Embed Size (px)
Citation preview

International Journal of Medical Informatics (2006) 75, 577—596
Empowering patients with essential informationand communication support in thecontext of diabetes
Chunlan Maa, Jim Warrena,∗, Patrick Phillipsb, Jan Staneka
a Advanced Computing Research Centre, University of South Australia,Mawson Lakes, SA 5095, Australiab Department of Endocrinology, The Queen Elizabeth Hospital,Adelaide, Australia
Received 15 December 2004; received in revised form 1 September 2005; accepted 2 September 2005
KEYWORDSConsumer healthinformation;Internet;Tailoring;Doctor—patientrelationship;Diabetes
SummaryObjectives: Patients with diabetes need to be aware of essential information tobe involved in decision-making, manage diabetes properly, and communicate withdoctors and other healthcare providers effectively. We have developed Violet Tech-nology (VT) to provide features beyond previous health information tailoring systemsby dynamically prioritizing diabetes learning topics and providing integrated directsupport for patient-provider communication through formulation of individualizedagendas to take to healthcare encounters.Methods: A particular feature of the VT approach is a Diabetes Information Profile(DIP) that models psychosocial and educational exposure features, as well as clinicalcharacteristics, and considers expressed patient information preferences and recentinformation browsing history. The agenda facility recommends questions that thepatients may have based on their profile, as well as helping to initialize a patientempowerment protocol. The technology uses a modular and extensible approachfor key components, including consumer health information, prioritization rules,and methods of instantiating the DIP. VT has been implemented into a web portalfor patient use. Two phases of evaluation studies have been conducted to collectpatient and healthcare provider feedback.Results and conclusions: Results indicate that VT prioritizes relevant and importantinformation for individual patients. Moreover, both patients and providers indicatethat formulating an agenda of questions is important for patients. More extensive
system use is needed to establish if the technology can deliver an improved patient-provider partnership and, ultimately, improved health outcomes.© 2005 Elsevier Ireland Ltd. All rights reserved.∗ Corresponding author. Tel.: +61 8 8302 3446; fax: +61 8 8302 3988.E-mail address: [email protected] (J. Warren).
1386-5056/$ — see front matter © 2005 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijmedinf.2005.09.001

cbittacpeltiptiidombtw
mdiiitpsmwgtctodtpo5otf
2
To
578
1. Background
Although comprehensive guidelines for diabetesmanagement have been developed, many patientswith diabetes do not achieve optimal outcomes andstill experience devastating complications due tothe current healthcare system, which is designedfor acute rather than chronic disease [1]. In dia-betes management, more than 95% of diabetes careis done by patients at their home base [2]. Patientsneed to set their own goals and priorities within thecontext of their health issues, living environmentand family demands. Health professionals have lit-tle control on how patients manage their diabetes.The reality is that patients do not normally receivenecessary training or support for effective carefrom the current health care system [2]. A qualita-tive study showed that people with diabetes gener-ally have a poor knowledge of care and that there isinconsistency in the way information is delivered topatients [3]. As a result, there is a gap between theideal doctor—patient partnership and what actuallyoccurs, and this gap forms a source of frustration forboth patients and healthcare professionals [4].
To close this gap, facilitating the collabora-tive relationships between doctors and patients— ‘‘doctor—patient partnership’’ — and fosteringpatient-centered practices are the key [1]. In dia-betes management, doctor—patient partnership inboth diabetes care and doctor—patient commu-nication improves patients’ compliance and out-come [2,5,6]. This partnership can be perceived ashealth professionals bringing expertise about dia-betes and its treatment, and patients bringing theirexpertise about their own life. A shared decision-making model has been developed for achieving thedoctor—patient partnership [7,8]. In this model, theinformation exchange between these two parties isin two ways. The patient is put at the center of thehealthcare process and patients have to take theirown responsibilities in this process.
Consequently, patients need to be empoweredwith essential knowledge and skills in order tobe involved in decision-making, manage diabetesproperly, and communicate with doctors and otherhealthcare providers (such as nurse educators andpharmacists) effectively. Patient empowerment isdefined as helping the patient discover and developthe inherent capacity to be responsible for one’sown life [1]. Tailored and personalized online infor-mation is considered one of the approaches forempowering patients and consumers to enable the
partnership [9].Lewis [10] reports that computer-based edu-cation is an effective strategy for transferringknowledge and skill development for patients with
psta
C. Ma et al.
hronic disease. However, she says that there haseen little research aimed at providing customizednformation that is flexible enough to adapt tohe dynamic nature of patients’ ongoing informa-ion needs and changes in their personal healthnd social circumstances. We believe this defi-iency relates to a number of factors: (1) neglectingatients’ change in knowledge of the specific dis-ase; (2) largely ignoring patients’ psychosocial andifestyle status, i.e., considering only clinical fac-ors; (3) the absence of information prioritizationn current tailoring systems; and (4) disregardingatients’ information preference in the informa-ion tailoring. In addition, provision of personal-zed information only indirectly supports patientsn their formulation of questions. Unvoiced agendauring the health encounter is a common and seri-us problem leading to poor doctor—patient com-unication [11—13]. We believe the patients shoulde directly supported in articulating their questionso formulate as agendas for subsequent encountersith healthcare providers.Our research aims to formulate an infor-
ation technology (IT) framework to supportoctor—patient partnership through: (1) provid-ng essential information to individual patients—–nformation that is not only relevant, but also prior-tized; and (2) providing, in close integration withhe information prioritization, direct support foratients to generate personalized agendas prior tocheduled health visits. We have designed, imple-ented and undertaken preliminary evaluation of aeb portal for diabetes patients. The suite of inte-rated components we have developed to createhis portal is called Violet Technology (VT). The VTomponents are described in the next section. Sec-ion 3 describes the web portal itself in terms ofverall architecture and user interface. Section 4escribes our two phases of evaluation study under-aken to date—–the first aimed at evaluating therioritization of information topics, and the sec-nd a field trial of the integrated portal. Sectiondiscusses our findings, including comparison with
ther technologies reported in the literature. Sec-ion 6 provides summary conclusions and directionsor further research.
. Violet Technology
he innovative technologies that have been devel-ped for implementing our approach to IT for
atient-provider partnership include: a comprehen-ive Diabetes Information Profile (DIP); informationailoring and prioritization algorithms (supportingn Information Service); quiz tailoring and prioriti-
E d co
zafSatoEnm
2
Taappaio[ppmtte
ccisl
Titfltphfitp
2
Titqaoitnaatcvta
mpowering patients with essential information an
ation algorithms (supporting a Quizzing Service);nd agenda personalization algorithms (supportingormulation of patient question sets as an Agendaervice). Collectively, the implementation of thesepproaches, including its embodiment in a web por-al for diabetes patients, is called Violet Technol-gy. VT has an extensible architecture based onxtensible Mark-up Language (XML) and Java tech-ologies. This section describes the design of theajor VT components.
.1. Diabetes Information Profile
he essential role of user modeling is to supportdaptation of the system to the needs of the userccording to the model [14]. Sources of a relevantatient profile for a health application include aatient’s Electronic Medical Record (EMR) [15,16]nd medical history collected through computer-zed medical forms filled out by patients (as in [17]),r from both patients and health providers (as in18,19]). Our approach uses both EMRs and com-uterized forms filled out by patients, the latterroviding additional more patient-centered infor-ation, covering a broader range of issues than
hose usually contained within the EMR. The por-al provides a service for the patient to view anddit this information.
We have developed a comprehensive user profilealled the Diabetes Information Profile. This profile
onsists of five parts (see Table 1). The first parts information about a patient’s diabetes-relatedituations, such as current lifestyle, physical andaboratory examination, medications and so forth.tooi
Table 1 Components of the Diabetes Information Profile (D
Profile component Contents of each compon
Diabetes-related situation • Current lifestyle• Diabetes educational ex• Diabetic complication r• Psychosocial issues• Risk factors of diabetic• Behaviour change due t• Self blood glucose tests• Physical and laboratory• Medications
History of information browsing • IDs of the information i10 seconds and the corres
Patient information preference • IDs of the information isomewhat interesting, in
History of quizzing • Dates, quiz question IDquestions.
History of agenda generation • Dates and the descripti• Dates and the descripti• Dates and agenda list g
mmunication support 579
he second part is the patient’s information brows-ng history, i.e., the IDs of information items thathe patient has opened at least three times on dif-erent sessions, and each viewing time lasting for ateast 10 s. The third part is the information abouthe patient’s information preferences. The fourthart is the information about the patient’s quizzingistory—–his/her answers to quiz questions. Thenal part is the information about the patient’s his-ory of agenda generation. The utilization of eachart of the DIP is detailed in the next section.
.2. Adaptation mechanisms
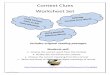
he system’s adaptive mechanisms include thenformation service (provision of tailored informa-ion), the quizzing service (provision of tailoreduiz) and the agenda service (provision of tailoredgenda question pool). The adaptation mechanismsf the information service have two stages: filter-ng and prioritization (see Fig. 1). Filtering retainshe information and quiz questions that the patienteeds to know and that which is nice to know,nd removes information and quiz questions thatre irrelevant in light of the patient’s profile. Afterhe filtering process the contents of the user spe-ific information and quiz questions are all rele-ant to the user’s profile. Prioritization matcheshe patient’s profile to the prioritization rules sos to assign appropriate weights (numeric scores)
o the relevant information and quiz questions. Pri-ritization rule matching uses Boolean comparisonf rule criteria to the DIP. The weights assigned tonformation items or quiz questions are used to sortIP)
ent
posureisk factors
complicationso diabetes
examination
tems that have been viewed each time for at leastponding date.tems with patient’s self rating (not interesting,teresting, very interesting) and the corresponding date.s and results of the patient’s answers to quiz
ons of agenda questions added/created by patients.ons of the agenda questions deleted by patients.enerated by patients.

580 C. Ma et al.
ering
2AnfoefiptscctbttcbiesPPe
Fig. 1 Process of information/quiz questions filt
content in a meaningful order. There is no filteringprocess involved in the mechanisms of the agendaservice. The following sections introduce the adap-tation mechanisms of the three services.
2.3. Mechanisms of the information service
Filtering and prioritization are applied, respec-tively.
2.3.1. Information filtering algorithmWe apply straightforward filtering rules that firsteliminate major topics of information that are irrel-evant (e.g., female issues for men), then performfiner-grained filtering of items and sub-items (e.g.,remove discussion of insulin if it is not used by theparticular patient). The filtering rules have onlytwo outcome values: relevant and irrelevant. Thepatient’s profile is matched against these rules.The mapping results determine the actual contentsof the user specific diabetes information resource,i.e., only true result makes the corresponding infor-mation topics, items or sub-items are copied to theuser specific diabetes information—–an XML docu-ment.
It is important to note that the information fil-tering approach does not mean that the informationmust be inaccessible to a patient interacting witha system based on this method—–the informationstopped by the filtering will not be presented aspriority information, but can still appear, for exam-ple, on a table of contents. This is significant withrespect to user control (to access what they want),will be important to some users who would other-
wise be disoriented by perceived incompleteness ofavailable information, and is essential to support auser who may, for instance, be looking up informa-tion for their spouse.Table 2 Sample content of one SigPRule
Name of the rule Criteria Info
Hyperglycemia Blood glucose test (before meals):>=8 mmol/L & <=10 mmol/L
C00(Hy
and prioritization using Violet Technology (VT).
.3.2. Information prioritizationfter filtering out the irrelevant information, theext step is to prioritize the relevant informationor the patient. The question is how to assign a pri-rity (i.e., weight) to an information item. Beeneyt al. mentioned in [20] that it might not be suf-cient to only rely on the perceptions of a healthrofessional to determine the educational priori-ies for the patient with diabetes. Beeney’s studyhows GPs (General Practitioners, i.e., family physi-ians) significantly overestimate complications as aoncern for patients at diagnosis. A patient’s emo-ional supports and information preference shoulde considered when individualizing his/her educa-ional priority. According to the suggestions fromhe literature [21,22], a patient’s acute physiologi-al needs, self-beliefs and knowledge level on dia-etes should be taken into account in setting prior-ties for information needs. Consequently, we cat-gorize the prioritization rules into three groups:ignificant data oriented prioritization rules (Sig-Rule); patient’s knowledge level oriented (Know-Rule); and patient’s information preference ori-nted (PrefPRule).
SigPRule: Significant data mean the factors thathave the greatest adverse effects on diabetesmanagement outcome (e.g., excess alcohol con-sumption, smoking, high fat diet) or that representan urgent situation needing to be dealt with (e.g.,hypoglycemia or the presence of ketoses in urine).In each rule, there are criteria for significant dataand corresponding information IDs (UMLs ConceptUnique Identifiers [CUIs]) with appropriate prede-fined weight. Table 2 shows one of the SigPRule
contents. The rules are represented in an XML doc-ument format.The recommendations in Diabetes & You—–Theessential guide [23] provide our starting point
rmation IDs (UMLS CUIs) Weight
20456 (Hyperglycemia), C0020615 C0020456poglycemia Hyperglycemia)
0.8

E d co
2
TnLike the information service, this quizzing serviceuses filtering and prioritization. The quiz filtering
mpowering patients with essential information an
for the rules and information items. This book,published by Diabetes Australia, is a profession-ally vetted and endorsed reference for peoplewith diabetes. In terms of how to determinethe value of the weight assigned to the relatedinformation item(s), the severity and likelihoodof consequences, as well as the preventable oractionable nature of the issues, are considered.We have implemented about 25 different typesof significant data-oriented prioritization rules.The rules cover the patient’s blood glucose level,excess alcohol consumption, smoking, high fatand sugar diet, frequency of dining out, trav-eling, checking feet, psychosocial issues due todiabetes, body mass index (BMI), HbA1c (glycosy-lated hemoglobin, which is a measure of blood glu-cose control), lipid profile, blood pressure, podi-atry test, and risk factors of retinopathy, neu-ropathy, vascular disease and nephropathy. Theserules represent our knowledge engineering of thedomain, based on: firstly, the content of thesource reference [23] itself; secondly, a review ofthe related medical literature; thirdly, the under-standing of the clinically-trained authors (Ma,Phillips and Stanek); and fourthly, an extensivereview with other healthcare providers and con-sumers, notably diabetic nurse educators at TheQueen Elizabeth Hospital (TQEH) Diabetes Cen-tre. However, the rule content and in particularthe weights the rules assign, must be viewed as amatter of opinion.KnowPRule: Our information prioritization takesinto account the patient’s estimated diabetesknowledge level in terms of educational expo-sure. This stands in contrast to a proficiency-adapted hypermedia educational system (e.g., forlearning a programming language [24]), wherea student’s knowledge is estimated by evaluat-ing the student’s attainment of key concepts andconcept-related practices. However, patient edu-cation is not a linear learning process. Rather it is asituation-centered learning process. For example,if a patient knows how to reduce fat in one’s diet,it does not necessarily mean that the patient mustknow the amount of food he/she needs a day, orthe symptoms of hyperglycemia. For this reason,we do not directly use quizzing to estimate knowl-edge level.
We categorize both patients and all informationitems into three levels. With respect to patients,Level 1 means the patient knows little or noth-ing about diabetes. Level 2 means the patient
knows basic information and survival informa-tion about diabetes, but does not know enoughabout diabetes self-management. Level 3 meansthe patient knows almost everything about dia-r
i
mmunication support 581
betes self-management and feels quite confidentin their knowledge level. With respect to infor-mation items, Level 1 contains the most basicand necessary information for a newly diagnosedpatient, such as explanation of diabetes, survivalinformation, insulin injection and available essen-tial resources for support (National Diabetes Sup-ply Scheme, Diabetes Centre, etc.). Level 2 con-tains further necessary information to perfect thepatient’s self-management skills, including labelreading, diet management and insulin dose adjust-ment. Level 3 mainly contains information on dia-betic complications, such as retinopathy and neu-ropathy.
The correspondence of the patient’s estimatedknowledge level and the rated level of the infor-mation item provides a basis for prioritizing rele-vant information according to patient knowledgeas well as significant data. We assign patients toknowledge levels, 1, 2 or 3 on the basis of diabeteseducational exposure. Table 3 illustrates the expo-sure details and how weight for information itemsis assigned on the basis of the match of patientlevel and information level.
In addition to considering the knowledge level,we use currency to indicate the patient’s famil-iarity with a piece of information. If a patienthas read an information item several times, thisitem will no longer be relevant to this patient. Ifa patient has opened an information item threetimes in three different log-ins, and each time theitem is opened for more than 10 s, this informationis assigned a weight of −1. For knowledge refresh-ing purposes, this weight is valid for 120 days.PrefPRules: apart from the above factors,patients’ information preferences are also consid-ered during the prioritization. Patients can rateeach piece of information as Not interesting,Somewhat interesting, Interesting, and Very inter-esting, and the corresponding weight is −1, 0, 0.5and 1, respectively.
We simply use the sum of all the four priorities(significant data, knowledge level, currency andpreference), as the final weight to sort the infor-mation items at this time.
.4. Mechanisms of quizzing service
he source of quiz questions, answers and expla-ations is ‘‘Novo Nordisk: Diabetes Web World1’’.
ules are matched against the patient’s DIP. Only if
1 http://www.yourdiabetesworld.com/health/dwk/nfo/ydww/index.asp.

582 C. Ma et al.
Table 3 Educational exposure collection questionnaire—–assessing patient knowledge level and weight assignmentto information items by level
Educational exposure data collectionquestionnaire items
Median score of the educationalexposure questionnaire
Knowledgelevel
Informationlevel
1 2 3
• Do you discuss your diabetes-relatedproblems with your GP? (Scores: 0—3)
Median sore <2 Level 1 0.8 0.5 0.2
• 2 <= median score <3 Level 2 0.2 0.8 0.5OR• Patient has ever been a carerfor a person with diabetesOR
• How many education sessions ondiabetes have you attended? (Scores:0—5)
• Patient is/was a diabetesrelated health professional
• How many times have you seen adiabetes educator? (Scores: 0—5)
Median score >= 3 Level 3 0.5 0.2 0.8
• How many times have you seen adietician to learn about a diabeticmeal plan or diet? (Scores: 0—5)
• Are you a diabetes-related healthprofessional (e.g., GP, nurse,pharmacist) or have you ever been acarer for a person with diabetes?
• How frequently have you soughtdiabetes information from otherresources, such as diabetesinformation booklets, TV, magazine, or
rp(sadmtsrbmdpcTppprp
library, etc.? (Scores: 0—3)
the matching result is true, the corresponding quizquestions are copied to an XML file—–‘‘Tailored quizquestions.’’ However, a number of quiz questionsare not modeled in the quiz filtering rules and aredirectly copied to the ‘‘Tailored quiz questions’’file.
The prioritization mechanisms of the Quizzingservice uses three mapping functions: significantdata mapping; patient’s educational exposure map-ping; and mapping the patient’s response to quizquestions. If a patient answers a question correctly,it may be assumed that the patient knows thequestion-specific knowledge. Therefore, this ques-tion will be given a weight of −1 in order that it willnot appear next time when the same patient takesthe quiz; this weight has a valid period of 120 days(after which the question may regain priority as a‘refresher’ for the patient if still relevant accordingto the profile).
2.5. Mechanisms of agenda service
Four sources form the patient-specific agenda ques-tion pool: (1) the patient’s greatest difficulties indiabetes management; (2) the patient’s diabetes-
imTt
elated issues; (3) the information items that theatient added during information browsing; and4) the questions that the patient created for her-elf/himself. The first source is the initialization ofpatient empowerment protocol. This protocol wasesigned to help patients participate in decision-aking by developing their knowledge, skills, atti-
udes and degree of self-awareness [25]. It has beenhown that both patients and health professionalsesponded positively to an empowerment protocol-ased program [26]. Furthermore, the empower-ent protocol philosophy was able to establishoctor—patient partnership and patient-centredractices, and improve doctor—patient communi-ation and diabetes management outcomes [1].hus, we prompt for information to initiate theatient empowerment protocol as the first com-onent of all agendas. For the second source, if aatient is found to match any of the significant dataules, these issues are put into the agenda questionool. The third source relates to the patient explic-
tly selecting, via the portal interface, that an infor-ation item should be added to his/her agenda.he fourth source consists of questions authored byhe patient in the agenda section of the portal, pre-
E d co
sk
3
Amts
3
TmcgibtpmfisfaX(pit
tiatt
pteawotfbfidr
Tm
d
tphDsmcqspXTtb
3
TctS
3Trsmgstmttdodtit‘aTtvfia
et
mpowering patients with essential information an
umably outside of the question pool offered by ournowledge base.
. The VT Web portal
web-based portal using the VT has been imple-ented. The following sections introduce its archi-
ecture and how the adaptation services are pre-ented to users.
.1. Architecture
he web portal is an adaptive system. The infor-ation presented is changed dynamically with the
hange of each user’s DIP. Extensible Markup Lan-uage is used to model: the consumer diabetesnformation base; the tailored, patient-specific dia-etes information; the quiz questions pool; theailored, patient-specific quiz questions; and theatient-specific agenda pool. In addition, the infor-ation filtering and prioritization rules, the quizltering and prioritization rules are also XML-tructured. Extensible Stylesheet Language Trans-ormations (XSLT) and XML Path Language (XPath)re used to copy, refer to, and present part of theML documents. JAXP and SAX in JAVA technologyj2sdk-1 4 2 version) and Xalan (version 2.02, forrocessing of XML documents) have been employedn implementing the information-tailoring proto-ype.
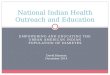
Fig. 2 shows the web portal’s high level architec-ure. The system inputs are the consumer diabetesnformation (CDI), quiz question pool and patient asuser, and the outputs are the presentation of the
ailored diabetes information, tailored quiz ques-ions and tailored agenda question pool.
The DIP collector collects data about theatient’s DIP (see Table 1). Generally speaking,here are two ways of user profile collection:xplicit and implicit. Explicit collection involvessking the user to provide the information directly,hile implicit collection occurs when the systembserves and uses user—system interactions to inferhe patient’s situation. In this web portal, exceptor collecting the history of a patient’s informationrowsing, profile collections require the patient toll in corresponding questionnaires. All collectedata are put into the DIP. The DIP is stored in aelational database implemented by mySQL.
The Information inference engine generates theailored & prioritized information — an XML docu-ent — on the basis of the patient’s DIP. Likewise,
2 Xalan-J 2.0 Design, http://xml.apache.org/xalan-j/design/esign2 0 0.html.
awtttb
mmunication support 583
he Quiz inference engine generates the Tailored &rioritized quiz questions. Both inference enginesave two stages: filtering and prioritization. TheIP evaluator determines whether the patient’s DIPatisfies the specific condition required by the Infor-ation prioritization rules. The Agenda generator
reates XML-structured agenda questions, includinguestions generated by the patients themselves,ystem recommended questions and the patients’revious agenda lists. The VT web portal uses theSLT processor to transform the XML-structuredailored & prioritized information, Agenda ques-ion pool and Tailored & prioritized quiz questionsased on the corresponding transformation scripts.
.2. User interface
he portal has three main adaptation services thatan be accessed by diabetes patients using the sys-em over the Web: Information Service, Quizzingervice and Agenda Service.
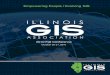
.2.1. Information Servicehe Information service provides the patient withelevant and prioritized information. Fig. 3 shows acreen snapshot of this service. The diabetes infor-ation source is modeled hierarchically, from cate-
ory, topic, to item. The menu bar at the left handide provides the top five important informationopics. The menu bar displays five prioritized infor-ation topics at a time. The ‘‘More’’ link under
he top five information topics brings the patiento the next five important topics. The main windowisplays the details of one topic. Information itemsf each topic are also prioritized and ranked in theescending order of importance (see ‘‘Most impor-ant to you’’ in Fig. 4). Similarly, five informationtems are presented at one time. Patients can goo the next five information items by clicking the‘More’’ link. The ‘‘Stars’’ indicate the importancessessment of the corresponding information item.he ‘‘Thumbs Up’’ conveys the patient’s rating ofhe information item. If the patient has recentlyiewed the item a number of times, the ‘‘Stars’’ade. Patients can also go through the informationtems of each topic one by one by using the ‘‘Next’’nd ‘‘Previous’’ links.
There are two actions users can undertake withach information item. The ‘‘Rate this informa-ion’’ button at the bottom of the main windowllows users to rate the presented item. The systemill use the patient’s rating to re-rank the order of
he tailored information items. The other action ishat the patient can add the information items intohe agenda by clicking the ‘‘Add to my agenda’’utton.

584 C. Ma et al.
ctur
3TbtSi
Fig. 2 High level archite
3.2.2. Quizzing ServiceThe quiz questions are also ranked in descendingorder of importance based on the patient’s DIP. Thequestion description, the right answer, the patient’sanswer and the further explanation of the answerare displayed. The purpose of the Quizzing Service
is not to test patients’ diabetes knowledge, butrather to provide an alternative way of learning. Ifthe patient’s answer is correct, this particular ques-tion will not be shown on the next patient log-in.tqcp
e of the VT Web portal.
.2.3. Agenda Servicehe four components of the Agenda Service haveeen introduced in Section 2.4. Fig. 4 showshe first and second components of the Agendaervice. The first component asks a patient tondicate: ‘‘What part of living with diabetes is
he most difficult or unsatisfying for you?’’ Thisuestion initializes a patient empowerment proto-ol [25]. The second component is the patient’sotential questions detected by the VT system.
Empowering patients with essential information and communication support 585
the I
Ttttdt
pt
Fp
Fig. 3 Snapshot of
his component shows both the questions andhe patient’s status that are related to the ques-
ions. For example, Fig. 4 shows the first ques-ion of the second component is the ‘‘Vascularisease risk factors,’’ and the patient’s status ofhe vascular disease risk factors are high bloodoat
ig. 4 First two components of the Agenda Service: (1) incoratient’s potential issues.
nformation Service.
ressure, smoking, and abnormal total choles-erol.
Fig. 5 shows the third and fourth componentsf the Agenda Service, and the patient’s previousgenda lists. The third component is the informa-ion selected by the patient during information
poration of the patient empowerment protocol; and (2)

586 C. Ma et al.
e inf
tCapetv
4ia
4Tbddfw(drpVmaso
tt
Fig. 5 Final two components of the Agenda Service: (1) thown questions.
browsing. The fourth component is the agendaquestions created by the patient herself/himself.For example, one of the questions (or ‘issues’)of this component is ‘‘How to adjust insulin’’.The patient’s previous agenda list allows thepatient to review previous asked questions orre-select the previously asked questions for thenext agenda list. For each component, the patientis able to delete the questions they think are nolonger useful. However, if the patient deletesthe diabetes-related issues (i.e., the questions ofthe second component), the deleted issues willappear again after 3 months since the deletiontime. The changes in a patient’s DIP are the onlyway to change the diabetes-related contents issuespermanently.
Apart from the above adaptation services, theportal also provides the patient with the entirediabetes information knowledge base without anyfiltering and prioritization. This facility gives thepatient user-controlled access to the total infor-mation along the lines of a traditional table of con-tents.
4. Evaluation of the Violet Technology
Two phases of evaluation have been conducted. Thefirst phase assessed the validity of the informationtailoring and prioritization algorithms in isolation,seeking patient and healthcare provider feedback
for algorithm improvement. The second phase ofevaluation involved a field trial using the VT webportal with patients as end users. All participants inthese two evaluation studies were recruited fromnTpT
ormation items selected by the patient; and (2) patient’s
he Endocrinology Department and the Diabetesentre of a metropolitan hospital (The Queen Eliz-beth Hospital, Adelaide, South Australia). Bothhases received approval by the human researchthics committees of the University of South Aus-ralia and the Adelaide North West Area Health Ser-ice.
.1. Phase 1 evaluation: validity ofnformation tailoring and prioritizationlgorithms
.1.1. Study design and methodshe evaluation participants were patients with dia-etes (a random sample of those identified asiagnosed in the past year through the hospitalatabase, recruited by mail-out with telephoneollow-up) and selected healthcare providers whoere familiar and involved in diabetes management
two doctors—–an endocrinologist and a GP; twoiabetes nurse educators; and one dietician). Theesearch aimed to establish the degree to whichatients and providers found topics prioritized byT to be relatively important, whether VT’s assess-ent of knowledge level from educational exposure
greed with patient self-assessment, and to seekpecific feedback for refining VT’s filtering and pri-ritization rules.
Patients were required to complete two ques-ionnaires each. The first questionnaire collectedhe data required by the DIP, with clinical compo-
ents obtained from the patients’ hospital records.hese data were then entered (remote from theatients) into the VT prototype by the first author.he VT algorithms were used to produce three lists
E d co
oi
•
•
•
dotmi1lvomopisn
qfE
wawmiabp
iatthtpfffawrti
4Ta
mpowering patients with essential information an
f 20 information items (consumer education top-cs) each:
InfoGroupR—–a random selection from the CDIsource file;InfoGroupS—–the top priority scores, after filter-ing, as weighted by the significant data-orientedprioritization rules (SigPRules); andInfoGroupB—–top priority scores as perInfoGroupS with additional weighting basedon estimated patient Knowledge Level (a subsetof the KnowPRules).
The three item lists were presented in ran-om order, with the patient blind to the naturef each list, as a component of the second ques-ionnaire. Patients were asked to score each infor-ation group in terms of its overall relevance and
mportance to their current situation (from 1—10,0 meaning most relevant) and to provide, from theists or otherwise, the 10 items they felt most rele-ant, in descending order of importance. The scoresf each information group on each of these twoeasures (i.e., the relevance score and the number
f items in the top-10 list) were contrasted using aaired t-test on the difference per patient to exam-ne contrasts among the information groups. Fig. 6hows an instance of a completed second question-aire.
After submitting (by post) the completed seconduestionnaire, a half hour semi-structured face-to-ace interview was conducted by the first author.ach interview was audio-taped and investigated:
cft5
Fig. 6 A sample of Questionnaire 2 of ph
mmunication support 587
hether the tailored topic lists (both InfoGroupBnd InfoGroupS) missed any topics that the patientsanted; why patients preferred a particular infor-ation group; whether the lists contained any
nformation that the patient did not think relevant;nd what the patients’ own estimates of their dia-etes knowledge level was (based on definitions, aser Section 2.3).
After completing the patient questionnaires andnterviews, healthcare providers participated in anudio-taped, one-hour focus group, facilitated byhe first author. One focus group meeting was withhe two doctors and a separate focus group waseld with the two nurses and dietician (to reducehe doctors’ influence over the other healthcareroviders). In these sessions, the providers gaveeedback on the DIPs and resultant InfoGroupB listsor three patients (one patient randomly selectedrom each Knowledge Level as estimated by the VTlgorithm). Providers were required to comment onhether they thought the tailored topic list was
elevant and important to the patient, in light ofhe patient’s DIP data and whether there were anymportant topics missing.
.1.2. Resultswelve patients (five females and seven males)greed to participate in the study and returned the
ompleted consent forms. One female dropped outrom the study due to acute illness. The age ofhe participants ranged from 38 to 62 years (mean3). Ten patients had type 2 diabetes and one hadase 1 evaluation (actual size is A3).

588 C. Ma et al.
Table 4 Patient relevance ratings and number of patients’ 10 most relevant items in list for random (InfoGroupR),significant data only (InfoGroupS) and both significant data and knowledge level (InfoGroupB) prioritized informationitems
Relevance rating (1—10) (n = 11) Number in 10 most relevant (n = 11)
Mean (standard deviation) P (paired-t) Mean (standard deviation) P (paired-t)
InfoGroupR 7.27 (2.05) N/A 2.63 (1.91) N/AInfoGroupS 7.91 (1.51) N/A 4.27 (1.90) N/AInfoGroupB 8.00 (1.48) N/A 4.27 (2.10) N/AInfoGroupS—InforGroupR 0.636 (2.84) 0.47 1.64 (2.73) 0.074
0.0.
pritoeriiswt
tsK2b0
atttobuatsitcitots
InfoGroupB—InfoGroupR 0.727 (2.61)InfoGroupB—InfoGroupS 0.901 (2.43)
type 1 diabetes. The period of diagnosis with dia-betes was 2—13 months at the time of interview(mean 7.5 months). All 11 patients completed andreturned the first and second questionnaires. Fig. 6shows one example of the completed second ques-tionnaire.
Table 4 summarizes findings on patient-assignedrelevance scores for each information group andfor number of patients’ 10 most-relevant informa-tion items appearing in each information group.InfoGroupR, InfoGroupS and InforGroupB have theexpected pattern in terms of means (S and B higherthan R, B highest) for relevance scores, but provideno statistically significant differences. The numberof information items from each group that appearin the patients’ 10 most-relevant items list showsInfoGroupS and InfoGroupB with equal means and ap-value between 0.05 and 0.10 for their superiorityover InfoGroupR.
Thirty-four percent of patients’ 10 most rele-vant items were covered in neither InfoGroupS norInfoGroupB. Reasons for omission were largely dueto information preferences outside the scope of thediabetes per se (e.g., depression, back pain andheadache) or outside the scope of the system imple-mentation at the time of the study (e.g., ‘sexualhealth’). Also, patient priority sometimes differedfrom the priority as assigned by our rules—–e.g.,‘overview of diabetes and eyes’ was ranked in thetop 10 by a newly diagnosed patient who had no eyeproblems.
During the interview sessions, all patients wereable to point out at least some irrelevant infor-mation items from InfoGroupR; and 8 out of 11patients (81.81%) agreed that the tailored infor-mation (InfoGroupS and InfoGroupB) was relevant.When asked why they preferred either InfoGroupBor InfoGroupS to InfoGroupR, reasons included: (1)
the tailored information answered their informa-tion preferences or interests better; (2) the tailoredinformation was directly related to their currentissues; (3) the tailored information met their com-ocwe
38 1.64 (2.65) 0.06890 0.00 (1.10) 1.00
rehension level; (4) the tailored information waselevant to their family history; and (5) the tailorednformation was ranked in an appropriate order. Onhe other hand, some patients did not think somef the tailored information items listed were rel-vant because: (1) they had not experienced theelated problems yet; (2) they felt they knew thenformation; and/or (3) they did not understand thenformation. Two participants preferred randomlyelected information despite the fact that some itas not relevant to their situation. This is because
hey liked the diversity of topics and wider scope.Patient-estimated Knowledge Level was similar
o the system estimate based on educational expo-ure (as per Table 3) with patients’ mean estimatednowledge Level at 2.23 and the system estimate at.00. System and patient estimates never differedy more than 1 (Pearson correlation coefficient is.55).
In the health provider focus groups, participantsgreed that the tailored information was relevanto the corresponding patient profiles. However,hey provided several suggestions for more informa-ion and prioritization rules, including: informationn the National Diabetes Services Scheme of Dia-etes Australia; information on sexual issues; andse of early symptoms of diabetic complicationss triggers for information on diabetic complica-ions. A number of rule categories entered discus-ion and received approval including those concern-ng patient behaviour changes, exercise, diet con-rol, frequency of dining out, medications and psy-hosocial problems. Moreover, the providers gavenput on tuning the priority of different informa-ion topics. Providers largely agreed with the basisf Knowledge Level estimation but were scepticalhat a person who had ever been a carer for a per-on with diabetes would know the correct skills
f diabetes management. They also thought thatounting a patient’s visits to diabetes educatorsas redundant with counting the patient’s diabetesducation sessions attended.
Empowering patients with essential information and communication support 589
Table 5 Web portal usage statistics
Patient registration Registration period: 23a to 126 days (median 73 days)Log-in times: 82 in total, individual patients had 2—15 log-ins (median 6)
Usage of the Information Service Access to the service: all 12 patientsAccess to the information items: 82 out of 257 information items have beenvisited for more than 10 s; individual patients accessed 1—55 items (mean20.2, very bimodal)
Usage of the Quizzing Service Access to the service: 5 out of 12 patientsNumber of quiz questions done: individual patients did 5—110 quiz ques-tions (mean 61.8)
an a
he sy
twc
4
4PftEtotgatan
(tcvtpu(gtpttidt
Vd
taptpenbtt
4Tfi(ttsVeltru
T
hIplfound the tailored information relevant. Patientsusing quizzes felt they were a good way to learn.Moreover, use of the portal inspired some patients
3 Actually, 24 patients were recruited but half were randomly
Usage of the Agenda Service Generation ofa Some patients experienced significant delays in accessing t
statistics were collected.
Observations from phase 1 were used to refinehe VT system, notably the SigPRule base, whichas then used for a field trial as a consumer edu-ation portal.
.2. Phase 2 evaluation: field trial
.2.1. Study design and methodsatients were recruited by response to flyers andace-to-face invitation (by the first author) athe waiting rooms of the Diabetes Centre andndocrinology Department. Patients had to agreeo using the web portal for 3 months (via homer public library Internet access), with the offer ofraining as required. Healthcare providers for focusroup feedback were the same as in phase 1. Theim was to assess the usability of the VT web portal,o see how it was used, what patients thought of it,nd what providers thought about the appropriate-ess of the web environment for diabetes patients.
Each patient was given a web portal accountusername and password). At the time of first log-inhey were directed through the registration pro-ess, leading to specification of DIP data (clinicalalues were verified remotely by the investiga-ors using data from the hospital database). Eachatient received a phone call reminding him/her tose the VT system, and to answer profile questionsif outstanding) every 2 weeks. An automated log-ing system was used throughout the field trial. Athe end of the study, patients were asked to com-lete a questionnaire collecting their feedback onhe VT system. Half of the patients were requestedo attend an audio-taped, half-hour, face-to-facenterview that firstly, investigated why they liked orid not like the system, and secondly, sought fur-
her suggestions for improving it.After the patients had completed 3 months ofT portal use, two provider focus groups were con-ucted (one for doctors and one for the nurses and
atimg
genda: 1 out of 12 patients
stem, greatly reducing the nominal 90-day trial period before
he dietician, as in phase (1). For the two mostctive portal users, the providers were shown theatients’ DIPs, tailored and prioritized informationopics, tailored and prioritized quiz questions andersonalized agenda questions. After a review ofach case, each provider completed a question-aire collecting his/her feedback on the systemehaviour with respect to that patient. In addition,he providers gave general comments on the VT sys-em.
.2.2. Resultswelve patients were recruited3, seven males andve females ranging in age from 35 to 65 yearsmean 51); all 12 had type 2 diabetes. There werehree patients who could not access the portal dueo not having a computer at home or other reasons,o the first author helped them to register with theT system in the Diabetes Centre and they werencouraged to use the VT system in a nearby publicibrary. None of the patients asked for training evenhough they knew that training was available onequest. Table 5 provides statistics on the patients’sage of the portal.
Nine patient questionnaires were returned.able 6 summarizes the questionnaire responses.
Six patients were randomly selected to attend aalf-hour, semi-structured face-to-face interview.n line with the questionnaire responses, mostatients agreed that the VT system is easy toearn and easy to use. Newly diagnosed patients
ssigned to a control group intended to commence portal usehree months after the initial group. For logistic reasons (includ-ng a high drop-out rate, probably exacerbated by the Christ-as/New Year holiday season), however, the use of the control
roup was abandoned.

590 C. Ma et al.
Table 6 Patient questionnaire responses on use of the VT-based web portal
Question Patient responses (n = 9)
Response Count
The prototype is easy to useAgree 7No opinion 1Disagree 1
The tailored information is relevantto my diabetes
Agree 7No opinion 1Disagree 1
The tailored information is useful
Strongly Agree 1Agree 6No opinion 1Disagree 1
The tailored agenda is usefulAgree 7No opinion 1Disagree 1
I would recommend this program toother people with diabetes
Strongly agree 4Agree 2No opinion 2Disagree 1
The questionnaires take too long tocomplete
Agree 4No opinion 2Disagree 3
The tailored information is easy tofollow
Agree 6No opinion 3
The tailored information meets myinformation needs
Agree 6No opinion 1Disagree 2
The tailored agenda questions areappropriate
Agree 6No opinion 2Disagree 1
The tailored agenda questions areeasy to follow
Agree 6No opinion 3
I suspect that the tailored agendareminds me with importantquestions that I might not haveasked my health providersotherwise
Strongly agree 5Agree 2No opinion 2
The tailored information is muchmore specific to my personalsituation
Strongly agree 1Agree 5No opinion 2Disagree 1
Would you like to continue usingthe web system?
Yes 5No response 3No 1

E d co
thtavins
•
•
•
•
hpasil
wmhvCff
If
Tcsp
t
•
•
mpowering patients with essential information an
o see the relevance of computers. On the otherand, experienced patients often found that theailored information was not useful because theylready knew it. A common suggestion was to pro-ide greater depth by linking on from the tailorednformation to external web sites. The portal wasot considered very useful for patients in severalpecific situations:
the patient was very experienced and aware ofall the tailored information;the patient’s diabetes was already well-controlled, and the patient was very comfortablewith his/her current knowledge and did not thinkit necessary to seek more information;the patient could not access the VT system easilyfor some reasons (e.g., did not have computer athome); andthe patient preferred general information to tai-lored information.
Table 7 shows questionnaire results for theealthcare providers in response to a review of theortal screens for the two most active users, Case A
nd Case B. In focus group discussions, the providersuggested that there was some information missingn both Case A and Case B, including cardiovascu-ar risk factors and psychosocial issues. Moreover, it•
Table 7 Healthcare providers’ questionnaire responses on
Question
The prototype is easy to use
The tailored information is relevantto the patient
There is much important information missingin the tailored information
The tailored information is important to the patient
The tailored agenda is useful
The tailored agenda questions areimportant for the patient to know
I suspect that the tailored agendaprovided important questions that Imight not have discussed with thepatient otherwise
I would recommend this program tomy patients with diabetes
mmunication support 591
as suggested that the priority of the tailored infor-ation should be adjusted so psychosocial issues
ad the highest priority (in the Information Ser-ice and as suggested issues in the Agenda Service).omments on the VT system from providers rein-orced the appropriateness of the items suggestedor the patient agenda, including:
think the agenda is good because the patients haveour questions, and they may forget two. (- GP)
he agenda did come through strong — cardiovas-ular at the top, the cardiovascular, blood pres-ure and foot care, whatever, so it seems to berioritized. . . (- Nurse)
Health professional suggestions for general sys-em improvement included:
A default page should be available for patientswho have well-controlled diabetes, such as pageof key consumer resources;The system should detect trend in weight orHbA1c so that the appropriate information or
agenda questions could be given to the patientsat an early stage;Patients should receive summary feedback oftheir quiz results;VT portal with respect to two cases
Healthcare provider responses (n = 5)
Response Case A Case B
Agree 5 5
Strongly agree 1 0Agree 3 3Disagree 1 2
Agree 2 3Disagree 3 2
Agree 5 5
Strongly agree 1 0Agree 4 4Disagree 0 1
Strongly agree 2 1Agree 3 4
Strongly agree 0 1Agree 3 3No opinion 1 0Disagree 1 1
Strongly agree 2 1Agree 3 4

ctopwniTatbuMmiwv
5
TslDtfopaAmd
sAustralia are high , yet the majority of patientsapproached to use the web portal declined, usu-ally on the grounds that they were not interested,
592
• More information is required in the CDI base, suchas how to deal with psychosocial issues; and
• The VT system should allow patients to track indi-vidual targets, plans or goals.
5. Discussion
We have developed a novel approach and architec-ture — VT — to help patients become empoweredand participate more in their own care throughgreater understanding and encouragement to askquestions of their healthcare providers. Patient andhealthcare provider responses to the technology, asrevealed through two phases of evaluation study,are encouraging and have provided direction forimproving the technology.
Generally, the results show support that VT andthe VT-based portal have substantial ‘face validity’(i.e., it looks right) as a mechanism to prioritizelearning and promote a focus on essential informa-tion. Face validity is demonstrated in three majorways:
Patient use and usability—–for patients willing toparticipate in the field trial, there was minimalexpression of difficulty in using or understandingthe system. Basically, if they could (and would)make it onto the Internet, they could use the sys-tem; there was minimal seeking of offered help,and nil expression of confusion.Patient feedback—–patient feedback was almostexclusively supportive with respect to the systemfeatures and their presentations. This is not to saythat some patients would not like more featuresor to act outside of those features.Healthcare provider feedback—–healthcareproviders gave strong support for the value ofthe system as a whole in the context of thespecific patients reviewed. Critical feedbackof healthcare providers became constrained tolimited and specific areas with the refinementsbetween phase 1 and phase 2. The providers areempowered, knowledgeable and passionate aboutquality diabetes care—–they are not inclined to‘hold back’ on criticism if any deficit can bediscerned.
Quantitative findings have to be viewed as pre-liminary and suggestive due to the scale of theevaluations; however, the questionnaire responsesare particularly worthy of highlighting, includingthe following:
Strong support (seven-to-one) for ease-of-use, rel-evance of tailored information, and utility of tai-lored information and agenda suggestions from thefield trial participants;
pc
C. Ma et al.
Agreement of all five healthcare providers (Agreeor Strongly Agree in the contexts of both cases)that: they would recommend the system to theirpatients with diabetes; the tailored informationand agenda suggestions were important; and theybelieved the portal was easy to use; andMixed levels of provider support (although alwayswith majority support) for the utility of theagenda function and the quality of prioritization(relevance of tailored information and suggestedagenda questions) with respect to specific cases.This demonstrates the willingness of the providersto disagree when a flaw could be identified.
The individuality of patients stands out, espe-ially in the phase 1 results. We were surprisedo find no significant superiority in patient ratingf the relevance of VT-selected topic lists as com-ared to random topics. Moreover, there is onlyeakly-positive association (p < 0.10) to the greaterumber of items in the VT-prioritized lists of top-cs appear in the patients’ own Top 10 topic lists.his owed to a range of individual priorities, suchs patients preferring random topic lists due toheir greater breadth and patients’ Top 10 topicseing outside of diabetes. These sorts of individ-al priorities re-emerged in the phase 2 interviews.oreover, from phase 2 we can identify two (notutually exclusive) patient groups for which prior-
tization may have minimal benefit: (a) those withell-controlled diabetes; and (b) those who areery confident in their diabetes knowledge.
.1. Limitations
he findings are obviously limited by the sampleizes in terms of patients and providers, but are alsoimited by the duration of the reported field trial.iabetes patients are typically expected to visitheir doctor once every 6 months. A trial, there-ore, should probably span several 6-month peri-ds in order to observe progressive improvement inatient-provider partnership due to online learningnd agenda-formulation support. Low usage of thegenda Service in the field trial is unsurprising sinceany patients did not attend a routine doctor visituring the field trial period.
Recruitment of participants for phase 2 wasurprisingly challenging. Levels of Internet use in
4
4 66.4% penetration, per Nielsen, as at February 2005, as com-ared to 67.8% for the United States (www.internetworldstats.om/stats.htm).

E d co
cwIl
ibabnMwtddfss
5
Mcdw
tSatcdemcnoti
appsqvHatcpfpmfin
bmRawadttpo
shgpptatve
atwtfmcihgtriqsataftvfsf
pBet
mpowering patients with essential information an
omfortable or able to access the Internet. Thereould be some age and socio-economic bias against
nternet use in the population approached, but theevel of resistance was still significant.
From an engineering perspective, more contents needed. Our key information resource [23], is,y title and design, an ‘essential guide,’ yet we seenumber of issues that are not covered. While a
ook for patients can suffer from intimidating thick-ess, this is less of a problem for a web resource.ore coverage on approaches to psychosocial issuesould be useful, as well as more detail on areas par-
icularly actionable by the patient, such as moreetailed food tips and even healthy recipes. At aifferent level, a segment of patients expressedrustration at the limitations of a fixed informationource, and a desire for integration with Internetearch facilities.
.2. Related work
any systems for provision of personalized health-are information have been developed. Herein weiscuss a few that are most relevant to the approache have taken with VT.A significant consumer health information sys-
em is CHESS [27]. In CHESS, its ‘‘Informationervices’’ provide frequently asked questions andnswers to some specific contexts, but the ques-ions are not tailored to the patient’s personal cir-umstance. The ‘‘Analysis Services’’ collect patientata (both the data on health status and other rel-vant data) and provides feedback and/or relevantaterials according to these data, which can be
onsidered as tailored information. However, CHESSeither systematically prioritizes information basedn the patient’s status nor does it take into accounthe patient’s knowledge level in providing tailorednformation.
The management of patient questions has beenddressed in a variety of ways. PEAS [17] providesatients with relevant information concerning theirersonal status with related questions and answers,o as to encourage patients to formulate their ownuestions prior to a health visit. CHESS [27] pro-ides disease-related frequently asked questions.owever, both of these systems are aimed moret providing questions with answers for knowledgeransfer, rather than stimulating patient-providerommunication. CareLink was developed to sup-ort families with premature infants [28]. CareLinkacilitates patients’ communication with health
rofessionals through online messaging. The com-unication facility provided by CareLink exempli-es use of the Internet as an alternative commu-ication channel between doctors and patients,cgss
mmunication support 593
ut provides no deep support for question for-ulation. The Accu-Chek Interview (ACI) is a CD-OM-based psychosocial assessment tool [29]. Thessessment is implemented via a questionnaireith 20 questions, and the assessment covers thereas of diabetes-related emotional distress, majorepression, hypoglycemia, and smoking. The sys-em presents five self-care topics for patientso select one for discussion with their healthroviders; it also allows patients to type in theirwn topics or select ‘‘No topic today.’’
The systems described above largely circum-cribe the approach to question management weave taken with VT. We believe, however, we haveone a step further in the representation of theatient questions as persistent objects (essentiallyart of the health record), where these ques-ions can be managed into compositions such as angenda, and where the basis for suggested ques-ions is deeply integrated with the information ser-ice, including patient knowledge level and prefer-nces.
A system for migraine sufferers by Buchanan etl. [18,19] uses natural language (NL) generationechnologies to create personalized explanationsith a focus on the system’s estimated communica-
ive goals of the user. This system is exceptionalor incorporating results of a study of patient infor-ation desires, including common fears and mis-
onceptions (e.g., concern that the migraine mayndicate a brain tumor). It collects a user’s medicalistory and — based on these data — dynamicallyenerates explanations of key concepts in a fashionailored to that particular user. It conducts impliciteasoning on the user’s knowledge level by observ-ng the user’s reading history. If a user asks the sameuestion twice, the system assumes that there is atate of user confusion or dissatisfaction with somespect of the explanation and, as a result of this,he system selects a different strategy for gener-ting an answer. The different explanation aims toacilitate the user’s understanding by introducinghe information from different angles. The disad-antage is that changeable information could con-use the user, and may be confusing if the userimply wants to review an explanation for rein-orcement.
While we have been inspired by their use ofatient profiles, we have chosen not to emulateuchanan et al. on the use of NL generation. Thengineering costs of developing NL generation sys-ems are high and, recently, some doubt has been
ast on the effectiveness of such methods. STOPenerates tailored smoking cessation letters formokers [30]. A clinical trial with 2553 smokershowed no significant difference in cessation rates
tocwr
6
Eaabctmoafnaaw
tiihmqtcatwfaigpspstotrrn
hf
594
between smokers who received a tailored letterand those who received a non-tailored letter. Moreimportantly, however, we believe NL generationcomes too close to aiming to supplant rather thansupport patient-provider communication. Generat-ing dynamic, personalized natural language servesto simulate a human healthcare provider, whichwe believe is an inappropriate metaphor for onlinelearning for patient self-management.
5.3. Implications
The motivation to continue investigating consumerinformation prioritization in chronic disease man-agement is high. Both patients and providersstrongly supported the importance of the tailoredinformation and generally supported the prioritiesassigned. The average amount of online readingconducted by patients in the field trial was fairlylimited at a mean of around two items per week(see Table 5), indicating a great deal of value in‘pushing’ a couple of truly essential topics. Patientfeedback indicates that the greatest benefit ofthis technology may lie with relatively newly diag-nosed patients. Both patient and provider feedbacksuggested provision of a display of patient self-monitoring results. A monitoring-centered displaymay be the more appropriate home base in a portalfor stable and well-informed patients.
Patient desire for links to Internet searchingcame through strongly in interviews, aligning withhigh use of the Internet for health queries in thosewith serious conditions generally (e.g., see [31]).Satisfying this desire for broad searching wouldclearly help to address user interest in the por-tal. It is a somewhat different issue, however, asto whether this would make the promotion of bet-ter patient outcomes more effective. The VT sys-tem is designed to promote, not supplant, patient-provider interaction. The source material indexedby the portal stays close to this philosophy, butthe same could not be said of all health mate-rials on the Internet. We believe it is the iden-tification of essential topics to promote patient-provider interaction, not their ‘answer’ throughonline reading, that is a key contribution of ourarchitecture.
Better integration of the portal with the main-stream healthcare system seems likely to improveits uptake, as well as having potential to improvepromotion of the patient-provider partnership. Ourrecruitment protocol for the field trial did not per-
mit direct ‘referral’ of the patient by their health-care provider. While recommendation was possible,there was no specific trigger for this in the processesat the participating clinical settings. VT-type priori-ogsl
C. Ma et al.
ization technology could add a significant elementf dynamism to existing technologies for healthonsumer online learning, especially if integratedith electronic health records and personal health
ecords.
. Conclusion and future research
ven though doctor—patient partnership has beendvocated for nearly two decades, using ITpproaches to support the partnership have noteen adequately explored. Consumer education islearly a requirement for effective communica-ion, partnership and empowerment, but to beost effective this education should be focused
n opportunities for action. We have taken anpproach based on customization of online learningor consumers incorporating emphasis of individualeeds, the fact that individual needs are dynamic,nd that providing the right information requiresddressing psychosocial issues and preference, asell clinical issues per se.We have developed an innovative architecture
hat emphasizes assignment of priority to consumernformation needs as the underlying mechanism forndividualized partnership support. The items ofighest priority are emphasized as essential infor-ation for online learning, based on readings anduizzes, in a dynamic web portal. In addition,he portal provides an agenda service to facilitateonsumer compilation of questions into hardcopygendas that they can take to appointments withheir healthcare providers. The agenda service,orking integrally with the prioritization algorithms
or online learning, facilitates placement of usernd machine-selected items of high priority and/ornterest into the agenda. Prioritization algorithmsive weight to topics on significant clinical andsychosocial issues, as well as educational expo-ure and user-assigned priority. The portal is under-inned by a modular architecture that makes exten-ive use of XML technologies (notably, to presenthe core consumer information, quizzes, and pri-ritization rules) and features a Diabetes Informa-ion Profile that supports the diverse patient dataequirements of the prioritization algorithms. Weefer to the components collectively as Violet Tech-ology.
Evaluation of the VT and the VT-based web portalas proceeded through two phases. The first phaseocused on information topic prioritization in a lab-
ratory setting, and the second phase involved aeneral field trial by diabetic consumers. While thecope and format of these studies permit only pre-iminary findings, we can say that the information
E d co
acoct
d1ptciarrrT2tsTueitRm
dtoqigcavcm
W
Ismc
em
W
Ab
ta
lipv
ttc
A
WQtwoDLpDcaLita
R
mpowering patients with essential information an
nd agenda services have ‘face validity’ in light ofonsumer and healthcare provider feedback. More-ver, usability issues appear minimal among thoseonsumers willing to enrol (at least those who thinkhey want to use it can).
Each evaluation phase has provided us withirections for enhancing the system. From phasewe identified several areas for improving the
rioritization rules (including use of early symp-oms of complications and location (Australia) spe-ific information on support services), which werencorporated for phase 2. Phase 2 revealed somereas for further rule refinements (e.g., greateresponsiveness to psychological issues) and (largelyelated) areas where it would be useful to incorpo-ate more consumer information for prioritization.he greatest consumer interest revealed in phasewas for the ability to move on from the informa-
ion provided within the portal to search externalources for more extensive and advanced reading.his demand is shaping our ongoing research towardsing the VT components for consumer search queryxpansion and reformulation. Provider feedbackndicated considerable interest in adding featureso the portal of a more general Personal Healthecord nature, such as trend graphs of consumeronitored data.A more extensive field trial, both in terms of
uration and patient numbers, is needed to providehe data to assess quantitative changes in indicatorsf patient-provider partnership (e.g., number ofuestions asked in healthcare visits) and ultimatelyn indicators of clinical outcomes (notably improvedlycaemic control as measured by HbA1c). We areurrently working to incorporate an automated userccount and profile creation procedure at our uni-ersity Podiatry Clinic (which has a high diabeticase load) as a mechanism for larger-scale enrol-ent in the VT-based web portal.
hat is already known on this topic
n diabetes management, doctor—patient partner-hip in both diabetes care and doctor—patient com-unication improves patients’ compliance and out-
omes.Computer-based education is an effective strat-
gy for transferring knowledge and skill develop-ent for patients with chronic disease.
hat this study adds
modular architecture using XML technologies cane used to map diabetes consumer profiles to priori-
mmunication support 595
ized consumer education topics for online learningnd consumer agenda creation.
The resultant web portal and prioritized topicists have face validity and are supported by pos-tive responses from consumers and healthcarerovider focus groups regarding ease-of-use, rele-ance and utility.
Consumers show remarkable individuality inheir ranking of topic relevance and in the topicshey identify as most relevant or important to theirurrent situation.
cknowledgements
e extend our thanks to all the patients of Theueen Elizabeth Hospital Diabetes Centre who par-icipated in our evaluation studies, as well as thoseho provided feedback in the formative stagesf the project, and also to Dr. Stephen Leow,r. Catherine Chittleborough, Dr. George Phillipov,uisa Pinto, Wendy Martin, Jane Giles, Melissa Cara-etis, Teresa Sgardelis, Lesley Roberts and all theiabetes Center staff for their support. We appre-iate the valuable feedback from Jean-Pierre Cal-bretto, Eric Brown, Sistine A. Barretto and Phillipock. We thank Amy Gordon for her contributionsn graphic design. We also thank Diabetes Aus-ralia, Novo Nordisk and Kidney Health Australia forpproving the use of their materials.
eferences
[1] M.M. Funnell, R.M. Anderson, Empowerment and self-management of diabetes, Clin. Diabetes 22 (3) (2004)123—127.
[2] M.M. Funnell, R.M. Anderson, The problem with compliancein diabetes, JAMA 284 (13) (2000) 1709.
[3] J. Hiscock, R. Legard, Snape D., Listening to Diabetes Ser-vice Users: Qualitative findings for the Diabetes NationalService Framework, National Centre for Social Research,2001.
[4] M.M. Funnell, R.M. Anderson, Working toward the next gen-eration of diabetes self-management education, Am. J.Prev. Med. 22 (4, Suppl. 1) (2002) 3—5.
[5] C.G. Pooley, C. Gerrard, S. Hollis, S. Morton, J. Astbury, ’Ohit’s a wonderful practice . . . you can talk to them’: a qual-itative study of patients’ and health professionals’ viewson the management of type 2 diabetes, Health Soc. CareCommunity 9 (5) (2001) 318—327.
[6] R. Street, V. Piziak, W. Carpentier, J. Herzog, J. Hejl,G. Skinner, L. McLellan, Provider-patient communicationand metabolic control, Diabetes Care 16 (5) (1993) 714—721.
[7] C. Charles, A. Gafni, T. Whelan, Shared decision-making inthe medical encounter — what does it mean — (or it takes atleast two to tango), Soc. Sci. Med. 44 (5) (1997) 681—692.
[8] C. Charles, A. Gafni, T. Whelan, Decision-making in thephysician-patient encounter: revisiting the shared treat-

596
ment decision-making model, Soc. Sci. Med. 49 (5) (1999)651—661.
[9] G. Eysenbach, Possibilities for fundamental change in thehealth system in the electronic world (2002).
[10] D. Lewis, Computer-based approaches to patient educa-tion: a review of the literature, J. Am. Med. Inform. Assoc.6 (4) (1999) 272—282.
[11] C.A. Barry, C.P. Bradley, N. Britten, F.A. Stevenson, N.Barber, Patients’ unvoiced agendas in general practiceconsultations: qualitative study, BMJ 320 (7244) (2000)1246—1250.
[12] C. Charles, A. Gafni, T. Whelan, How to improve communi-cation between doctors and patients, BMJ 320 (7244) (2000)1220—1221.
[13] P. Little, M. Dorward, G. Warner, K. Stephens, J. Senior,M. Moore, Importance of patient pressure and perceivedpressure and perceived medical need for investigations,referral, and prescribing in primary care: nested observa-tional study, BMJ 328 (7437) (2004) 444.
[14] B. Shapira, P. Shoval, U. Hanani, Stereotypes in informationfiltering systems, Inform. Process. Manage. 33 (3) (1997)273—287.
[15] Generating personalised information using the medicalrecord, in: K. Binsted, A. Cawsey, R. Jones (Eds.), Proceed-ings of AIME 95, Artif. Intell. Med., Springer-Verlag, Berlin,New York, 1995, pp. 29—41.
[16] S.S.R. Abidi, C.Y. Han, S.R. Abidi. Patient Empower-ment via ‘Pushed’ Delivery of Personalised HealthcareEducational Content Over the Internet. MEDINFO 2001,in: Proceedings of the 10th World Congress on Medi-cal Informatics, Amsterdam, IOS Press, 2001, pp. 1425—1429.
[17] S.W. McRoy, A. Liu-Perez, S.S. Ali, Interactive computerizedhealth care education, J. Am. Med. Inform. Assoc. 5 (4)(1998) 347—356.
[18] B.G. Buchanan, G. Carenini, V.O. Mittal, J.D. Moore,
Designing computer-based frameworks that facilitatedoctor—patient collaboration, Artif. Intell. Med. 12 (2)(1998) 169—191.[19] B.G. Buchanan, J.D. Moore, D.E. Forsythe, G. Carenini,S. Ohlsson, G. Banks, An intelligent interactive system
C. Ma et al.
for delivering individualized information to patients, Artif.Intell. Med. 7 (2) (1995) 117—154.
[20] L.J. Beeney, A.A. Bakry, S.M. Dunn, Patient psychologi-cal and information needs when the diagnosis is diabetes,Patient Educ. Counsel. 29 (1) (1996) 109—116.
[21] K. Lorig and associates, Patient education: a practicalapproach, Sage Publications, Inc., 2001.
[22] S.H. Rankin, K.D. Stallings, Patient Education: Issues, Prin-ciples, Practices, Lippincott, Philadelphia, 1990.
[23] P. Phillips, L. Brown, T. Dunning, Diabetes & You—–The Essen-tial Guide, Diabetes Australia, 2002.
[24] L. Calvi, P. De Bra, Proficiency-adapted information brows-ing and filtering in hypermedia educational systems,User Modeling and User-Adapted Interaction 7 (4) (1997)257—277.
[25] R.M. Anderson, M. Pibernik-Okanovic, The patient empow-erment approach to diabetes care, Diabetologia Croatica28 (3) (1999).
[26] M.M. Funnell, R. Nwankwo, M.L. Gillard, R.M. Anderson,T.S. Tang, Implementing an empowerment-based diabetesself-management education program, Diabetes Educator 31(1) (2005) 53—61.
[27] D.H. Gustafson, R.P. Hawkins, E.W. Boberg, F. McTavish, B.Owens, M. Wise, H. Berhe, S. Pingree, CHESS: 10 years ofresearch and development in consumer health informaticsfor broad populations, including the underserved, Int. J.Med. Inform. 65 (3) (2002) 169—177.
[28] H.S. Goldberg, A. Morales, L. Gottlieb, L. Meador, C. Safran.Reinventing Patient-centered Computing for the Twenty-first Century, MEDINFO, Amsterdam, IOS Press, 2001, pp.1455—1458.
[29] G. Welch, D.W. Guthrie, Supporting lifestyle change witha computerized psychosocial assessment tool, DiabetesSpectr. 15 (3) (2002) 203—207.
[30] E. Reiter, R. Robertson, L.M. Osman, Lessons from a failure:generating tailored smoking cessation letters, Artif. Intell.144 (1—2) (2003) 41—58.
[31] S. Dickerson, A.M. Reinhart, T.H. Feeley, R. Bidani, E. Rich,
V.K. Garg, C.O. Hershey, Patient internet use for healthinformation at three urban primary care clinics, J. Am. Med.Inform. Assoc. 11 (6) (2004) 499—504.