-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
1/86
C
gH2AX Foci Analysis
Histon H2AX is phosporylated rapidly in response to
DNA double-strand breaks (DSB), leading to the forma-
tion of nuclear foci visualized by immunocytochemical
detection of gH2AX. gH2AX analysis is an exquisitely
sensitive technique to monitor DSB repair, amenable for
use with very low doses.
2-(Carbamimidoyl-Methyl-Amino)Acetic Acid
Creatine
Ca2+
Release ChannelsExcitationContraction Coupling
Ryanodine Receptors
Ca2+-Induced Ca2+ Release (CICR)
Ca2+-induced Ca2+ release (CICR) in myocytes is medi-
ated via opening of ryanodine receptors on the SR.
Ryanodine receptors are activated by adjacent
L-typevoltage-operated Ca2+ channels, which are in turn acti-
vated by depolarized plasma membranes. CICR subse-
quently leads to significant elevation of Ca2+ levels
intracellularly, allowing Ca2+ to bind to myofilament pro-
teins and initiate contraction of myocytes.
Caffeine
JAYNEM. KALMAR
Wilfrid Laurier University, Waterloo, ON, Canada
Synonyms3,7-dihydro-1,3,7-trimethyl-1
H-purine-2,6-dione;1,3,7-
trimethylxanthine;1,3,7-trimethyl-2,6-dioxopurine
DefinitionCaffeine (1,3,7-trimethylxanthine) is a plant
alkaloid
with a purine structure. Its chemical formula is
C8H10N4O2 and it has a molecular weight of 194.19 g.
Pharmacologically, caffeine is most frequently defined as
a central nervous system stimulant, although it is also
a weak diuretic and smooth muscle relaxant [1].
DescriptionCaffeine is an alkaloid that can be extracted from
plants
such as tea leaves, cacaoseeds, cola nuts, and coffee beans
or
synthesized from uric acid. Once purified, caffeine is
a white crystalline substance that is somewhat soluble in
water (as caffeine citrate) and many organic solvents.
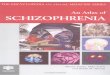
Caffeine has a number of dimethylated metabolites includ-
ing paraxanthine, theobromine, and theophylline
that differ with respect to the number and location of
methyl groups on their purine heterocyclic ring structure
(Fig. 1). Paraxanthine is the primary metabolite of caffeine
that acts as a central nervous system stimulant with potency
similar to caffeine. The metabolites theobromine and the-
ophylline are also naturally occurring plant alkaloids.
Asindicated by its chemical name (1,3,7-trimethylxanthine),
caffeine has three methyl groups positioned on N1, N3, and
N7 of the purine ring structure [1].
Pharmacologically, caffeine is best known for its
actions as a central nervous system stimulant; however,
Frank C. Mooren (ed.),Encyclopedia of Exercise Medicine in
Health and Disease, DOI 10.1007/978-3-540-29807-6,# Springer-Verlag
Berlin Heidelberg 2012
http://dx.doi.org/10.1007/978-3-540-29807-6_233http://dx.doi.org/10.1007/978-3-540-29807-6_233http://dx.doi.org/10.1007/978-3-540-29807-6_71http://dx.doi.org/10.1007/978-3-540-29807-6_71http://dx.doi.org/10.1007/978-3-540-29807-6_2990http://dx.doi.org/10.1007/978-3-540-29807-6_2990http://dx.doi.org/10.1007/978-3-540-29807-6_4010http://dx.doi.org/10.1007/978-3-540-29807-6_4005http://dx.doi.org/10.1007/978-3-540-29807-6_4005http://dx.doi.org/10.1007/978-3-540-29807-6_4004http://dx.doi.org/10.1007/978-3-540-29807-6_2061http://dx.doi.org/10.1007/978-3-540-29807-6_2061http://dx.doi.org/10.1007/978-3-540-29807-6_2835http://dx.doi.org/10.1007/978-3-540-29807-6_2835http://dx.doi.org/10.1007/978-3-540-29807-6_3116http://dx.doi.org/10.1007/978-3-540-29807-6_3116http://dx.doi.org/10.1007/978-3-540-29807-6_3117http://dx.doi.org/10.1007/978-3-540-29807-6_3117http://dx.doi.org/10.1007/978-3-540-29807-6_3117http://dx.doi.org/10.1007/978-3-540-29807-6_3116http://dx.doi.org/10.1007/978-3-540-29807-6_2835http://dx.doi.org/10.1007/978-3-540-29807-6_2061http://dx.doi.org/10.1007/978-3-540-29807-6_4004http://dx.doi.org/10.1007/978-3-540-29807-6_4005http://dx.doi.org/10.1007/978-3-540-29807-6_4005http://dx.doi.org/10.1007/978-3-540-29807-6_4010http://dx.doi.org/10.1007/978-3-540-29807-6_2990http://dx.doi.org/10.1007/978-3-540-29807-6_71http://dx.doi.org/10.1007/978-3-540-29807-6_233
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
2/86
the drug is sufficiently small and hydrophobic to cross the
blood-brain barrier and other cell membranes and there-fore has
the capacity to affect many tissues depending on
its concentration. Caffeine and other methylxanthines are
used therapeutically to prevent drowsiness, to treat mild to
moderate headaches in combination with analgesics, and
to treat apnea and arrhythmias in preterm infants [1].
Caffeine is approved by the US Food and Drug Adminis-
tration as a safe and effective stimulant and is available
over the counter. Three mechanisms of caffeines actions
have been observed in vitro: (1) intracellular calcium
mobilization via direct interaction with calcium channels
in the sarcoplasmic reticulum, (2) phosphodiesterase
inhibition, and (3) adenosine receptor antagonism [2].
The first two of these three mechanisms require millimolar
concentrations of caffeine that would be toxic in humans.
Nonetheless, it has been suggested that endogenous
modulators such as ATP may potentiate caffeine and
paraxanthines effects on the ryanodine receptor to
increase intracellular calcium concentration in intact skel-
etal muscle preparations. If this is the case, caffeine may
alter muscle function in vivo at concentrations much
lower than predicted by in vitro studies. In contrast, caf-
feine functions as an adenosine receptor antagonist at
caffeine concentrations in the micromolar range associ-
ated with plasma and brain levels following low to mod-erate
oral doses of the drug. Accordingly, the widespread
effects of caffeine on human tissues are largely attributed
to antagonism of adenosine receptors [2].
ApplicationCaffeine is well known for its effects on wakefulness
and
mental alertness. In 1958, Axelsson and Thesleff reported
that caffeine could generate muscle contractions in the
absence of neural or electrical activation, suggesting that
this legal, widely available, and socially acceptable drug
may improve both physical and mental performance. Sev-
eral decades of research have since clearly established that
caffeine is indeed ergogenic, enhancing performance in
many types of sports and exercise. It is now clear, however,
that the primary mechanism for these ergogenic effects
is via adenosine receptor antagonism rather than direct
effects on muscle.
Caffeines effects on human performance are most
evident in endurance sports such as running and cycling.
In these sports, dosages ranging from 3 to 9 mg/kg body
weight have been found to increase time to exhaustion or
time trial performance in placebo-controlled studies [4].
Caffeine. Fig. 1 Caffeine is a trimethylated xanthine that is
metabolized to three dimethylated xanthines including
theobromine, theophylline, and paraxanthine. Caffeine,
theobromine, and theophylline are plant alkaloids widely consumed
in
a variety of foods and beverages such as coffee, tea, and
chocolate, while the primary metabolite, paraxanthine, is only
found
endogenously. Due to its structural similarity to adenosine,
caffeine acts as a competitive adenosine receptor antagonist. This
is
the primary mechanism for caffeines effects as a central nervous
system stimulant
146C Caffeine
http://dx.doi.org/10.1007/978-3-540-29807-6_2990http://dx.doi.org/10.1007/978-3-540-29807-6_2990http://dx.doi.org/10.1007/978-3-540-29807-6_2990
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
3/86
The effects of caffeine on high-intensity exercise are not
as
clear. There are some reports that caffeine improves per-
formance on tests of anaerobic power, such as the Wingate
test, and other studies that report no effect of caffeine or
a decline in anaerobic performance in the caffeine trail
compared to placebo. In tests of anaerobic performance, it
appears that caffeine is more likely to enhance the perfor-
mance of trained athletes than untrained individuals [3].
Although caffeine is a weak diuretic, it does not appear
to alter sweat rate and total body water loss to an extent
that would impair performance or pose any risk to the
athlete [3].
Because caffeine is distributed to all body compart-
ments, it is difficult to isolate the biological mechanisms
responsible for its ergogenic effects. Previously, caffeine
was thought to enhance endurance performance through
enhanced lipolysis and glycogen sparing secondary to
phosphodiesterase inhibition and increased catecholaminerelease.
However, caffeine does not inhibit phosphodiester-
ase activity at physiological doses and while caffeine is
associated with elevated plasma epinephrine levels, there
is very little evidence to suggest that caffeine enhances
fat
oxidation [4]. Consequently, it is now generally accepted
that the ergogenic effects of caffeine are not of a
metabolic
origin and focus has shifted to alternative theories.
One possibility is that caffeine enhances skeletal mus-
cle contractile force, although there is some question as to
whether physiological levels of caffeine would be sufficient
to elicit the increase in intracellular calcium observedin
vitro. Most human studies report no effect of caffeine
on twitch amplitude, twitch half relaxation time, or max-
imal instantaneous rate of twitch relaxation in either
unfatigued or fatigued human muscle [5]. However, caf-
feine does offset the decline in tetanic force observed
during low-frequency electrical stimulation of muscle.
Because low-frequency fatigue has been attributed to
a reduction in calcium release by the ryanodine receptor, it
is possible that caffeine improves contractile output of
fatigued muscle under some conditions.
Placebo-controlled studies report increased muscle
activation and endurance times following caffeine admin-
istration that could not be attributed to changes in neu-
romuscular transmission or muscle contractile function.
This suggests that caffeine may also enhance human per-
formance via central mechanisms [5]. Adenosineis an
endogenous neuromodulator that exerts a tonic inhibi-
tory influence in the central nervous system by decreasing
excitatory neurotransmitter release and the firing rates of
central neurons. Due to its structural similarity to adeno-
sine, caffeine functions as an adenosine receptor antago-
nist and reverses many of the inhibitory effects of
adenosine at microMolar concentrations [2]. Caffeine has
been found to increase neurotransmitter release and firing
rates via A1 receptor antagonism, increase dopaminergic
transmission, and increase spontaneous motor activity
and treadmill running time of rats [5]. In human studies
of corticomotor excitability, caffeine potentiates
cortically
evoked potentials and reduces the duration of the cor-
tical silent period. It also increases the amplitude of the
Hoffman reflexand self-sustained firing of motor units
which suggests that the drug may also act on the neuro-
muscular system at a spinal level. Finally, caffeine is
asso-
ciated with reductions in pain and force sensation which
may contribute to enhanced endurance performance [5].
Restricting or banning a substance consumed in foods
and beverages by many people on a daily basis poses
a challenge to anti-doping agencies. In the past, the Inter-
national Olympic Committee (IOC) restricted the use of
caffeine by athletes, allowing a maximal urine level of12 mg/ml.
Over 95% of ingested caffeine, however, is
excreted as paraxanthine-derived urinary metabolites
rather than caffeine. As such, athletes would have to con-
sume approximately 9 mg of caffeine per kg body weight
to reach the IOC urinary caffeine limit whereas ergogenic
effects have been demonstrated following oral caffeine
dosages as low as 3 mg/kg body weight. Although caffeine
use is not prohibited by the World Anti-Doping Agency
(WADA), it is monitored for use in competition via the
WADA Monitoring Program for the purposes of detecting
patterns of misuse of this stimulant in sport. Use ofcaffeine
out of competition is not monitored.
References1. Brunton LB, Lazo JS, Parker KL (eds) (2005) Goodman
& Gilmans
the pharmacological basis of therapeutics, 11th edn.
McGraw-Hill,
New York
2. Fredholm BB (1995) Astra award lecture. Adenosine,
adenosine
receptors and the actions of caffeine. Pharmacol Toxicol
76:93101
3. Goldstein ER, Ziegenfuss T, Kalman D, Kreider R, Campbell
B,
Wilborn C, Taylor L, Willoughby D, Stout J, Graves BS,
Wildman R, Ivy JL, Spano M, Smith AE, Antonio J (2010)
Interna-
tional society of sports nutrition position stand: caffeine and
perfor-
mance. J Int Soc Sports Nutr 7:54. Graham TE (2001) Caffeine and
exercise: metabolism, endurance
and performance. Sports Med 31:785807
5. Kalmar JM (2005) The influence of caffeine on voluntary
muscle
activation. Med Sci Sports Exerc 37:21132119
Calcium
Calcium is a chemical element belonging to the group of
alkaline earth metals. It has the atomic number 20 and an
Calcium C 147
C
http://dx.doi.org/10.1007/978-3-540-29807-6_2611http://dx.doi.org/10.1007/978-3-540-29807-6_2611http://dx.doi.org/10.1007/978-3-540-29807-6_2030http://dx.doi.org/10.1007/978-3-540-29807-6_2030http://dx.doi.org/10.1007/978-3-540-29807-6_2261http://dx.doi.org/10.1007/978-3-540-29807-6_2261http://dx.doi.org/10.1007/978-3-540-29807-6_2261http://dx.doi.org/10.1007/978-3-540-29807-6_2493http://dx.doi.org/10.1007/978-3-540-29807-6_2493http://dx.doi.org/10.1007/978-3-540-29807-6_2493http://dx.doi.org/10.1007/978-3-540-29807-6_2261http://dx.doi.org/10.1007/978-3-540-29807-6_2261http://dx.doi.org/10.1007/978-3-540-29807-6_2030http://dx.doi.org/10.1007/978-3-540-29807-6_2611
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
4/86
atomic mass of 40.078 Da. Ca is named as a macroelement
as the Ca content of humans amounts to about 1 kg, which
is used predominantly for mineralization of bones. Impor-
tant food sources include milk and milk products, nuts,
and vegetables such as broccoli, beans, and collard greens.
Serum Ca is under hormonal control, e.g., calcitriol, cal-
citonin, and parathyroid hormone, and its typical concen-
tration range is between 2.1 and 2.6 mmol/L. There exists
a steep concentration gradient for calcium across the
plasma membrane as the intracellular levels are around
100200 nmmol/L. This gradient is an important prereq-
uisite for calciums role as an important intracellular sig-
naling factor thereby activating many cellular processes
such as myofilament contraction, gating of ion channels,
derangement of cytoskeletal and organelle structures, and
gene expression.
Cross-References Intracellular Signaling
Calmodulin
Calmodulin (CaM) is an abbreviation for calcium-
modulated protein, which is an important calcium-binding
protein ubiquitously expressed in eukaryotic cells. It
contains four so-called EF-hands motifs, which represent
the calcium-binding unit. Upon Ca2+ binding, calmodulinbecomes
an important regulator of several intracellular tar-
gets which are involved in processes such as inflammation,
immune response, metabolism, apoptosis, cell growth, etc.
Canaliculi
Small canals that run through the bone matrix. Fluid flows
through these canals when strain is applied to bone. This
fluid flow is thought to stimulate bone formation.
Cancer
Cancer is a group of diseases characterized by uncontrolled
growth and spread of abnormal cells. If the spread is not
controlled, it can result in death. Cancer is caused by both
external (e.g., tobacco, chemicals, radiation, infectious
organisms, etc.) and internal (e.g., inherited mutations,
hormones, immune conditions, metabolic conditions,
etc.) factors. These casual factors may act together or in
sequence to initiate or promote carcinogenesis.
Cancer Cachexia
A complex metabolic syndrome associated with underly-
ing illness and characterized by skeletal muscle wasting
with or without loss of fat mass. It is associated with
muscle weakness and fatigue and accounts for more
than 20% of all cancer-related deaths. Cancer cachexia is
associated with reduced mobility, increased risk of com-
plications in surgery, impaired response to chemo-/
radiotherapy, and increased psychological distress, leading
to an overall reduction in qualityof life. Cachectic
pertains
to a state of poor health, malnutrition, and weight loss.
Cancer Survivorship
Term given to describe individuals who have been diag-
nosed with cancer from the point of diagnosis through
end of life.
Cancer, Prevention
BRIGIDM. LYNCH, CHRISTINEM. FRIEDENREICH
Department of Population Health Research, Alberta
Health Services Cancer Care, Calgary,
AB, Canada
SynonymsMalignancy;Neoplasm;Tumor
DefinitionCancerdescribes diseases that arise when normal
regen-
erative processes are disrupted by uncontrolled cell growth
or by cellular loss of the ability to undergo apoptosis.
Abnormal cells continue dividing, forming tumors that
can spread to other tissues via invasion or metastasis.
Cancer can originate nearly anywhere in the body. The
most common type of cancer, carcinoma, begins in the
skin or in cells that line or cover internal organs, such as
the lungs or colon. Other forms of cancer include sarcoma
148C Calmodulin
http://dx.doi.org/10.1007/978-3-540-29807-6_267http://dx.doi.org/10.1007/978-3-540-29807-6_267http://dx.doi.org/10.1007/978-3-540-29807-6_4331http://dx.doi.org/10.1007/978-3-540-29807-6_4399http://dx.doi.org/10.1007/978-3-540-29807-6_4565http://dx.doi.org/10.1007/978-3-540-29807-6_2183http://dx.doi.org/10.1007/978-3-540-29807-6_2183http://dx.doi.org/10.1007/978-3-540-29807-6_2183http://dx.doi.org/10.1007/978-3-540-29807-6_4565http://dx.doi.org/10.1007/978-3-540-29807-6_4399http://dx.doi.org/10.1007/978-3-540-29807-6_4331http://dx.doi.org/10.1007/978-3-540-29807-6_267
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
5/86
(arises in bone, cartilage, fat, muscle, or other connective
tissue); myeloma (plasma cells); lymphoma (lymphatic
system); and leukemia (white blood cells).
Each year, an estimated 13 million people are diag-
nosed with cancer, and there are approximately eight
million cancer-related deaths [1]. Breast cancer is the
leading cancer site amongst women (representing 23% of
new diagnoses and 14% of deaths), whilst lung cancer is
the most frequently diagnosed cancer in men (17% of new
diagnoses and 23% of deaths) [1]. Cancer is the leading
cause of death in developed countries, and the second
most common cause of death in developing countries
[1]. The developing world has cancer incidence rates
approximately half those seen in the developed world;
however, overall cancer mortality rates are similar. The
poorer cancer survival rates in developing countries is
likely due to the disease being diagnosed at a later stage
and limited access to appropriate treatments [1].The burden of
disease is expected to increase globally:
by 2030, the number of people with cancer is projected to
double, to more than 20 million new cases [2]. This
increase will be partly attributable to population growth
and aging, but also because of increasing adoption of
a western lifestyle amongst the developing world.
Hence, a disproportionate increase in cancer incidence
will occur within the developing world in years to come.
Pathogenesis
The etiological pathway leading to cancer is a complexone,
involving a series of changes that likely occur over
decades. Various models of carcinogenesis have been
proposed, but generally there are four definable stages:
initiation, promotion, progression, and malignant conver-
sion. Initiation describes the point at which genetic errors
occur spontaneously when cells divide or as a result of
exposure to carcinogens. Cells have a number of mecha-
nisms to repair damaged DNA, but if repair does not
occur, the mutated cells may begin to replicate (promo-
tion), eventually becoming a benign tumor. During
progression, the tumor cells continue to replicate and
additional mutations may occur in genes that regulate
growth and cell function. These changes contribute to
further growth until malignant conversion occurs.
Epidemiological studies have identified a wide range of
environmental and genetic factors associated with
increased cancer risk. Some environmental risk factors,
such as tobacco smoking, alcohol consumption, exposure
to UVradiation, dietary intake, and physical activity
levels,
are modifiable. Hence, a large proportion of common
cancers are potentially preventable. Expert review has con-
cluded that approximately one third of cancer cases are
attributable to tobacco smoking or exposure, and another
third of cases are due to a combination of poor diet,
physical inactivity, and overweight/obesity [2].
Physical activity is thought to reduce cancer risk via
a number of biological mechanisms [3]. These mecha-
nisms may impact different stages of carcinogenesis: for
an in-depth review, see [4]. Key biological mechanisms by
which physical activity may reduce cancer risk include:
AdiposityPhysical activity may reduce body fat, which is
associated
with colon, postmenopausal breast, endometrial, ovarian,
kidney and esophageal cancers, and cancer-related mor-
tality. Adiposityis likely an independent contributor to
cancer risk, and it may facilitate carcinogenesis through
a number of pathways, including increased levels of sex
hormones, insulin resistance, chronic inflammation,
and altered secretion of adipokines.
Endogenous Sex HormonesPhysical activity decreases endogenous
sex hormone levels
and increases circulating sex hormone binding globulin
(SHBG). Exposure to estrogens/androgens is a risk factor
for breast, endometrial, ovarian, and prostate cancers.
SHBG may affect cancer risk by binding to sex hormones,
rendering them biologically inactive.
In premenopausal women, estrogens are predomi-
nantly produced by the ovaries. Very high levels of physical
activity might lower estrogen exposure by delaying onset
ofmenarche, causing menstrual irregularity or reducing the
total number of menstrual cycles. For postmenopausal
women, adipose tissue is the primary source of endogenous
estrogens. Physical activity may decrease adiposity and thus
production of estrogens. In men, the effect of physical
activity on androgen levels is unclear, but dihydroxy-
testerone (a testosterone metabolite) may be increased.
Insulin ResistancePhysical activity improves insulin sensitivity
by increasing
the number and activity of glucose transporters in both
muscle and adipose tissue. In addition, physical activity
may indirectly reduce insulin resistance by promoting
fat loss and preservation of lean body mass. Associations
between insulin levels and colorectal, postmenopausal
breast, pancreatic, and endometrial cancers have been
demonstrated in epidemiological studies. Fasting
glucose levels have been directly associated with pancre-
atic, kidney, liver, endometrial, biliary, and urinary
tract cancers.
Neoplastic cells use glucose for proliferation; there-
fore, hyperglycemia may promote carcinogenesis by
Cancer, Prevention C 149
C
http://dx.doi.org/10.1007/978-3-540-29807-6_2040http://dx.doi.org/10.1007/978-3-540-29807-6_2040http://dx.doi.org/10.1007/978-3-540-29807-6_3025http://dx.doi.org/10.1007/978-3-540-29807-6_3025http://dx.doi.org/10.1007/978-3-540-29807-6_3025http://dx.doi.org/10.1007/978-3-540-29807-6_114http://dx.doi.org/10.1007/978-3-540-29807-6_114http://dx.doi.org/10.1007/978-3-540-29807-6_112http://dx.doi.org/10.1007/978-3-540-29807-6_112http://dx.doi.org/10.1007/978-3-540-29807-6_112http://dx.doi.org/10.1007/978-3-540-29807-6_114http://dx.doi.org/10.1007/978-3-540-29807-6_3025http://dx.doi.org/10.1007/978-3-540-29807-6_3025http://dx.doi.org/10.1007/978-3-540-29807-6_2040
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
6/86
providing an amiable environment for tumor growth.
High insulin levels increase bioavailable insulin-like
growth factor-I, which is involved in cell differentiation,
proliferation, and apoptosis. Decreasing blood insulin
levels also results in increased hepatic synthesis of
SHBG; hence, insulin indirectly increases bioavailability
of endogenous sex hormones.
InflammationPhysical activity may decrease levels of
proinflammatory
factors, namely adipokines (leptin, tumor necrosis
factor-a, interleukin-6) and C-reactive protein, and
increase anti-inflammatory factors (adiponectin).
Chronic inflammation is acknowledged as a risk factor
for most types of cancer.
Obesity represents a low-grade, systematic inflamma-
tory state. It has been hypothesized that perpetual cell
proliferation, microenvironmental changes, and oxidativestress
associated with chronic inflammation could dereg-
ulate normal cell growth to promote malignancy.
Other Possible MechanismsPhysical activity results in improved
pulmonary function,
which may promote expulsion of carcinogenic agents
from the lungs. This mechanism is specific to physical
activity and lung cancer.
Physical activity may increase circulating levels of
25-hydroxyvitamin D, possibly through increased ultravi-
olet radiation exposure as a result of time spent outdoors.In
addition, vitamin D is fat soluble and is readily
stored in adipose tissue. Hence, physical activity may
also increase vitamin D levels by reducing adiposity.
Vitamin D has been associated with colorectal, breast,
and pancreatic cancer risk.
Regular, moderate physical activity may also modulate
the immune systems ability to recognize and repair or
eliminate damaged cells.
It is likely that these proposed mechanisms are inter-
related, and that the relative contribution of each mecha-
nism varies by cancer type. Further research is required to
elicit a clearer understanding of the biological mecha-
nisms involved in the pathways between physical activity
and cancer [3].
Training/Exercise ResponseThe association between physical
activity and cancer has
been systematically reviewed by international agencies [2]
and individual scientists [3,5]. The level of epidemiolog-
ical evidence varies by cancer site. There is convincing
evidence that physical activity decreases the risk of devel-
oping colon cancer, probable evidence for an effect on
breast and endometrial cancer, and possible evidence for
a reduced risk of developing ovarian, prostate, and lung
cancer [3,5].
Epidemiological reviews estimate that physical activity
reduces colon cancer risk by 2025% amongst both men
and women who report participation in the highest level
of physical activity assessed, compared with men and
women who report participating in the lowest level of
physical activity. There is a 25% average breast risk
reduction amongst most physically active women com-
pared to least active women. A stronger physical activity-
associated risk reduction exists amongst postmenopausal
women. For endometrial cancer, reviews have concluded
that physical activity reduces risk by 2030%. There is
consistent evidence for a doseresponse effect for colon
and breast cancer, whereas for endometrial cancer a dose
response effect has been found in approximately half of
all studies.Whilst the evidence is weaker for ovarian,
prostate
and lung cancers, epidemiological reviews estimate that
risk reductions are modest (1020%) for ovarian and
prostate cancer. For lung cancer, there appears to be no
effect of physical activity on risk amongst nonsmokers.
However, there may be substantial risk reductions (20
40%) among smokers. The associations between physical
activity and cancer risk for other sites are either null or
there is insufficient evidence to draw any conclusions
about the link.
It remains unclear what type and dose of physicalactivity are
required to achieve significant cancer risk
reductions. Randomized, controlled trials are required to
provide answers about these areas of uncertainty. None-
theless, there is strong and consistent epidemiological
evidence that physical activity reduces the risk of several
major cancers types. Public health guidelines for physical
activity and cancer prevention recommend 3060 min
of moderate-to-vigorous-intensity physical activity per
day [2].
References1. Jemal A, Bray F, Center MM, Ferlay J, Ward E,
Forman D (2011)
Global cancer statistics. CA Cancer J Clin 61:6990
2. World Cancer Research Fund, The American Institute for
Cancer
Research (2007) Food, nutrition, physical activity, and the
preven-
tion of cancer: a global perspective. American Institute for
Cancer
Research, Washington, DC
3. Friedenreich CM, Neilson HK, Lynch BM (2010) State of the
epidemiological evidence on physical activity and cancer
prevention.
Eur J Cancer 46:25932604
4. Rundle A (2005) Molecular epidemiology of physical activity
and
cancer. Cancer Epidemiol Biomarkers Prev 14:227236
5. Courneya KS, Friedenreich CM (eds) (2011) Recent results in
cancer
research: physical activity and cancer. Springer, Heidelberg
150C Cancer, Prevention
http://dx.doi.org/10.1007/978-3-540-29807-6_3176http://dx.doi.org/10.1007/978-3-540-29807-6_3176http://dx.doi.org/10.1007/978-3-540-29807-6_3176
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
7/86
Cancer, Therapy
LEEW. JONES
Department of Surgery, Duke University Medical Center,
Duke Cancer Institute, Durham, NC, USA
SynonymsExercise and cancer-related side effects; Exercise
and
prognosis after cancer diagnosis
DefinitionThe benefits of physical activity to reduce the
primary and
secondary risk of cardiovascular-related diseases have
been recognized since antiquity. The first formal investi-
gation was not until the early 1950s when James Morris
and colleagues reported that occupational exercise wasassociated
with substantial reductions in coronary heart
disease in the seminal London Busmen study [1]. This
pioneering work led to extensive epidemiological investi-
gation of the association between both occupational
and leisure-time exercises and the risk of cardiovascular
disease by numerous research groups. As a result of the
burgeoning evidence, in 1995, the American College of
Sports Medicine and Centers for Disease Control
published the first prescription guidelines to encourage
increased participation in exercise in Americans of all ages
for health promotion and disease prevention [2]. Over thepast 15
years, physical activity guidelines have been
published for secondary prevention of numerous chronic
conditions, including type II diabetes, chronic obstructive
pulmonary disease, heart failure, and heart transplant
recipients [3].
The putative relationship between exercise and
cancerwas not formally recognized until 2002 wherein
the American Cancer Society recommended regular
exercise to reduce the risk of breast, colon, and several
other forms of cancer. In contrast, investigation of the
role
of exercise following a diagnosis of cancer has, until
recently, received scant attention. The precise reasons forthis
are not known but likely reflect the prevailing dogma
that a cancer diagnosis and associated therapeutic man-
agement preclude participation in and benefit from phys-
ical activity. The reversal of interest in exercise results
from
the alignment of several factors including recognition of
cancer survivorshipas a major public health concern,
a stronger evidence base, and strong interest of cancer
patients themselves in pursuing adjunct approaches to
optimize recovery and longevity. In the past decade, how-
ever, exerciseoncology research has become increasingly
recognized as a legitimate and important field of research
in cancer management [4]. This review will provide an
overview of the putative evidence supporting the role of
exercise across the cancer survivorship continuum (i.e.,
diagnosis to palliation).
CharacteristicsThe use of conventional and novel cytotoxic
therapies
is associated with a diverse range of debilitating physio-
logical (e.g., deconditioning, skeletal muscle atrophy,
cardiac
and pulmonary dysfunction) and psychosocial (e.g., fatigue,
nausea, depression, anxiety) toxicities that impair recovery
and increase susceptibility to concomitant age-related con-
ditions [5]. To address these concerns, in the mid- to late
1980s, researchers initiated the first studies to explore
whether structured physical activity may be an appropriate
intervention to mitigate chemotherapy- and radiation-
induced fatigue and anticipated loss of functional capacityamong
women with early-stage breast cancer. Since this
early work, 80 studies have now examined the safety,
feasibility, and preliminary efficacy of structured physical
activity interventions on a broad range of physiological
and psychosocial outcomes before, during, and/or follow-
ing cancer therapy. Since this early seminal work, the
number of publications has steadily increased over the
past 20 years, with studies becoming progressively more
sophisticated in scope, design, and size to address the
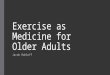
major questions in the field. A chronological timeline of
significant landmarks in exerciseoncology research ispresented
inFig. 1.
Several excellent systematic reviews and meta-analyses
have evaluated the pertinent literature [6]. Findings of
these reviews indicate that structured exercise training is
a safe and well-tolerated intervention associated with
favorable improvements in cancer-related symptoms and
functional outcomes both during and following the com-
pletion of adjuvant therapy. To summarize, the majority of
studies were conducted in women with early breast cancer,
with fewer studies in nonsmall-cell lung cancer (NSCLC),
hematologic malignancies, or mixed cancer populations.
Exercise modality consisted of aerobic training alone,
resistance training alone, or the combination of aerobic
and resistance training prescribed at a moderatevigorous
intensity (5075% of baseline maximum heart rate or
cardiorespiratory fitness), three sessions or more per
week, for 1060 min per exercise session. The length of
the exercise training ranged from 2 to 24 weeks. Overall,
exercise was associated with significant improvements in
muscular strength, cardiorespiratory fitness, functional
quality of life (QOL), fatigue, anxiety, and self-esteem.
Few adverse events (AEs) were observed. It was concluded
Cancer, Therapy C 151
C
http://dx.doi.org/10.1007/978-3-540-29807-6_4185http://dx.doi.org/10.1007/978-3-540-29807-6_4192http://dx.doi.org/10.1007/978-3-540-29807-6_4192http://dx.doi.org/10.1007/978-3-540-29807-6_2183http://dx.doi.org/10.1007/978-3-540-29807-6_2183http://dx.doi.org/10.1007/978-3-540-29807-6_2186http://dx.doi.org/10.1007/978-3-540-29807-6_2186http://dx.doi.org/10.1007/978-3-540-29807-6_2222http://dx.doi.org/10.1007/978-3-540-29807-6_2222http://dx.doi.org/10.1007/978-3-540-29807-6_2222http://dx.doi.org/10.1007/978-3-540-29807-6_2186http://dx.doi.org/10.1007/978-3-540-29807-6_2183http://dx.doi.org/10.1007/978-3-540-29807-6_4192http://dx.doi.org/10.1007/978-3-540-29807-6_4192http://dx.doi.org/10.1007/978-3-540-29807-6_4185
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
8/86
that exercise is a beneficial adjunct therapy both during
and following the completion of adjuvant therapy in adult
cancer patients, with low incidence of AEs [6].
To further clarify this issue, Jones et al. [7] conducted
a meta-analysis to determine the effects of supervised
exercise training on cardiorespiratory fitness, including
only those studies employing a randomized controlleddesign and
direct measurement of peak oxygen consump-
tion (VO2peak), the gold standard assessment of cardiore-
spiratory fitness. Cardiorespiratory fitness is determined
by the integrative capacity of the cardiopulmonary system
(i.e., pulmonarycardiacvascularskeletal muscle axis) to
deliver oxygen from the atmosphere to muscle mitochon-
dria. Cardiorespiratory fitness is one of the most powerful
predictors of cardiovascular and all-cause mortality in
healthy adults as well as those with cardiovascular disease
(CVD) even after controlling for traditional CVD risk
factors.
Jones et al. [7] only identified a total of six studies thatmet
eligibility criteria involving a total of 571 adult cancer
patients (n= 344, exercise; n= 227, usual-care control).
Pooled data indicated that exercise training was associated
with a statistically significant increase in VO2peak(WMD = 2.91
mLkg1min1; 95% CI, 1.184.64) withminimal adverse events, although
significant heterogene-
ity was evident in this estimate (I2 = 87%). It was con-
cluded that the effect of exercise on VO2peakis promising
but the current evidence base is emergent with many
fundamental questions (e.g., optimal prescription, timing,
and setting of exercise; effects of exercise on tumor biol-
ogy; and therapeutic efficacy) remaining to be addressed.
In the following sections, we review the efficacy of
exercise training in specific areas across the cancer survi-
vorship continuum (i.e., presurgery, postsurgery during
adjuvant therapy, survivorship (following the completion
of primary adjuvant therapy), and palliation), with a viewtoward
areas requiring future research.
Clinical Relevance
Exercise Therapy Prior to Surgical ResectionSurgery is the most
common form of cancer therapy
for patients with solid tumors. Pulmonary resection is
the treatment of choice for a variety of disorders, includ-
ing non-small cell lung cancer and selected cases of
oligometastatic disease (sarcoma, colorectal cancer, mela-
noma, etc.), and involves removal of a substantial portion
of lung parenchyma that can negatively impact VO2peak.
Inaddition, the majority of lung cancer patients also present
with several significant concomitant comorbid diseases.
The extent of surgery, together with comorbid disease,
significantly complicates the treatment process, and peri-
operative and postoperative complications are common.
In order to evaluate complication risk, cancer surgeons
often assess VO2peakto determine preoperative physiologic
status of operable candidates. VO2peakis strongly inversely
associated with surgical complication rate in NSCLC
patients. Given this, an important question is whether
1986 2001 2002 2003 2005
Jones et al. [11] investigates the interaction between exercise
and chemotherapy efficacy in a
mouse model of breast cancer
Holmes et al. [13] reports that self-reported regular exercise
is
associated with substantial
reductions in breast-cancer specific and all-cause mortality
2007 2008 2009
First study toinvestigate thefeasibility andeffects of
exercise
training in
patients withcancer [30]
Kolden et al. [28]investigates theeffects of thecombination
of
aerobic andresistance training
First randomized trial is launched
by the National Cancer Institute of
Canada to investigate the effects
of exercise on disease-free
survival in patients with operable
colon cancer following the
completion of adjuvant therapy [30]
Segal et al. [27] reports theeffects of aerobic training in
women undergoingchemotherapy for operablein the Journal of
Clinical
Oncology
The American Cancer Society
convenes a group of expertsto create exerciserecommendations for
cancerpatients in CA: A Cancer
Journal for Clinicians [29]
First studies to comparethe effects of differenttypes of
exercise in
patients with cancer [10]
The benefit of exercise onmortality in colon cancermay be
influenced bytumor molecular
expression of p27 [14]
Cancer, Therapy. Fig. 1 Exerciseoncology research timeline
152C Cancer, Therapy
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
9/86
exercise training prior to surgical resection can improve
VO2peakand, in turn, lower surgical complications.
To date, two studies have addressed the initial feasibil-
ity, tolerability, and potential efficacy of presurgical
exercise-based rehabilitation in patients diagnosed with
NSCLC. In the first study, Jones et al. [8] examined the
efficacy of presurgical aerobic training on VO2peakamong
20 patients with suspected NSCLC. Mean VO2peakincreased by 2.4
mLkg1min1 from baseline to
presurgery. Exploratory analyses indicated that
presurgical VO2peak decreased postsurgery but did not
decrease beyond baseline values. In the second study,
Bobbio et al. [9] reported that short-term exercise-
based pulmonary rehabilitation increased VO2peak by
2.8 mL kg1min1 prior to pulmonary resection in
12 NSCLC patients with chronic obstructive disease.
Larger randomized trials investigating the efficacy of exer-
cise training on surgical complications and postsurgicalrecovery
in cancer patients appear warranted.
Exercise Therapy During Adjuvant TherapyThe use of anticancer
therapies is associated with unique
and varying degrees of direct and indirect physiological
injury that dramatically reduces patients ability to toler-
ate exercise (i.e., low VO2peak), predisposing them to
morbidity, poor psychosocial functioning, and increase
susceptibility to concomitant age-related conditions [5].
To address these concerns, in mid- to late 1980s,
researchers explored whether structured exercise trainingmay be
an effective intervention to prevent and/or
mitigate adjuvant therapyassociated toxicities and poor
cardiorespiratory fitness among women with early-stage
breast cancer. Since these early studies, approximately
40 studies have been conducted, investigating the safety,
tolerability, and efficacy of structured exercise training
on symptom control and other pertinent outcomes in
patients undergoing cancer therapy. In summary, the
current evidence base provides promising evidence that
exercise training is a well-tolerated and safe adjunct ther-
apy that can mitigate several common treatment-related
side effects among patients undergoing different types of
cytotoxic therapy, including chemotherapy, radiation,
and androgen deprivation therapy (ADT).
In addition to examining symptom control, a question
of significant importance is whether the effects of exercise
are similar among those patients undergoing therapy as
those who have completed therapy. The meta-analysis by
Jones et al. [7] indicated that exercise training was
associ-
ated with superior VO2peak improvements following
adjuvant therapy compared to during adjuvant therapy,
although no study has formally investigated this question.
For example, Courneya et al. [10] found that17 weeks of
aerobic training did not improve VO2peakamong women
receiving anthracycline-containing chemotherapy for
early breast cancer. Similarly, Jones et al. reported that
14 weeks of aerobic training led to negligible improve-
ments in VO2peak
among patients undergoing cisplatin-
based adjuvant chemotherapy for early NSCLC. It is also
important to stress that although exercise training caused
minimal improvements in VO2peak, these effects occurred
against the background of declines in VO2peakin patients
assigned to the control condition; in the study by
Courneya et al., VO2peakdeclined 5% among womenrandomized to
usual-care control. Intriguingly, several
other studies have reported significant improvements in
VO2peakand other pertinent outcomes in patients receiv-
ing other types of conventional cytotoxic therapies, such
as radiation and ADT. These findings suggest that
exercise-induced adaptations in the cardiopulmonarysystem may be
contingent on the type of cytotoxic therapy
being administered.
Another question that has received less attention but is
one of critical importance is whether exercise impacts the
therapeutic efficacy of conventional or novel cytotoxic
agents. Exercise is a potent multifactorial intervention
that influences a wide spectrum of pathways that could
potentially modulate the cytotoxicity of chemotherapeu-
tic agents. Jones et al. [11] investigated the effects of
8 weeks of forced exercise (treadmill running) on the
antitumor efficacy of
doxorubicinin female mice bear-ing human breast cancer
xenografts. Overall, there were
no significant differences on tumor growth between
groups receiving doxorubicin alone versus doxorubicin
plus exercise training (p= 0.33), suggesting that exercise
does not significantly modulate doxorubicin-induced
breast cancer growth inhibition. However, further work
by Jones et al. [12] found that although tumor growth was
comparable between exercised and sedentary animals
bearing orthotopically implanted breast cancer xeno-
grafts, tumors from exercising animals had significantly
improved blood perfusion/vascularization relative to the
sedentary control group, suggesting that aerobic exercise
can significantly increase intratumoral vascularization,
which may normalize the tumor microenvironment
and, in turn, inhibit tumor cell metastatic dissemina-
tionand improve therapeutic efficacy. Future studies are
required to test these intriguing questions.
Exercise Therapy Following the Completionof Adjuvant Therapy
(Survivorship)Improvements in early detection and surveillance
together
with more effective locoregional and systemic therapies
Cancer, Therapy C 153
C
http://dx.doi.org/10.1007/978-3-540-29807-6_2282http://dx.doi.org/10.1007/978-3-540-29807-6_2282http://dx.doi.org/10.1007/978-3-540-29807-6_2306http://dx.doi.org/10.1007/978-3-540-29807-6_2306http://dx.doi.org/10.1007/978-3-540-29807-6_3195http://dx.doi.org/10.1007/978-3-540-29807-6_3195http://dx.doi.org/10.1007/978-3-540-29807-6_2787http://dx.doi.org/10.1007/978-3-540-29807-6_2787http://dx.doi.org/10.1007/978-3-540-29807-6_3151http://dx.doi.org/10.1007/978-3-540-29807-6_3151http://dx.doi.org/10.1007/978-3-540-29807-6_2661http://dx.doi.org/10.1007/978-3-540-29807-6_2661http://dx.doi.org/10.1007/978-3-540-29807-6_2661http://dx.doi.org/10.1007/978-3-540-29807-6_2661http://dx.doi.org/10.1007/978-3-540-29807-6_2661http://dx.doi.org/10.1007/978-3-540-29807-6_3151http://dx.doi.org/10.1007/978-3-540-29807-6_2787http://dx.doi.org/10.1007/978-3-540-29807-6_3195http://dx.doi.org/10.1007/978-3-540-29807-6_2306http://dx.doi.org/10.1007/978-3-540-29807-6_2282
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
10/86
have led to significant survival gains for individuals
diagnosed with early-stage cancer. Indeed, 13 million
Americans who have been diagnosed with cancer are
alive today. However, it is becoming increasingly apparent
that improved outcomes in patients with early stage
disease may come at the price of therapy-induced late
effects. As a result, there has been a significant paradigm
shift toward long-term therapy-associated toxicity and its
resultant effects on morbidity, premature noncancer,
competing causes of mortality, and QOL.
Exercise has emerged as an intervention of central
importance in cancer survivorship, with numerous
research groups examining whether exercise performed
following the completion of therapy can accelerate recov-
ery from the rigors of adjuvant cytotoxic therapy [4].
Similar to during therapy, the current literature base
suggests that exercise is a safe and well-tolerated therapy
associated with significant improvements in certain
phys-iological and psychosocial therapy late effects.
A major goal in exerciseoncology survivorship
research is to determine the optimal exercise prescription
in cancer survivors. The vast majority of studies to date
have investigated the effects of either aerobic training
alone, resistance training alone, or the combination of
aerobic and resistance training following traditional exer-
cise prescription guidelines (35 day week1 at 5075% of
baseline VO2peakfor 1215 weeks) in cancer survivors. As
the field progresses, it will be important to conduct ade-
quately powered studies that identify the optimal
type,intensity, duration, and frequency of exercise training to
improve symptom control in cancer survivors. At least
three ongoing trials are addressing different aspects of
this question in NSCLC, breast, and prostate cancer sur-
vivors. Of particular interest is high-intensity exercise
training. Several recent randomized trials have demon-
strated that high-intensity aerobic training (i.e., 75%
of baseline exercise capacity) causes superior improve-
ments in VO2peakrelative to low- or moderate-intensity
exercise training in patients with or at risk of CVD. How-
ever, there is a dearth of data regarding effects of
exercise
intensity following a cancer diagnosis.
Arguably, one of the most important questions in
exerciseoncology research is to determine whether the
benefits of exercise extend beyond to impact prognosis
following a cancer diagnosis [4,6]. The extant literature
indicates that, in general, regular physical activity is
asso-
ciated with 1561% reduction in the risk of death from
breast or colorectal cancer (Table 1). The association
between physical activity and cancer-specific mortality is
not uniform and appears to vary according to volume
of physical activity and even cancer type. In breast cancer,
the amount of physical activity that was significantly
inversely associated with cancer death ranged from
9 MET-h week1 (brisk walking for 30 min, 5 dayweek1) to 21 MET-h
week1 (brisk walking for
75 min, 5 day week1); in colorectal cancer, the range
was
18 MET-h week1 (brisk walking for 60 min, 5 day
week1) to 27 MET-h week1 (brisk walking for 90 min,5 day week1).
In addition, exploratory analyses suggest
that the effects of physical activity may also differ by
histological subtype and tumor expression of certain
molecular markers. For example, Holmes et al. [13]
reported that 9 MET-h week1 was associated witha relative risk
reduction in mortality of only 9% in
women with estrogen receptor (ER)negative tumors rel-
ative to a mortality reduction of 50% in women with ER-
positive tumors. Meyerhardt et al. [14] reported that the
association between exercise and mortality in patients
with stage IIII colon cancer may depend on p27
status.Specifically, in tumors with loss of p27, the HR for
colon
cancer mortality was 1.40 (95% CI, 0.414.72) for patients
reporting 18 MET-h week1 relative to those reporting
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
11/86
Cancer, Therapy. Table 1 Association between postdiagnosis
physical activity and cancer-specific mortality and all-cause
mortality following a cancer diagnosis
Cancer site/
author N Cohort/setting
Cancer-specific mortality All-cause mortality
Risk
reduction
(HR) Exercise dose
Dose
response
Risk
reduction
(HR)
Exercise
dose
Dose
response
Breast cancer
Holmes
et al. [13]
2,987 Stages IIII; Nurses
health study
0.50a 914.9
METs-h
weekb
No 0.56a 1523.9
METsbNo
Sternfeld
et al. [16]
1,970 Stages IIIIa; Life after
cancer epidemiology
0.69a 3
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
12/86
receiving aggressive combination cytotoxic and support-
ive care therapies. As such, these patients are likely
experiencing more disease-related and treatment-related
toxicities that will modify the exercise response.
A recent systematic review by Lowe et al. [15] identi-
fied a total of six studies investigating the effect of
exercise
training on symptom control in patients with advanced
cancer. In general, all studies reported positive findings,
but overall, methodological quality was poor. There is
currently insufficient evidence for definitive conclusions
regarding the tolerability, safety, or efficacy of exercise
in
cancer patients with advanced disease. Given the poorer
prognosis and elevated treatment toxicity in this setting,
we stress the importance of rigorous AE and safety mon-
itoring in planned exercise studies is comparable to that
required for pharmaceutical intervention trials, in con-
junction with appropriate correlative science components.
Such an approach will ensure the optimal safety andefficacy of
exercise in this unique setting.
SummaryResearch, as well as clinical interest, in the role of
exercise
following a cancer diagnosis has increased dramatically
and is likely to increase even further over the next decade
with the emergence and increasing importance placed on
cancer survivorship. The current evidence base provides
strong but preliminary evidence that exercise training is
a well-tolerated and safe adjunct therapy that can mitigate
several common treatment-related side effects amongpatients
receiving adjuvant therapy for early-stage disease.
Results of these first-generation studies provide a solid
platform to launch second-generation studies that will
extend the scope and application of exerciseoncology
research to address the major unanswered questions in
this emerging field.
AcknowledgementsDr. Jones is supported by NIH CA143254,
CA142566,
CA138634, CA133895, CA125458 and George and Susan
Beischer.
References1. Morris JN, Heady JA, Raffle PA et al (1953)
Coronary heart disease
and physical activity of work. Lancet 265:111120
2. Pate RR, Pratt M, Blair SN et al (1995) Physical activity and
public
health. A recommendation from the Centers for Disease Control
and
Prevention and the American College of Sports Medicine. J Am
Med
Assoc 273:402407
3. Warburton DE, Nicol CW, Bredin SS (2006) Health benefits
of
physical activity: the evidence. Canadian Med Assoc J
174:801809
4. Jones LW, Peppercorn J (2010) Exercise research: early
promise
warrants further investment. Lancet Oncol 11:408410
5. Jones LW, Eves ND, Haykowsky M et al (2009) Exercise
intolerance in
cancer and the role of exercise therapy to reverse dysfunction.
Lancet
Oncol 10:598605
6. Schmitz KH, Courneya KS, Matthews C et al (2010) American
College of Sports Medicine roundtable on exercise guidelines
for
cancer survivors. Med Sci Sports Exerc 42:14091426
7. Jones LW, Liang Y, Pituskin EN et al (2011) Effect of
exercise training
on peak oxygen consumption in patients with cancer: a meta-
analysis. Oncologist 16:112120
8. Jones LW, Eves ND, Peddle CJ et al (2009) Effects of
presurgical
exercise training on systemic inflammatory markers among
patients
with malignant lung lesions. Appl Physiol Nutr Metab
34:197202
9. Bobbio A, Chetta A, Ampollini L et al (2008) Preoperative
pulmo-
nary rehabilitation in patients undergoing lung resection for
non-
small cell lung cancer. Eur J Cardiothorac Surg 33:9598
10. Courneya KS, Segal RJ, Mackey JR et al (2007) Effects of
aerobic
and resistance exercise in breast cancer patients receiving
adjuvant
chemotherapy: a multicenter randomized controlled trial. J
Clin
Oncol 25:43964404
11. Jones LW, Eves ND, Courneya KS et al (2005) Effects of
exercise
training on antitumor efficacy of doxorubicin in
MDA-MB-231breast cancer xenografts. Clin Cancer Res 11:66956698
12. Jones LW, Viglianti BL, Tashjian JA et al (2010) Effect of
aerobic
exercise on tumor physiology in an animal model of human
breast
cancer. J Appl Physiol 108:343348
13. Holmes MD, Chen WY, Feskanich D et al (2005) Physical
activity and
survival after breast cancer diagnosis. J Am Med Assoc
293:24792486
14. Meyerhardt JA, Ogino S, Kirkner GJ et al (2009) Interaction
of
molecular markers and physical activity on mortality in
patients
with colon cancer. Clin Cancer Res 15:59315936
15. Lowe SS, Watanabe SM, Courneya KS (2009) Physical activity
as a
supportive careintervention in palliative cancer patients:a
systematic
review. J Support Oncol 7:2734
16. SternfeldB, Weltzien E, Quesenberry CP Jr et al (2009)
Physical activity
andrisk of recurrence andmortality in breastcancer survivors:
findingsfrom the LACE study. Cancer Epidemiol Biomarkers Prev
18:8795
17. Holick CN, Newcomb PA, Trentham-Dietz A et al (2008)
Physical
activity and survival after diagnosis of invasive breast cancer.
Cancer
Epidemiol Biomarkers Prev 17:379386
18. Irwin ML, Smith AW, McTiernan A et al (2008) Influence of
pre- and
postdiagnosis physical activity on mortality in breast cancer
survi-
vors: the health, eating, activity, and lifestyle study. J Clin
Oncol
26:39583964
19. Pierce JP, Stefanick ML, Flatt SW et al (2007) Greater
survival after
breast cancer in physically active women with high
vegetable-fruit
intake regardless of obesity. J Clin Oncol 25:23452351
20. Dal Maso L, Zucchetto A, Talamini R (2008) Effect of
obesity
and other lifestyle factors on mortality in women with breast
cancer.
Int J Cancer 123:21889421. Meyerhardt JA, Heseltine D,
Niedzwiecki D et al (2006) Impact of
physical activity on cancer recurrence and survival in patients
with
stage III colon cancer: findings from CALGB 89803. J Clin
Oncol
24:35353541
22. Meyerhardt JA, Giovannucci EL, Holmes MD et al (2006)
Physical
activity and survival after colorectal cancer diagnosis. J Clin
Oncol
24:35273534
23. Meyerhardt JA, Giovannucci EL, Ogino S et al (2009) Physical
activity
and male colorectal cancer survival. Arch Intern Med
169:21022108
24. Kenfield SA, Stampfer MJ, Giovannucci E et al (2011)
Physical activ-
ity and survival after prostate cancer diagnosis in the
health
professionals follow-up study. J Clin Oncol 29:726732
156C Cancer, Therapy
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
13/86
25. Moorman PG, Jones LW, Akushevich L et al (2011)
Recreational
physical activity and ovarian cancer risk and survival. Ann
Epidemiol
21:178187
26. Ruden E, Reardon DA, Coan AD et al (2011) Exercise
behavior,
functional capacity, and survival in adults with malignant
recurrent
glioma. J Clin Oncol 29(2):29182923
27. Segal R, Evans W, Johnson D et al (2001) Structured
exercise
improves physical functioning in women with stages I and II
breast
cancer: results of a randomized controlled trial. J Clin
Oncol
19:657665
28. Kolden GG, Strauman TJ, Ward A et al (2002) A pilot study of
group
exercise training (GET) for women with primary breast
cancer:
feasibility and health benefits. Psycho Oncol 11:447456
29. Brown JK, Byers T, Doyle C et al (2003) Nutrition and
physical
activity during and after cancer treatment: an American
Cancer
Society guide for informed choices. CA Cancer J Clin
53:268291
30. Courneya KS, Booth CM, Gill S et al (2008) The colon health
and
life-long exercise change trial: a randomized trial of the
national
cancer institute of Canada clinical trials group. Curr Oncol
15:279285
Capillarization
Angiogenesis
Capillary Hematocrit
The ratio of red blood cells (RBCs) to plasma volume
within the capillaries at any given time. The number ofRBCs
within the capillaries that lie adjacent to the
myocytes determines, in part, the O2 diffusion capacity
(DO2).
Carbohydrate
Nutrition
Carbohydrate Loading
A. N. BOSCH
Human Biology, University of Cape Town MRC Research
Unit for Exercise Science and Sports Medicine, Sports
Science Institute of South Africa, Newlands, South Africa
SynonymsGlycogen loading;Glycogen super-compensation
DefinitionCarbohydrate loading is the use of a dietary technique
used
primarily by endurance athletes before participation in
prolonged events such as the marathon. It involves ingestion
of high-carbohydrate foods or drinks for 13 days before
competition to increase muscle glycogen stores.
Mechanism of ActionIn 1967, the introduction of the needle
biopsy technique
for the sampling of muscle tissue in exercise physiology
studies provided important new data on the relationships
between diet, muscle glycogen concentration, and fatigue
during prolonged exercise.
Muscle Glycogen ConcentrationsUsing the biopsy technique,
initial studies determined that
the concentration of glycogen in the leg muscles ofuntrained
people eating a normal diet varies from approx-
imately 80 to 120 mmol/kg of wet muscle (ww), whereas
average muscle glycogen concentrations of athletes who
ingest a diet high in carbohydrate and are in training are
somewhat higher, around 130 mmol/kg ww [1]. Values as
high as 140200 mmol/kg ww are attained in trained
athletes who have not exercised for 2448 h and who
have consumed a high-carbohydrate diet.
Muscle Glycogen Concentrations, Diet, and
Exercise PerformanceDiet can affect both muscle glycogen content
and exerciseperformance. Possibly the best known studies that
con-
tributed to the development of the dietary practice that
was to become known as carbohydrate loading are those
of Ahlborg et al. [2] and Bergstrom et al. [3] in which
muscle glycogen concentrations were manipulated
through various combinations of diet and exercise. In
these studies, muscle glycogen concentration was found
to average 97 mmol/kg ww at the start of exercise. Subjects
then cycled to exhaustion at 75% of VO2maxon a cycle
ergometer, which averaged 114 min. Following this initial
exercise bout, for the next 3 days a high fat-protein dietwas
ingested, after which muscle glycogen concentrations
had decreased to 35 mmol/kg ww and average exercise
time to exhaustion was reduced to 57 min. The dietary
regimen was then changed to a high carbohydrate one for
the next 7 days. With this regimen, mean muscle glycogen
concentrations increased to 184 mmol/kg ww and exercise
time increased to 167 min. Thus, it became apparent that
initial glycogen concentration influenced exercise time to
exhaustion, and that muscle glycogen concentration could
be influenced by dietary manipulation. It was not long
Carbohydrate Loading C 157
C
http://dx.doi.org/10.1007/978-3-540-29807-6_23http://dx.doi.org/10.1007/978-3-540-29807-6_23http://dx.doi.org/10.1007/978-3-540-29807-6_147http://dx.doi.org/10.1007/978-3-540-29807-6_147http://dx.doi.org/10.1007/978-3-540-29807-6_4246http://dx.doi.org/10.1007/978-3-540-29807-6_4247http://dx.doi.org/10.1007/978-3-540-29807-6_4247http://dx.doi.org/10.1007/978-3-540-29807-6_4246http://dx.doi.org/10.1007/978-3-540-29807-6_147http://dx.doi.org/10.1007/978-3-540-29807-6_23
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
14/86
before this procedure of first depleting muscle glycogen
stores by an exercise bout followed by 3 days of a diet low
in carbohydrate (high fat-protein diet), followed subse-
quently by eating a large amount of carbohydrate (600 g
of carbohydrate daily), was used by endurance athletes in
an effort to enhance performance. This became known as
the carbohydrate loading diet, although the period of
high carbohydrate intake became reduced from 7 to 3 days
when used by athletes.
Importantly, this original work was done using rela-
tively untrained people in the experiments. Subsequently,
it was demonstrated that the depletion phase of eating
only protein and fat is unnecessary in well-trained athletes
[4,5]. Simply eating a high-carbohydrate diet for 3 days
(500600 g/day; 10 g/kg body weight/day), combined
with a reduction in training, was found to result in similar
amounts of glycogen being stored to that obtained
when the original loading regimen was followed. This isbecause
glycogen synthase, one of the enzymes involved
in muscle glycogen synthesis, is activated by the carbohy-
drate and glycogen depletion regimen in untrained
people; in trained individuals, however, glycogen synthase
is already maximally activated as a result of daily training
and no further activation occurs following a period of low
carbohydrate intake.
More recently, it has been shown that in highly trained
athletes even 3 days of carbohydrate loading is longer than
needed to maximize muscle glycogen stores. By ingesting
10 g/kg body weight/day of carbohydrate, maximal muscleglycogen
concentrations can be attained within 24 h [6,7].
Carbohydrate loading with high glycemic index car-
bohydrate foods rather than low glycemic index foods
has been found to have no effect on performance in
a 10-km performance run, after an initial run for 1 h at
70% VO2max[8]. Unfortunately, muscle glycogen concen-
tration was not measured in this study, and the total
exercise performed may not have been sufficient to deplete
muscle glycogen stores, and therefore, it cannot be
assumed that the high glycemic index foods did not result
in higher initial muscle glycogen stores, based only there
being no differences in performance in this particular
study. The effect of glycemic index on the rate of muscle
glycogen storage remains to be resolved. It should be
noted, however, that in the study which showed that
maximal muscle glycogen stores could be attained within
24 h, a high glycemic index carbohydrate was ingested to
carbohydrate load.
Once a high muscle glycogen concentration has been
attained by carbohydrate loading, it is possible for an
athlete to maintain these high concentrations without
continued loading. Specifically, the muscle glycogen
concentration remains elevated for 3 [9] to 5 days [10],
provided only moderate intensity exercise of approxi-
mately only 20 min duration is performed during
that time.
Following the findings of Bergstrom et al. [3] of
increased dietary carbohydrate resulting in increased mus-
cle glycogen stores and an apparently related increase in
exercise time to exhaustion, a number of papers were
published which examined in greater detail the relation-
ship between diet, muscle glycogen content, and the pos-
sibility of improved exercise performance. These studies
showed that fatigue in endurance exercise appeared to
consistently coincide with low muscle glycogen concen-
trations, and it was therefore concluded that exhaustion
during prolonged exercise was due to muscle glycogen
depletion. Therefore, starting exercise with raised muscle
glycogen levels by prior carbohydrate loading was con-
firmed as being advantageous. In some respects, however,the
coincidence between muscle glycogen depletion and
exhaustion during prolonged exercise may be an over
simplification, as in many of the studies that examined
the effect of carbohydrate loading on performance, blood
glucose concentration was either not measured or not
carefully considered when results were analyzed. It appears
that in some studies which attributed fatigue to depleted
muscle glycogen stores, lowered blood glucose concentra-
tion could also have accounted for the fatigue experienced
by the subjects. Nevertheless, the majority of studies have
shown that starting exercise with high muscle
glycogenconcentration delays the onset of fatigue.
Although, in some cases, low blood glucose concen-
trations together with low muscle glycogen concentration
make interpretation of the cause of fatigue difficult, the
importance of muscle glycogen concentrations alone was
demonstrated in a study in which subjects started exercise
with either high or low muscle glycogen content as a result
of ingesting a diet either low in carbohydrate or after
having carbohydrate loaded for 4 days prior to the exper-
iment. As expected, time to fatigue was longer in the
athletes with high initial muscle glycogen content. At
exhaustion, glucose was infused to restore plasma glucose
to pre-exercise levels. Interestingly, although this elimi-
nated symptoms of hypoglycemia, it did not improve
performance time, suggesting that muscle glycogen
depletion specifically, and not hypoglycemia was respon-
sible for exhaustion in these subjects. In contrast,
Coyle et al. [11] showed that exercise could be continued
even when muscle glycogen content was low, provided
that the blood glucose concentration remained high.
Cyclists ingested either a glucose polymer solution or
water placebo while cycling at 70% of VO2max. Those
158C Carbohydrate Loading
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
15/86
subjects ingesting the carbohydrate solution were able to
exercise for an hour longer than subjects ingesting the
placebo, even though the muscle glycogen concentrations
of the carbohydrate ingesting subjects during the final
hour were as low as those of the subjects who could not
continue and who were exhausted. Thus, it was concluded
that it could not have been muscle glycogen depletion that
stopped the subjects from continuing to exercise, but
rather an inadequate supply of plasma glucose for oxida-
tion. The final conclusion of the study was that as long as
the muscle was provided with sufficient glucose to oxidize,
exercise could be continued when normally this would not
be possible because hypoglycemia terminated exercise pre-
maturely. However, if the data are examined carefully, it
becomes apparent that the muscle glycogen concentra-
tions at exhaustion in this study did not reach the very
low concentrations that are usually associated with
exhaustion. Values were around 40 mmol/kg ww, whereasit has
previously been reported that 1728 mmol/kg ww is
the concentration consistent with exhaustion [12]. Thus,
it is likely that the ergogenic effect of the carbohydrate
was
mainly due to the maintenance of euglycemia, and there-
fore the concept of muscle glycogen being implicated in
exhaustion remains.
One of the few field studies that have investigated the
theory that glycogen depletion is an important element in
the cause of fatigue is that of Karlsson and Saltin [12].
Using well-trained subjects, they found that after follow-
ing a carbohydrate-loading regimen, subjects ran a fastertime in
a 30-km road race than when eating a normal diet.
Of particular interest was the finding that loading did not
result in a faster initial running speed. Rather, it allowed
the athletes to maintain their initial speed for longer
before slowing down. The time in the race at which the
runners slowed down correlated with their starting muscle
glycogen concentrations.
Although there have been many studies that have
concentrated on the effect of high muscle glycogen con-
centration subsequent to carbohydrate loading on
endurance exercise performance at moderate intensity
(70% VO2max), there have also been studies which have
shown that even if exercise intensity is low, high muscle
glycogen content at the start of exercise is important. For
example, muscle glycogen depletion has been implicated
in exhaustion in exercise performed as low as 43% of
VO2max. At the other extreme, it has also been shown
that exercise at very high exercise intensities (greater
than 80% VO2max) may also be affected by muscle glyco-
gen content at the start of exercise. Specifically, an
increase
in time to exhaustion after carbohydrate loading and
decreased time to exhaustion after glycogen depletion
compared to exercise which commenced with normal
muscle glycogen levels, has been shown when exercise
was performed at 100% of VO2max. This was despite the
short duration of exercise performed at such a high
intensity.
Despite the majority of studies showing a positive
effect on exercise performance as a result of starting exer-
cise with high muscle glycogen content after carbohydrate
loading, there have been some that have shown no effect.
For example, in one study, there was no difference in
running time to fatigue (77 min) at 7580% of VO2maxbetween
carbohydrate-loaded and non-loaded groups
of well-trained runners. Glycogen concentrations at
exhaustion, however, were too high in both groups to
be considered a possible cause of fatigue (125 and
100 mmol/kg ww, respectively). Similarly, a field trial
over a distance of 21 km showed no improvement in
running performance as a result of prior carbohydrateloading.
The failure to show an improvement over this
distance is most likely due to muscle glycogen stores not
becoming depleted before the end of the 21-km distance.
Other studies, however, have shown an effect over
a distance of 25 km. Thus, although there is some
conflicting evidence, generally it appears that carbohy-
drate loading only becomes important when exercise
duration is so long, or of such high intensity that muscle
glycogen becomes depleted during the event. It is also
important to remember that fatigue can occur due to
factors other than muscle glycogen depletion or lowblood glucose
concentration. For example, Costill et al.
[13] found that trained runners may became fatigued
even though muscle glycogen concentrations at exhaus-
tion were 63 mmol/kg ww in the vastus lateralis and
86 mmol/kg ww in the soleus.
In summary, carbohydrate loading increases muscle
glycogen concentration, which has generally been shown
to enhance endurance performance, and in some studies,
to enhance shorter duration exercise performed at
a higher intensity.
References1. Sahlin K, Katz A, Broberg S (1990) Tricarboxylic
acid cycle interme-
diates in human muscle during prolonged exercise. Am J
Physiol
259(5 Pt 1):C834C841
2. Ahlborg B, Bergstrom J, Brohult J et al (1967) Human muscle
glyco-
gen content and capacity for prolonged exercise after different
diets.
Forvarsmedicin 3:8599
3. Bergstrom J, Hermansen L, Hultman E, Saltin B (1967) Diet,
muscle
glycogen and physical performance. Acta Physiol Scand 71(2):
140150
4. Sherman WM, Costill DL, Fink WJ, Miller JM (1981) Effect
of
exercise-diet manipulation on muscle glycogen and its
subsequent
utilization during performance. Int J Sports Med 2(2):114118
Carbohydrate Loading C 159
C
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
16/86
5. Costill DL, Sherman WM, Fink WJ et al (1981) The role of
dietary
carbohydrates in muscle glycogen resynthesis after strenuous
run-
ning. Am J Clin Nutr 34(9):18311836
6. Bussau VA, Fairchild TJ, Rao A et al (2002) Carbohydrate
loading in
human muscle: an improved 1 day protocol. Eur J Appl Physiol
87(3):290295
7. Fairchild TJ, Fletcher S, Steele P et al (2002) Rapid
carbohydrate
loading aftera shortbout of near maximal-intensity exercise.Med
Sci
Sports Exerc 34(6):980986
8. Chen Y, Wong SH, Xu X et al (2008) Effect of CHO loading
patterns
on running performance. Int J Sports Med 29(7):598606
9. Goforth HW Jr, Arnall DA, Bennett BL, Law PG (1997)
Persistence of
supercompensated muscle glycogen in trained subjects after
carbo-
hydrate loading. J Appl Physiol 82(1):342347
10. Arnall DA, Nelson AG, Quigley J et al (2007)
Supercompensated
glycogen loads persist 5 days in resting trained cyclists. Eur J
Appl
Physiol 99(3):251256
11. Coyle EF, Coggan AR, Hemmert MK, Ivy JL (1986) Muscle
glycogen
utilization during prolonged strenuous exercise when fed
carbohy-
drate. J Appl Physiol 61(1):165172
12. Karlsson J, Saltin B (1971) Diet, muscle glycogen, and
enduranceperformance. J Appl Physiol 31(2):203206
13. Costill DL, Sparks K, Gregor R, Turner C (1971) Muscle
glycogen
utilization during exhaustive running. J Appl Physiol
31(3):353356
Carbon Dioxide Output
Gas Exchange, Alveolar
Cardiac Arrhythmias
ALESSANDRO BLANDINO, ELISABETTA TOSO, FIORENZO GAITA
Cardiology Division, Department of Internal Medicine,
San Giovanni Battista Hospital, University of Turin,
Turin, Italy
SynonymsAbnormal cardiac electrical activity; Disturbance of
the
heartbeat;Rhythm disorder
DefinitionThe term arrhythmia comes from the ancient Greek
a-rhuthmos) and identifies a loss of normal heart activity.
Cardiac arrhythmias can be classified into bradyarrhythmias
(when heart rate is < than 60 beats for minute) or
Tachyarrhythmias (when heart rate is >than 100 beat
for minute), that may arise from supraventricular
regions or ventricles. Bradyarrhythmias include sinus bra-
dycardia, wandering pacemaker, sinus pause, and
atrioventricular blocks. Supraventricular tachyarrhyth-
mias include premature ectopic beats, AV nodal reentrant
tachycardia (AVNRT), orthodromic AV reentrant tachy-
cardia (AVRT) due to an Accessory Pathway, ectopic
atrial tachycardia, atrial fibrillation (AF), and atrial
flutter
(AF1). Ventricular tachyarrhythmias include premature
ectopic beats, non-sustained ventricular tachycardia,
idio-ventricular accelerated rhythm, benign idiopathic
ventricular tachycardia, and malignant ventricular
tachycardia, such as sustained ventricular tachycardia,
polymorphic ventricular tachycardia, torsades de pointes,
and ventricular fibrillation.
Characteristics and Eligibility for SportsPractice
Bradyarrhythmias
In the trained athlete, sinus bradycardia (defined assinus heart
rate < 60 beats per minute) and sinus pauses
are frequent and are generally benign conditions, second-
ary to high vagal tone and reduced sympathetic tone
(Bradyarrhythmias). These conditions are generally
asymptomatic and do not affect maximum heart rate attain-
ment. Anyway, if symptomatic, 24-h Holter monitoring and
exercise testing are recommended, plus echocardiography
whether structural heart disease is suspected.
High vagal tone and reduced adrenergic tone are also
responsible for the high prevalence of atrioventricular
(AV) blocks in athletes. In AV block, atrial activation
isconducted to the ventricles with a delay, or it is not
conducted at all, during a period when the AV conduction
pathway (AV node or His-Purkinje system) is not expected
to be refractory. On the basis of the electrocardiographic
criteria, AV block is classified as first, second, or third
degree, and depending on the anatomical point at which
the conduction of the activation wave front is impaired, it
is described as supra-Hisian, intra-Hisian, or infra-Hisian.
In the athletes, the most common AV blocks seen are
as follows: first-degree AV block (each atrial stimulus
is conducted to the ventricles with a prolonged PR
interval more than 200 ms) and second-degree AV block
type I (Wenckebach or Mobitz I, defined as progressively
increased PR interval until an atrial stimulus is not
conducted to the ventricles). AV blocks typically occur
during sleep or at rest and resolve during exercise, showing
the supra-hisian nature of conduction impairment.
If asymptomatic, with no cardiac disease, and with
resolution of block during exercise, the athlete is eligible
for all sports. In case of severe bradycardia (heart rate
3 s, and when symptomatic, it
is necessary to interrupt any sports activity and further
160C Carbon Dioxide Output
http://dx.doi.org/10.1007/978-3-540-29807-6_83http://dx.doi.org/10.1007/978-3-540-29807-6_83http://dx.doi.org/10.1007/978-3-540-29807-6_4011http://dx.doi.org/10.1007/978-3-540-29807-6_4158http://dx.doi.org/10.1007/978-3-540-29807-6_4158http://dx.doi.org/10.1007/978-3-540-29807-6_4508http://dx.doi.org/10.1007/978-3-540-29807-6_3108http://dx.doi.org/10.1007/978-3-540-29807-6_3108http://dx.doi.org/10.1007/978-3-540-29807-6_2004http://dx.doi.org/10.1007/978-3-540-29807-6_2004http://dx.doi.org/10.1007/978-3-540-29807-6_2173http://dx.doi.org/10.1007/978-3-540-29807-6_2173http://dx.doi.org/10.1007/978-3-540-29807-6_2173http://dx.doi.org/10.1007/978-3-540-29807-6_2004http://dx.doi.org/10.1007/978-3-540-29807-6_3108http://dx.doi.org/10.1007/978-3-540-29807-6_4508http://dx.doi.org/10.1007/978-3-540-29807-6_4158http://dx.doi.org/10.1007/978-3-540-29807-6_4158http://dx.doi.org/10.1007/978-3-540-29807-6_4011http://dx.doi.org/10.1007/978-3-540-29807-6_83
-
7/27/2019 Encyclopedia of Exercise Medicine in Health and
Disease (2012) - C
17/86
diagnostic monitoring (24-h Holter monitoring and
exercise testing) be recommended. At least after 3 months
when the symptoms are absent, physical effort can be
restarted with yearly clinical controls.
TachyarrhythmiasAs previously described, tachyarrhythmias are
classifiedinto supraventricular (when they originate from atria
or
AV junction) and ventricular (when they originate from
myocardium under the AV junction).
Supraventicular Arrhythmias
Premature Supraventricular ComplexSupraventricular premature
ectopic beats (PSVCs) are
premature activation of the atria or AV junction arising
from a site other than the sinus node. They are a common
finding in many individuals, including athletes, and theymay be
asymptomatic or cause mild symptoms such as
skipping sensation or palpitations; they are often single
and isolated, but may be frequent or occur in a bigeminal
pattern. In predisposed individuals, PSVCs may trigger sup-
raventricular and, less commonly, ventricular arrhythmias.
In the absence of structural heart disease, thyroid dysfunc-
tion, initiation of sustained arrhythmias and moderate/
severe symptoms, no further evaluation or therapy is
required. If the athlete is asymptomatic, with no cardiac
disease, eligibility is for all sports, without further
yearly
clinical assessment.
Atrioventricular Nodal ReciprocatingTachycardiaAtrioventricular
nodal reciprocating tachycardia (AVNRT)
is the most common form of paroxysmal supraventricular
tachycardia. It is more prevalent in females, is associated
with palpitations, dizziness, and neck pulsations, and
rarely
is associated with structural heart disease.
Rates of tachycardia are often between 140 and
250 per minute. The reentrant circuit comprises the
compact AV node and frequently a perinodal atrial tissue.
AVNRT involves reciprocation between two functionally
and anatomically distinct pathways (fast and slow
pathways). The fast pathway appears to be located near
the His bundle at the Kochs triangle apex, whereas
the slow pathway extends infero-posterior to the compact
AV-node tissue and stretches along the septal margin of
the tricuspid annulus at the level of the coronary sinus.
During typical AVNRT, the fast pathway serves as the
retrograde limb of the circuit, whereas the slow pathway is
the anterograde limb (slowfast AV-node reentry). After
conduction through the slow pathway to the His bundle
and ventricle, brisk conduction back to the atrium
over the fast pathway results in inscription of the shorter
duration (40 ms) P wave during or close to the
QRS complex (less than or equal to 70 ms) often with
a pseudo-r in V1. Less commonly (approximately 510%),
the tachycardia circuit is reversed such that conduction
proceeds anterogradely over the fast pathway and retro-
gradely over the slow pathway (fastslow AV-node reentry,
or atypical AVNRT) producing a long R-P tachycardia.
The P wave, negative in leads III and augmented vector
foot (aVF), is inscribed prior to the QRS. Infrequently,
both limbs of the tachycardia circuit are composed of
slowly conducting tissue (slowslow AV-node reentry),
and the P wave is inscribed after the QRS, producing an
RP interval more tha