Embed Size (px)
Citation preview
LIVERPOOL CLINICAL LABORATORIES
Empirical Management of
Infection on Critical Care
Units at AUH and RLUH
Patricia Crossey (Critical Care Pharmacist, RLUH), Alison Hall (ITU Consultant, RLUH), Jenifer Mason (Microbiology Consultant LCL), Robert Parker (ITU
Consultant, AUH) and Clare Sales (Critical Care Pharmacist, AUH)
2017
These Guidelines refer to common ITU presentations and relate to
empirical management only. For indications not covered refer to
the Trust Antibiotic Formulary (Royal and Aintree).
Enquiries to: [email protected] or
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 1
Contents General Principles ............................................................................................................................................................................................. 2
Abdominal Infection .......................................................................................................................................................................................... 3
Non Healthcare associated Intra-abdominal Infection................................................................................................................................. 3
Healthcare associated intra-abdominal infection ........................................................................................................................................ 4
Variceal bleeds and acute liver failure ......................................................................................................................................................... 4
Central Nervous System .................................................................................................................................................................................... 5
Meningitis/Encephalitis ............................................................................................................................................................................... 5
ENT or Dental Infection ..................................................................................................................................................................................... 6
Epiglottitis .................................................................................................................................................................................................... 6
Dental Abscess or other oral infection ......................................................................................................................................................... 6
Respiratory Tract Infection ................................................................................................................................................................................ 7
Community acquired pneumonia ................................................................................................................................................................ 7
Hospital Acquired Pneumonia or Ventilator Associated Pneumonia ........................................................................................................... 7
Aspiration Pneumonia ................................................................................................................................................................................. 8
Infective Exacerbation of Chronic Lung Disease (COPD, bronchiectasis) ..................................................................................................... 8
Suspected influenza with concurrent pneumonia........................................................................................................................................ 8
Sepsis of Unknown Origin.................................................................................................................................................................................. 9
Sepsis of Unknown Origin – Non Neutropenic ............................................................................................................................................. 9
Neutropenic Sepsis ...................................................................................................................................................................................... 9
Skin and Soft Tissue Infection .......................................................................................................................................................................... 10
Necrotising soft tissue infection of any anatomical site ............................................................................................................................. 10
Cellulitis ..................................................................................................................................................................................................... 10
Trauma Prophylaxis ......................................................................................................................................................................................... 11
Prophylaxis in head and neck trauma ........................................................................................................................................................ 11
Prophylaxis for Compound Fractures ......................................................................................................................................................... 11
Selective Decontamination of the Digestive Tract ......................................................................................... Error! Bookmark not defined.
Urosepsis ......................................................................................................................................................................................................... 13
Urosepsis/pyelonephritis ........................................................................................................................................................................... 13
Appendix ......................................................................................................................................................................................................... 14
Infection Control Precautions .................................................................................................................................................................... 14
Weekly Screening ...................................................................................................................................................................................... 15
Notifiable Diseases..................................................................................................................................................................................... 17
Tetanus Prone Wounds .............................................................................................................................................................................. 18
Processing Urgent Specimens Out of Hours (Mon-Fri 1630-0900 and Sat-Sun) ......................................................................................... 19
Gentamicin and Teicoplanin Dosing ........................................................................................................................................................... 21
Gentamicin ........................................................................................................................................................................................... 21
Teicoplanin ........................................................................................................................................................................................... 21
Contact Details ........................................................................................................................................................................................... 21
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 2
General Principles 1. Antibiotic treatment should NEVER be delayed in an emergency. However,
wherever possible, microbiological specimens should always be obtained before antibiotic therapy is commenced
2. Prior to antibiotic therapy patients should ALWAYS have TWO sets of blood cultures taken i.e. x2 aerobic and x2 anaerobic bottles. If there are lines present
culture from the line AND a peripheral site. Send other specimens as appropriate
(respiratory, drain fluid, wound swabs etc.)
3. Always check previous Microbiology results, with particular attention to resistant
organisms (see below for common resistance patterns). Note the empirical antibiotic choice
may not cover resistant organisms – please discuss with Microbiology if unsure
4. Antibiotics are not a substitute for source control (i.e. surgical drainage of an abscess)
5. Antibiotics should be administered within 1 hour in patients with signs of severe sepsis or
septic shock
6. Allergy status must be checked BEFORE prescribing and administering any antibiotic and documented on the patient’s drug chart, including where possible the nature of the allergy
7. An antibiotic history should be taken and recorded in the critical care notes 8. All antibiotic prescriptions should have an indication, start date and review or stop date.
9. These guidelines are for empirical management only. Antibiotics should be focussed at the
earliest opportunity on the Microbiology ward round with culture results
10. Do not dose adjust antibiotics in acute kidney injury (including Gentamicin) in the first 24
hours. Following this, and in chronic renal failure seek advice from Pharmacy
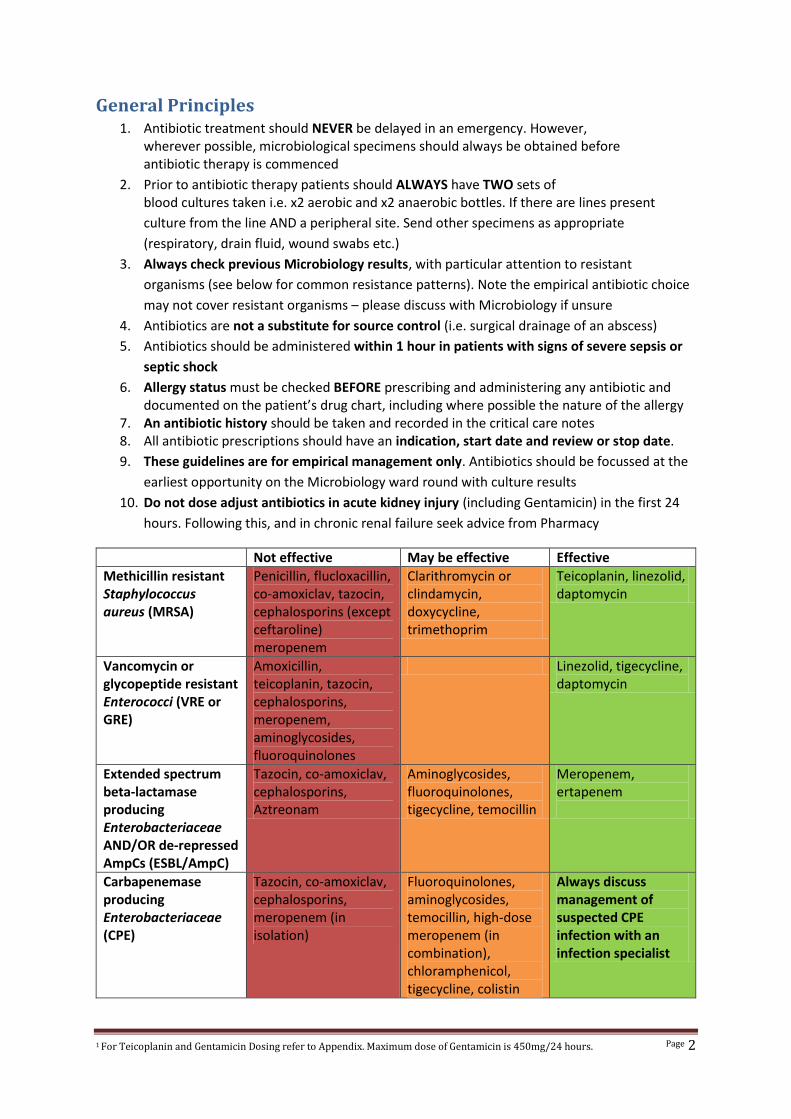
Not effective May be effective Effective
Methicillin resistant Staphylococcus aureus (MRSA)
Penicillin, flucloxacillin, co-amoxiclav, tazocin, cephalosporins (except ceftaroline) meropenem
Clarithromycin or clindamycin, doxycycline, trimethoprim
Teicoplanin, linezolid, daptomycin
Vancomycin or glycopeptide resistant Enterococci (VRE or GRE)
Amoxicillin, teicoplanin, tazocin, cephalosporins, meropenem, aminoglycosides, fluoroquinolones
Linezolid, tigecycline, daptomycin
Extended spectrum beta-lactamase producing Enterobacteriaceae AND/OR de-repressed AmpCs (ESBL/AmpC)
Tazocin, co-amoxiclav, cephalosporins, Aztreonam
Aminoglycosides, fluoroquinolones, tigecycline, temocillin
Meropenem, ertapenem
Carbapenemase producing Enterobacteriaceae (CPE)
Tazocin, co-amoxiclav, cephalosporins, meropenem (in isolation)
Fluoroquinolones, aminoglycosides, temocillin, high-dose meropenem (in combination), chloramphenicol, tigecycline, colistin
Always discuss management of suspected CPE infection with an infection specialist
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 3
Abdominal Infection
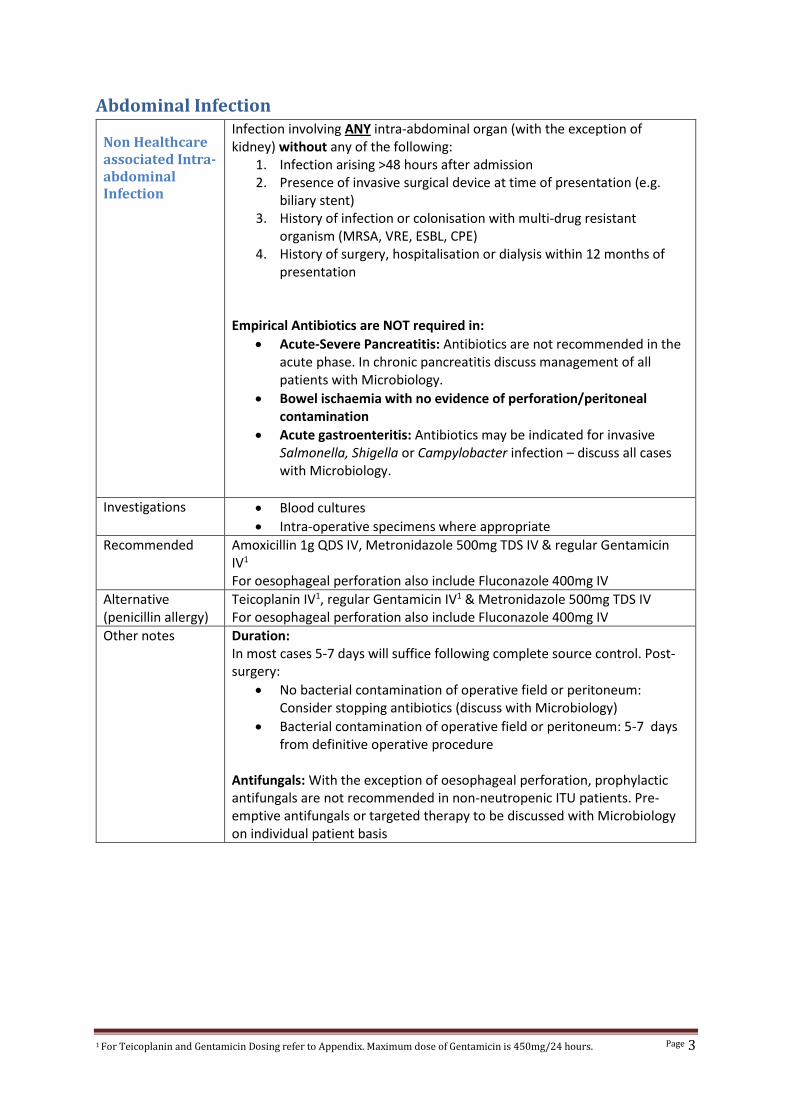
Non Healthcare associated Intra-abdominal Infection
Infection involving ANY intra-abdominal organ (with the exception of kidney) without any of the following:
1. Infection arising >48 hours after admission 2. Presence of invasive surgical device at time of presentation (e.g.
biliary stent) 3. History of infection or colonisation with multi-drug resistant
organism (MRSA, VRE, ESBL, CPE) 4. History of surgery, hospitalisation or dialysis within 12 months of
presentation
Empirical Antibiotics are NOT required in:
Acute-Severe Pancreatitis: Antibiotics are not recommended in the acute phase. In chronic pancreatitis discuss management of all patients with Microbiology.
Bowel ischaemia with no evidence of perforation/peritoneal contamination
Acute gastroenteritis: Antibiotics may be indicated for invasive Salmonella, Shigella or Campylobacter infection – discuss all cases with Microbiology.
Investigations Blood cultures
Intra-operative specimens where appropriate
Recommended Amoxicillin 1g QDS IV, Metronidazole 500mg TDS IV & regular Gentamicin IV1 For oesophageal perforation also include Fluconazole 400mg IV
Alternative (penicillin allergy)
Teicoplanin IV1, regular Gentamicin IV1 & Metronidazole 500mg TDS IV For oesophageal perforation also include Fluconazole 400mg IV
Other notes Duration: In most cases 5-7 days will suffice following complete source control. Post-surgery:
No bacterial contamination of operative field or peritoneum: Consider stopping antibiotics (discuss with Microbiology)
Bacterial contamination of operative field or peritoneum: 5-7 days from definitive operative procedure
Antifungals: With the exception of oesophageal perforation, prophylactic antifungals are not recommended in non-neutropenic ITU patients. Pre-emptive antifungals or targeted therapy to be discussed with Microbiology on individual patient basis
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 4
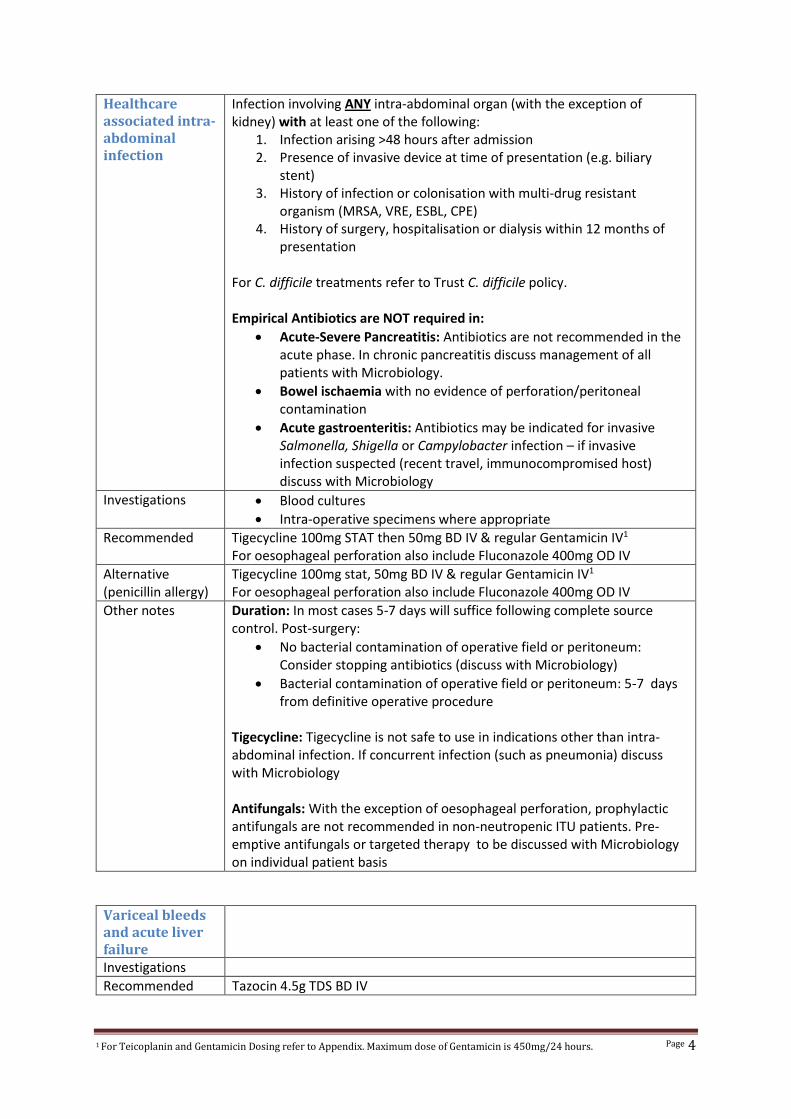
Healthcare associated intra-abdominal infection
Infection involving ANY intra-abdominal organ (with the exception of kidney) with at least one of the following:
1. Infection arising >48 hours after admission 2. Presence of invasive device at time of presentation (e.g. biliary
stent) 3. History of infection or colonisation with multi-drug resistant
organism (MRSA, VRE, ESBL, CPE) 4. History of surgery, hospitalisation or dialysis within 12 months of
presentation
For C. difficile treatments refer to Trust C. difficile policy. Empirical Antibiotics are NOT required in:
Acute-Severe Pancreatitis: Antibiotics are not recommended in the acute phase. In chronic pancreatitis discuss management of all patients with Microbiology.
Bowel ischaemia with no evidence of perforation/peritoneal contamination
Acute gastroenteritis: Antibiotics may be indicated for invasive Salmonella, Shigella or Campylobacter infection – if invasive infection suspected (recent travel, immunocompromised host) discuss with Microbiology
Investigations Blood cultures
Intra-operative specimens where appropriate
Recommended Tigecycline 100mg STAT then 50mg BD IV & regular Gentamicin IV1 For oesophageal perforation also include Fluconazole 400mg OD IV
Alternative (penicillin allergy)
Tigecycline 100mg stat, 50mg BD IV & regular Gentamicin IV1 For oesophageal perforation also include Fluconazole 400mg OD IV
Other notes Duration: In most cases 5-7 days will suffice following complete source control. Post-surgery:
No bacterial contamination of operative field or peritoneum: Consider stopping antibiotics (discuss with Microbiology)
Bacterial contamination of operative field or peritoneum: 5-7 days from definitive operative procedure
Tigecycline: Tigecycline is not safe to use in indications other than intra-abdominal infection. If concurrent infection (such as pneumonia) discuss with Microbiology Antifungals: With the exception of oesophageal perforation, prophylactic antifungals are not recommended in non-neutropenic ITU patients. Pre-emptive antifungals or targeted therapy to be discussed with Microbiology on individual patient basis
Variceal bleeds and acute liver failure
Investigations
Recommended Tazocin 4.5g TDS BD IV
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 5
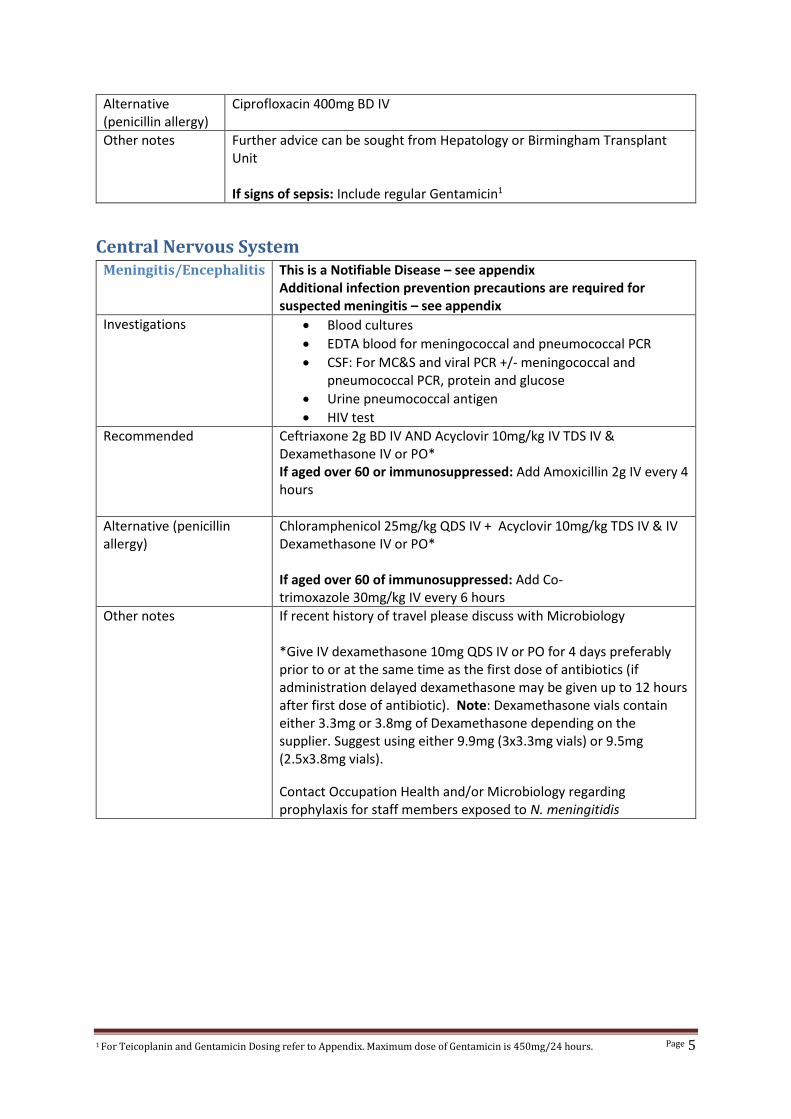
Alternative (penicillin allergy)
Ciprofloxacin 400mg BD IV
Other notes Further advice can be sought from Hepatology or Birmingham Transplant Unit If signs of sepsis: Include regular Gentamicin1
Central Nervous System Meningitis/Encephalitis This is a Notifiable Disease – see appendix
Additional infection prevention precautions are required for suspected meningitis – see appendix
Investigations Blood cultures
EDTA blood for meningococcal and pneumococcal PCR
CSF: For MC&S and viral PCR +/- meningococcal and pneumococcal PCR, protein and glucose
Urine pneumococcal antigen
HIV test
Recommended Ceftriaxone 2g BD IV AND Acyclovir 10mg/kg IV TDS IV & Dexamethasone IV or PO* If aged over 60 or immunosuppressed: Add Amoxicillin 2g IV every 4 hours
Alternative (penicillin allergy)
Chloramphenicol 25mg/kg QDS IV + Acyclovir 10mg/kg TDS IV & IV Dexamethasone IV or PO* If aged over 60 of immunosuppressed: Add Co-trimoxazole 30mg/kg IV every 6 hours
Other notes If recent history of travel please discuss with Microbiology *Give IV dexamethasone 10mg QDS IV or PO for 4 days preferably prior to or at the same time as the first dose of antibiotics (if administration delayed dexamethasone may be given up to 12 hours after first dose of antibiotic). Note: Dexamethasone vials contain either 3.3mg or 3.8mg of Dexamethasone depending on the supplier. Suggest using either 9.9mg (3x3.3mg vials) or 9.5mg (2.5x3.8mg vials).
Contact Occupation Health and/or Microbiology regarding prophylaxis for staff members exposed to N. meningitidis
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 6
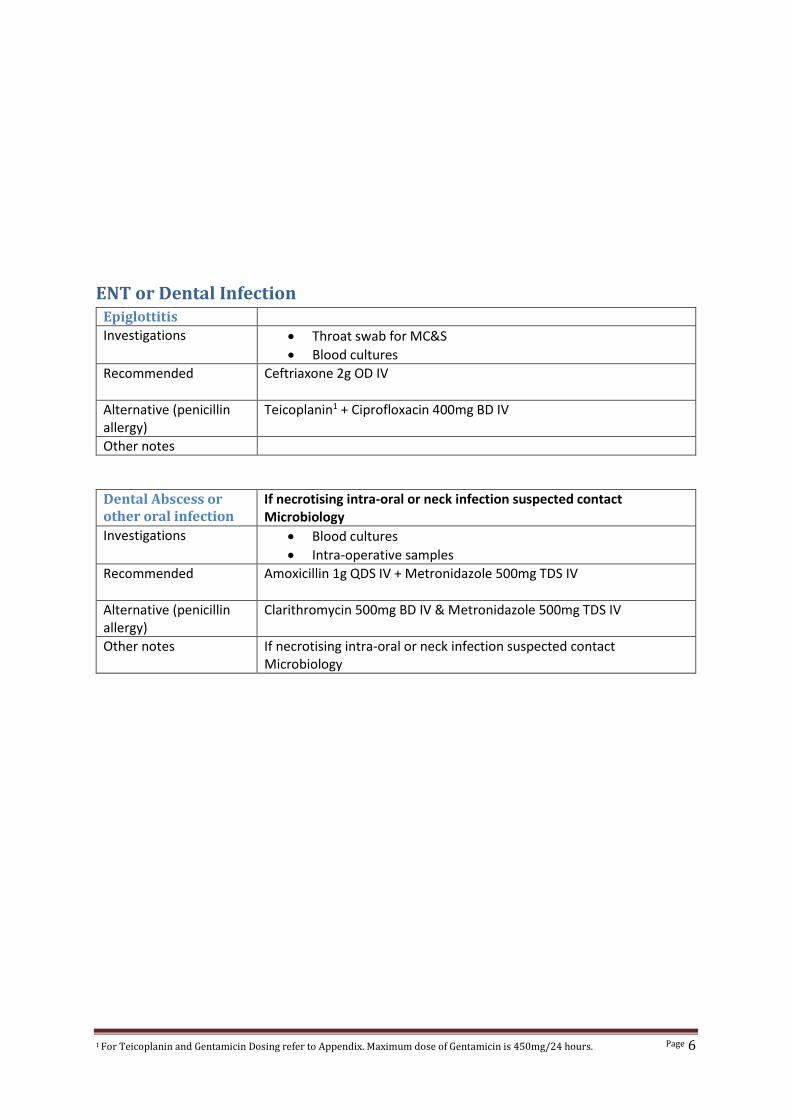
ENT or Dental Infection Epiglottitis
Investigations Throat swab for MC&S
Blood cultures
Recommended Ceftriaxone 2g OD IV
Alternative (penicillin allergy)
Teicoplanin1 + Ciprofloxacin 400mg BD IV
Other notes
Dental Abscess or other oral infection
If necrotising intra-oral or neck infection suspected contact Microbiology
Investigations Blood cultures
Intra-operative samples
Recommended Amoxicillin 1g QDS IV + Metronidazole 500mg TDS IV
Alternative (penicillin allergy)
Clarithromycin 500mg BD IV & Metronidazole 500mg TDS IV
Other notes If necrotising intra-oral or neck infection suspected contact Microbiology
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 7
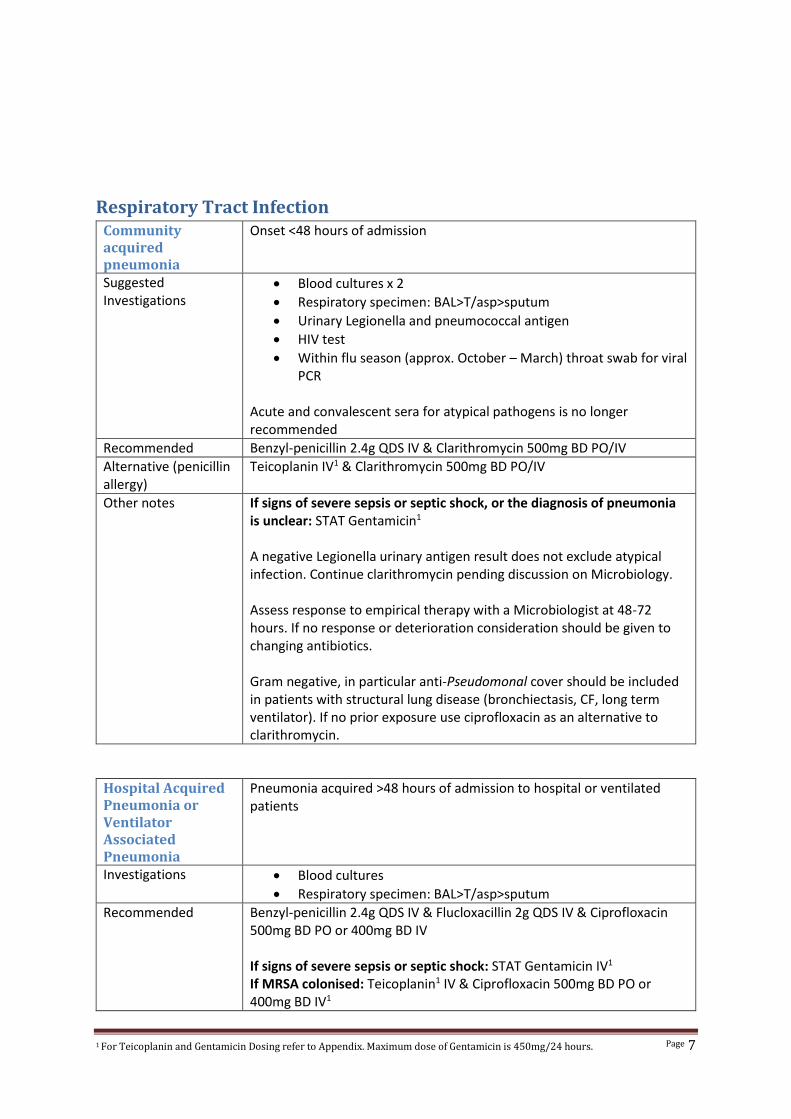
Respiratory Tract Infection Community acquired pneumonia
Onset <48 hours of admission
Suggested Investigations
Blood cultures x 2
Respiratory specimen: BAL>T/asp>sputum
Urinary Legionella and pneumococcal antigen
HIV test
Within flu season (approx. October – March) throat swab for viral PCR
Acute and convalescent sera for atypical pathogens is no longer recommended
Recommended Benzyl-penicillin 2.4g QDS IV & Clarithromycin 500mg BD PO/IV
Alternative (penicillin allergy)
Teicoplanin IV1 & Clarithromycin 500mg BD PO/IV
Other notes If signs of severe sepsis or septic shock, or the diagnosis of pneumonia is unclear: STAT Gentamicin1
A negative Legionella urinary antigen result does not exclude atypical infection. Continue clarithromycin pending discussion on Microbiology. Assess response to empirical therapy with a Microbiologist at 48-72 hours. If no response or deterioration consideration should be given to changing antibiotics. Gram negative, in particular anti-Pseudomonal cover should be included in patients with structural lung disease (bronchiectasis, CF, long term ventilator). If no prior exposure use ciprofloxacin as an alternative to clarithromycin.
Hospital Acquired Pneumonia or Ventilator Associated Pneumonia
Pneumonia acquired >48 hours of admission to hospital or ventilated patients
Investigations Blood cultures
Respiratory specimen: BAL>T/asp>sputum
Recommended Benzyl-penicillin 2.4g QDS IV & Flucloxacillin 2g QDS IV & Ciprofloxacin 500mg BD PO or 400mg BD IV If signs of severe sepsis or septic shock: STAT Gentamicin IV1 If MRSA colonised: Teicoplanin1 IV & Ciprofloxacin 500mg BD PO or 400mg BD IV1
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 8
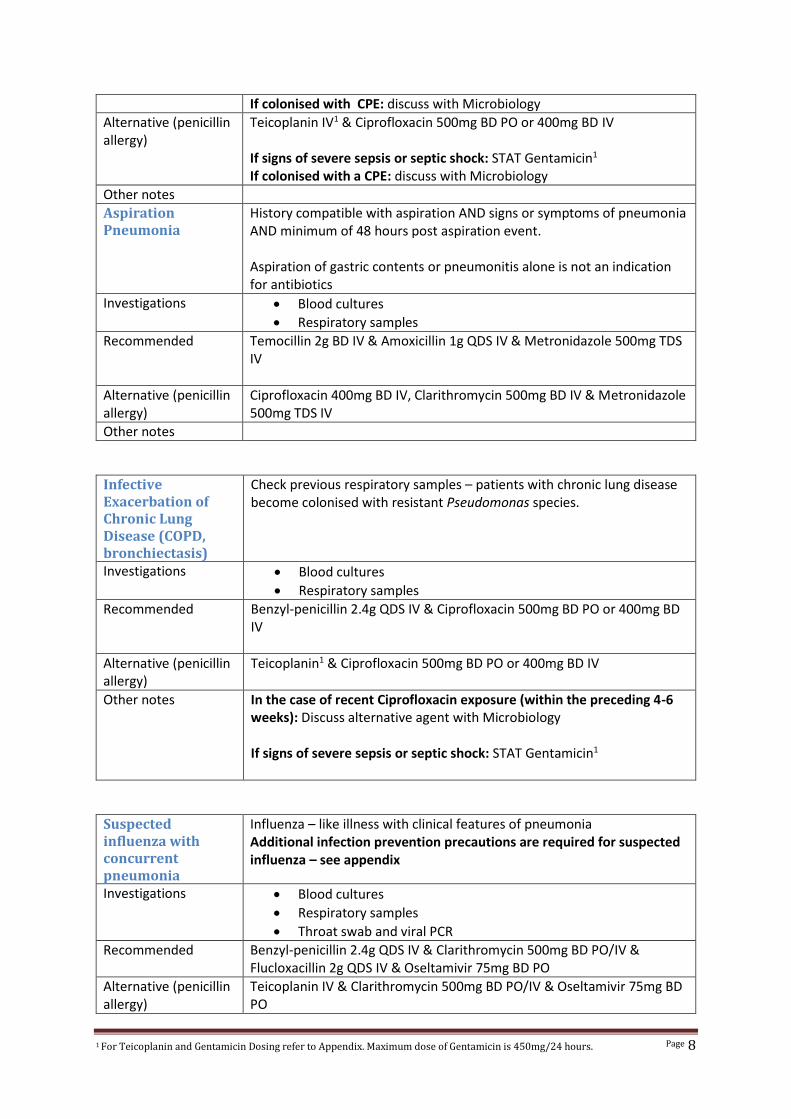
If colonised with CPE: discuss with Microbiology
Alternative (penicillin allergy)
Teicoplanin IV1 & Ciprofloxacin 500mg BD PO or 400mg BD IV If signs of severe sepsis or septic shock: STAT Gentamicin1 If colonised with a CPE: discuss with Microbiology
Other notes
Aspiration Pneumonia
History compatible with aspiration AND signs or symptoms of pneumonia AND minimum of 48 hours post aspiration event. Aspiration of gastric contents or pneumonitis alone is not an indication for antibiotics
Investigations Blood cultures
Respiratory samples
Recommended Temocillin 2g BD IV & Amoxicillin 1g QDS IV & Metronidazole 500mg TDS IV
Alternative (penicillin allergy)
Ciprofloxacin 400mg BD IV, Clarithromycin 500mg BD IV & Metronidazole 500mg TDS IV
Other notes
Infective Exacerbation of Chronic Lung Disease (COPD, bronchiectasis)
Check previous respiratory samples – patients with chronic lung disease become colonised with resistant Pseudomonas species.
Investigations Blood cultures
Respiratory samples
Recommended Benzyl-penicillin 2.4g QDS IV & Ciprofloxacin 500mg BD PO or 400mg BD IV
Alternative (penicillin allergy)
Teicoplanin1 & Ciprofloxacin 500mg BD PO or 400mg BD IV
Other notes In the case of recent Ciprofloxacin exposure (within the preceding 4-6 weeks): Discuss alternative agent with Microbiology If signs of severe sepsis or septic shock: STAT Gentamicin1
Suspected influenza with concurrent pneumonia
Influenza – like illness with clinical features of pneumonia Additional infection prevention precautions are required for suspected influenza – see appendix
Investigations Blood cultures
Respiratory samples
Throat swab and viral PCR
Recommended Benzyl-penicillin 2.4g QDS IV & Clarithromycin 500mg BD PO/IV & Flucloxacillin 2g QDS IV & Oseltamivir 75mg BD PO
Alternative (penicillin allergy)
Teicoplanin IV & Clarithromycin 500mg BD PO/IV & Oseltamivir 75mg BD PO
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 9
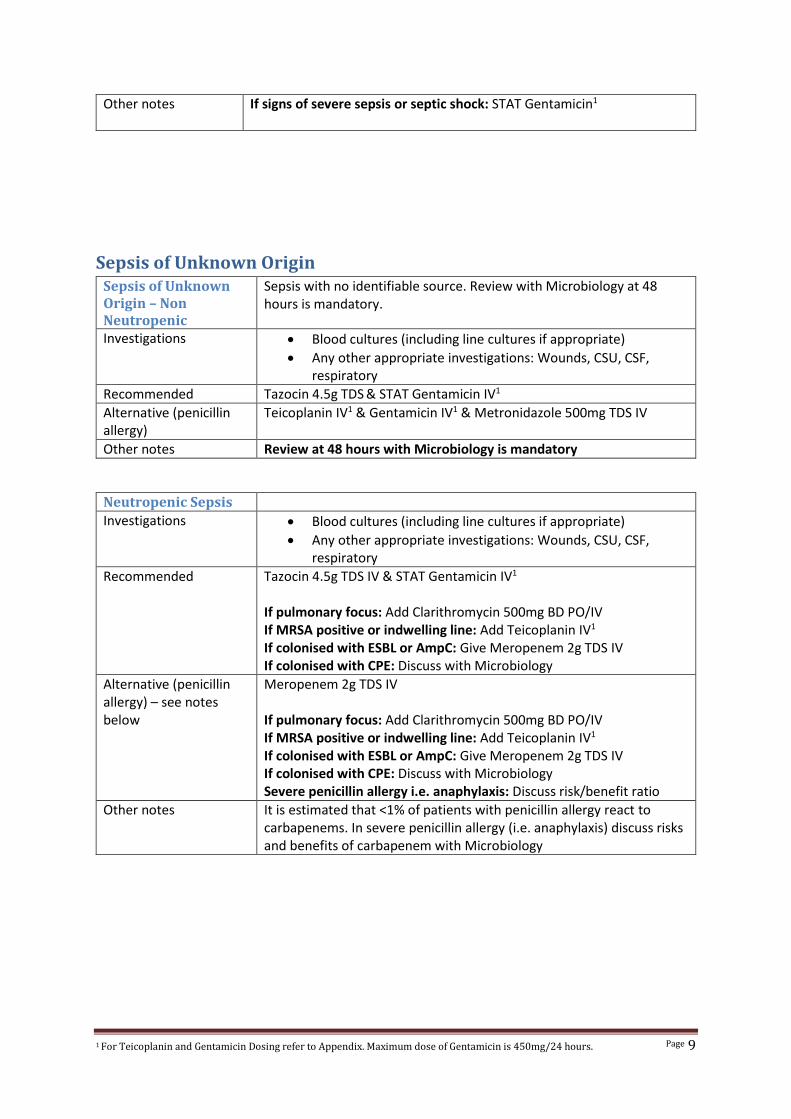
Other notes If signs of severe sepsis or septic shock: STAT Gentamicin1
Sepsis of Unknown Origin Sepsis of Unknown Origin – Non Neutropenic
Sepsis with no identifiable source. Review with Microbiology at 48 hours is mandatory.
Investigations Blood cultures (including line cultures if appropriate)
Any other appropriate investigations: Wounds, CSU, CSF, respiratory
Recommended Tazocin 4.5g TDS & STAT Gentamicin IV1
Alternative (penicillin allergy)
Teicoplanin IV1 & Gentamicin IV1 & Metronidazole 500mg TDS IV
Other notes Review at 48 hours with Microbiology is mandatory
Neutropenic Sepsis
Investigations Blood cultures (including line cultures if appropriate)
Any other appropriate investigations: Wounds, CSU, CSF, respiratory
Recommended Tazocin 4.5g TDS IV & STAT Gentamicin IV1 If pulmonary focus: Add Clarithromycin 500mg BD PO/IV If MRSA positive or indwelling line: Add Teicoplanin IV1
If colonised with ESBL or AmpC: Give Meropenem 2g TDS IV If colonised with CPE: Discuss with Microbiology
Alternative (penicillin allergy) – see notes below
Meropenem 2g TDS IV If pulmonary focus: Add Clarithromycin 500mg BD PO/IV If MRSA positive or indwelling line: Add Teicoplanin IV1
If colonised with ESBL or AmpC: Give Meropenem 2g TDS IV If colonised with CPE: Discuss with Microbiology Severe penicillin allergy i.e. anaphylaxis: Discuss risk/benefit ratio
Other notes It is estimated that <1% of patients with penicillin allergy react to carbapenems. In severe penicillin allergy (i.e. anaphylaxis) discuss risks and benefits of carbapenem with Microbiology
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 10
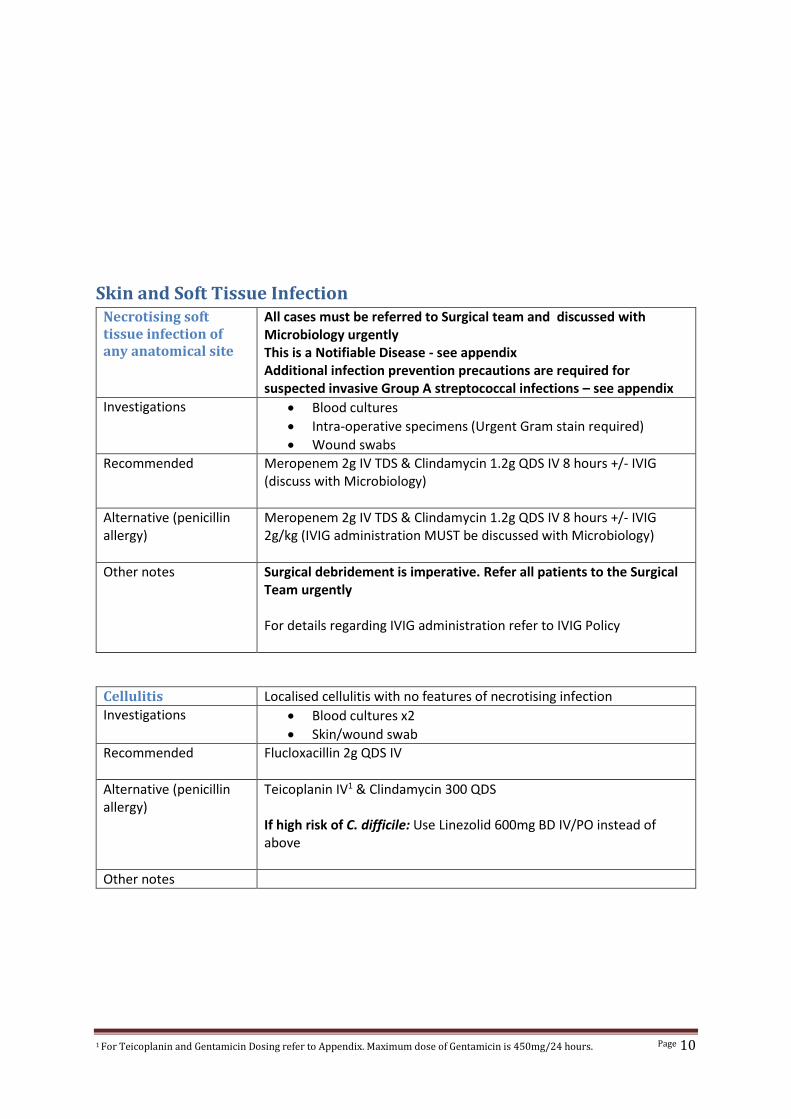
Skin and Soft Tissue Infection Necrotising soft tissue infection of any anatomical site
All cases must be referred to Surgical team and discussed with Microbiology urgently This is a Notifiable Disease - see appendix Additional infection prevention precautions are required for suspected invasive Group A streptococcal infections – see appendix
Investigations Blood cultures
Intra-operative specimens (Urgent Gram stain required)
Wound swabs
Recommended Meropenem 2g IV TDS & Clindamycin 1.2g QDS IV 8 hours +/- IVIG (discuss with Microbiology)
Alternative (penicillin allergy)
Meropenem 2g IV TDS & Clindamycin 1.2g QDS IV 8 hours +/- IVIG 2g/kg (IVIG administration MUST be discussed with Microbiology)
Other notes Surgical debridement is imperative. Refer all patients to the Surgical Team urgently For details regarding IVIG administration refer to IVIG Policy
Cellulitis Localised cellulitis with no features of necrotising infection
Investigations Blood cultures x2
Skin/wound swab
Recommended Flucloxacillin 2g QDS IV
Alternative (penicillin allergy)
Teicoplanin IV1 & Clindamycin 300 QDS If high risk of C. difficile: Use Linezolid 600mg BD IV/PO instead of above
Other notes
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 11
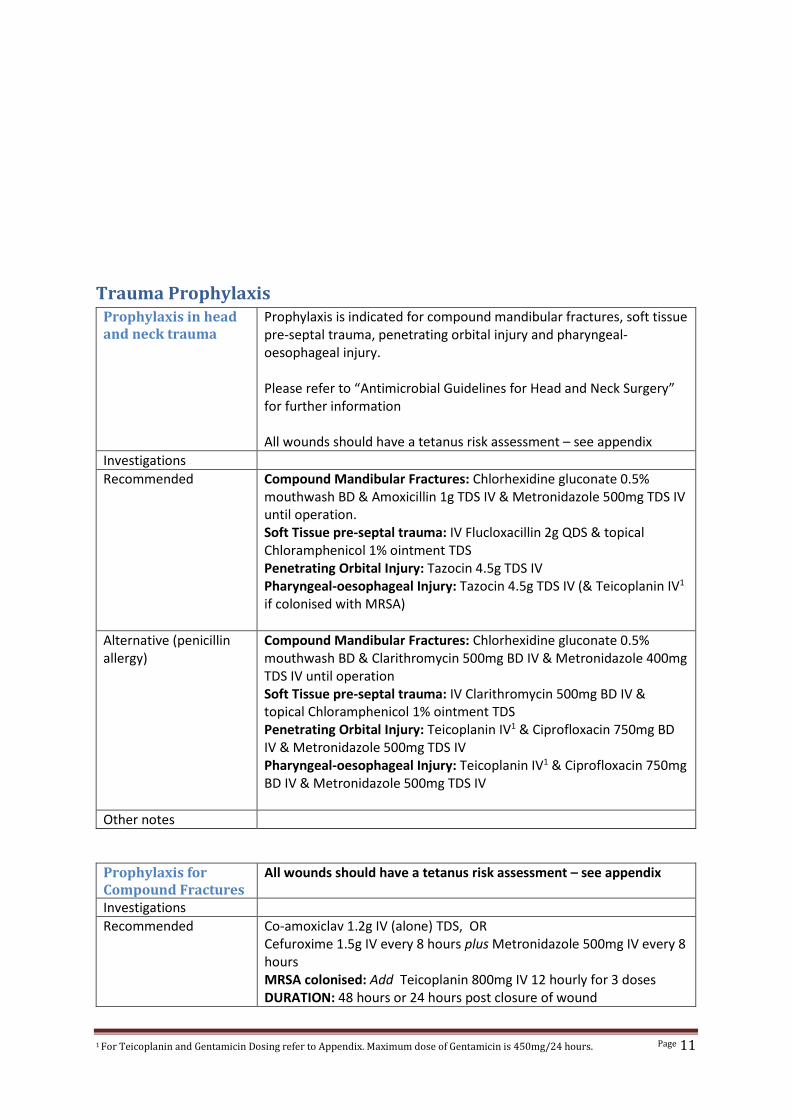
Trauma Prophylaxis Prophylaxis in head and neck trauma
Prophylaxis is indicated for compound mandibular fractures, soft tissue pre-septal trauma, penetrating orbital injury and pharyngeal-oesophageal injury. Please refer to “Antimicrobial Guidelines for Head and Neck Surgery” for further information All wounds should have a tetanus risk assessment – see appendix
Investigations
Recommended Compound Mandibular Fractures: Chlorhexidine gluconate 0.5% mouthwash BD & Amoxicillin 1g TDS IV & Metronidazole 500mg TDS IV until operation. Soft Tissue pre-septal trauma: IV Flucloxacillin 2g QDS & topical Chloramphenicol 1% ointment TDS Penetrating Orbital Injury: Tazocin 4.5g TDS IV Pharyngeal-oesophageal Injury: Tazocin 4.5g TDS IV (& Teicoplanin IV1 if colonised with MRSA)
Alternative (penicillin allergy)
Compound Mandibular Fractures: Chlorhexidine gluconate 0.5% mouthwash BD & Clarithromycin 500mg BD IV & Metronidazole 400mg TDS IV until operation Soft Tissue pre-septal trauma: IV Clarithromycin 500mg BD IV & topical Chloramphenicol 1% ointment TDS Penetrating Orbital Injury: Teicoplanin IV1 & Ciprofloxacin 750mg BD IV & Metronidazole 500mg TDS IV Pharyngeal-oesophageal Injury: Teicoplanin IV1 & Ciprofloxacin 750mg BD IV & Metronidazole 500mg TDS IV
Other notes
Prophylaxis for Compound Fractures
All wounds should have a tetanus risk assessment – see appendix
Investigations
Recommended Co-amoxiclav 1.2g IV (alone) TDS, OR Cefuroxime 1.5g IV every 8 hours plus Metronidazole 500mg IV every 8 hours MRSA colonised: Add Teicoplanin 800mg IV 12 hourly for 3 doses DURATION: 48 hours or 24 hours post closure of wound
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 12
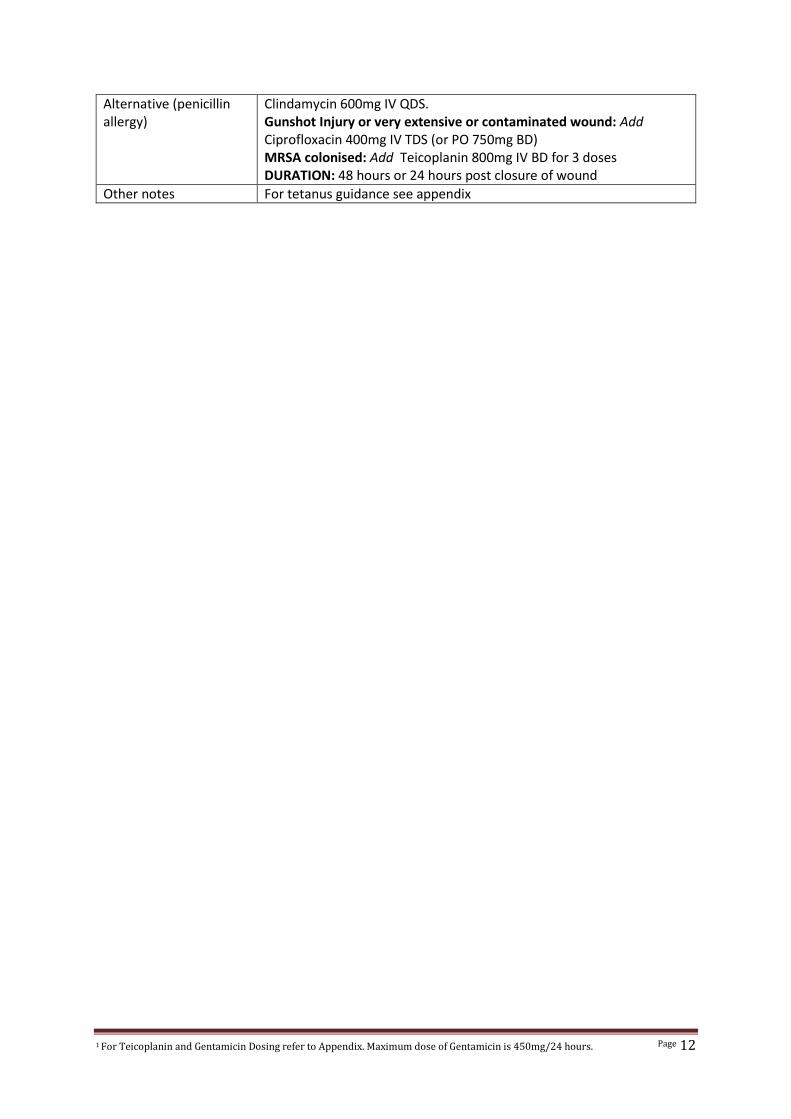
Alternative (penicillin allergy)
Clindamycin 600mg IV QDS. Gunshot Injury or very extensive or contaminated wound: Add Ciprofloxacin 400mg IV TDS (or PO 750mg BD) MRSA colonised: Add Teicoplanin 800mg IV BD for 3 doses DURATION: 48 hours or 24 hours post closure of wound
Other notes For tetanus guidance see appendix
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 13
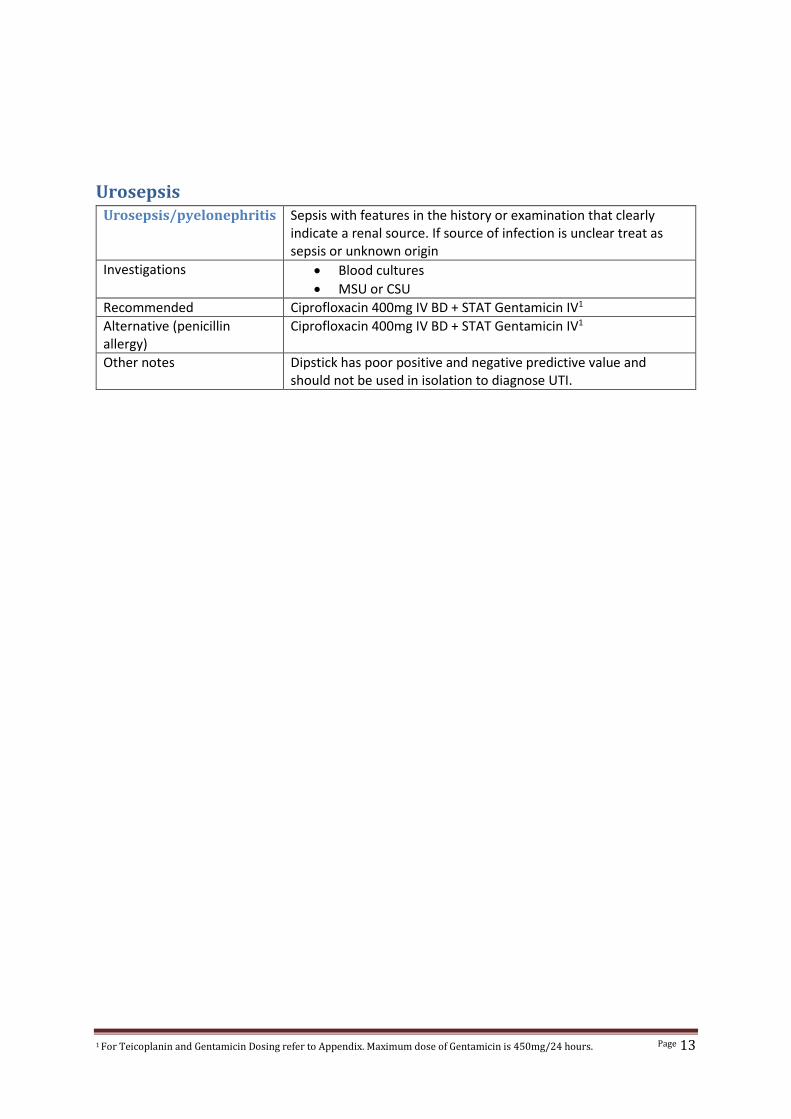
Urosepsis Urosepsis/pyelonephritis Sepsis with features in the history or examination that clearly
indicate a renal source. If source of infection is unclear treat as sepsis or unknown origin
Investigations Blood cultures
MSU or CSU
Recommended Ciprofloxacin 400mg IV BD + STAT Gentamicin IV1
Alternative (penicillin allergy)
Ciprofloxacin 400mg IV BD + STAT Gentamicin IV1
Other notes Dipstick has poor positive and negative predictive value and should not be used in isolation to diagnose UTI.
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 14
Appendix
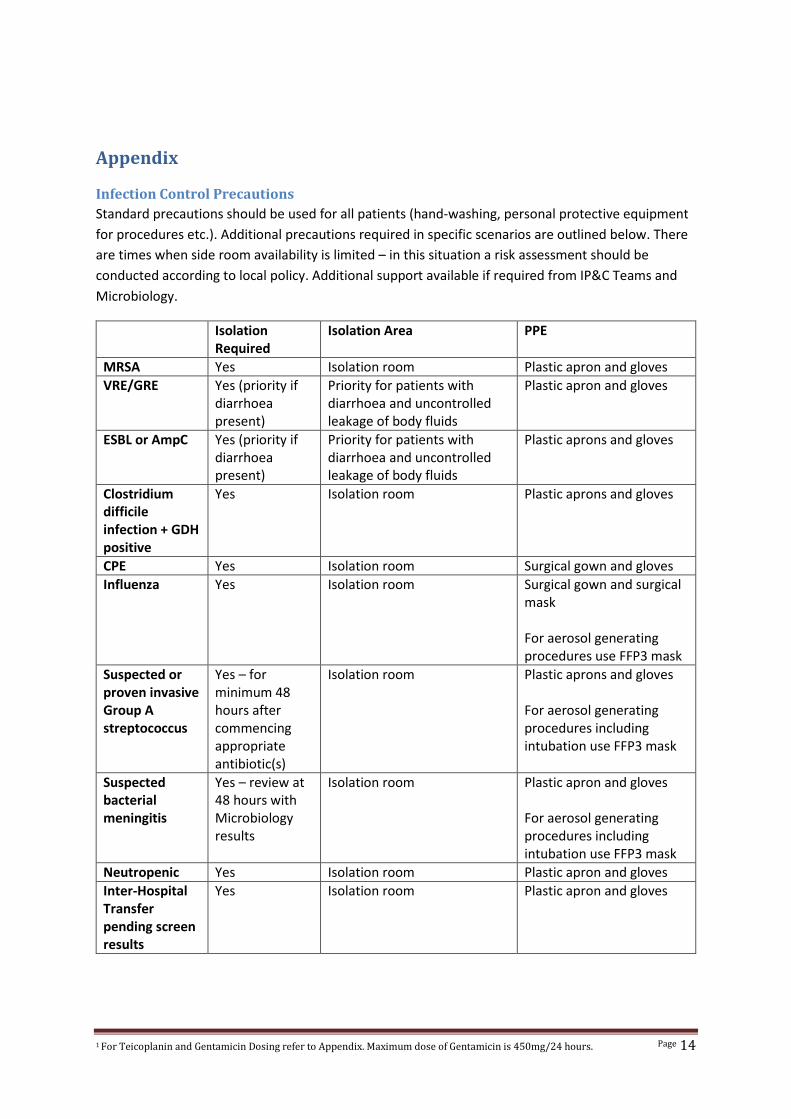
Infection Control Precautions
Standard precautions should be used for all patients (hand-washing, personal protective equipment
for procedures etc.). Additional precautions required in specific scenarios are outlined below. There
are times when side room availability is limited – in this situation a risk assessment should be
conducted according to local policy. Additional support available if required from IP&C Teams and
Microbiology.
Isolation Required
Isolation Area PPE
MRSA Yes Isolation room Plastic apron and gloves
VRE/GRE Yes (priority if diarrhoea present)
Priority for patients with diarrhoea and uncontrolled leakage of body fluids
Plastic apron and gloves
ESBL or AmpC Yes (priority if diarrhoea present)
Priority for patients with diarrhoea and uncontrolled leakage of body fluids
Plastic aprons and gloves
Clostridium difficile infection + GDH positive
Yes Isolation room Plastic aprons and gloves
CPE Yes Isolation room Surgical gown and gloves
Influenza Yes Isolation room Surgical gown and surgical mask For aerosol generating procedures use FFP3 mask
Suspected or proven invasive Group A streptococcus
Yes – for minimum 48 hours after commencing appropriate antibiotic(s)
Isolation room Plastic aprons and gloves For aerosol generating procedures including intubation use FFP3 mask
Suspected bacterial meningitis
Yes – review at 48 hours with Microbiology results
Isolation room Plastic apron and gloves For aerosol generating procedures including intubation use FFP3 mask
Neutropenic Yes Isolation room Plastic apron and gloves
Inter-Hospital Transfer pending screen results
Yes Isolation room Plastic apron and gloves

1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 15
Weekly Screening
Patients on ITU should have a multidrug resistant organism (MDRO) screen (rectal & groin AND nose
& throat) for ESBL, AmpC, MRSA, VRE and CPE colonisation on admission and weekly thereafter.
Transfers It is essential that MDRO colonisation status from referring Trust is ascertained prior to transfer.
Refer to local policy regarding isolation. In patients transferred from Aintree ITU, Royal ITU or HDU,
Liverpool Heart and Chest ITU or Walton Centre Horsley ITU consideration may be given to early
removal from side room - discuss with Microbiology or IP&C Team.
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 16
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 17
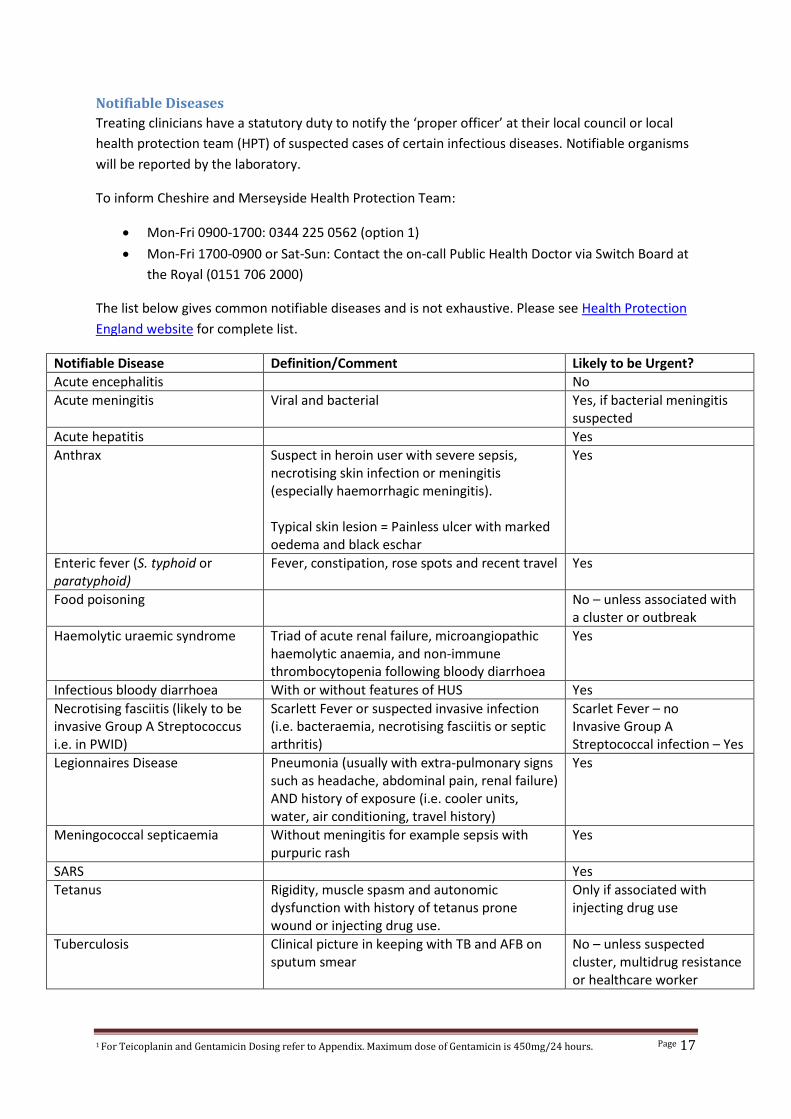
Notifiable Diseases
Treating clinicians have a statutory duty to notify the ‘proper officer’ at their local council or local
health protection team (HPT) of suspected cases of certain infectious diseases. Notifiable organisms
will be reported by the laboratory.
To inform Cheshire and Merseyside Health Protection Team:
Mon-Fri 0900-1700: 0344 225 0562 (option 1)
Mon-Fri 1700-0900 or Sat-Sun: Contact the on-call Public Health Doctor via Switch Board at
the Royal (0151 706 2000)
The list below gives common notifiable diseases and is not exhaustive. Please see Health Protection
England website for complete list.
Notifiable Disease Definition/Comment Likely to be Urgent?
Acute encephalitis No
Acute meningitis Viral and bacterial Yes, if bacterial meningitis suspected
Acute hepatitis Yes
Anthrax Suspect in heroin user with severe sepsis, necrotising skin infection or meningitis (especially haemorrhagic meningitis). Typical skin lesion = Painless ulcer with marked oedema and black eschar
Yes
Enteric fever (S. typhoid or paratyphoid)
Fever, constipation, rose spots and recent travel Yes
Food poisoning No – unless associated with a cluster or outbreak
Haemolytic uraemic syndrome Triad of acute renal failure, microangiopathic haemolytic anaemia, and non-immune thrombocytopenia following bloody diarrhoea
Yes
Infectious bloody diarrhoea With or without features of HUS Yes
Necrotising fasciitis (likely to be invasive Group A Streptococcus i.e. in PWID)
Scarlett Fever or suspected invasive infection (i.e. bacteraemia, necrotising fasciitis or septic arthritis)
Scarlet Fever – no Invasive Group A Streptococcal infection – Yes
Legionnaires Disease Pneumonia (usually with extra-pulmonary signs such as headache, abdominal pain, renal failure) AND history of exposure (i.e. cooler units, water, air conditioning, travel history)
Yes
Meningococcal septicaemia Without meningitis for example sepsis with purpuric rash
Yes
SARS Yes
Tetanus Rigidity, muscle spasm and autonomic dysfunction with history of tetanus prone wound or injecting drug use.
Only if associated with injecting drug use
Tuberculosis Clinical picture in keeping with TB and AFB on sputum smear
No – unless suspected cluster, multidrug resistance or healthcare worker
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 18
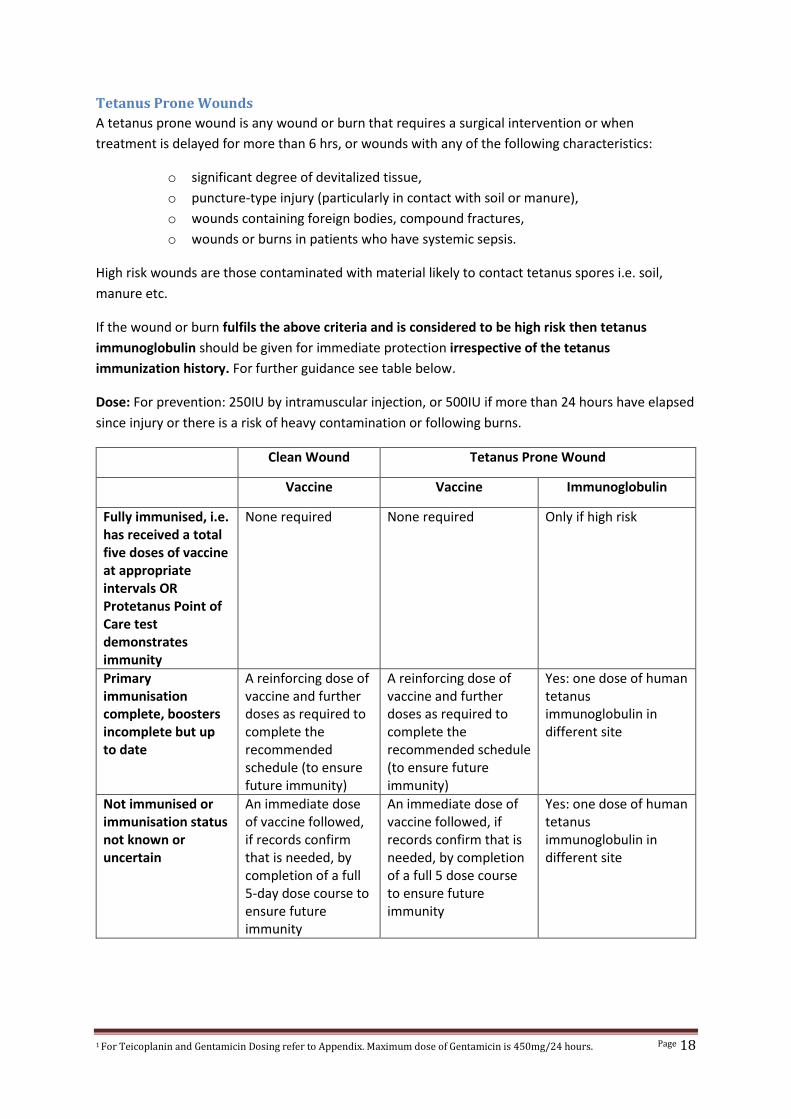
Tetanus Prone Wounds
A tetanus prone wound is any wound or burn that requires a surgical intervention or when
treatment is delayed for more than 6 hrs, or wounds with any of the following characteristics:
o significant degree of devitalized tissue,
o puncture-type injury (particularly in contact with soil or manure),
o wounds containing foreign bodies, compound fractures,
o wounds or burns in patients who have systemic sepsis.
High risk wounds are those contaminated with material likely to contact tetanus spores i.e. soil,
manure etc.
If the wound or burn fulfils the above criteria and is considered to be high risk then tetanus
immunoglobulin should be given for immediate protection irrespective of the tetanus
immunization history. For further guidance see table below.
Dose: For prevention: 250IU by intramuscular injection, or 500IU if more than 24 hours have elapsed
since injury or there is a risk of heavy contamination or following burns.
Clean Wound Tetanus Prone Wound
Vaccine Vaccine Immunoglobulin
Fully immunised, i.e. has received a total five doses of vaccine at appropriate intervals OR Protetanus Point of Care test demonstrates immunity
None required None required Only if high risk
Primary immunisation complete, boosters incomplete but up to date
A reinforcing dose of vaccine and further doses as required to complete the recommended schedule (to ensure future immunity)
A reinforcing dose of vaccine and further doses as required to complete the recommended schedule (to ensure future immunity)
Yes: one dose of human tetanus immunoglobulin in different site
Not immunised or immunisation status not known or uncertain
An immediate dose of vaccine followed, if records confirm that is needed, by completion of a full 5-day dose course to ensure future immunity
An immediate dose of vaccine followed, if records confirm that is needed, by completion of a full 5 dose course to ensure future immunity
Yes: one dose of human tetanus immunoglobulin in different site
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 19
Processing Urgent Specimens Out of Hours (Mon-Fri 1630-0900 and Sat-Sun)
The following specimens will be processed urgently out of hours: CSF, joint aspirates, ascitic fluid,
and tissue specimens in suspected necrotising fasciitis. Other specimens may be processed upon
request.
For urgent specimens taken out-of hours:
1) Inform the On-call Microbiology Biomedical Scientist at Royal Liverpool University Hospital
via Switch board (0151 706 2000)
2) Specimen transport to Laboratory:
a. For Royal ITU or HDU: Pod specimen to pod no. 710
b. For Aintree ITU: Take the specimen to Specimen Reception at Aintree (Ground floor
of the main corridor, opposite A&E). The BMS will arrange transport to Liverpool
Clinical Laboratories
3) The on-call BMS or Microbiologist will ring ITU with the result once processed

1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 20
1 For Teicoplanin and Gentamicin Dosing refer to Appendix. Maximum dose of Gentamicin is 450mg/24 hours. Page 21
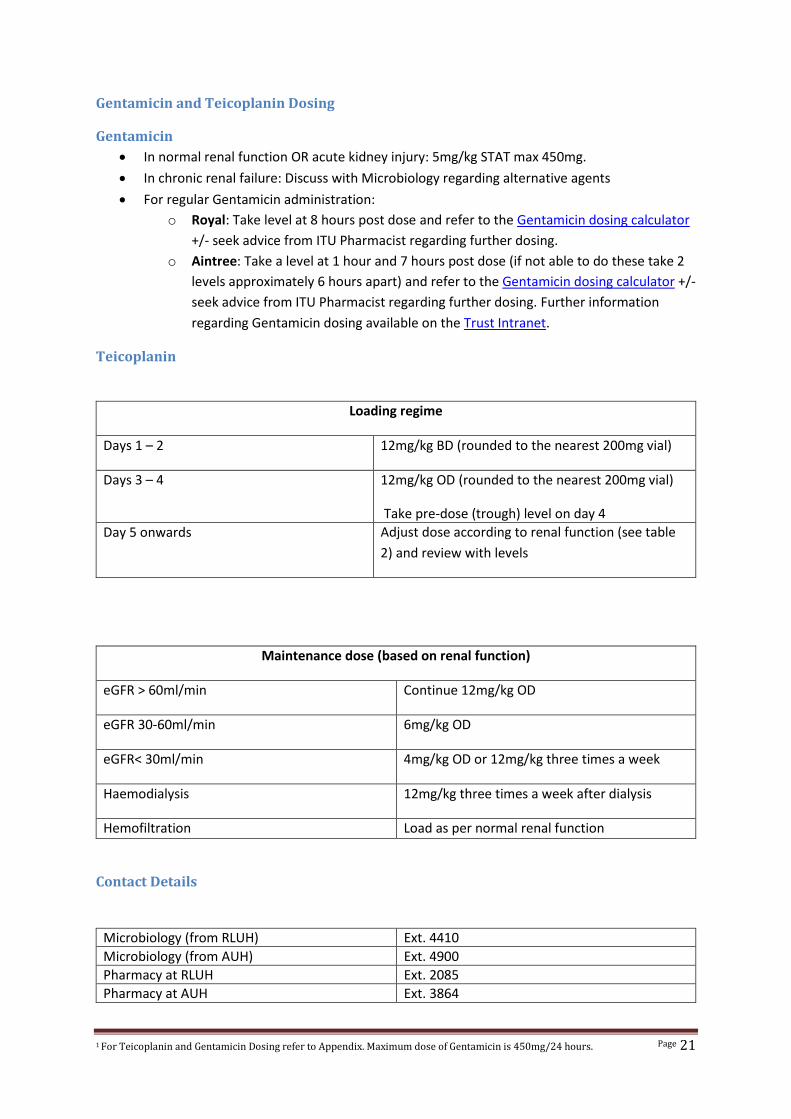
Gentamicin and Teicoplanin Dosing
Gentamicin
In normal renal function OR acute kidney injury: 5mg/kg STAT max 450mg.
In chronic renal failure: Discuss with Microbiology regarding alternative agents
For regular Gentamicin administration:
o Royal: Take level at 8 hours post dose and refer to the Gentamicin dosing calculator
+/- seek advice from ITU Pharmacist regarding further dosing.
o Aintree: Take a level at 1 hour and 7 hours post dose (if not able to do these take 2
levels approximately 6 hours apart) and refer to the Gentamicin dosing calculator +/-
seek advice from ITU Pharmacist regarding further dosing. Further information
regarding Gentamicin dosing available on the Trust Intranet.
Teicoplanin
Loading regime
Days 1 – 2 12mg/kg BD (rounded to the nearest 200mg vial)
Days 3 – 4 12mg/kg OD (rounded to the nearest 200mg vial)
Take pre-dose (trough) level on day 4
Day 5 onwards Adjust dose according to renal function (see table
2) and review with levels
Maintenance dose (based on renal function)
eGFR > 60ml/min Continue 12mg/kg OD
eGFR 30-60ml/min 6mg/kg OD
eGFR< 30ml/min 4mg/kg OD or 12mg/kg three times a week
Haemodialysis 12mg/kg three times a week after dialysis
Hemofiltration Load as per normal renal function
Contact Details
Microbiology (from RLUH) Ext. 4410
Microbiology (from AUH) Ext. 4900
Pharmacy at RLUH Ext. 2085
Pharmacy at AUH Ext. 3864