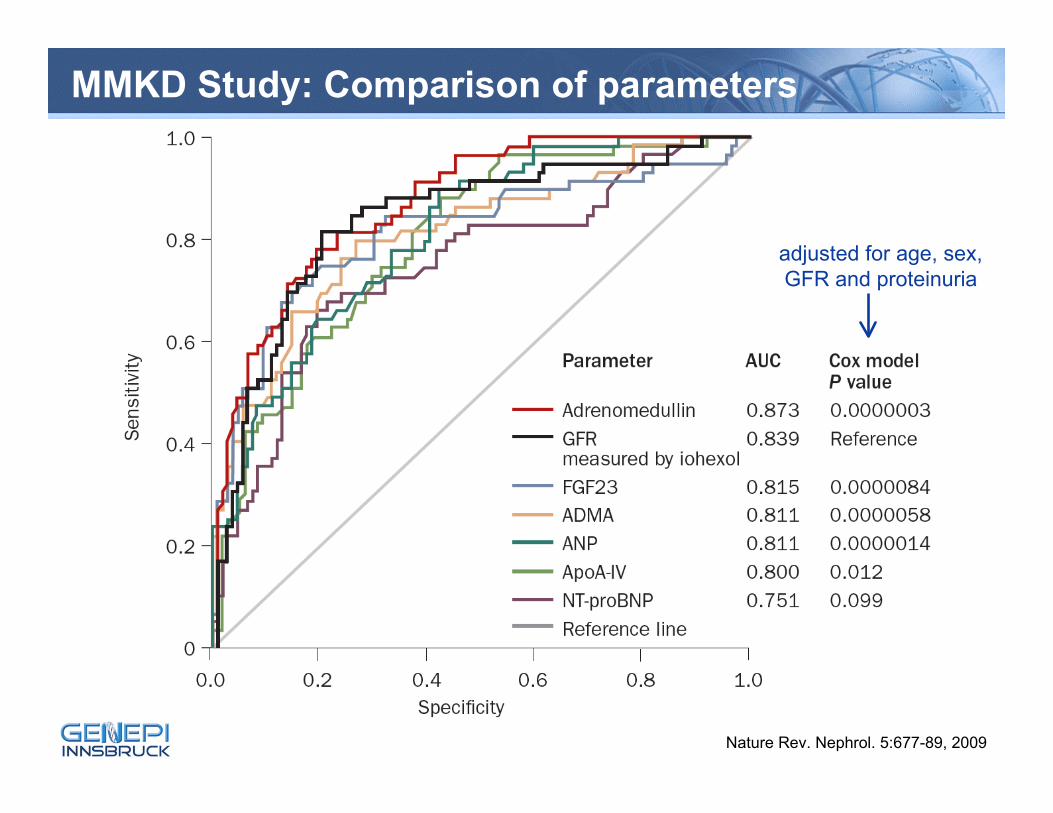
MMKD Study: Comparison of parameters
Nature Rev. Nephrol. 5:677-89, 2009
adjusted for age, sex, GFR and proteinuria
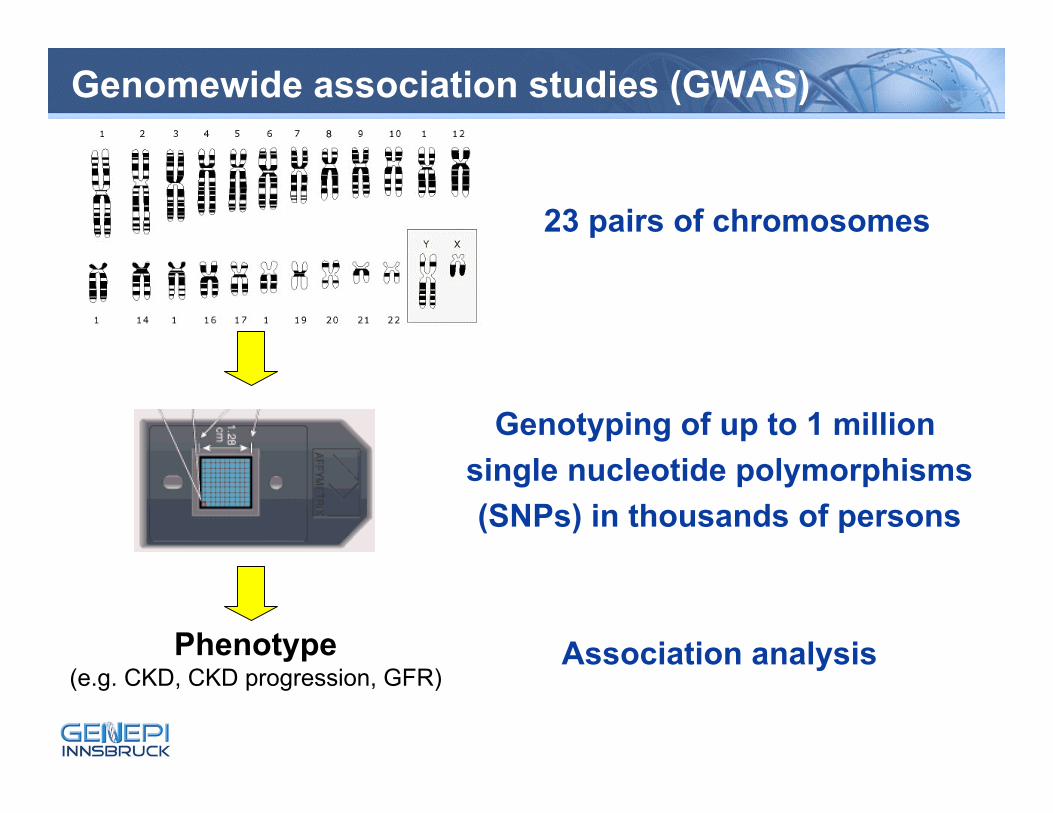
Genomewide association studies (GWAS)
Phenotype(e.g. CKD, CKD progression, GFR)
23 pairs of chromosomes
Genotyping of up to 1 million single nucleotide polymorphisms(SNPs) in thousands of persons
Association analysis
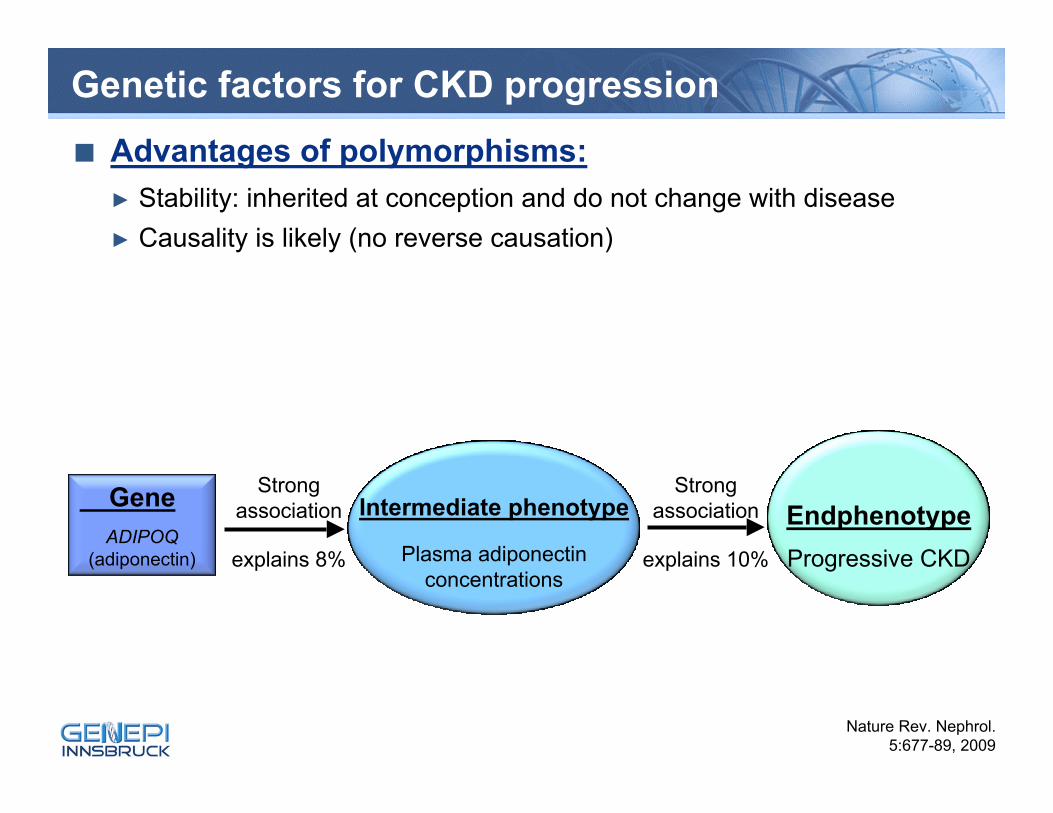
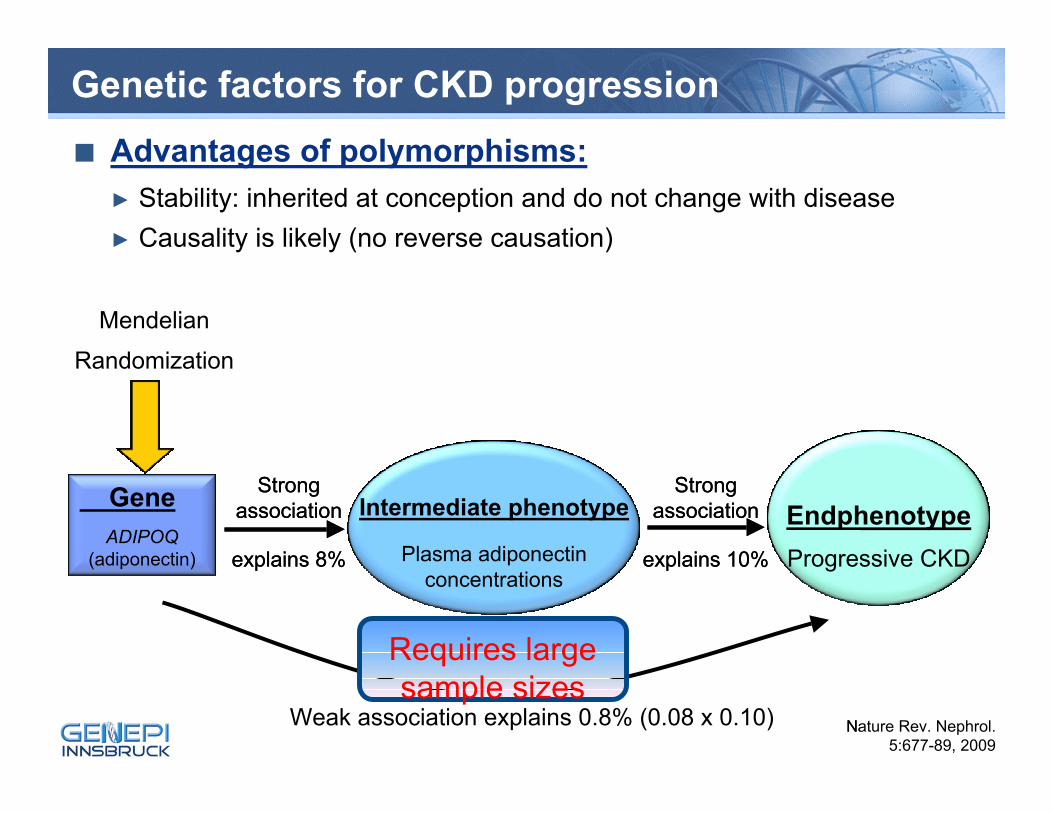
Genetic factors for CKD progression■ Advantages of polymorphisms:
► Stability: inherited at conception and do not change with disease► Causality is likely (no reverse causation)
EndphenotypeProgressive CKD
Intermediate phenotype
Plasma adiponectinconcentrations
GeneADIPOQ
(adiponectin)
Strong association
explains 8%
Strong association
explains 10%
Nature Rev. Nephrol. 5:677-89, 2009
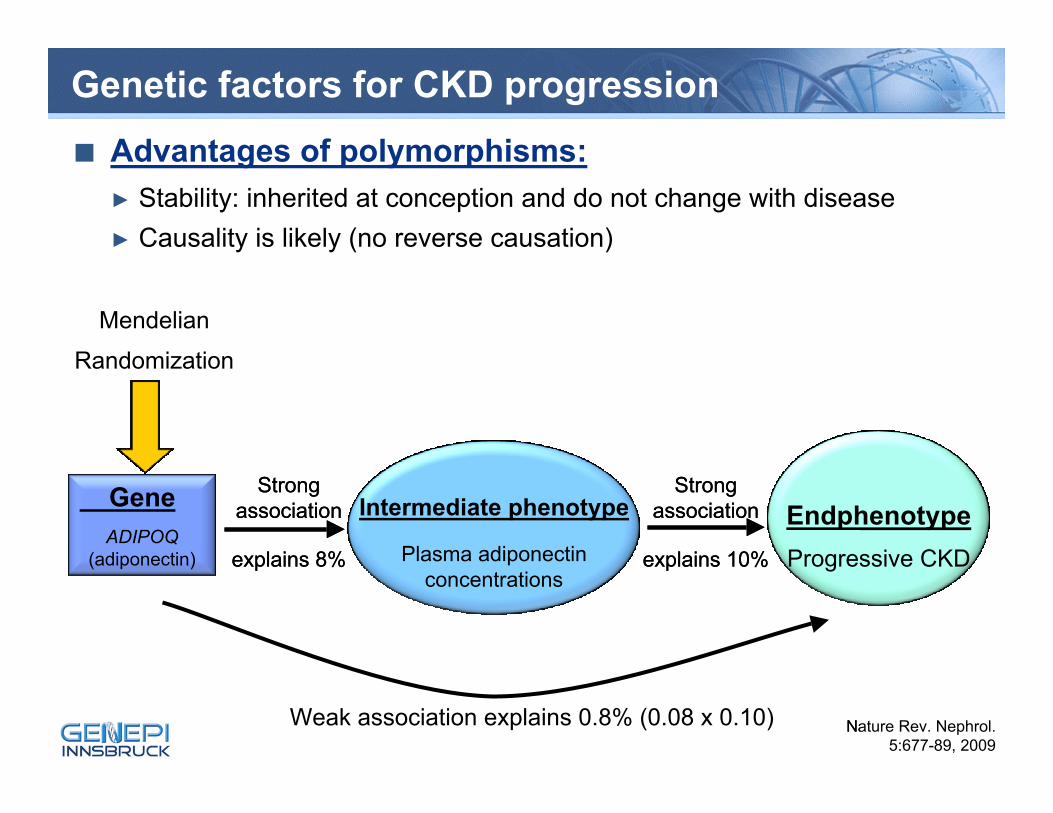
Genetic factors for CKD progression■ Advantages of polymorphisms:
► Stability: inherited at conception and do not change with disease► Causality is likely (no reverse causation)
EndphenotypeProgressive CKD
Intermediate phenotype
Plasma adiponectinconcentrations
GeneADIPOQ
(adiponectin)
Strong association
explains 8%
Strong association
explains 10%
Nature Rev. Nephrol. 5:677-89, 2009
Weak association explains 0.8% (0.08 x 0.10)
Mendelian
Randomization
EndphProgres
Intermediate phenotype
Plasma adiponectinconcentrations
GeneADIPOQ
(adiponectin)
Strong association
explains 8%
Strong association
explains 10%
Na
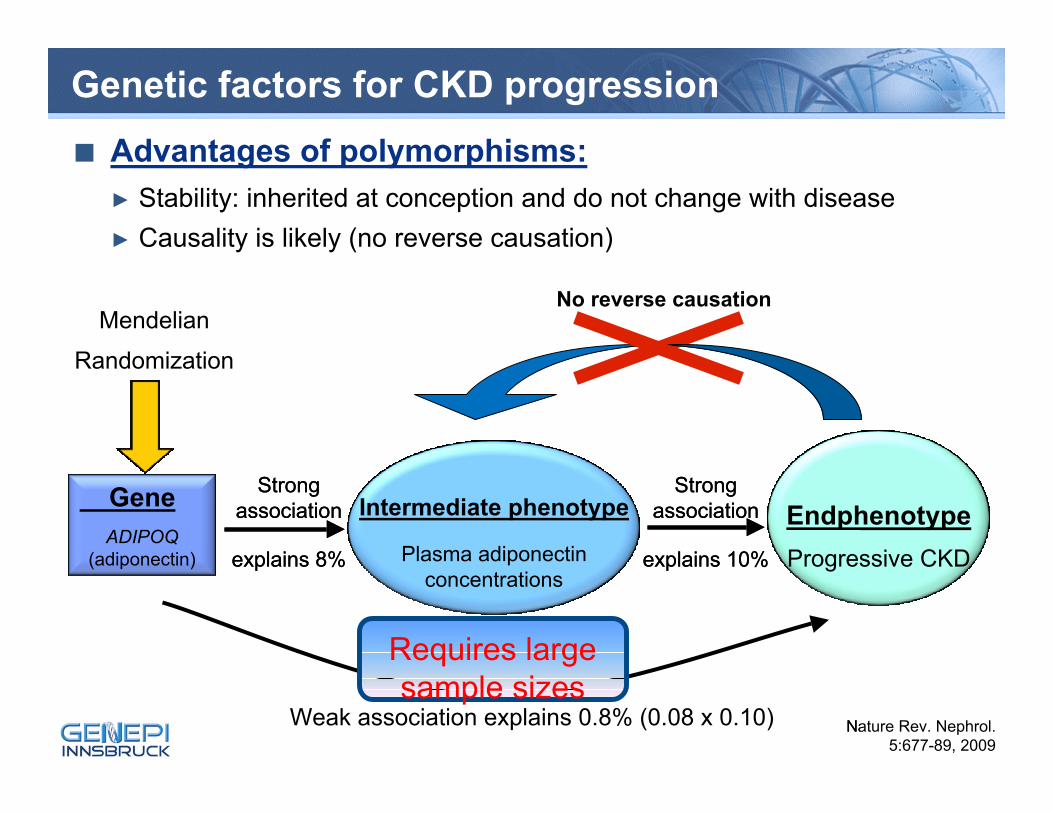
Genetic factors for CKD progression■ Advantages of polymorphisms:
► Stability: inherited at conception and do not change with disease► Causality is likely (no reverse causation)
EndphenotypeProgressive CKD
Intermediate phenotype
Plasma adiponectinconcentrations
GeneADIPOQ
(adiponectin)
Strong association
explains 8%
Strong association
explains 10%
Nature Rev. Nephrol. 5:677-89, 2009
Weak association explains 0.8% (0.08 x 0.10)
Mendelian
Randomization
EndphProgres
Intermediate phenotype
Plasma adiponectinconcentrations
GeneADIPOQ
(adiponectin)
Strong association
explains 8%
Strong association
explains 10%
Na
Requires large sample sizes
Genetic factors for CKD progression■ Advantages of polymorphisms:
► Stability: inherited at conception and do not change with disease► Causality is likely (no reverse causation)
EndphenotypeProgressive CKD
Intermediate phenotype
Plasma adiponectinconcentrations
GeneADIPOQ
(adiponectin)
Strong association
explains 8%
Strong association
explains 10%
Nature Rev. Nephrol. 5:677-89, 2009
Weak association explains 0.8% (0.08 x 0.10)
Mendelian
Randomization
EndphProgres
Intermediate phenotype
Plasma adiponectinconcentrations
GeneADIPOQ
(adiponectin)
Strong association
explains 8%
Strong association
explains 10%
Na
Requires large sample sizes
No reverse causation
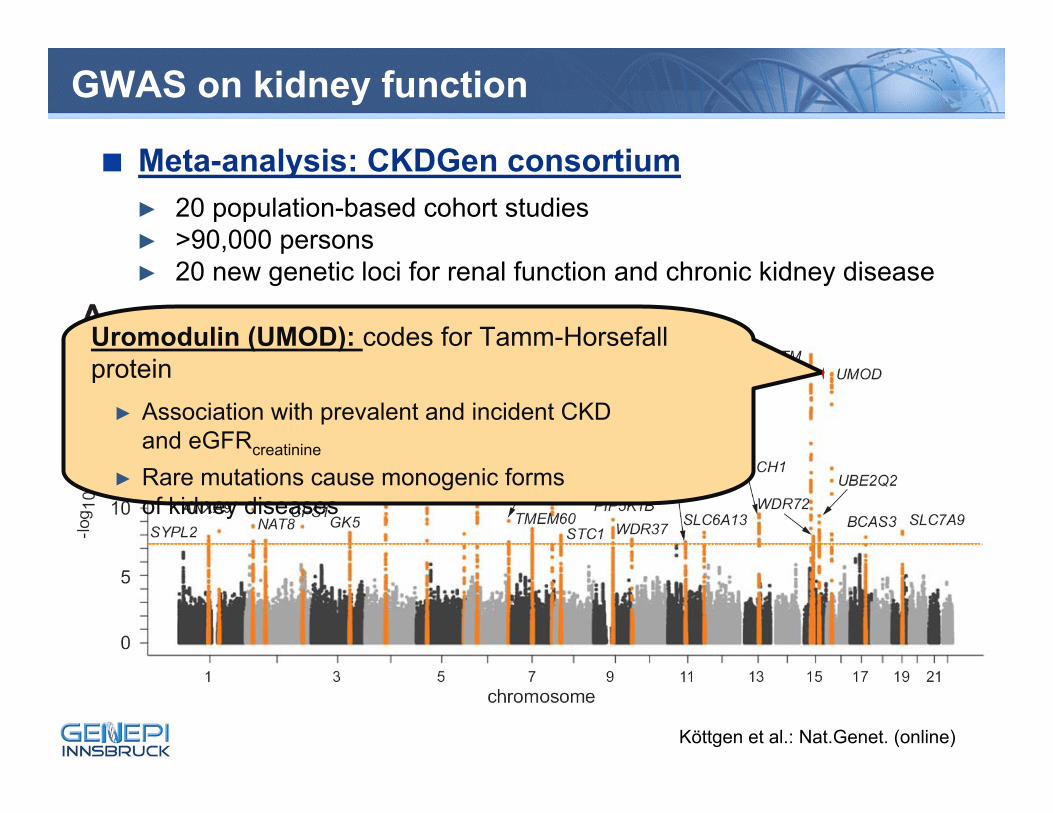
GWAS on kidney function
Köttgen et al.: Nat.Genet. (online)
■ Meta-analysis: CKDGen consortium► 20 population-based cohort studies► >90,000 persons► 20 new genetic loci for renal function and chronic kidney disease
Uromodulin (UMOD): codes for Tamm-Horsefall protein
► Association with prevalent and incident CKD and eGFRcreatinine
► Rare mutations cause monogenic forms of kidney diseases
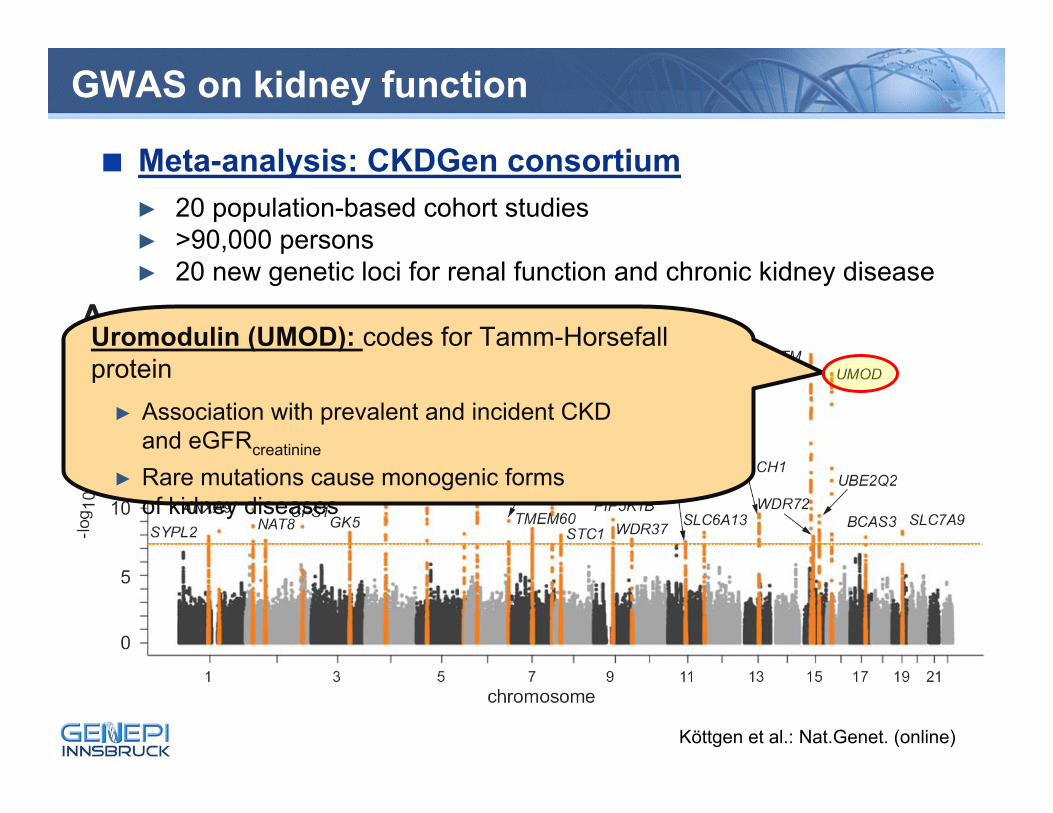
GWAS on kidney function
Köttgen et al.: Nat.Genet. (online)
■ Meta-analysis: CKDGen consortium► 20 population-based cohort studies► >90,000 persons► 20 new genetic loci for renal function and chronic kidney disease
Uromodulin (UMOD): codes for Tamm-Horsefall protein
► Association with prevalent and incident CKD and eGFRcreatinine
► Rare mutations cause monogenic forms of kidney diseases
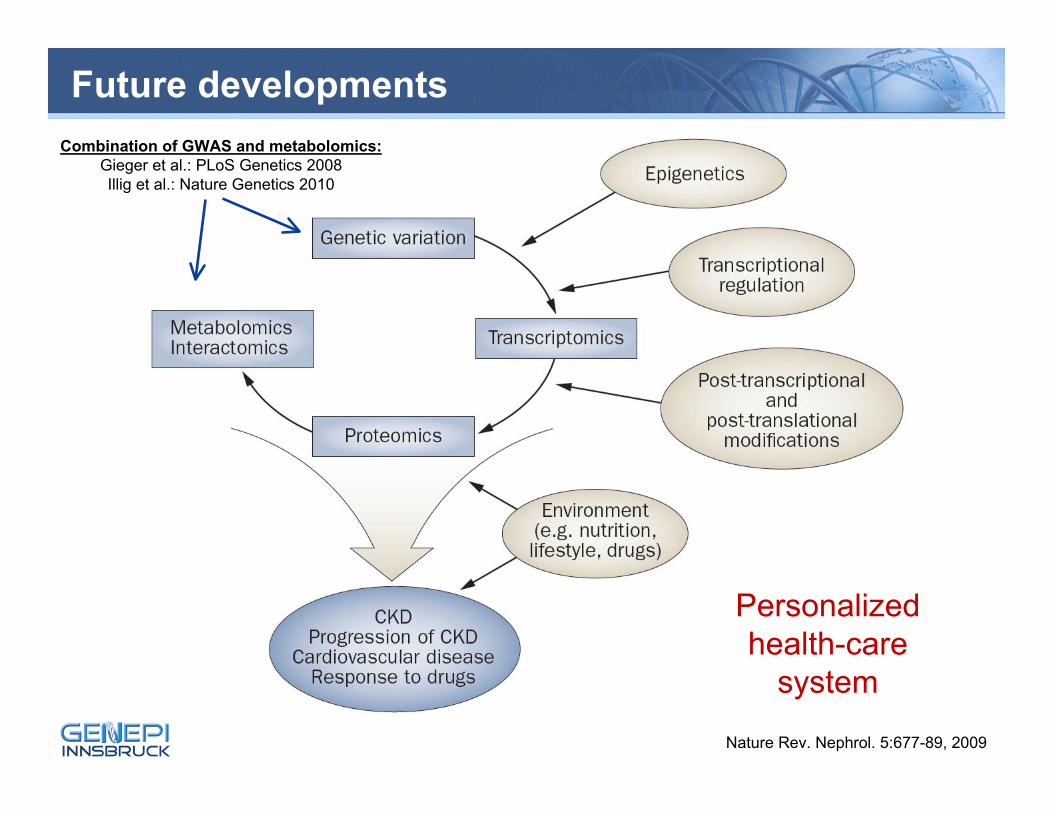
Future developments
Nature Rev. Nephrol. 5:677-89, 2009
Combination of GWAS and metabolomics:Gieger et al.: PLoS Genetics 2008Illig et al.: Nature Genetics 2010
Personalized health-care
system
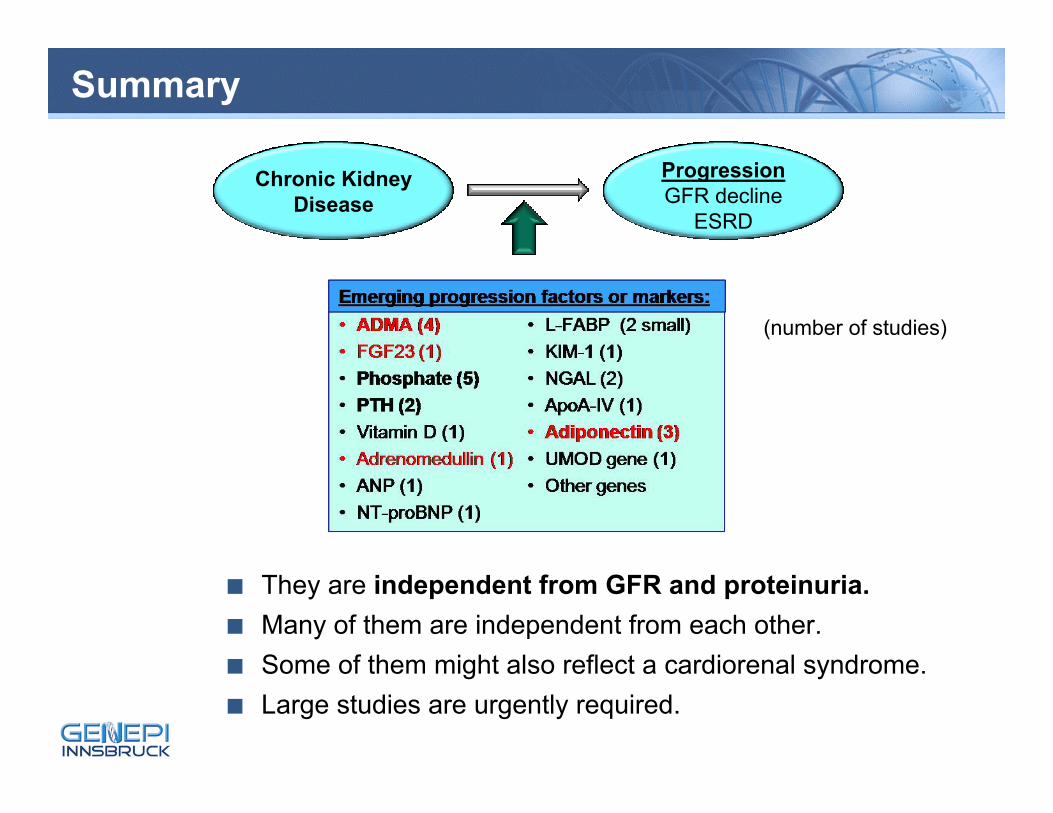
Summary
■ They are independent from GFR and proteinuria.■ Many of them are independent from each other.■ Some of them might also reflect a cardiorenal syndrome.■ Large studies are urgently required.
Chronic KidneyDisease
ProgressionGFR decline
ESRD
Emerging progression factors or markers:
(number of studies)
The MMKD Study Group
Barbara Kollerits Eberhard RitzEva Boes Gerhard MüllerPaul König Günter KraatzKarl Lhotta Johannes MannUlrich Neyer Werner RiegelDanilo Fliser Vedat SchwengerJan Kielstein Katharina-Susanne SpanausIris M. Heid Arnold von EckardsteinBenjamin Dieplinger Peter Riegler
Renal Units: Innsbruck, Feldkirch, Greifswald, Heidelberg, München-Schwabing,Göttingen, Homburg/Saar, Bozen
Project Support: GEN-AU (Austrian Genome Project)Austrian Science Fund, Austrian National BankAustrian Academy of SciencesAustrian Heart FundElse Kröner-Fresenius Stiftung


![W J N World Journal of Nephrology - Microsoft · Chronic kidney disease (CKD) affects approximately one-seventh of adults above the age of 20 years[1]. Progression of CKD is a major](https://img.pdfslide.net/doc/110x75/6077dcc629ad451db7746a58/w-j-n-world-journal-of-nephrology-microsoft-chronic-kidney-disease-ckd-affects.jpg)