Embed Size (px)
Citation preview
EMS
81010
Intranasal Medications: Prehospital Setting
Todd Davis, MD, EMT-BEmergency Medicine
University of Cincinnati Cincinnati, OH
EMS
81010
Objectives1. Recognize the anatomy of
the intranasal route and its implications for the prehospital setting.
EMS
81010
Objectives2. Identify pharmacology of
common intranasal medications used in the prehospital setting.
EMS
81010
Objectives3. Indicate pharmacological
variances among intravenous (IV), intranasal (IN), and intramuscular (IM) routes.
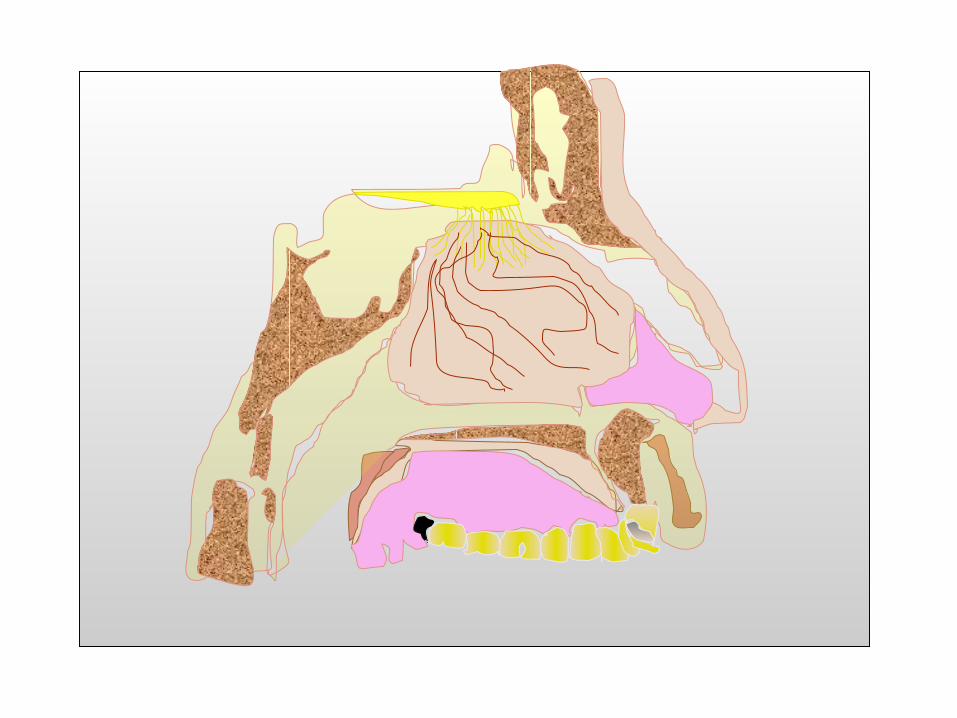
Intranasal Route

Video of needle stick Goes Right HERE!
15-57%
The Nose
• 30 square inches of total mucosal surface
Many Devices(mucosal atomizer is
most common)
Many Devices(plastic catheter)
Many Devices(metered dose)
Contraindications
Is the dosage higher?
Yes
Does the rate of absorption
vary?
Naloxone (Narcan)
Who gets Naloxone?
Texas and Opioids
• 922,208,500 mg of oxycodone (Percocet)
• 3,064,043,640 mg of hydrocodone (Vicodin)
Dosing Naloxone
• Concentration 1mg/mL
• Adult: 2mg IN (1mg per nare)
Dosing Naloxone
• Pediatric: 0.1mg/kg (20kg child may get up to 2mg)
Study (Naloxone)
• Bioavailability was 100% via both routes
–peak levels of intranasal (IN) within 3 minutes
Study (Naloxone)
– intravenous (IV) and IN have same half-life (t½)
Pharmacokinetic Study (Naloxone)
• Crossover, volunteer study with 6 healthy males
Pharmacokinetic Study (Naloxone)
• Levels at 5, 10, 15, 30, 45, 60, 90, 120, 180, 240 minutes
Predicted Concentrations
• Dowling et al. Population pharmacokinetics of intravenous, intramuscular, and intranasal naloxone in human volunteers, Ther Drug Monit, 2008;30(4):490-496
Predicted Concentrations
• .08 milligrams (mg)
Predicted Concentrations
• 2 mg
Predicted Concentrations
• Takes longer to peak
– intramuscular
– intranasal
Do you still treat to effect?
Key Limitations
• Healthy volunteers versus unconscious patients
Key Limitations
• Low concentrations
• Small sample for study
Study• Nasal Administration of
Naloxone for Detection of Opiate Dependence -Journal of Psychiatric Research. 1992 Jan; 26(1):39-43
End Points
• Clinical rating scale Clinical rating scale ((CRSCRS))
– nauseanausea
– vomitingvomiting
– see hand out...see hand out...
End Points
• Physicians’ ratings Physicians’ ratings were blinded to patient were blinded to patient groupgroup
End Points
• CRS measured at 0, 1, CRS measured at 0, 1, 5, 10, 15, and 30 5, 10, 15, and 30 minutes (min)minutes (min)
End Points
• Vital signs measured Vital signs measured at 0, 10 and 30 minat 0, 10 and 30 min
• Pupil measurements Pupil measurements taken at times 0, 10, 30 taken at times 0, 10, 30 min via cameramin via camera

Rating Scale Graph
• CRS revealed signs of withdrawal by 1 minute
• No significant difference in vital signs
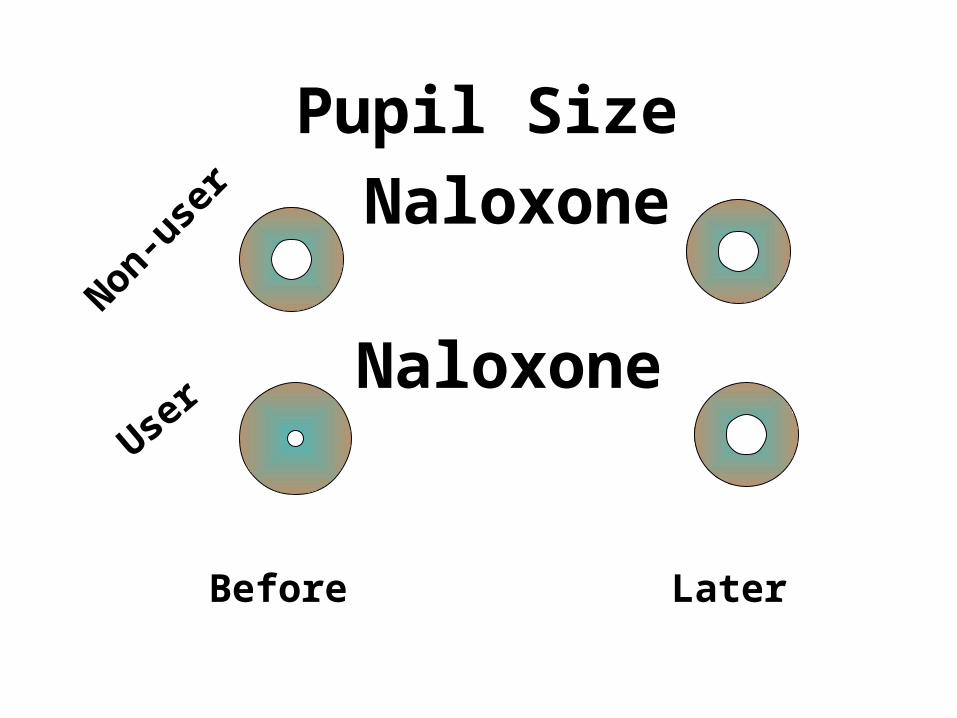
Pupil Size
Naloxone
Naloxone
Non-user
User
Before Later
Naloxone in the Emergency Department• Kelly et al. Intranasal Kelly et al. Intranasal
naloxone for life naloxone for life threatening opioid threatening opioid overdose. overdose. Emergency Emergency Medicine JournalMedicine Journal 2002; 2002; 19(4):37519(4):375
Naloxone in the Emergency Department• Dose of 0.8-2.0mg INDose of 0.8-2.0mg IN
• End point was time to End point was time to spontaneous spontaneous respirationrespiration
Naloxone in the Emergency Department• Key limitations:Key limitations:
– unblinded study unblinded study without control groupwithout control group
– unblinded reviewersunblinded reviewers
2005Society for Academic Emergency Medicine
(SAEM) Abstract
2005 SAEM Abstract
• Primary outcomes:
2005 SAEM Abstract
• Primary outcomes:
– time of medication administration to clinical response
2005 SAEM Abstract
• 154 patients
–104 IV Naloxone
–50 IN Naloxone
2005 SAEM Abstract
• Administration response
– IV 8.1 min
– IN 12.9 min
2005 SAEM Abstract
• Patient contact to response
– IV 20.3 min
– IN 20.7 min
Prospective Study
• Barton, et al. Efficacy of intranasal naloxone as a needleless alternative for treatment of opioid overdose...
Prospective Study
...in the pre-hospital setting. Journal of Emergency Medicine, 2005, 29(3): 265-271
Prehospital Study
• 14 year-olds
–overdose (OD)
– found down (FD)
–altered mental status (AMS)
Prehospital Study
• Outcomes
–number of subjects who “responded”
– time to response
Response
• 95 cases of administration
• 52 responders to IV or IN
• 43 Non-responders
Response
• 43 (83%) IN
• 9 (17%) no response to IN - required IV (5 had nose problem)
Is a deviated septum a contraindication?
Why did they follow up with IV if they did
respond to IN?
Time to Response(Administration)
• IN 4.2 min
• IV 3.7 min
Time to Response(Initial Patient Contact)
• IN 9.9 min
• IV 12.9 min
INVersus
Intramuscular (IM) Naloxone Study
IN Versus IM Study
• Kelly AM, et al. Randomized trial of intranasal versus intramuscular naloxone in the pre-hospital treatment...
IN Versus IM Study
...for suspected opioid overdose. The Medical Journal Of Australia. 2005; 182(1):24-27.
IN Versus IM Study
• Primary outcome: response time with RR>10
IN Versus IM Study
• Secondary outcomes: RR and Glasgow Coma Scale (GCS) at 8 minutes, need for rescue naloxone, and adverse events
IN Versus IM Study
• 182 patients
IN Versus IM Study
• Final sample
– IN 84
– IM 71
IN Versus IM Study
• Mean time to spontaneous respiration:
IN Versus IM Study
– IM 6 min, 95%, CI 5-7
– IN 8 min, 95%, CI 7-8
–probability (p)=0.006
IN Versus IM Study
• Time to GCS>11 (p=0.27)
IN Versus IM Study
• Presence of agitation (IM 13% versus IN 2%, p=0.02)
Naloxone use in a Tiered-Response
Emergency Medical Services System
Tiered-Response EMS
• 164 received Naloxone
Tiered-Response EMS
• Tiered EMS dispatch
–42% simultaneous dispatch
Tiered-Response EMS
• Tiered EMS dispatch
–24% advanced life support (ALS) dispatched based on additional information
Tiered-Response EMS
• Tiered EMS dispatch
–28% ALS dispatched based on basic life support (BLS) request
Tiered-Response EMS
• Simultaneous dispatch
–BLS 5.9 min
–ALS 11.6 min
–5.7 min difference
Tiered-Response EMS
• ALS request by BLS on scene (28% of the time):
– ALS time 16.1 minALS time 16.1 min
– 10.2 min difference 10.2 min difference
NOMAD:Not One More
Anonymous Death (overdose
prevention project)

http://http://nomadoverdoseproject.nomadoverdoseproject.
googlepages.comgooglepages.com
How about some How about some fentanyl for your fentanyl for your
pain?pain?
How about some How about some fentanyl for your fentanyl for your
pain?pain?
IV FentanylIV FentanylVersusVersus
IV MorphineIV Morphine
IV fentanylIV fentanylvs IV morphinevs IV morphine
• 54 adult patients with acute pain
• Randomized to which medication
IV fentanylIV fentanylvs IV morphinevs IV morphine
–equivalent doses
–re-dosed every 5 min, up to 30 min
IV fentanylIV fentanylvs IV morphinevs IV morphine
• Outcomes:
– initial and final visual analog scale score (0-100 scale)
–change in score
IV fentanylIV fentanylvs IV morphinevs IV morphine
• Outcomes: NONO difference difference
IV MorphineIV Morphinevsvs
IN FentanylIN Fentanyl
IV morphine vs IN IV morphine vs IN fentanylfentanyl
• 258 adult patients with severe pain
IV morphine vs IN IV morphine vs IN fentanylfentanyl
• Outcomes: initial, final, and change in verbal rating score (0-10 scale)
IV morphine vs IN IV morphine vs IN fentanylfentanyl
• NO difference
IV morphine vs IN IV morphine vs IN fentanylfentanyl
• IN fentanyl (15% serious adverse events)
IV morphine vs IN IV morphine vs IN fentanylfentanyl
– 3.8% poor tolerance3.8% poor tolerance
– <1% atomizer <1% atomizer malfunctionmalfunction
IV morphine vs IN IV morphine vs IN fentanylfentanyl
• IV morphine
–7% unable to establish IV
–3% difficult IV
Fentanyl in ChildrenFentanyl in Children
Fentanyl in ChildrenFentanyl in Children
• Borland M, Jacobs I, and Geelhoed G. Intranasal fentanyl reduces acute pain...
Fentanyl in ChildrenFentanyl in Children
...in children in the emergency department: A safety and efficacy study. Emergency Medicine 2002;14:275-280.
Fentanyl in ChildrenFentanyl in Children
• 45 children aged 3-12 45 children aged 3-12 needing immediate needing immediate analgesia per triage analgesia per triage nursenurse
Fentanyl in ChildrenFentanyl in Children
• IN fentanyl IN fentanyl administered followed administered followed by q5 min pain scores by q5 min pain scores by patient, caregiver, by patient, caregiver, and staffand staff
Fentanyl in ChildrenFentanyl in Children
• Rescue medication Rescue medication available at 20 minutesavailable at 20 minutes
Fentanyl in ChildrenFentanyl in Children
• Safe and effectiveSafe and effective
– 35.5 % single dose35.5 % single dose
– 31.1% two doses31.1% two doses
– 17.7% three doses17.7% three doses
– 15.5% four doses15.5% four doses
Fentanyl in ChildrenFentanyl in Children
• Safe and effectiveSafe and effective
– one needed rescue IV one needed rescue IV morphine at 20 morphine at 20 minutes minutes

Benzodiazepine Benzodiazepine MedicationsMedications
BenzodiazepineBenzodiazepine
• diazepam (Valiumdiazepam (Valium®®))
• lorazepam (Ativanlorazepam (Ativan®®))
• midazolam (Versedmidazolam (Versed®®))
• alprazolam (Xanaxalprazolam (Xanax®®))
BenzodiazepineBenzodiazepine
Ever use Ketamine? Ever use Ketamine?
Dosing - MidazolamDosing - Midazolam
• Use the 5mg/1mL concentration
• Adults: 5mg (2.5mg or 0.5mL per nare)
• Pediatrics: 0.2mg/kg
Dosing - MidazolamDosing - Midazolam
• Seizure complaints are common
• 71% - via EMS71% - via EMS
Dosing - MidazolamDosing - Midazolam
• Increase in dosage for IN medication to stop a seizure?
Optimal dosing/concentrations
still unidentified
Dosing - MidazolamDosing - Midazolam
• IV access is not easy in seizing patients
PharmacokineticsPharmacokineticsWermeling et al. Pharmacokinetics and pharmacodynamics of a new intranasal midazolam formulation...
PharmacokineticsPharmacokinetics...in healthy volunteers. Anesth Analg 2006;103:344-349.
PharmacokineticsPharmacokinetics• IN peaks faster and
higher than IM
PharmacokineticsPharmacokinetics• Lindhardt, et al.
Electro-encephalographic effects and serum concentrations after intranasal...
PharmacokineticsPharmacokinetics...and intravenous administration of diazepam to healthy volunteers. Br. J Clin Pharmacol 2001;52:521-527
PharmacokineticsPharmacokinetics• In healthy volunteers -In healthy volunteers -
4mg IN diazepam 4mg IN diazepam produced similar... produced similar...
PharmacokineticsPharmacokinetics
......electro-encephalography (EEG) (EEG) findings to 5mg IV findings to 5mg IV diazepamdiazepam
IV DiazepamIV DiazepamVersusVersus
IN MidazolamIN Midazolam
IV Diazepam Versus IV Diazepam Versus IN MidazolamIN Midazolam
• Arrival to seizure cessation was 8.0 min with diazepam IV
IV Diazepam Versus IV Diazepam Versus IN MidazolamIN Midazolam
• Arrival to seizure cessation was 6.1 minutes with midazolam IN

Prehospital Prehospital Intranasal MidazolamIntranasal Midazolam
Prehospital Intranasal Prehospital Intranasal MidazolamMidazolam
• Rectal diazepam intranasal midazolam
Prehospital Intranasal Prehospital Intranasal MidazolamMidazolam
• 124 patients witnessed seizure
–67 (54%) given no medication
Prehospital Intranasal Prehospital Intranasal MidazolamMidazolam
–18 (15%) given rectal diazepam
–39 (32%) given intranasal midazolam
OutcomesOutcomes
• Median seizure time
–per rectum (PR) diazepam 30 min
– IN midazolam 11 min
OutcomesOutcomes
• Patients with rectal diazepam were more likely to:
OutcomesOutcomes
–more likely to be intubated in the emergency department (ED)
OutcomesOutcomes
–need additional seizure (Sz) medication in ED
OutcomesOutcomes
–get admitted to the intensive care unit (ICU)
How about IN How about IN midazolam at home?midazolam at home?
ConclusionsConclusions

THANK YOU
Intranasal Medications: Prehospital Setting
If you have any questions about the program you have just watched, you may call us at: (800) 424-4888 or fax (806) 743-2233.Direct your inquiries to Customer Service.Be sure to include the program number, title and speaker.
EMS
81010
Release Date:
04/01/2010
EMS
81010
The accreditation for this program can be found by
signing in to
www.ttuhsc.edu/health.edu
This continuing education activity is approved by the Continuing Education Coordinating Board for Emergency Medical Services for 1.5 Advanced CEH. You have participated in a continuing education program that has received CECBEMS approval for continuing education credit. If you have any comments regarding the quality of this program and/or your satisfaction with it, please contact CECBEMS at: CECBEMS -12200 Ford Road, Suite 478Dallas, TX 75234 Phone: 972-247-4442 [email protected]
EMS
81010





























