Embed Size (px)
Citation preview
2018
EMPLOYEE BENEFITS
HIGHLIGHTS

2
3 Benefit resource directory
4 Open enrollment / new hires
5 Healthcare reform overview
6-9 Health insurance
10 Dental insurance
11 Vision insurance
12 Flexible spending account (FSA)
13-17 Get the most of your benefits
Member services website registration
Telemedicine
Wellness program GO365™
18 Life and AD&D Insurance
19 Short Term & Long Term Disability
20 Employee assistance programs (EAP)
21 Supplemental insurance
22-24 Federal Laws/Disclosures/Notices
Medicare Part-D Section 125 HIPAA CHIP-Children’s Health Insurance Women’s Health & Cancer Rights Act Newborn’s and Mother’s Health Protection Act Cobra
25-26 Education
Prescription Discounts
Where to go for care
27-30 Health & Wellness
Importance of prevention
Know your numbers
Maintaining healthy weight
Managing stress
31 Demographics
3
HEALTH INSURANCE
Humana (866) 427-7478
www.humama.com
DENTAL INSURANCE
MetLife DHMO: (800) 880-1800 DPPO: (800) 275-4638
www.metlife.com
VISION INSURANCE
MetLife (855) 638-3931
www.metlife.com
LIFE / AD&D & DISABILITY INSURANCE
Lincoln Financial Group (800) 423-2765
www.lfg.com
EMPLOYEE ASSISTANCE PROGRAM
Aetna Resources for Living (800) 272-7252
www.mylifevalues.com
SUPPLEMENTAL INSURANCE
AFLAC Shirley Sastre Souto
[email protected] (305) 801-9093 www.aflac.com
HUMAN RESOURCES DEPARTMENT
Cassandra Fulwood Vice President of Human Resource [email protected]
(561) 848-7200
Tamatha R. Dunlap Director of Human Resources
[email protected] (561) 848-7200 ext 3222
SAPOZNIK INSURANCE
Betty Goodman VP, Benefits Consultants
Priscilla Porras Benefits Account Champion
1100 NE 163 Street North Miami Beach, FL 33162
Telephone: (877) 948-8887 Fax: (305) 949-1099
www.sapoznik.com
3 Benefit resource directory
4 Open enrollment / new hires
5 Healthcare reform overview
6-9 Health insurance
10 Dental insurance
11 Vision insurance
12 Flexible spending account (FSA)
13-17 Get the most of your benefits
Member services website registration
Telemedicine
Wellness program GO365™
18 Life and AD&D Insurance
19 Short Term & Long Term Disability
20 Employee assistance programs (EAP)
21 Supplemental insurance
22-24 Federal Laws/Disclosures/Notices
Medicare Part-D Section 125 HIPAA CHIP-Children’s Health Insurance Women’s Health & Cancer Rights Act Newborn’s and Mother’s Health Protection Act Cobra
25-26 Education
Prescription Discounts
Where to go for care
27-30 Health & Wellness
Importance of prevention
Know your numbers
Maintaining healthy weight
Managing stress
31 Demographics
PLEASE NOTE: This Benefit Highlight Booklet is solely intended as a high-level overview and general reference guide on your employee benefits. This booklet is NOT your Summary of Benefits and Coverage (SBC) document required by the Affordable Care Act of 2010. As an enrollee, your actual SBC will be provided under separate cover, by your health carrier.
4
All new hire enrollments
are effective the 1st of the month
following 60 days of date of hire
Must notify HR within 30 days of qualifying event
Medical
Dental
Vision
Employer Paid Life Insurance
Voluntary Life Insurance
Short Term Disability
Long Term Disability
Employee Assistance Program
(EAP)
Supplemental Insurance
Retirement Plan
Annual Opportunity to:
Add, change, or drop dependents
Qualifying Events:
Marriage
Divorce
Legal separation
Birth of child
Change in employment status
Dependent ceasing to be eligible
Death
5
The law is made up of two major components:
I. Employer Mandate
To comply with the law, employers must meet two requirements:
An employee’s required contribution cannot exceed 9.69% of his or her income for 2017
The plan must pay for at least 60 %, on average, of covered health expenses
II. Individual Mandate
Under the health care reform law, beginning January 1, 2014,
all individuals must have minimum essential coverage.
“Minimum Essential Coverage" if they have a:
� Government-sponsored plan
� Employer-sponsored plan
� Individual plan
2017 Penalty: $695 per uninsured adult in the household ($347.50 per child under 18)
or 2.5% of your yearly household income, whichever is greater. ($2,085 maximum
penalty).
For tax year 2018 and beyond, the penalty amounts have not been announced, but are
expected to increase.
On March 23, 2010, President Barack Obama signed into law the Patient
Protection and Affordable Care Act (PPACA) also known as ACA.
All Plans offered are compliant with Employer Mandate
If enrolled in any of our plans, you are compliant with Individual Mandate
6
H U M A N A | w w w . h u m a n a . c o m | ( 8 6 6 ) 4 2 7 - 7 4 7 8
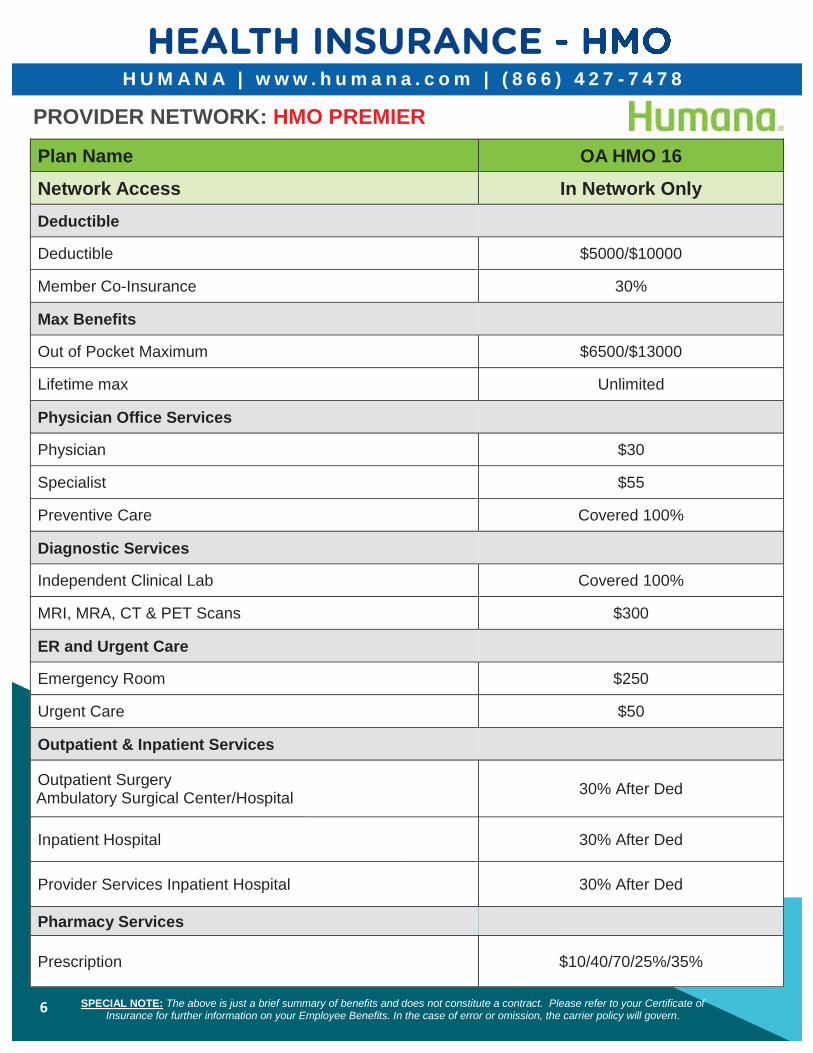
PROVIDER NETWORK: HMO PREMIER
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
Plan Name OA HMO 16
Network Access In Network Only
Deductible
Deductible $5000/$10000
Member Co-Insurance 30%
Max Benefits
Out of Pocket Maximum $6500/$13000
Lifetime max Unlimited
Physician Office Services
Physician $30
Specialist $55
Preventive Care Covered 100%
Diagnostic Services
Independent Clinical Lab Covered 100%
MRI, MRA, CT & PET Scans $300
ER and Urgent Care
Emergency Room $250
Urgent Care $50
Outpatient & Inpatient Services
Outpatient Surgery Ambulatory Surgical Center/Hospital
30% After Ded
Inpatient Hospital 30% After Ded
Provider Services Inpatient Hospital 30% After Ded
Pharmacy Services
Prescription $10/40/70/25%/35%
7
H U M A N A | w w w . h u m a n a . c o m | ( 8 6 6 ) 4 2 7 - 7 4 7 8
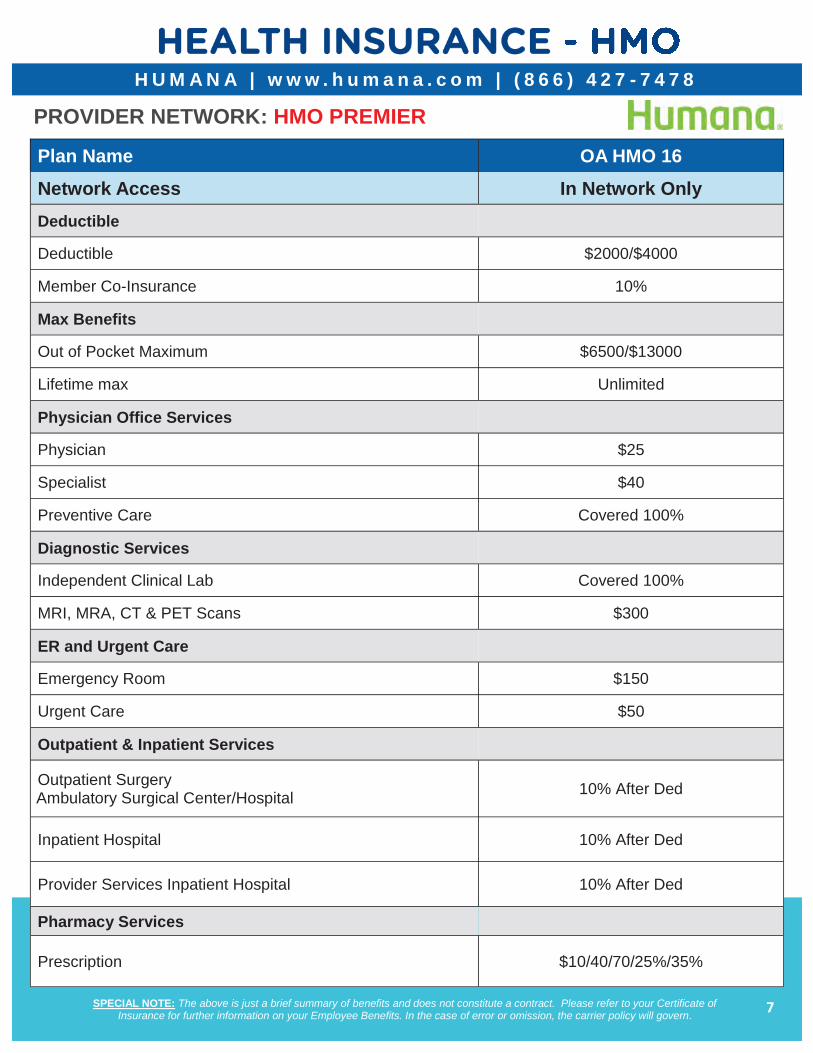
PROVIDER NETWORK: HMO PREMIER
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
Plan Name OA HMO 16
Network Access In Network Only
Deductible
Deductible $2000/$4000
Member Co-Insurance 10%
Max Benefits
Out of Pocket Maximum $6500/$13000
Lifetime max Unlimited
Physician Office Services
Physician $25
Specialist $40
Preventive Care Covered 100%
Diagnostic Services
Independent Clinical Lab Covered 100%
MRI, MRA, CT & PET Scans $300
ER and Urgent Care
Emergency Room $150
Urgent Care $50
Outpatient & Inpatient Services
Outpatient Surgery Ambulatory Surgical Center/Hospital
10% After Ded
Inpatient Hospital 10% After Ded
Provider Services Inpatient Hospital 10% After Ded
Pharmacy Services
Prescription $10/40/70/25%/35%
8
H U M A N A | w w w . h u m a n a . c o m | ( 8 6 6 ) 4 2 7 - 7 4 7 8
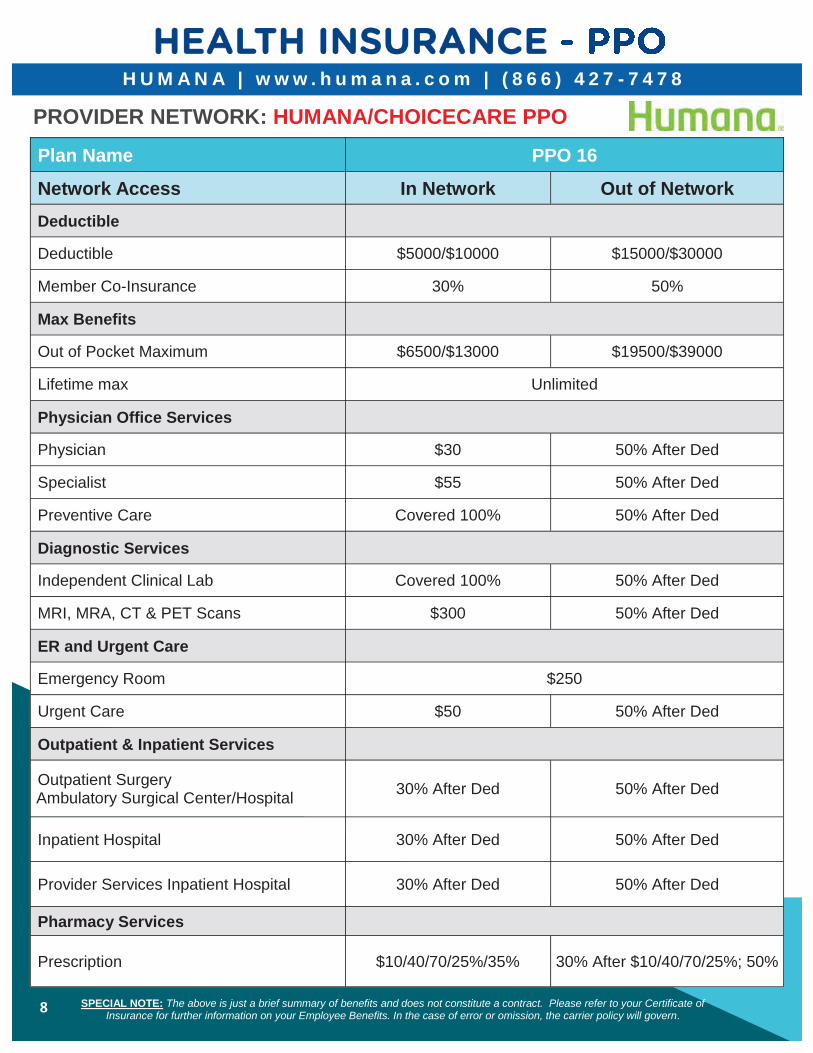
PROVIDER NETWORK: HUMANA/CHOICECARE PPO
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
Plan Name PPO 16
Network Access In Network Out of Network
Deductible
Deductible $5000/$10000 $15000/$30000
Member Co-Insurance 30% 50%
Max Benefits
Out of Pocket Maximum $6500/$13000 $19500/$39000
Lifetime max Unlimited
Physician Office Services
Physician $30 50% After Ded
Specialist $55 50% After Ded
Preventive Care Covered 100% 50% After Ded
Diagnostic Services
Independent Clinical Lab Covered 100% 50% After Ded
MRI, MRA, CT & PET Scans $300 50% After Ded
ER and Urgent Care
Emergency Room $250
Urgent Care $50 50% After Ded
Outpatient & Inpatient Services
Outpatient Surgery Ambulatory Surgical Center/Hospital
30% After Ded 50% After Ded
Inpatient Hospital 30% After Ded 50% After Ded
Provider Services Inpatient Hospital 30% After Ded 50% After Ded
Pharmacy Services
Prescription $10/40/70/25%/35% 30% After $10/40/70/25%; 50%
9
H U M A N A | w w w . h u m a n a . c o m | ( 8 6 6 ) 4 2 7 - 7 4 7 8
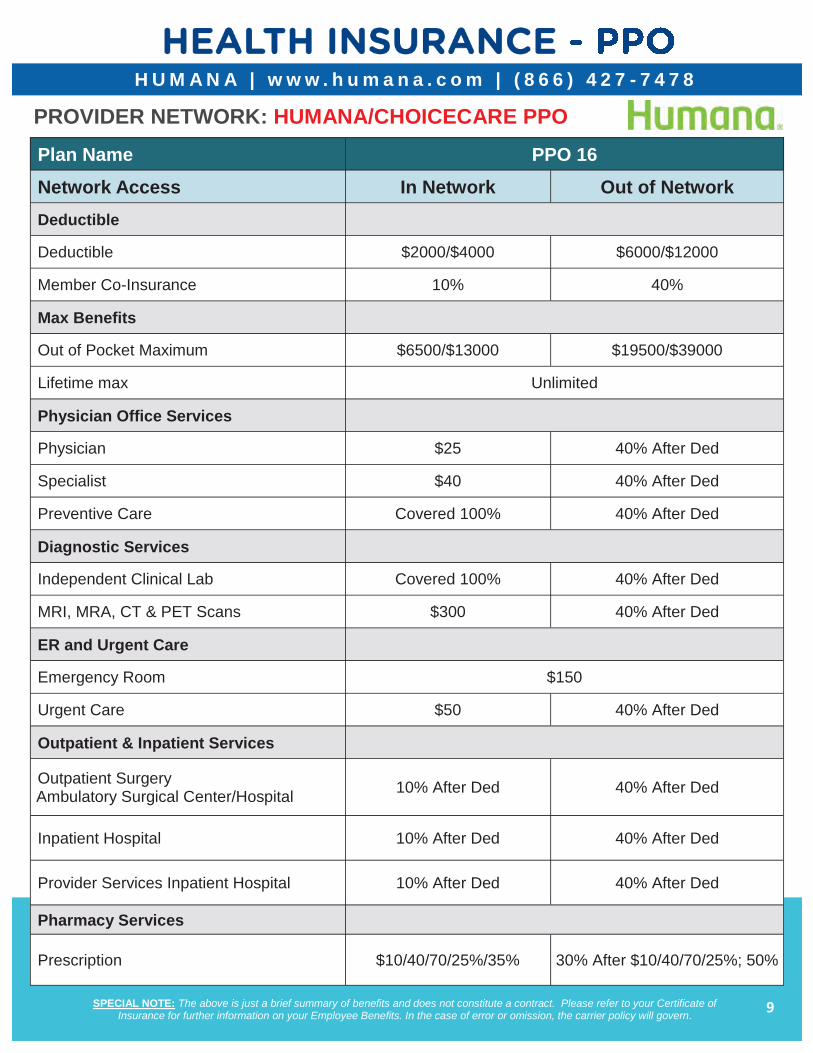
PROVIDER NETWORK: HUMANA/CHOICECARE PPO
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
Plan Name PPO 16
Network Access In Network Out of Network
Deductible
Deductible $2000/$4000 $6000/$12000
Member Co-Insurance 10% 40%
Max Benefits
Out of Pocket Maximum $6500/$13000 $19500/$39000
Lifetime max Unlimited
Physician Office Services
Physician $25 40% After Ded
Specialist $40 40% After Ded
Preventive Care Covered 100% 40% After Ded
Diagnostic Services
Independent Clinical Lab Covered 100% 40% After Ded
MRI, MRA, CT & PET Scans $300 40% After Ded
ER and Urgent Care
Emergency Room $150
Urgent Care $50 40% After Ded
Outpatient & Inpatient Services
Outpatient Surgery Ambulatory Surgical Center/Hospital
10% After Ded 40% After Ded
Inpatient Hospital 10% After Ded 40% After Ded
Provider Services Inpatient Hospital 10% After Ded 40% After Ded
Pharmacy Services
Prescription $10/40/70/25%/35% 30% After $10/40/70/25%; 50%
10
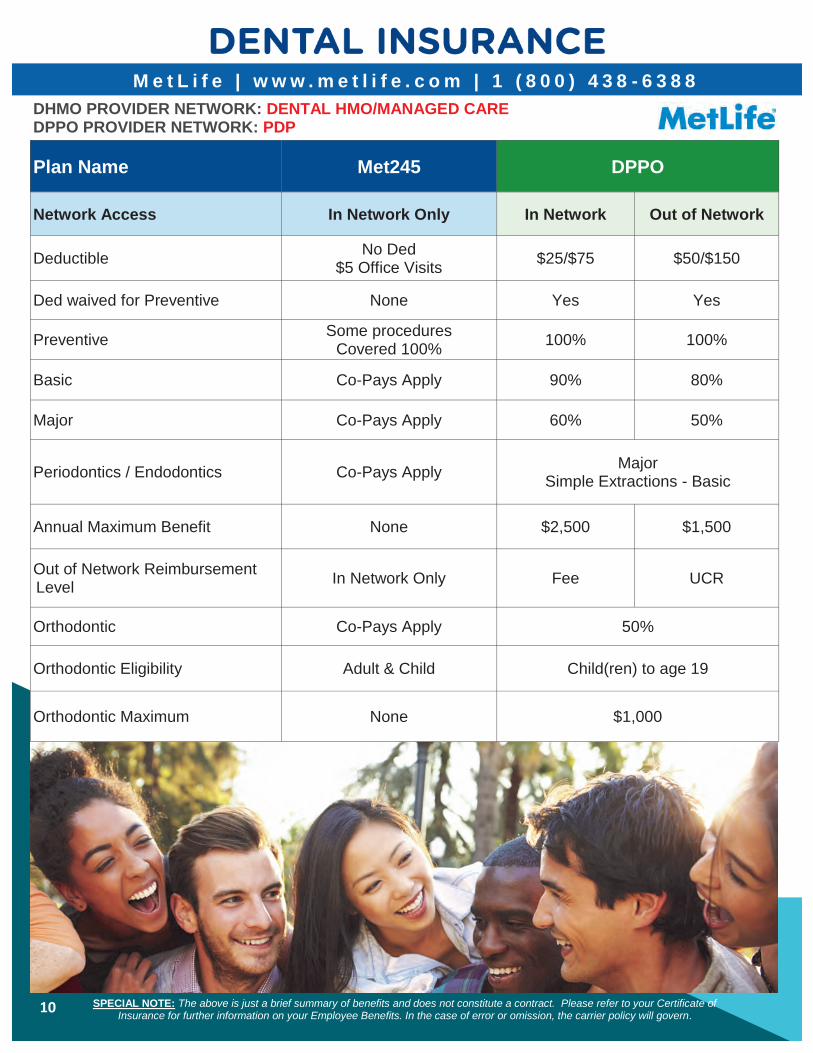
M e t L i f e | w w w . m e t l i f e . c o m | 1 ( 8 0 0 ) 4 3 8 - 6 3 8 8
Plan Name Met245 DPPO
Network Access In Network Only In Network Out of Network
Deductible No Ded
$5 Office Visits $25/$75 $50/$150
Ded waived for Preventive None Yes Yes
Preventive Some procedures
Covered 100% 100% 100%
Basic Co-Pays Apply 90% 80%
Major Co-Pays Apply 60% 50%
Periodontics / Endodontics Co-Pays Apply Major
Simple Extractions - Basic
Annual Maximum Benefit None $2,500 $1,500
Out of Network Reimbursement Level
In Network Only Fee UCR
Orthodontic Co-Pays Apply 50%
Orthodontic Eligibility Adult & Child Child(ren) to age 19
Orthodontic Maximum None $1,000
DHMO PROVIDER NETWORK: DENTAL HMO/MANAGED CARE DPPO PROVIDER NETWORK: PDP
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
11
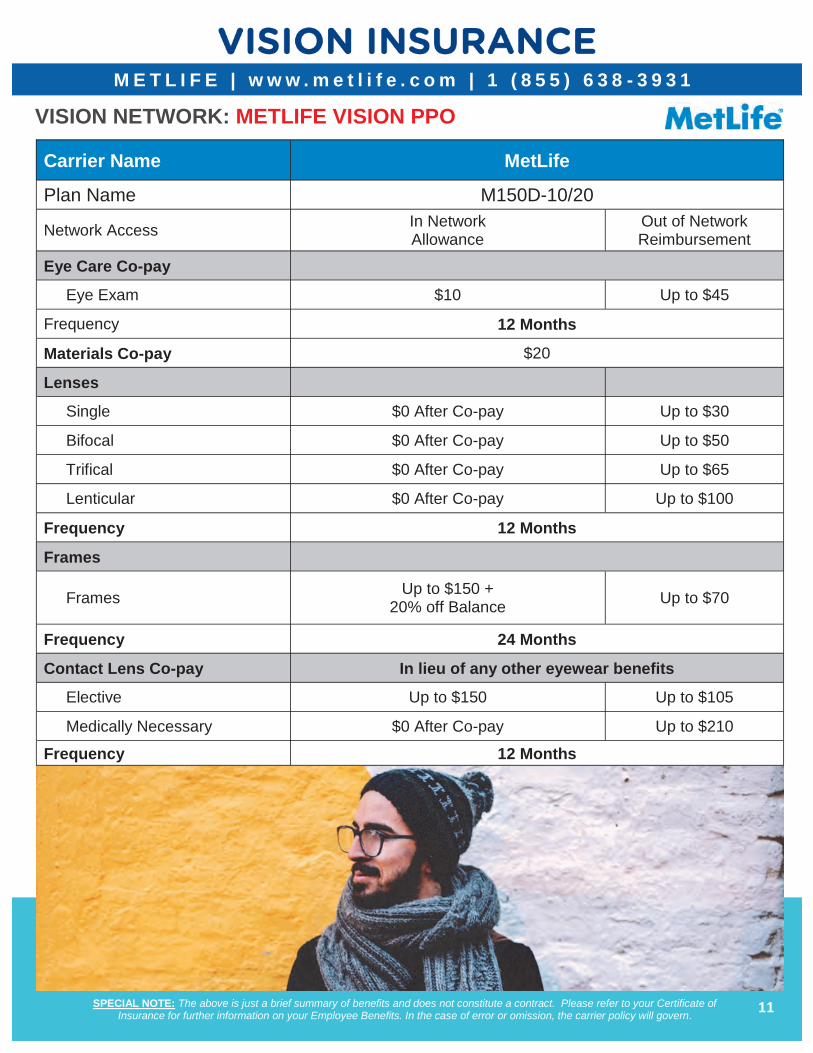
M E T L I F E | w w w . m e t l i f e . c o m | 1 ( 8 5 5 ) 6 3 8 - 3 9 3 1
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
VISION NETWORK: METLIFE VISION PPO
Carrier Name MetLife
Plan Name M150D-10/20
Network Access In Network Allowance
Out of Network Reimbursement
Eye Care Co-pay
Eye Exam $10 Up to $45
Frequency 12 Months
Materials Co-pay $20
Lenses
Single $0 After Co-pay Up to $30
Bifocal $0 After Co-pay Up to $50
Trifical $0 After Co-pay Up to $65
Lenticular $0 After Co-pay Up to $100
Frequency 12 Months
Frames
Frames Up to $150 +
20% off Balance Up to $70
Frequency 24 Months
Contact Lens Co-pay In lieu of any other eyewear benefits
Elective Up to $150 Up to $105
Medically Necessary $0 After Co-pay Up to $210
Frequency 12 Months
12
WageWorks | www.takecarewageworks.com | 1 (800) 950 -0105
Gulfstream Goodwill offers a Flexible Spending Account (FSA) administered through WageWorks.
If you have predictable health care expenses for yourself or your family, such as deductibles and co-pays, the FSA may be right for you. A Health Care FSA allows you to set aside money for reimbursement of health care expenses you regularly pay. The amount you set aside is not taxed and is automatically deducted from your paycheck and deposited into the FSA. During the year, you have access to this account for reimbursement of some expenses that are not covered by insurance. An FSA not only results in a substantial tax savings, it also increases your spending power.
A sample list of qualified expenses eligible for reimbursement include, but are not limited to, the following:
Ambulance service
Chiropractic care
Dental fees/Orthodontic fees
Diagnostic tests/Health screenings
Doctor fees
Drug addiction/Alcoholism treatment
Experimental medical treatment
Eyeglasses/Contact lenses (corrective)
Hearing aids and exams
Injections & vaccinations
Lasik surgery
Mental healthcare
Nursing services
Optometrist fees
Physician office visits
Prescription drugs
Medically necessary sunscreen
Wheelchairs
Filing a Claim To file a claim, you must submit your completed claim form and include a copy of the receipt as proof of the expense. Once completed, you may submit your claim either by mail or fax. The IRS requires FSA partici-pants to maintain complete documentation, including keeping copies of receipts for reimbursed expenses, for a minimum of one year.
Debit Card FSA participants can request a debit card for payment of eligible expenses. Participants are able to pay for most qualified services and products at the point of sale versus paying out of pocket and requesting reimbursement. The debit card is accepted at a number of medical providers and facilities and most pharmacy retail outlets. WageWorks may request supporting documentation for expenses paid with your debit card. Failure to provide supporting documentation, when requested, may result in suspension of your card and account until funds are substantiated or refunded back to Gulfstream Goodwill.
FSA Guidelines Your plan year ends December 31, 2018. Note: You have a
grace period at the end of your plan year that allows you to claim reimbursement for eligible expenses incurred through March 15, 2019. Additionally you will have until March 31, 2019 to file claims for expenses incurred through the grace period (March 15, 2019).
Any unused funds after a plan year ends and all claims have been filed cannot be returned to you nor carried forward to the next plan year.
You can enroll in the Health Care FSA during the open enrollment period, qualifying event or new hire eligibility only.
You cannot deduct reimbursed expenses for income tax purposes.
You cannot be reimbursed for a service which you have not received.
You cannot receive insurance benefits or any other compensation for expenses which are reimbursed through your FSA.
Domestic partners are not eligible as federal law does not recognize them as a qualified dependent.
Health Care Reimbursement Account
This account allows you to set aside up to an annual maximum of $2,650. This money will not be taxable income to you and can be used to offset the cost of a wide variety of eligible health care expenses that generate out-of-pocket costs for you or your qualified dependents. Employees can also receive reimbursement for expenses related to dental and vision care (that are not classified as cosmetic).
Examples of common expenses that qualify for reimbursement are listed below.
*NOTE: The entire Health Care FSA election is available to you on the first day coverage is effective.
Please Note: Be conservative when estimating your health care expenses. IRS regulations state that any unused funds which remain in your FSA after a plan year ends and all claims have been filed cannot be returned to you nor carried forward to the next plan year. This is known as the “USE IT OR LOSE IT” rule.
13
Find your personalized health and benefits information in one place – MyHumana As a Humana member, you have a secure website on Humana.com called MyHumana. With MyHumana, you have fast, easy access to your personalized benefits information, planning tools and wellness resources. Some of what you can do on MyHumana: Claims – Check if a claim has been paid along with your
estimated cost, if any
ID cards – View, print and email up-to-date medical and dental Humana member ID cards
Coverage details – Review deductibles, coverage levels and limits
Provider search – Use “Find a doctor” to find in-network providers near you
Humana’s cost comparison tool - compare providers and services, choose wisely and estimate costs
Drug pricing – Look up coverage, estimated prices and possible alternatives
Rx calculator – Plan for out-of-pocket drug costs
Health and condition centers – Access health information specific to your conditions and life stage
Year-to-date summary – See an at-a-glance view of your financial information – including balances in your health savings account, flexible spending account or personal care account and amounts applied to deductibles
Manage access – Give other adults on your policy permission to access your health information
Update your communications preferences – Select which communications you want to receive from Humana and how you want to receive them – via paper or email
Registering is easy
Have your Humana member ID or Social Security number available
Go to Humana.com
Select “Register” at the top of the page
Choose “Member all other plan types”
Fill in some basic information - like your Humana member ID number or Social Security number, date of birth, ZIP code, and email and click “next”
Create a username, password and security prompt and click “next” to finish
Now, how easy was that? You’re all set – jump in and start exploring!
You don’t have to wait for health and benefits guidance – you can get it right away with MyHumana. Please note, all features may not be available to all members.
MEMBER SERVICES WEBSITE REGISTRATION

14
With Doctor On Demand, you can:
Video visit with a physician from one of Doctor On Demand’s U.S. board-certified doctors
Immediately video visit with a doctor 24 hours a day, 7 days a week from any location
Your primary care physician can access your telemedicine visit at your request
If medically necessary, a Doctor On Demand can send a prescription to a preferred pharmacy
Visit the Doctorondemand.com/humana
What can be treated by telemedicine Telemedicine should be considered when your primary care doctor is unavailable, after-hours or on holidays for non-emergency needs. Doctor On Demand physicians can treat ailments, such as:
Colds, sore throat, and flu symptoms
Upper respiratory infections
Allergies and sinus infections
Ear and eye problems
Skin conditions
This service is not for emergency situations such as chest pain, abdominal pain or shortness of breath.
Video visit with a
doctor for PCP copay
TELEMEDICINE
15
READY. SET. Go365.
It’s simple to get started with Go365TM. Here’s
how to get rewarded for your healthy behaviors.
1. Register now. Download the Go365 App or visit Go365.com to access your secure, password- protected Go365 account and program. Already had a HumanaVitality username and password? Just use those credentials to login (no need to re-register). If you never participated in HumanaVitality however, then you'll want to register for Go365.
2. Take the next step. Three easy ways to start earning Points and get to Bronze Status: complete at least one section of your Health Assessment (or more for more points!). Access the Health Assessment on Go365.com by going to activities, or via the app by going to the menu and selecting Health Assessment.
3. Enjoy the rewards. Keep earning Points by completing healthy activities. The more Points you earn, the more Bucks you will have to spend in the Go365 Mall. Reward yourself with brands including:
Complete at least one section of your Health Assessment (or more for more
points!). Access the Health Assessment on Go365.com by going to activities, or via the app by going to the menu and selecting Health Assessment.
Get your biometric screening
Log a verified workout
Get Tracking! Earn points for walking! iPhone users: Apple Health
Samsung Galaxy users: S Health 1,000 steps = 1 point & buck
Sync to the Go365 app by going to
menu (or "More" on iPhones)> Ac-count & settings >App and device connections
WELLNESS PROGRAM
16
WELLNESS PROGRAM
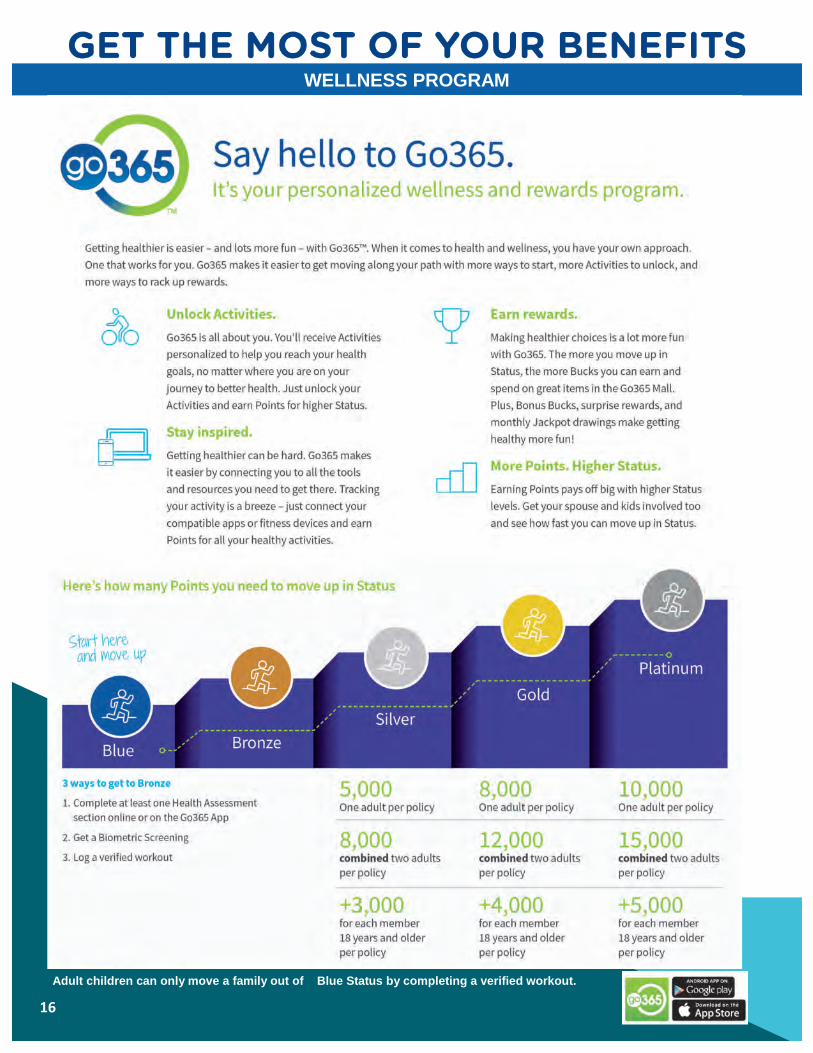
Adult children can only move a family out of Blue Status by completing a verified workout.

17
WELLNESS PROGRAM
18
L i n c o l n | w w w . l i n c o l n 4 b e n e f i t s . c o m | 1 ( 8 0 0 ) 4 2 3 - 2 7 6 5
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
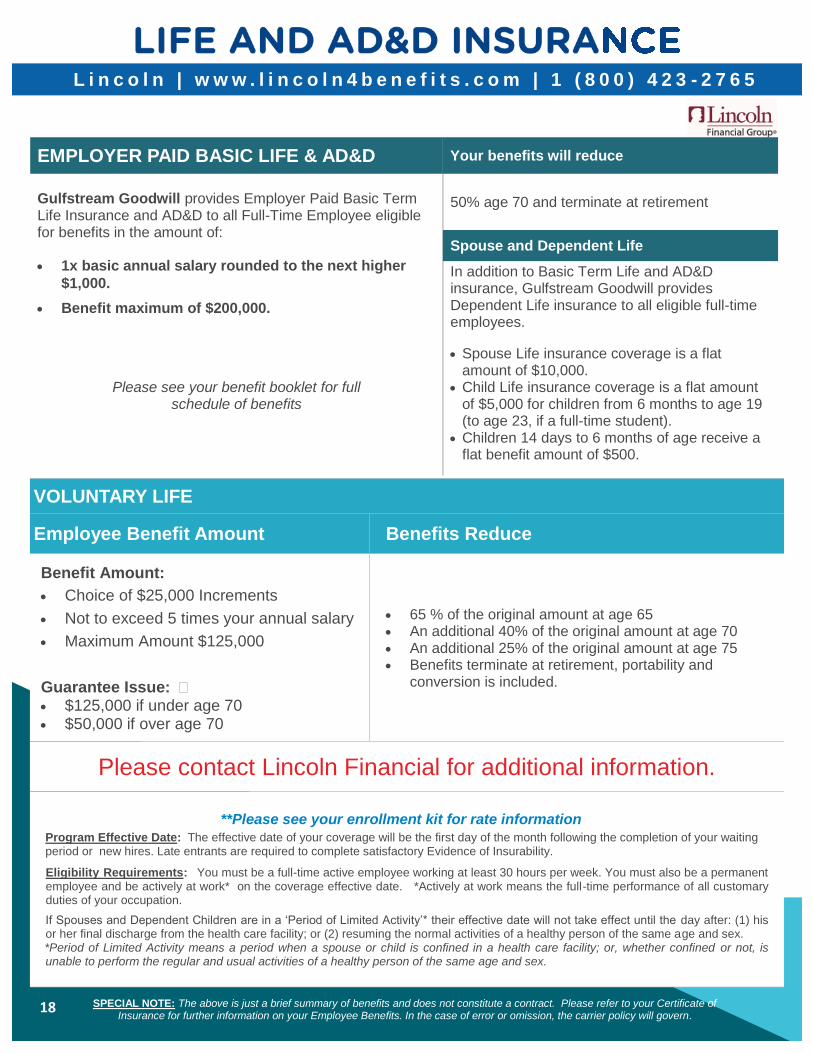
EMPLOYER PAID BASIC LIFE & AD&D Your benefits will reduce
Gulfstream Goodwill provides Employer Paid Basic Term Life Insurance and AD&D to all Full-Time Employee eligible for benefits in the amount of: 1x basic annual salary rounded to the next higher
$1,000.
Benefit maximum of $200,000.
50% age 70 and terminate at retirement
Spouse and Dependent Life
In addition to Basic Term Life and AD&D insurance, Gulfstream Goodwill provides Dependent Life insurance to all eligible full-time employees.
Please see your benefit booklet for full schedule of benefits
Spouse Life insurance coverage is a flat amount of $10,000.
Child Life insurance coverage is a flat amount of $5,000 for children from 6 months to age 19 (to age 23, if a full-time student).
Children 14 days to 6 months of age receive a flat benefit amount of $500.
VOLUNTARY LIFE
Employee Benefit Amount Benefits Reduce
Benefit Amount:
Choice of $25,000 Increments
Not to exceed 5 times your annual salary
Maximum Amount $125,000
Guarantee Issue: � $125,000 if under age 70 $50,000 if over age 70
65 % of the original amount at age 65 An additional 40% of the original amount at age 70 An additional 25% of the original amount at age 75 Benefits terminate at retirement, portability and
conversion is included.
Please contact Lincoln Financial for additional information.
**Please see your enrollment kit for rate information
Program Effective Date: The effective date of your coverage will be the first day of the month following the completion of your waiting period or new hires. Late entrants are required to complete satisfactory Evidence of Insurability.
Eligibility Requirements: You must be a full-time active employee working at least 30 hours per week. You must also be a permanent employee and be actively at work* on the coverage effective date. *Actively at work means the full-time performance of all customary duties of your occupation.
If Spouses and Dependent Children are in a ‘Period of Limited Activity’* their effective date will not take effect until the day after: (1) his or her final discharge from the health care facility; or (2) resuming the normal activities of a healthy person of the same age and sex. *Period of Limited Activity means a period when a spouse or child is confined in a health care facility; or, whether confined or not, is unable to perform the regular and usual activities of a healthy person of the same age and sex.
19
L i n c o l n | w w w . l i n c o l n 4 b e n e f i t s . c o m | 1 ( 8 0 0 ) 4 2 3 - 2 7 6 5
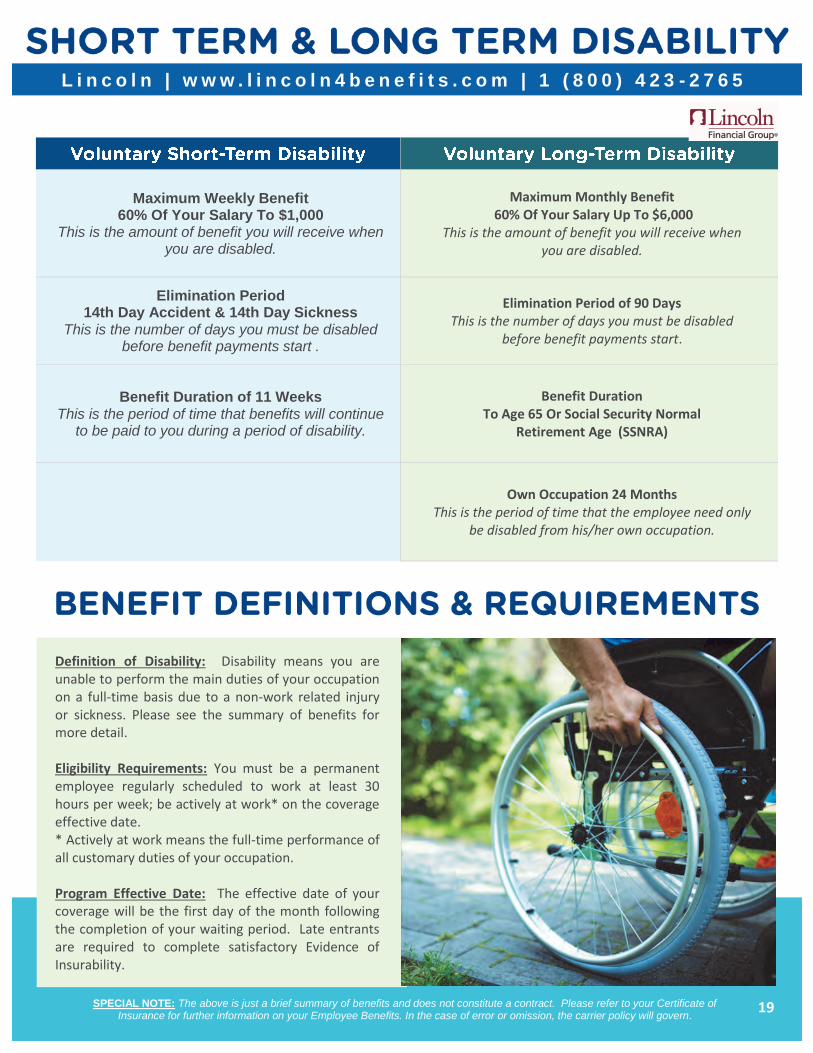
Maximum Weekly Benefit 60% Of Your Salary To $1,000
This is the amount of benefit you will receive when you are disabled.
Maximum Monthly Benefit 60% Of Your Salary Up To $6,000
This is the amount of benefit you will receive when you are disabled.
Elimination Period 14th Day Accident & 14th Day Sickness
This is the number of days you must be disabled before benefit payments start .
Elimination Period of 90 Days This is the number of days you must be disabled
before benefit payments start.
Benefit Duration of 11 Weeks This is the period of time that benefits will continue
to be paid to you during a period of disability.
Benefit Duration To Age 65 Or Social Security Normal
Retirement Age (SSNRA)
Own Occupation 24 Months This is the period of time that the employee need only
be disabled from his/her own occupation.
Definition of Disability: Disability means you are unable to perform the main duties of your occupation on a full-time basis due to a non-work related injury or sickness. Please see the summary of benefits for more detail. Eligibility Requirements: You must be a permanent employee regularly scheduled to work at least 30 hours per week; be actively at work* on the coverage effective date. * Actively at work means the full-time performance of all customary duties of your occupation. Program Effective Date: The effective date of your coverage will be the first day of the month following the completion of your waiting period. Late entrants are required to complete satisfactory Evidence of Insurability.
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
20
Aetna Resources for Living | www.mylifevalues.com | 1 (800) 272-7252
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
Username: ggwill Password: ggwill
Provided by Gulfstream Goodwill at no cost to you, a comprehensive Employee Assistance Program (EAP) is available to you and each member of your family through Aetna Resources for Living. Aetna Resources for Living offers access to mental health professionals through a confidential program that is protected by state and federal laws. The EAP program is available to help you gain a better understanding of problems that affect you, locate the best professional help for your particular problem, and decide upon a plan of action. Counselors are available 24 hours a day, 7 days a week.
What is an Employee Assistance Program? An Employee Assistance Program (EAP) offers covered employees and their family members free and convenient access to a range of confidential and professional services to help them address a variety of problems that can negatively affect their well-being such as:
Anxiety Legal and financial concerns Depression
Life improvements Family and/or marriage prob-
lems Stress
Grief and bereavement Substance abuse Eldercare issues
Lincoln EmployeeConnect | www.guidanceresources.com | 1 (888) 628-4824
EmployeeConnectSM - Practical Help For Life's Challenges 1 (888) 628-4824
There are times in all of our lives when we need a little help. No matter what the issue is, Employee Connect is available 24 hours a day, seven days a week with support, guidance and resources.
Employee Connect Includes:
Assistance for you or an immediate household family member
24/7 telephone and Web access
Telephone access to legal counsel
A 25 % discount for services resulting from an attorney referral
Confidentiality
Username: LFGsupport Password: LFGsupport1
Work/life services for assistance with Parenting and Childcare Eldercare Relationships Work and career Financial
21
AFLAC | www.aflac.com | 1 (800) 992-3522
SPECIAL NOTE: The above is just a brief summary of benefits and does not constitute a contract. Please refer to your Certificate of Insurance for further information on your Employee Benefits. In the case of error or omission, the carrier policy will govern.
Aflac offers a variety of voluntary supplemental insurance plans that may be purchased separately on a voluntary basis and premiums paid by payroll deduction. Aflac pays money directly to you, regardless of what other insurance plans you may have. Available Aflac plans include:
MUTUAL OF AMERICA | w w w.mutua lofamer ica .com | 1 (800) 468 - 3785
Gulfstream Goodwill’s employees are eligible to enroll at any time of the year, in a voluntary tax-deferred 403(b) Thrift Plan. This plan allows you to save money for retirement through convenient payroll deductions. To learn more about the 403(b) Thrift Plan and/or to schedule a personal appointment, contact Gulfstream Goodwill’s local Agent, at (561) 471-1445. You may also contact Mutual of America at (800) 468-3785 or online at www.mutualofamerica.com.
HOSPITAL ADVANTAGE PLAN
ACCIDENT INDEMNITY PLAN
CANCER INDEMNITY PLAN
To learn more about these Aflac plans and/or to schedule a personal appointment, contact Gulfstream Goodwill ’s Aflac Agent, Shirley Sastre Souto
Agent: Shirley Satre Souto Phone: (305) 801-9093
Email: [email protected]

22
About Your Prescription Drug Coverage and Medicare
Attention All Medicare Eligible Employees and Dependents of
Gulfstream Goodwill’s Humana plans:
The following information will apply to you only if you or one of your covered family members is currently eligible for Medicare or soon to be eligible for Medicare. In an effort to ensure that all those who are both eligible for Medicare and covered by our plan receive this important information regarding Medicare Part D, we are sending it to all plan mem-bers.
Beginning January 1, 2006, Medicare offered prescription drug plans to help you pay for the prescriptions you need. This program is called Medicare Part D. If you don’t join a Medicare Part D plan, you will pay a higher premium unless you already have drug coverage that, on average, is at least as good as the standard Medicare Part D plan.
Part of the new law required that employers provide Medicare eligible retirees and active employees and dependents with written certification of whether or not the company's prescription drug coverage is "as good as" the standard Medicare Part D plan. When an employer's plan meets this standard, it is called "creditable".
Please be advised that Gulfstream Goodwill Humana plans that cover you and your eligible dependents are CREDITABLE. Creditable coverage means that the employer plan offered has a value equal to or greater than the Medicare Part D plans.
M E D I C A R E P A R T D
On Medicare Part D, you can read the "Medicare & You" Handbook which will be mailed to you during
October
visit www.medicare.gov on the web
or call 1-800 MEDICARE (1-800-633-4227) TTY users should call 1-877-846-2048
This notice officially confirms:
The fact that your prescription drug coverage is creditable does not prevent you from enrolling in Medicare Part D if you wish. The open enrollment for Part D is November 15 to December 31. However, delaying enrollment in Medicare Part D until a future date will not result in higher premium payments as long as you are covered by a creditable prescription drug plan.
As someone who is Medicare eligible, you will be receiving information on the Medicare Part D plans in your area. Premiums will vary depending upon where you live, but are expected to average about $32-$37/Month. If you do decide to enroll, coordination of benefits will be required.
If you are Medicare eligible please review the enclosed notice and put it with your other important insurance papers. If you have any questions, please feel free to contact your Human Resources Department.
23
HIPAA SPECIAL ENROLLMENT NOTICE
This notice is being provided to ensure that you understand your right to apply for group health insurance coverage. You should read this notice even if you plan to waive coverage at this time.
Loss of Other Coverage If you are declining coverage for yourself or your dependents (including your spouse) because of other health insurance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage (or if the employer stops contributing toward your or your dependents’ other coverage). However, you must request enrollment within 30 days after your or your dependents’ other coverage ends (or after the employer stops contributing toward the other coverage).
Marriage, Birth or Adoption If you have a new dependent as a result of a marriage, birth, adoption or placement for adoption, you may be able to enroll yourself and your dependents. However, you must request enrollment within 30 days after the marriage, birth or placement for adoption.
Medicaid or CHIP If you or your dependents lose eligibility for coverage under Medicaid or the Children’s Health Insurance Program (CHIP) or become eligible for a premium assistance subsidy under Medicaid or CHIP, you may be able to enroll yourself and your dependents. You must request enrollment within 60 days of the loss of Medicaid or CHIP coverage or the determination of eligibility for a premium assistance subsidy. For More Information or Assistance To request special enrollment or obtain more information, please contact your local Human Resources Department.
PREMIUM ASSISTANCE UNDER MEDICAID AND THE CHILDREN’S HEALTH INSURANCE PROGRAM (CHIP)
If you or your children are eligible for Medicaid or CHIP and you are eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage. These states use funds from their Medicaid or CHIP programs to help people who are eligible for these programs, but also have access to health insurance through their employer. If you or your children are not eligible for Medicaid or CHIP, you will not be eligible for these premium assistance programs.
If you or your dependents are already enrolled in Medicaid or CHIP, you can contact your state Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, you can contact your state Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, you can ask the state if it has a program that might help you pay the premiums for an employer-sponsored plan.
Once it is determined that you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must permit you to enroll in your employer plan if you are not already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance.
If you have questions about enrolling in your employer plan, you can contact the Department of Labor electronically at
www.askebsa.dol.gov or by calling toll-free 1-866-444-EBSA (3272).
SECTION 125 Under certain circumstances, you may be allowed to make changes to your benefits elections during the plan year, such as additions, deletions and cancellations, depending on whether or not you experience an eligible qualifying event as determined by the Internal Revenue Service (IRS) Code, Section 125. You may change a benefit election upon the occurrence of a valid qualifying event only if the event affects your own, your spouse’s or your dependent’s coverage eligibility.
If you experience a qualifying event, you must report the qualifying event to Human Resources Department within 30 days of the event. Beyond 30 days, additions and deletions will be denied and you may be responsible both legally and financially for any claims and/or expenses incurred as a result of any dependent(s) who continued to be enrolled who no longer meet the entity’s eligibility requirements.
If approved, most election changes will be effective on the date of the qualifying event for additions; cancellations will be processed at the end of the month.
Payroll deductions for health, dental, vision and certain supplemental accident insurance premiums, are deducted from your gross income before your income is taxed. The entity's plan is known as a Cafeteria Benefit Plan and is governed by IRS Code, Section 125. This pre-tax benefit means you pay less tax on a per-pay and annual basis. See examples of Qualifying Life Events for allowable enrollment changes as determined by Section 125 of the IRS Code.
Examples of a Qualifying Life Event The birth/adoption/legal custody of a child
A marriage
A divorce
A covered dependent is no longer eligible for cover-age
A dependent returns to full-time student status
A spouse or dependent child dies
An increase in your work hours from part-time to full time
A decrease in your work hours
A spouse obtains employment
A spouse’s employment is terminated
A child gains or loses coverage with an ex-spouse (responsibility for health coverage changes)
S E C T I O N 1 2 5 | H I P A A | C H I L D R E N S H E A L T H I N S U R A N C E
24
W O M E N C A N C E R | N E W B O R N S & M O T H E R S | C O B R A
Under the law, the employee or a family member has the responsibility to inform the entity group health plan Administrator of a divorce, legal separation or a child losing dependent status under the entity group health plan within 30 days of the date in which coverage would end under the plan because of the event, whichever is later. The Entity has the responsibility to notify the Plan Administrator of the employee’s death, termination, reduction of hours of employment or Medicare entitlement.
WOMEN’S HEALTH AND CANCER RIGHTS ACT Enrollment Notice
If you have had or are going to have a mastectomy, you may be entitled to certain benefits under the Women’s Health and Cancer Rights Act of 1998 (WHCRA). For individuals receiving mastectomy-related benefits, coverage will be provided in a manner determined in consultation with the attending physician and the patient, for:
All stages of reconstruction of the breast on which the mastectomy was
performed;
Surgery and reconstruction of the other breast to produce a symmetrical
appearance;
Prostheses; and
Treatment of physical complications of the mastectomy, including lymphedema.
These benefits will be provided subject to the same deductibles and coinsurance applicable to other medical and surgical benefits provided under this plan. If you would like more information on WHCRA benefits, please contact your local Human Resource Representative.
Annual Notice
Do you know that your plan, as required by the Women’s Health and Cancer Rights Act of 1998, provides benefits for mastectomy-related services, including all stages of reconstruction and surgery to achieve symmetry between the breasts, prostheses, and complications resulting from a mastectomy, including lymphedema? Please contact your local Human Resource Representative for more information.
NEWBORN’S AND MOTHER’S HEALTH PROTECTION ACT Group health plans and health insurance issuers generally may not, under federal law, restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a cesarean section. However, federal law generally does not prohibit the mother’s or newborn’s attending provider, after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and issuers may not, under federal law, require that a provider obtain authorization from the plan or the insurance issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours).
COBRA
The Consolidated Omnibus Budget Reconciliation Act (COBRA) of 1985 requires that most employers sponsoring group health plans offer employees and their families the opportunity for a temporary extension of health coverage (called ‘continuation coverage’) at group rates in certain instances where coverage under the plan would otherwise end.
An employee, spouse of an employee or a dependent child of an employee covered by the Entity’s group health plan has the righ t to choose this continuation coverage if coverage is lost for any of the following reasons provided below.
HUMANA OA HMO 16 70%
OA HMO 16 90%
PPO 16 70%
PPO 16 90%
Individual $5,000 $2,000 $5,000 $2,000
Family $10,000 $4,000 $10,000 $4,000
Co-Insurance 30% 10% 30% 10%
Employee: Reduction in hours of employment (that disqualifies group insurance participation eligibility); or
Termination of employment (for reasons other than gross misconduct).
Spouse of an Employee:
The death of your spouse; or
A termination of your spouse’s employment (for reasons other than gross misconduct) or a reduction in your spouse’s hours of employment; or
Divorce or legal separation from your spouse; or
Your spouse becomes entitled to Medicare
Dependent Child of an
Employee:
The death of a parent; or
A termination of the parent’s employment (for reasons other than gross misconduct) or a reduction in the parent’s hours of employment with the Entity; or
Parent’s divorce or legal separation; or
A parent becomes entitled to Medicare; or
The dependent child ceases to be a “dependent child” under the Entity’s group health-plan.
25
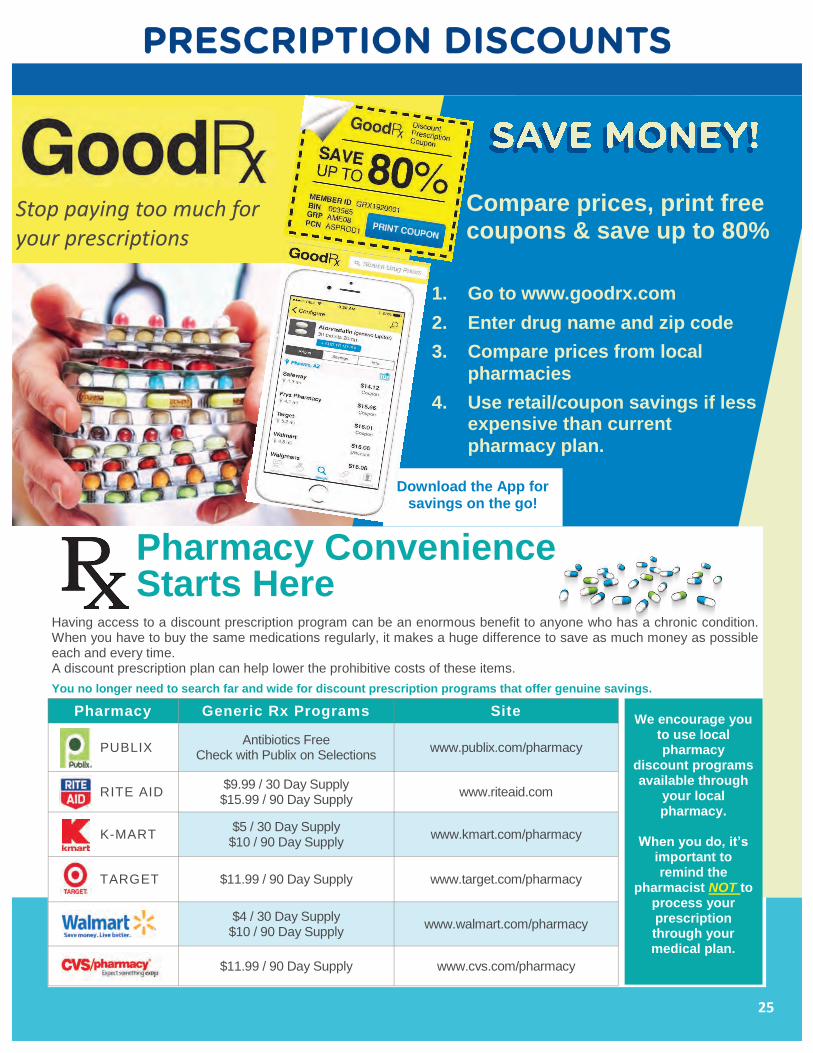
Stop paying too much for your prescriptions
Compare prices, print free coupons & save up to 80%
Pharmacy Convenience Starts Here
Having access to a discount prescription program can be an enormous benefit to anyone who has a chronic condition. When you have to buy the same medications regularly, it makes a huge difference to save as much money as possible each and every time. A discount prescription plan can help lower the prohibitive costs of these items.
You no longer need to search far and wide for discount prescription programs that offer genuine savings.
Pharmacy Generic Rx Programs Site
PUBLIX Antibiotics Free
Check with Publix on Selections www.publix.com/pharmacy
RITE AID $9.99 / 30 Day Supply $15.99 / 90 Day Supply
www.riteaid.com
K-MART $5 / 30 Day Supply $10 / 90 Day Supply
www.kmart.com/pharmacy
TARGET $11.99 / 90 Day Supply www.target.com/pharmacy
WALMART $4 / 30 Day Supply $10 / 90 Day Supply
www.walmart.com/pharmacy
CVS $11.99 / 90 Day Supply www.cvs.com/pharmacy
1. Go to www.goodrx.com
2. Enter drug name and zip code
3. Compare prices from local
pharmacies
4. Use retail/coupon savings if less expensive than current
pharmacy plan.
Download the App for savings on the go!
We encourage you to use local pharmacy
discount programs available through
your local pharmacy.
When you do, it’s
important to remind the
pharmacist NOT to process your prescription through your medical plan.
26
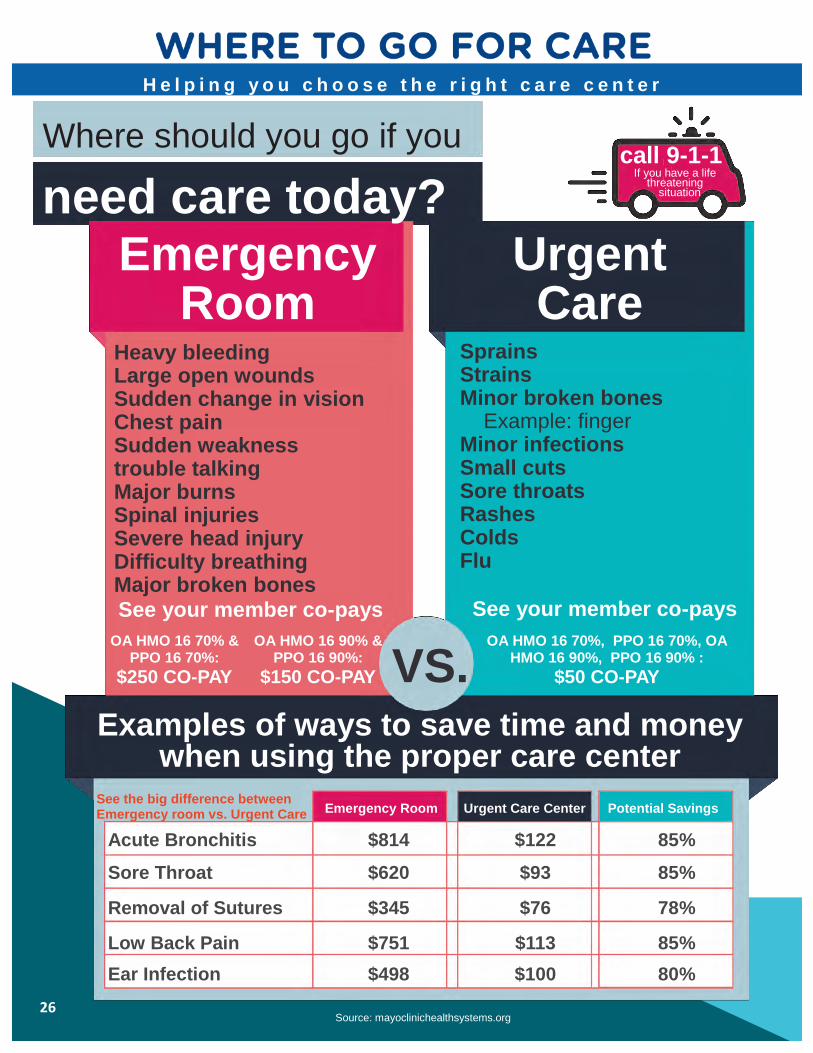
H e l p i n g y o u c h o o s e t h e r i g h t c a r e c e n t e r
Where should you go if you
need care today? Emergency
Room
VS.
Source: mayoclinichealthsystems.org
Examples of ways to save time and money when using the proper care center
Emergency Room Urgent Care Center Potential Savings
Acute Bronchitis $814 $122 85%
Sore Throat $620 $93 85%
Removal of Sutures $345 $76 78%
Low Back Pain $751 $113 85%
Ear Infection $498 $100 80%
See the big difference between Emergency room vs. Urgent Care
Sprains Strains Minor broken bones Example: finger Minor infections Small cuts Sore throats Rashes Colds Flu
See your member co-pays
Heavy bleeding Large open wounds Sudden change in vision Chest pain Sudden weakness trouble talking Major burns Spinal injuries Severe head injury Difficulty breathing Major broken bones
See your member co-pays
call 9-1-1 If you have a life
threatening situation
Urgent Care
OA HMO 16 70% & PPO 16 70%:
$250 CO-PAY
OA HMO 16 90% & PPO 16 90%:
$150 CO-PAY
OA HMO 16 70%, PPO 16 70%, OA HMO 16 90%, PPO 16 90% :
$50 CO-PAY
27
T h e I m p o r t a n c e o f P r e v e n t a t i v e C a r e
PREVENTIVE CARE FOR
CHILDREN Most health plans must also cover a set of preventive health services for children. These services must be provided at no cost to beneficiaries if they are requested from and delivered by an in-network pro-vider.
Autism screening
Behavioral assessments
Blood pressure screening
Cervical dysplasia screening
Depression screening
Developmental screening
Dyslipidemia screening
Fluoride chemoprevention supplements
Gonorrhea preventive medication
Hearing screening
Height, weight and body mass index
Hematocrit or hemoglobin screening
HIV screening
Hypothyroidism screening
Iron supplements
Lead screening
Obesity screening and counseling
Oral health risk assessment
Phenylketonuria (PKU) screening
STI prevention counseling and screening
Tuberculin testing
Vaccinations
Vision screening
Maintaining or improving your health is important – and a focus on regular preventive care, along with following the advice of your doctor, can help you stay healthy.
Routine checkups and screenings can help you avoid serious health problems, allowing you and your doctor to work as a team to manage your overall health, and help you reach your personal health and wellness goals. Preventive care focuses on maintaining your health, and establishing your baseline health status. This may include immunizations, vaccines, physical evaluations, lab work, x-rays and medically appropriate health screenings. During your preventive visit, your doctor will determine what tests or screenings are appropriate for you based on many factors such as your age, gender, overall health status, personal health history and your current symptoms or chronic health concerns.
In addition to mandated no-cost preventive care, there are other existing preventive services that may be included by an insurer as part of a health group plan. These include things like adult vision and hearing screenings and vitamin and mineral supplements. Check with your insurer to see if additional preventive services are available for your plan’s recipients.
PREVENTIVE CARE FOR ADULTS The following types of preventive care are available to all adults within specified age ranges or risk groups.
Abdominal aortic aneurysm screening
Alcohol misuse screening and counseling
Aspirin use
Blood pressure screening
Cholesterol screening
Colorectal cancer screening
Depression screenings
Diabetes screening
Diet counseling
HIV screenings
Obesity screening and counseling
Sexually transmitted infection (STI)
prevention counseling
Syphilis screening
Tobacco use screening
Vaccinations
PREVENTIVE CARE FOR WOMEN The ACA also mandates coverage for the following preventive services for adult women as part of all non-grandfathered health plans.
Anemia screening
Breast cancer genetic test counseling
(BRCA)
Breast cancer mammography screening
Breast cancer chemoprevention
Breastfeeding support and counseling
Cervical cancer screening
Chlamydia infection screening
Contraception
Domestic and interpersonal violence
screening and counseling
Folic acid supplements
Gestational diabetes screening
Gonorrhea screening
Hepatitis B screening
Human papillomavirus (HPV) DNA test
Osteoporosis screening
RH incompatibility screening
Urinary tract or other infection screening
Well-woman visits

28
American Heart Association recommends that all adults age 20 or older have their cholesterol and other traditional risk factors checked every four to six years, and work with their healthcare providers to determine their risk for cardiovascular disease and stroke.
GOAL: Your total cholesterol score is calculated by the following equation: HDL + LDL + 20% of your triglyceride level. A total cholesterol score of less than 180 mg/dL is considered optimal.
GOAL: Less than 120/80 mmHg
GOAL: Less than 100 mg/dL
GOAL: Greater than 18.5 but less than 25 kg/m²
The distance around your natural waist (just above the navel). If your BMI is greater than or equal to 25 kg/m2, your goal for waist circumference is less than 40 inches if you're a man and less than 35 inches if you're a woman.
Numbers that count for a Healthy Heart Source: American Heart Association; heart.org
This chart reflects blood pressure categories defined by the American Heart Association.
K N O W Y O U R N U M B E R S
Blood Pressure Category
Systolic mm Hg (upper #)
Diastolic
mm Hg (lower #)
Normal less than 120 and less than 80
Prehypertension 120 – 139 or 80 – 89
High Blood Pressure (Hypertension) Stage 1
140 – 159 or 90 – 99
High Blood Pressure (Hypertension) Stage 2
160 or higher or 100 or higher
Hypertensive Crisis (Emergency care needed)
Higher than 180 or Higher than 110
29
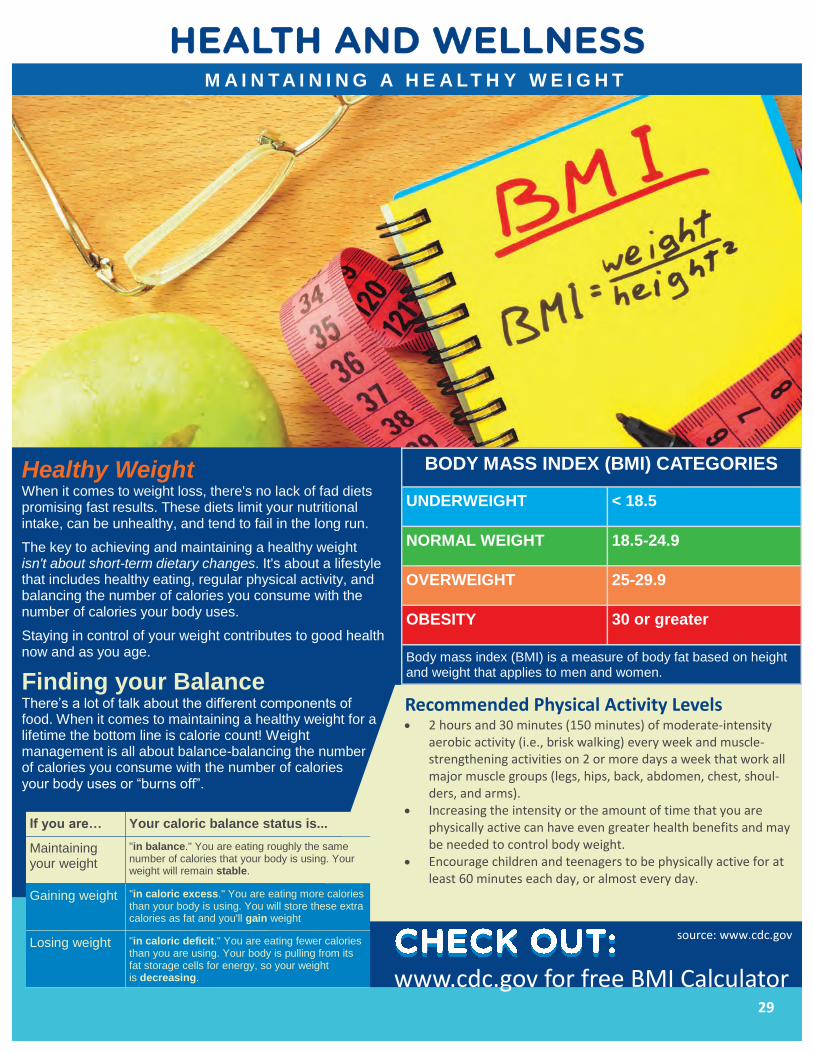
M A I N T A I N I N G A H E A LT H Y W E I G H T
www.cdc.gov for free BMI Calculator
Recommended Physical Activity Levels 2 hours and 30 minutes (150 minutes) of moderate-intensity
aerobic activity (i.e., brisk walking) every week and muscle-strengthening activities on 2 or more days a week that work all major muscle groups (legs, hips, back, abdomen, chest, shoul-ders, and arms).
Increasing the intensity or the amount of time that you are physically active can have even greater health benefits and may be needed to control body weight.
Encourage children and teenagers to be physically active for at least 60 minutes each day, or almost every day.
Healthy Weight When it comes to weight loss, there's no lack of fad diets promising fast results. These diets limit your nutritional intake, can be unhealthy, and tend to fail in the long run.
The key to achieving and maintaining a healthy weight isn't about short-term dietary changes. It's about a lifestyle that includes healthy eating, regular physical activity, and balancing the number of calories you consume with the number of calories your body uses.
Staying in control of your weight contributes to good health now and as you age.
Finding your Balance There’s a lot of talk about the different components of food. When it comes to maintaining a healthy weight for a lifetime the bottom line is calorie count! Weight management is all about balance-balancing the number of calories you consume with the number of calories your body uses or “burns off”.
If you are… Your caloric balance status is...
Maintaining your weight
"in balance." You are eating roughly the same number of calories that your body is using. Your weight will remain stable.
Gaining weight "in caloric excess." You are eating more calories than your body is using. You will store these extra calories as fat and you'll gain weight
Losing weight "in caloric deficit." You are eating fewer calories than you are using. Your body is pulling from its fat storage cells for energy, so your weight is decreasing.
BODY MASS INDEX (BMI) CATEGORIES
UNDERWEIGHT < 18.5
NORMAL WEIGHT 18.5-24.9
OVERWEIGHT 25-29.9
OBESITY 30 or greater
Body mass index (BMI) is a measure of body fat based on height and weight that applies to men and women.
source: www.cdc.gov
30
H O W C A N I M A N A G E S T R E S S ?
It’s important to learn how to recognize how stress
affects you, learn how to deal with it, and develop
healthy habits to ease your stress. What is stressful to
one person may not be to another. Stress can come
from happy events (a new marriage, job promotion,
new home) as well as unhappy events (illness, over-
work, family problems).
Taking steps to manage stress will help you feel more in control of your life. Here are some good ways to cope.
Try positive self talk – turning negative thoughts into positives ones. For example, rather than thinking “I can’t do this,” say “I’ll do the best I can.”
Take 15 to 20 minutes a day to sit quietly, relax, breathe deeply and think of a peaceful situation.
Engage in physical activity regularly. Do what you enjoy- walk, swim, ride a bike or do yoga. Letting go of the tension in your body will help you feel a lot better.
Try to do at least one thing every day that you enjoy, even if you only do it for 15 minutes.
Stress is your body’s response to change. The body reacts to it by releasing adrenaline ( a hormone) that causes your breathing and heart rate to speed up, and your blood pressure to rise. These reactions help you deal with the situation.
The problems come when stress is constant (chronic) and your body remains in high gear, off and on, for days or weeks at a time. Chronic Stress may cause an increase in heart rate and blood pressure.
Not all stress is bad. Speaking to a group or watching
a close football game can be stressful, but they can
be fun, too. The key is to manage stress properly.
Unhealthy responses to stress may lead to health
problems in some people.
Here are some positive healthy habits you may want to develop to manage stress and life a more relaxed life.
Think ahead about what may upset you. Some things you can avoid. For example, spend less time with people who bother you or avoid driving in rush-hour traffic.
Learn to say “no.” Don’t promise too much.
Give up the bad Habits. Too much alcohol, cigarettes or caffeine can increase stress. If you smoke, make the decision to quit now.
Slow down. Try to “pace” not “race.” Plan ahead and allow enough time to get the most important things done.
Get enough sleep. Try to get 6 to 8 hours of sleep each night.
Get organized. Use “To Do” lists to help you focus on your most important tasks. Approach big tasks one step at a time.
31
S E L F / S P O U S E / D E P E N D E N T S
CHILD
SSN ______________________Date of Birth ______________
First Name ________________________MI ______________
Last Name _____________________Gender ______________
CHILD
SSN ______________________Date of Birth ______________
First Name ________________________MI ______________
Last Name _____________________Gender ______________
PRIMARY BENEFICIARY
SSN ______________________Date of Birth ______________
First Name ________________________MI ______________
Last Name _____________________Gender ______________
CHILD
SSN ______________________Date of Birth ______________
First Name ________________________MI ______________
Last Name _____________________Gender ______________
CHILD
SSN ______________________Date of Birth ______________
First Name ________________________MI ______________
Last Name _____________________Gender ______________
CONTINGENT BENEFICIARY
SSN ______________________Date of Birth ______________
First Name ________________________MI ______________
Last Name _____________________Gender ______________
EMPLOYEE (INSURED)
SSN ______________________ Date of Birth ______________
First Name ________________________ MI ______________
Last Name _____________________ Gender ______________
Street Address ______________________________________
City __________________________ ST _____ ZIP __________
Date of Hire _________________________________________
Email Address ________________________________________
Home Phone _________________________________________
SPOUSE
SSN ______________________Date of Birth ______________
First Name ________________________MI ______________
Last Name _____________________Gender ______________
IMPORTANT NOTICE: Please secure the information on this page so
that you do not become a victim of identity theft!

1100 NE 163 Street | North Miami Beach, Florida 33162 Telephone: (877) 948-8887 Fax: (305) 949-1099
www.sapoznik.com




![Welcome [cfly.trustedpartner.com]cfly.trustedpartner.com/docs/library/BethesdaHealthcare2016/ERC... · Welcome Welcome to Bethesda Health, Inc. We are pleased to be an integral part](https://img.pdfslide.net/doc/110x75/5b4f4df87f8b9a206e8c1442/welcome-cfly-cfly-welcome-welcome-to-bethesda-health-inc-we-are-pleased.jpg)
























