Embed Size (px)
Citation preview
Empowering patients: how to implement a diabetespassport in hospital care$
Rob Dijkstra*, Joze Braspenning, Richard GrolCentre for Quality of Care Research-229, University Medical Centre St. Radboud, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands
Received 6 April 2001; received in revised form 10 July 2001; accepted 24 September 2001
Abstract
The purpose was to ascertain the views of patients with diabetes and patient care teams on the introduction of a recently developed
diabetes passport in order to plan effective implementation. A semi-qualitative study by eight semi-structured focus group discussions with
patient care teams and patients in four Dutch hospitals was organised. In total 29 patients participated (range five to nine per hospital).
Patient care teams ranged from four to six participants. Each team included at least one specialised diabetic nurse and an internist. Taped
views were transcribed and coded on the basis of a structured checklist. Various potential barriers to the implementation of the diabetes
passport were found. Although patients recognized the diabetes passport as a handy tool, most of them expected starting problems and little
co-operation from the internists; in this respect they rely more on the diabetes specialist nurse (DSN). Internists had mixed feelings about
the diabetes passport. Lack of motivation and lack of time were important perceived barriers. The specialised diabetes nurses had the
highest expectations of the diabetes passport and perceived themselves as those who would effectuate implementation. The main potential
barriers to effective implementation of the diabetes passport were found in setting the agenda of the passport and fitting it into the
organization of diabetes care. These barriers need to be considered when implementing the passport. The DSN could play an important part
in its implementation. # 2002 Elsevier Science Ireland Ltd. All rights reserved.
Keywords: Empowerment; Diabetes; Patient involvement; Barriers
1. Introduction
Involving patients as partners in their care is increasingly
recognized as a prerequisite for its effectiveness and effi-
ciency [1,2]. Provider based care with patients as consumers
should give way to a situation where patients become the co-
producers of their own health care [1,3,4]. In this perspective
the provider’s role would become more facilitating than
directing [5,6]. Empowerment and a collaborative patient
provider relationship are essential in a chronic disease such
as diabetes, where patients are responsible for the main
aspects of their daily diabetes management [4,7]. Improved
glycaemic control [8], greater patient satisfaction, better
quality of life, improved communication with health provi-
ders [9] and fewer limitations imposed by the disease may
thereby result [10].
In a situation where ineffective and provider centered
communication is still seen as a barrier to effective diabetes
treatment [11] the diabetes passport might fill a gap, because
it enables patients to evaluate the process and outcome
measures of their personal care in relation to recently
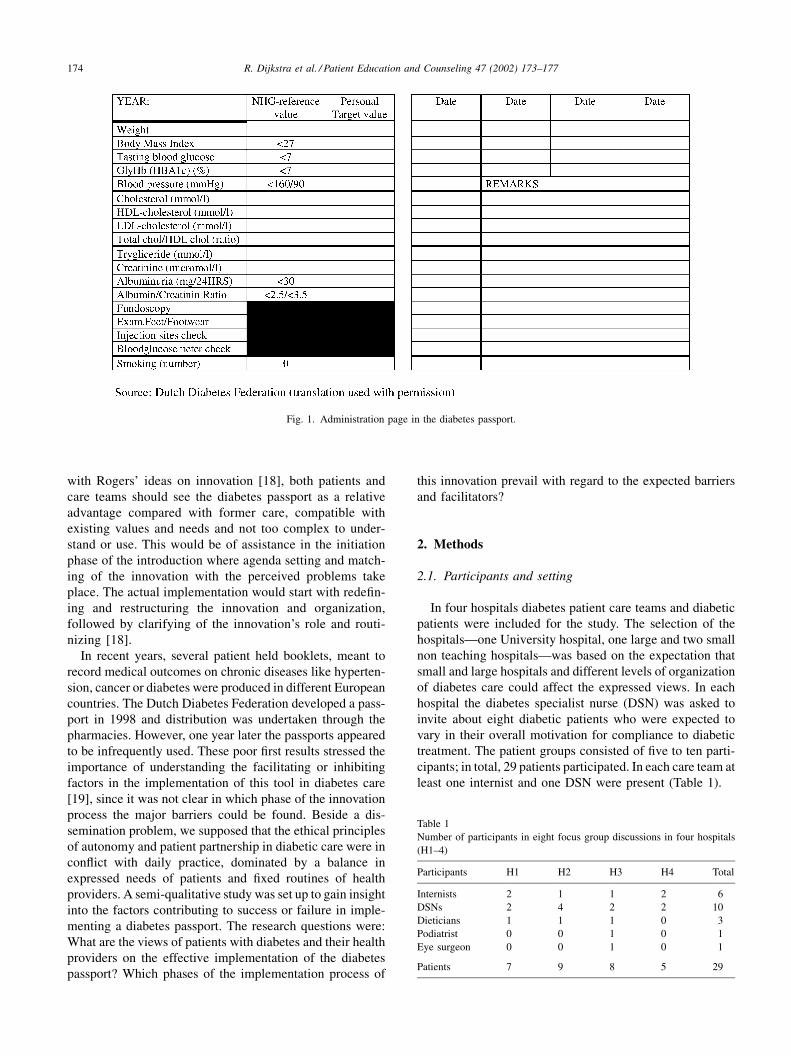
developed evidence based guidelines. Other than patient
held glucose diaries that are used by patients to document
glucose levels obtained from self monitoring, the diabetes
passports are designed to describe, record, and evaluate
medical screening results, see Fig. 1. The passport is an
indirect product of the 1989 St. Vincent declaration in which
the active partnership of medical services and patients was
put forward as a way of achieving diabetes treatment goals
[12]. More than sharing of information or decision making
[13]; the passport enables patients to follow closely the
monitoring of their disease over time and facilitates ‘‘shared
disease management’’. Although the introduction of patient
held booklets, mostly in preventive or chronic care, demon-
strated an increase in several, but not all, services and patient
outcomes [14–17] the question remains to what extent a
diabetes passport is accepted and used and would be effec-
tive in normal practice.
As an innovative attribute in diabetic care, much of the
success of the diabetes passport depends on how it is
perceived by health professionals and patients. In line
Patient Education and Counseling 47 (2002) 173–177
$ This study was made possible by a grant from The Netherlands
Ministry of Health, Welfare and Sport. No conflict of interest.* Corresponding author. Tel.: þ31-24-361640; fax: þ31-24-3540166.
E-mail address: [email protected] (R. Dijkstra).
0738-3991/02/$ – see front matter # 2002 Elsevier Science Ireland Ltd. All rights reserved.
PII: S 0 7 3 8 - 3 9 9 1 ( 0 1 ) 0 0 1 9 6 - 3
with Rogers’ ideas on innovation [18], both patients and
care teams should see the diabetes passport as a relative
advantage compared with former care, compatible with
existing values and needs and not too complex to under-
stand or use. This would be of assistance in the initiation
phase of the introduction where agenda setting and match-
ing of the innovation with the perceived problems take
place. The actual implementation would start with redefin-
ing and restructuring the innovation and organization,
followed by clarifying of the innovation’s role and routi-
nizing [18].
In recent years, several patient held booklets, meant to
record medical outcomes on chronic diseases like hyperten-
sion, cancer or diabetes were produced in different European
countries. The Dutch Diabetes Federation developed a pass-
port in 1998 and distribution was undertaken through the
pharmacies. However, one year later the passports appeared
to be infrequently used. These poor first results stressed the
importance of understanding the facilitating or inhibiting
factors in the implementation of this tool in diabetes care
[19], since it was not clear in which phase of the innovation
process the major barriers could be found. Beside a dis-
semination problem, we supposed that the ethical principles
of autonomy and patient partnership in diabetic care were in
conflict with daily practice, dominated by a balance in
expressed needs of patients and fixed routines of health
providers. A semi-qualitative study was set up to gain insight
into the factors contributing to success or failure in imple-
menting a diabetes passport. The research questions were:
What are the views of patients with diabetes and their health
providers on the effective implementation of the diabetes
passport? Which phases of the implementation process of
this innovation prevail with regard to the expected barriers
and facilitators?
2. Methods
2.1. Participants and setting
In four hospitals diabetes patient care teams and diabetic
patients were included for the study. The selection of the
hospitals—one University hospital, one large and two small
non teaching hospitals—was based on the expectation that
small and large hospitals and different levels of organization
of diabetes care could affect the expressed views. In each
hospital the diabetes specialist nurse (DSN) was asked to
invite about eight diabetic patients who were expected to
vary in their overall motivation for compliance to diabetic
treatment. The patient groups consisted of five to ten parti-
cipants; in total, 29 patients participated. In each care team at
least one internist and one DSN were present (Table 1).
Fig. 1. Administration page in the diabetes passport.
Table 1
Number of participants in eight focus group discussions in four hospitals
(H1–4)
Participants H1 H2 H3 H4 Total
Internists 2 1 1 2 6
DSNs 2 4 2 2 10
Dieticians 1 1 1 0 3
Podiatrist 0 0 1 0 1
Eye surgeon 0 0 1 0 1
Patients 7 9 8 5 29
174 R. Dijkstra et al. / Patient Education and Counseling 47 (2002) 173–177
2.2. Focus group discussion
A focus group discussion was preferred over individual
interviews, because more considered views were expected to
yield after group interaction [20,21], in line with policy
making in a multidisciplinary setting. The interviews were
organized separately for patient care teams and patient groups.
All group interviews were chaired by the same person and
commenced with the distribution of copies of the diabetes
passport and information about its contents and purpose,
especially to the group members who were not familiar with
it yet. A semi-structured discussion was then initiated by
asking: ‘‘What is your opinion of the initiative of the Diabetes
Federation in introducing the diabetes passport?’’ After col-
lectinggeneral remarksabout thepassport, thecontent, current
dissemination and the perceived importance, group members
were specifically asked to give their views on the possibilities
of its introduction in their hospital, to indicate who should be
responsible for the introduction, filling out and maintaining
the passport, and to discuss barriers and facilitators.
2.3. Analysis
The interviews were taped and transcribed. An 11-item
structured checklist based on the different steps in the
process of change was designed to cluster the views
[22,23] (Table 2). Two reviewers independently coded the
views expressed according to the structured checklist. A
value for k was calculated to check the consistency in the
interpretation of the results by two reviewers. It was found to
be 0.73. After learning the prevailing themes from the
interviews the checklist was adapted accordingly. To give
a rough indication of how often a particular remark was
made comments have been added in the Section 3. One is
used in the case of the personal view of one person; some,
several, or more to indicate that at least two persons and up
to half the group shared a view; most, or majority is used
when over half the group members shared a particular view.
3. Results
The results are ordered along the chapters in the checklist:
orientation, outline and content, acceptance and change [22].
Theremarks that most strongly represented the commonviews
expressed on each item were selected to appear as quotes.
3.1. Orientation
Only a few patients had received the diabetes passport
from their pharmacies. Most of them did not find the
intention of the diabetes passport clear. Health providers
were particularly critical of the fact that the diabetes pass-
port had been distributed by the pharmacies without invol-
ving diabetes care teams. They also had their doubts on most
pharmacies’ dissemination activities.
Patient ‘‘It looks like a combined glucose diary and
medication card’’.
DSN ‘‘Some pharmacies are active, some not . . . .
Patients whose drugs are brought to their homes
won’t get it at all’’.
3.2. Outline and content
Several patients saw the passport as a real passport: small,
handy, and easy to take with you when travelling. One DSN
indicated that it took some time to find out where to record
what. Several patients said that it was an advantage that the
passport contained more information than the blood glucose
diaries. One patient considered that giving reference values
was too rigid.
Patient ‘‘The passport is very comprehensive and that is
good’’.
Internist ‘‘The accent should be more on education and
less on recording’’.
Several patients and health personnel said that the pass-
ports would be too difficult for some patients to use. Some
internists added that people who understand it would not
need it, because they already record the main data, while for
those who did not yet register this booklet might be too
difficult.
Patient ‘‘There are words in it that I cannot even
pronounce, let alone understand’’.
DSN ‘‘It would be too difficult for more than half of
the patients’’.
3.3. Acceptance
Several patients said that the passport was very useful as a
source of information to others, especially when travelling
or outside surgery hours. Most patients saw the passport as a
method of getting more insight into their treatment. Others
said that the value would be greater for patients with unstable
Table 2
Structured checklist
Orientation
Being informed of the passport
Current dissemination
Outline and content
Appearance
Text and records
Difficulty
Acceptance
Motivation/use
Empowerment
Change
Person responsible for introduction
Person responsible for filling out
Barriers and facilitators to introduction
Barriers and facilitators to filling out
R. Dijkstra et al. / Patient Education and Counseling 47 (2002) 173–177 175

diabetes. Patients varied considerably in their motivation
towards the use of the diabetes passport. Some were glad to
see a handy tool, but most patients had mixed feelings. An
important negative argument was that the booklet reminded
them constantly of having diabetes. Some were afraid that
diabetes treatment would concentrate on target values rather
than on the quality of life, others were not interested in the
exact results. DSNs and dieticians appreciated the passport
as an aid in communication, since they had no ready access
to patient data. They also felt that most patients would
benefit from it. Internists explained that the passport did
not contribute anything new, although one internist saw the
benefit of having a checklist. Most internists considered the
passport a waste of time in their limited consultation hours,
but one saw it as his task to motivate patients to use the
passport. Only two patients and one DSN indicated that they
expected the passport to help patients ask their doctor
questions about their treatment.
Patient ‘‘I don’t need the figures; when the doctor says
it’s good, that’s enough for me’’.
Patient ‘‘The passport will make it easier for some
patients to ask for their blood pressure’’.
Internist ‘‘The passport is not part of the care we offer. We
already give the HbA1c results and now suddenly
this comes up’’.
DSN ‘‘We all want the patient to take more responsi-
bility; now we have an instrument to go in that
direction, so I think we should start using it’’.
3.4. Change
Although most patients agreed that both health profes-
sionals and patients should be responsible for bringing up
the subject, the DSN was mentioned most frequently as the
most suitable person to introduce the passport. One patient
suggested that for patients with newly diagnosed diabetes
the initiative should be with the health professional, while
patients who were already under treatment should come up
with the proposal themselves.
Patient ‘‘The hospital management should facilitate it in
the starting phase’’.
DSN ‘‘The DSN should fulfil the central role to its
introduction’’.
With regard to filling out the passport after its introduc-
tion, most patients and health professionals emphasized that
the patients themselves should be responsible for that, but
some added that co-operation is necessary because the
internist or DSN have all the data available.
Patient ‘‘It’s your own responsibility . . . but the DSN
should help those who can’t do it’’.
Internist ‘‘A patient said: You have to fill it out and when I
answered: No, you have to fill it out, I will give
you the data, he put it back in his pocket’’.
At the patient level, lack of information and knowledge
about the aims of the passport and its difficulties were
mentioned as important barriers to its introduction. Also,
a perceived negative attitude from health professionals was
expected to hinder introducing the passport to patients.
Some patients said that their own motivation was the main
success factor, but quite a few patients and health profes-
sionals felt that most patients would not be interested.
Patient ‘‘It does not motivate me at all and on top of that I
will definitely lose the passport’’.
DSN ‘‘It depends to a large extent on your own attitude
towards the patient; if that is not positive, they
will stop’’.
Concerning the filling out, some patients did not want to
spend valuable consultation time. At the DSN level, a
positive attitude on the part of DSNs and the fact that they
have more time available for each patient were mentioned as
the main facilitators by patients, internists, and the DSNs
themselves. However, some DSNs indicated that they would
have insufficient personnel if the team were to decide to start
introducing the passport. Also, poor access to patient data
for some DSNs and the fact that the DSN mostly saw only
part of the diabetic patients was expected to inhibit imple-
mentation. At the internist level, most patients and health
personnel said that the internist would not want to spend
precious time on introducing or filling out the passport.
Several internists indicated that it was not only the filling out
that would cost time, but also answering all the questions
from patients that would arise from it. They preferred to
spend their time on direct patient education, or on a physical
examination.
Patient ‘‘Just give me a copy of the laboratory results and
I will fill it out at home’’.
DSN ‘‘There wouldn’t be enough of us if we had to do
it’’.
4. Discussion
With regard to the consecutive stages of an innovation
[18], this study yields a compilation of potential barriers,
most of which refer to the first phases of the introduction.
Most patients seem to welcome the idea of a passport, but it
is surprising how many have low expectations about initiat-
ing the project within their own group. Although not being
familiar with the passport may play a role here, it can be
concluded that patients expect little co-operation from their
internists and rely more on the DSN. Compared to internists,
the DSNs have most positive ideas on its value, however, for
effective implementation they expect that they should have a
more central role within the organization of diabetes care. In
line with other studies the majority of the internists fear loss
of control over consultancy time [24] and content [25,26]
176 R. Dijkstra et al. / Patient Education and Counseling 47 (2002) 173–177

and have low expectations of any increase in patient invol-
vement, compared to the DSNs [27,28].
Although the need for change in diabetes management is
repeatedly expressed and introduction of a diabetes passport
could theoretically be of assistance, this study shows that
focusing on the first stages of implementation at the level of
each hospital probably can prevent disappointing results.
This process might be helped by giving more insight into the
gaps between expected and actual health care delivery and
better knowledge of health care expectations by patients and
providers (agenda setting). Furthermore, clear evidence of
its value in diabetic care would assist in matching the
diabetes passport to the perceived need for change. And
specific attention to the organization of diabetic care, includ-
ing the role of the DSN, would contribute in matching the
diabetes passport to the existing structures.
4.1. Practice implications
Implementation of a diabetes passport will not be effec-
tive if it takes place irrespective of the different kinds of
health care settings, providers and patients. Health care
providers that consider implementing a diabetes passport
should examine the gaps between their actual diabetic care
and the care as perceived by both providers and patients.
Consequently, they should decide whether this is the appro-
priate tool for each specific health care setting.
Acknowledgements
The authors would like to thank the patients and diabetes
patient care teams of UMC-St. Radboud Nijmegen, Bosch
Medicentrum S’Hertogenbosch, Ziekenhuis Zevenaar and
Medisch Centrum Molendael Baarn for their participation in
this study and A.F. Casparie for comments on the manuscript.
References
[1] Holman H, Lorig K. Patients as partners in managing chronic
disease. Br Med J 2000;320:526–7.
[2] Guadagnoli E, Ward P. Patient participation in decision making. Soc
Sci Med 1998;47:329–39.
[3] Anderson RM. Patient empowerment and the traditional medical
model: a case of irreconcilable differences? Diabetes Care 1995;
18:412–5.
[4] Etzwiler DD. Chronic care: a need in search of a system. Diabetes
Educ 1997;23:569–73.
[5] Feste C, Anderson RM. Empowerment from philosophy to practice.
Patient Educ Couns 1995;26:139–44.
[6] Wagner EH, Austin BT, Von Korff M. Improving outcomes in
chronic illness. Manage Care Q 1996;4:12–25.
[7] Glasgow RE, Anderson RM. In diabetes care, moving from com-
pliance to adherence is not enough. Diabetes Care 1999;22:2090–2.
[8] Anderson RM, Funnell MM, Butler PM, Arnold MS, et al. Patient
empowerment. Results of a randomised controlled trial. Diabetes
Care 1995;18:943–9.
[9] Kinmonth AL, Woodcock A, Griffin S, Speigel N, Campbell MJ.
Randomised controlled trial of patient centred care of diabetes in
general practice: impact on current well-being and future risk. Br
Med J 1998;317:1202–8.
[10] Greenfield S, Kaplan S, Ware JE. Expanding patient involvement in
care. Ann Intern Med 1985;102:520–8.
[11] Freeman J, Loewe R. Barriers to communication about diabetes
mellitus. J Fam Pract 2000;49:507–12.
[12] Diabetes care and research in Europe: the Saint Vincent declaration.
Diabetic Med. 7:1990;360.
[13] O’Connor A. Patient education in the year 2000: tailored decision
support, empowerment and mutual aid. Qual Health Care 1999;8:5.
[14] Giglio RJ, Papazian B. Acceptance an use of patient-carried health
records. Med Care 1986;24:1084–92.
[15] Turner RC, Waivers LE, O’Brien K. The effect of patient-carried
reminder cards on the performance of health maintenance measures.
Arch Intern Med 1990;150:645–7.
[16] Dickey LL, Pettiti D. A patient held minirecord to promote adult
preventive care. J Fam Pract 1992;24:457–63.
[17] van Wersch A, de Boer MF, Van der Does E, De Jong P, et al.
Continuity of information in cancer care: evaluation of a logbook. Pat
Educ Couns 1997;31:223–36.
[18] Rogers EM. Diffusion of Innovations, 4th Edition. New York: The
Free Press, 1995.
[19] Grol RTPM. Beliefs and evidence in changing clinical practice. Br
Med J 1997;315:418–21.
[20] Basch CE. Focus group interview: an under-utilized research
technique for improving theory and practice in health education.
Health Educ Q 1987;14:411–48.
[21] Powell RA. Methodology matters, focus groups. Int J Qual Health
Care 1996;8:499–504.
[22] Krueger RA. Analysing and Reporting Focus Group Results. New
York: Sage, 1998.
[23] Grol R. Implementing guidelines in general practice. Qual Health
Care 1992;1:184–91.
[24] Dijkstra RF, Braspenning JCC, Uiters E, van Ballegooie E, Grol
RTPM. Perceived barriers to the implementation of diabetes guide-
lines in hospitals in The Netherlands. Neth J Med 2000;56:80–5.
[25] Greco PJ, Eisenberg JM. Changing physicians’ practices. New Engl J
Med 1993;329:1271–4.
[26] Tunis SR, Hayward RSA, Wilson MC, Rubin HR, et al. Internists’
attitudes about clinical practice guidelines. Ann Intern Med
1994;120:956–63.
[27] Anderson RM, Donnely MB, Dedrick RF. The attitude of nurses,
dieticians and physicians towards diabetes. Diabetes Educ
1991;17:261–8.
[28] Morris DB. Developing a patient education program: overcoming
physician resistance. Diabetes Educ 1998;24:41–7.
R. Dijkstra et al. / Patient Education and Counseling 47 (2002) 173–177 177