Embed Size (px)
Citation preview
ClinicalRadiology(1980) 31, 121-135 0009-9260/80/00060121502.00 © 1980 Royal txouege of Radiologists
,End-points in Cancer Therapy' The Glyn Evans Memorial Lecture of the Royal College of Radiologists*
ARTHUR JONES
Department of Radiotherapy, St Bartholomew's Hospital and Medical College, London
Mr President, Ladies and Gentleman, Clinicians would I think be reluctant to accept,
with Helmholtz, that 'all science is measurement': nevertheless the remarkable advances in medicine of the last 30 years have depended in great measure on quantitation. While the individual disciplines which make up oncology can be as precise in methodology as any others in clinical science, the ultimate assess- ments of therapy have in the nature of things often been less substantial. The most sophisticated of clinical trials can only be as good as its data, its end- points and the perspective of their interpretation. A look over the nature and diversity of some of the end- points adopted by different disciplines may therefore be timely.
I would like to thank you, Mr President, and the Council of the Royal College of Radiologists most sincerely for the honour of being invited to give this Glyn Evans Memorial Lecture, and for the privilege of discussing this topic before a multidisciplinary audience at Cambridge. May I also take this oppor- tunity of thanking my friends in various branches of oncology who by their stimulating discussions have made this review possible?
The subject would I believe have appealed to Glyn Evans, who by his vision and achievement did so much to further the treatment of patients with cancer. He not only built up the outstanding Radio- therapy Centre at Velindre Hospital in Cardiff, but in a wider sphere he was the first medical adviser of Tenovus, which has had such a beneficial influence on cancer research in many centres. Glyn Evans was essentially foward4ooking, and he would be showing his delight at the progress which is now being achieved on such a broad front.
Survival statistics in cancer are under discussion, not to say under fire, from both epidemiologists and clinicians, who are in fact each looking at extremes of a diversity of problems. In the community at large mortality rates and incidence rates of cancer are highly correlated, while neither is related to the actual survival rates. Engstrom and Austin (1977) have pointed out that survival rates should not be
*Delivered at Cambridge, 16 September 1978.
10
used as the sole or primary measurement of progress in national cancer control because factors unrelated to the efficacy of treatment play an important part in determining those rates and their trends. A telling instance is the improved survival reported by clinicians for most forms of leukaemia, while the global survival for all forms of leukaemia may in fact have remained constant because of increasing incidence of the highly fatal forms; and the converse situation seems to hold for carcinoma of the prostate.
From the clinical point of view, for the individual 'tumour species' of defined type and stage the time- honoured survival rate, say at five years, provides very incomplete information even when 'corrected' for age and so on; for it fails to distinguish between early and late deaths, and it wastes information on patients followed for less than the whole period. There is no doubt that a 'life table' is the most accurate descrip- tion of a set of data on the times to death of a group of patients. This gives of course an estimate of the proportion who will still be alive at different times after entry, calculated with due allowance for in- complete follow-up: essentially it characterises the survival pattern of the series. It requires regular determination of the status of all patients at risk, and it permits use of all data; its major disadvantages are (a) the requirement of a large study sample in order to provide reasonable confidence limits as the analysis proceeds and the number of individuals at risk diminishes, and (b) that patients may also die from disease not directly related to neoplasia or from causes induced by therapy. Nevertheless, correctly used and interpreted, the Kaplan-Meier method is the most useful available for series characterisation, and two points of difficulty related to misuse and misapprehension have therefore to be mentioned. As the method uses probability theory and the term 'projected' or 'expected' five-year disease-free survival is employed, this engenders scepticism in the minds of clinicians as to how many patients had actually survived for the five years; and this actual versus actuarial controversy demands that the survival by the 'direct method', presenting the results at the end of a period, should also be given at the same time.
122 CLINICAL R A D I O L O G Y
The second difficulty arises from its use in a small series and too early in the course of a disease, thereby spuriously bolstering the results of a new method of treatment. A similar situation may follow publication of a too-early analysis of a major trial, to show a temporary difference which is later smoothed out by larger numbers, but which in the interim may have an unconscious bearing on practice outside the trial. That this can occur also with the direct method is exemplified in the data of the excellently conducted CRC breast study which compares survival and recurrence after mastectomy, both with and without postoperative X-ray therapy. Murray (1974), giving a preliminary report in the British Journal o f Surgery, was careful to point out that at four years too few patients had been followed for too short a time to give meaningful results; but he also mentioned that the divergence of the graphs showed a difference approaching statistical significance, suggesting 'that the occurrence of distant metastases is higher in the group treated with irradiation'. Of course, with time the apparent difference disappeared and the recent report (Leiberman, 1978) showed no difference in survival but a useful reduction in local recurrence in those irradiated.
Changes in diagnostic criteria and in the detail of delineation and characterisation, as well as in suppor- tive medical care, have been shown to alter signifi- cantly the apparent natural history of many types of neoplastic disease. For instance, in Hodgkin's disease lymphopenia and immunological anergy at presen- tation were formerly regarded as bad prognostic features, but have lost this significance in modern staging; and an initial thrombocytopenia in acute myelogenous leukaemia has been robbed of its former dire import by the advent of platelet transfusion. So that despite the arguments put forward by Gehan and Freireich (1974) for the use of historical controls, once a pilot study has been completed, and unless large differences in responses are to be expected, there is rarely any alternative to a well-designed randomised clinical trial; and the publication last year of the MRC Report by Peto et aL (1976, 1977) is a landmark in the analysis of such trials.
CONCEPTS OF CURE
The idea of 'cure' in cancer was for generations linked to arbitrary and f'mite survival periods, often 5 or 10 years, but some 20 years ago Russell (1958) of Manchester, modifying an idea of Greenwood (1926), enunciated a new definition: 'We can speak of cure when in time - probably a decade or so after treatment - there remains a group of disease-free survivors whose progressive death rate from all causes
is similar to that of a normal population of the same sex and age constitution'. This concept Was elaborated by Easson and Russell (1963) and by Easson (1966) particularly in relation to Hodgkins disease; and it has had such an influence on oneo. logical thought that by 1977 Carter (1977), a medical oncologist, wrote 'by "cure" is meant that the life expectancy of the treated cancer patient is the same as the "normal" life expectancy - specifically the same as that in a matched cohort of the general population'.
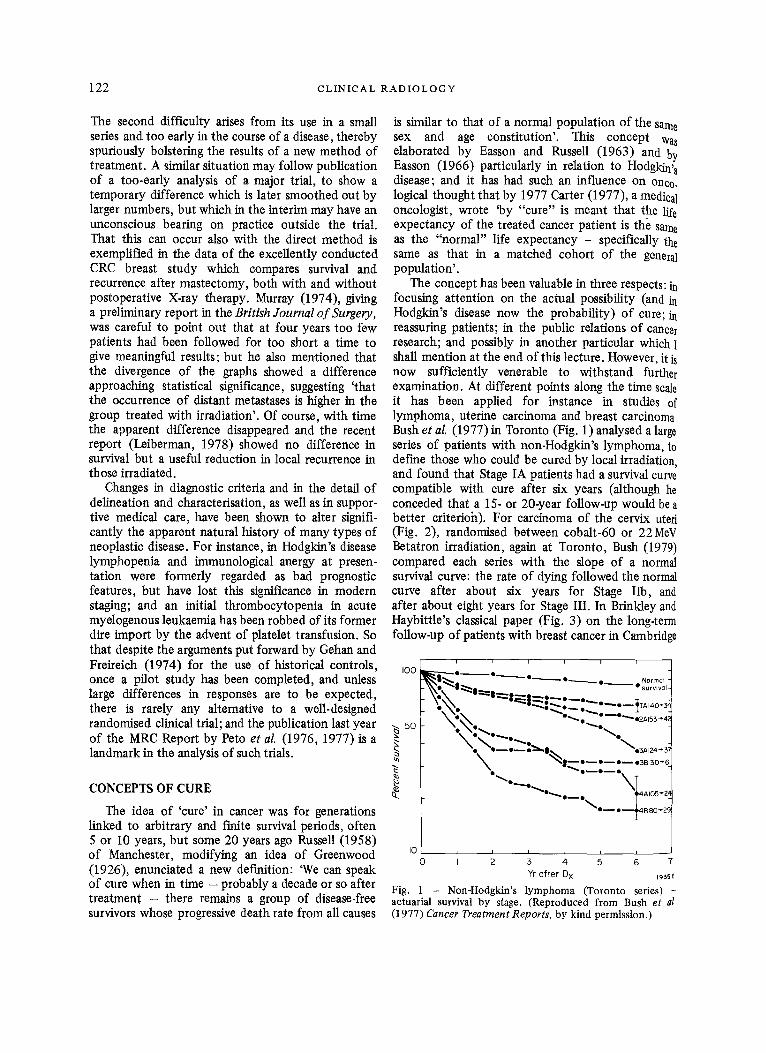
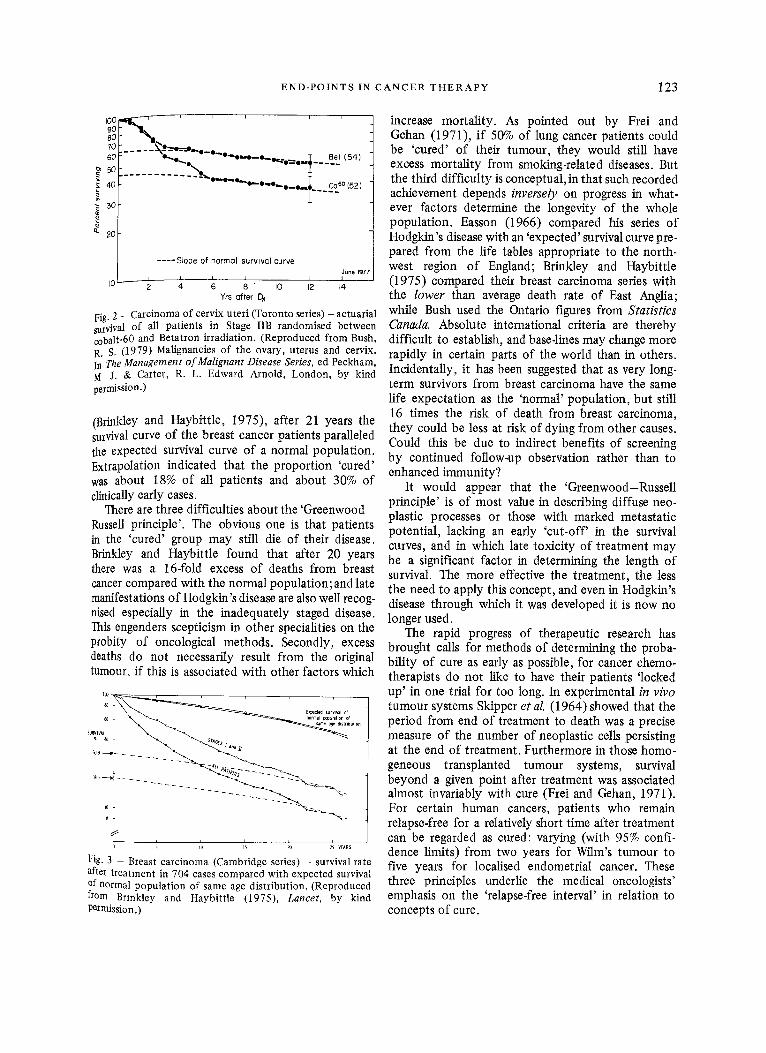
The concept has been valuable in three respects: in focusing attention on the actual possibility (and in Hodgkin's disease now the probability) of cure; in reassuring patients; in the public relations of cancer research; and possibly in another particular which I shall mention at the end of this lecture. However, it is now sufficiently venerable to withstand further examination. At different points along the time scale it has been applied for instance in studies of lymphoma, uterine carcinoma and breast carcinoma Bush et al. (1977) in Toronto (Fig. 1) analysed a large series of patients with non-Hodgkin's lymphoma, to define those who could be cured by local irradiation, and found that Stage IA patients had a survival curve compatible with cure after six years (although he conceded that a 15- or 20-year follow-up would be a better criterioh). For carcinoma of the cervix uteri (Fig. 2), randomised between cobalt-60 or 22MeV Betatron irradiation, again at Toronto, Bush (1979) compared each series with the slope of a normal survival curve: the rate of dying followed the normal curve after about six years for Stage lib, and after about eight years for Stage III. In Brinldey and Haybitfle's classical paper (Fig. 3) on the long-term follow-up of patients with breast cancer in Cambridge
I00 • e ~ o ~ ' - - ° ' ~ o N°rmal I
l-\~a, " ~ | ~ . ~ • survival.
I \ " . ' , . " ~ o "--''"..z+,+3+,+; % ~ ~O ~ O
I - \ " % . . . . . . . . +,+ +o++
I ~ i - - o - - i n
Io i u n i i
0 I 2 3 4 5 6 7
Yr a f te r Dx 1935E
Fig. 1 - Non-Hodgkin's lymphoma (Toronto series) actuarial survival by stage. (Reproduced from Bush et al (1977) Cancer Treatment Reports, by kind permission.)
E N D - P O I N T S IN C A N C E R T H E R A P Y 123
100 9O 8O 7O 6O 50 40
m 30
~- zo
I0
e L Q i i i i i
; . . . . . ( 5 o ,
. . . . . . . . . . . . . ~'°"e-"e"°- ' - -o- , . . t ._ . co 6° (52)
. . . . Slope o f no rmQI surVWQI c u r v e June 197~
~ l I I I I / I 2 4 6 8 " I0 12 14
Yrs efter Dx
Fig. 2 - Carcinoma of cervix uteri (Toronto series) - actuarial survival of all patients in Stage IIB randomised between cobalt-60 and Betatron irradiation. (Reproduced from Bush, R. S. (1979) Malignancies of the ovary, uterus and cervix. In The Management of Malignant Disease Series, ed Peckham, M J. & Carter, R. L. Edward Arnold, London, by kind permission.)
(Brinkley and Haybittle, 1975), after 21 years the survival curve of the breast cancer patients paralleled the expected survival curve of a normal population. Extrapolation indicated that the proportion 'cured' was about 18% of all patients and about 30% of clinically early cases.
There are three difficulties about the 'Greenwood- Russell principle'. The obvious one is that patients in the 'cured' group may still die of their disease. Brinkley and Haybittle found that after 20 years there was a 16-fold excess of deaths from breast cancer compared with the normal population;and late manifestations of Hodgkin's disease are also well recog- nised especially in the inadequately staged disease. This engenders scepticism in other specialities on the probity of oncological methods. Secondly, excess deaths do not necessarily result from the original tumour, if this is associated with other factors which
100- , , , , ,
60 ~ r m | / ~pu)atlon ef . m s age dlsttlbUt on
SURVIVAL
1o
s
i i i 5 11) 115 20 215 Y~AR5
Fig. - Breast carcinoma (Cambridge series) - survival rate afte treatment in 704 cases compared with expected survival of normal population of same age distribution. (Reproduced from Brmkley and Haybittle (1975), Lancet, by kind permission.)
increase mortality. As pointed out by Frei and Gehan (1971), if 50% of lung cancer patients could be 'cured' of their tumour, they would still have excess mortality from smoking-related diseases. But the third difficulty is conceptual, in that such recorded achievement depends inversely on progress in what- ever factors determine the longevity of the whole population. Easson (1966) compared his series of Hodgkin's disease with an 'expected' survival curve pre- pared from the life tables appropriate to the north- west region of England; Brinkley and Haybittle (1975) compared their breast carcinoma series with the lower than average death rate of East Anglia; while Bush used the Ontario figures from Statistics Canada. Absolute international criteria are thereby difficult to establish, and base4ines may change more rapidly in certain parts of the world than in others. Incidentally, it has been suggested that as very long- term survivors from breast carcinoma have the same life expectation as the 'normal' population, but still 16 times the risk of death from breast carcinoma, they could be less at risk of dying from other causes. Could this be due to indirect benefits of screening by continued follow-up observation rather than to enhanced immunity?
It would appear that the 'Greenwood-Russell principle' is of most value in describing diffuse neo- plastic processes or those with marked metastatic potential, lacking an early 'cut-off' in the survival curves, and in which late toxicity of treatment may be a significant factor in determining the length of survival. The more effective the treatment, the less the need to apply this concept, and even in Hodgkin's disease through which it was developed it is now no longer used.
The rapid progress of therapeutic research has brought calls for methods of determining the proba- bility of cure as early as possible, for cancer chemo- therapists do not like to have their patients 'locked up' in one trial for too long. In experimental in vivo tumour systems Skipper et al. (1964) showed that the period from end of treatment to death was a precise measure of the number of neoplastic cells persisting at the end of treatment. Furthermore in those homo- geneous transplanted tumour systems, survival beyond a given point after treatment was associated almost invariably with cure (Frei and Gehan, 1971). For certain human cancers, patients who remain relapse-free for a relatively short time after treatment can be regarded as cured: varying (with 95% confi- dence limits) from two years for Wilm's turnout to five years for localised endometrial cancer. These three principles underlie the medical oncologists' emphasis on the 'relapse-free interval' in relation to concepts of cure.
124 C L I N I C A L R A D I O L O G Y
5O
25 Lu
14 zoo 4bo 6~o s~o i~oo i;oo f~oo t&o i~oo z~oo z~oo
DAYS
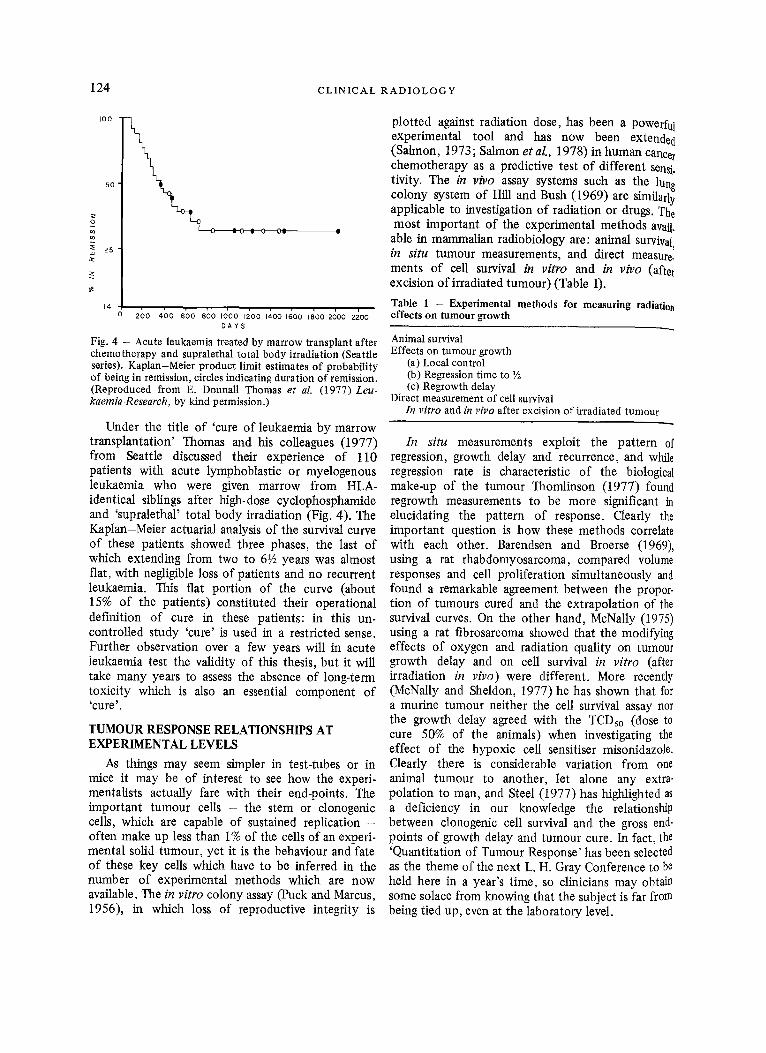
Fig. 4 - Acute leukaemia treated by marrow transplant after chemotherapy and supralethal total body irradiation (Seattle series). Kaplan-Meier product limit estimates of probability of being in remission, circles indicating duration of remission. (Reproduced from E. DonnaU Thomas et al. (1977) Leu- kaemia-Research, by kind permission.)
Under the title of 'cure of leukaemia by marrow transplantation' Thomas and his colleagues (1977) from Seattle discussed their experience of 110 patients with acute lymphoblastic or myelogenous leukaemia who were given marrow from HLA- identical siblings after high-dose cyclophosphamide and 'supralethal' total body irradiation (Fig. 4). The Kaplan-Meier actuarial analysis of the survival curve of these patients showed three phases, the last of which extending from two to 6½ years was almost flat, with negligible loss of patients and no recurrent leukaemia. This flat portion of the curve (about 15% of the patients) constituted their operational definition of cure in these patients: in this un- controlled study 'cure' is used in a restricted sense. Further observation over a few years will in acute leukaemia test the validity of this thesis, but it will take many years to assess the absence of long-term toxicity which is also an essential component of ~ c u r e ~.
TUMOUR RESPONSE RELATIONSHIPS AT EXPERIMENTAL LEVELS
As things may seem simpler in test-tubes or in mice it may be of interest to see how the experi- mentalists actually fare with their end-points. The important tumour cells - the stem or clonogenic cells, which are capable of sustained replication -- often make up less than 1% of the cells of an experi- mental solid tumour, yet it is the behaviour and fate of these key cells which have to be inferred in the number of experimental methods which are now available. The in vitro colony assay (Puck and Marcus, 1956), in which loss of reproductive integrity is
plotted against radiation dose, has been a powerful experimental tool and has now been extended (Salmon, 1973; Salmon etal. , 1978) in human cancer chemotherapy as a predictive test of different sensi. tivity. The in vivo assay systems such as the lung colony system of Hill and Bush (1969) are similarly applicable to investigation of radiation or drugs. The most important of the experimental methods avail.
able in mammalian radiobiology are: animal survival, in situ tumour measurements, and direct measure. ments of cell survival in vitro and in vivo (after excision of irradiated tumour) (Table 1).
Table 1 - Experimental methods for measuring radiation effects on tumour growth
Animal survival Effects on turnout growth
(a) Local control (b) Regression time to ½ (c) Regrowth delay
Direct measurement of cell survival In vitro and in vivo after excision of irradiated tumour
In situ measurements exploit the pattern of regression, growth delay and recurrence, and while regression rate is characteristic of the biological make-up of the tumour Thomlinson (1977) found regrowth measurements to be more significant in elucidating the pattern of response. Clearly the important question is how these methods correlate with each other. Barendsen and Broerse (1969), using a rat rhabdomyosarcoma, compared volume responses and cell proliferation simultaneously and found a remarkable agreement between the proper. tion of tumours cured and the extrapolation of the survival curves. On the other hand, McNaUy (1975) using a rat fibrosarcoma showed that the modifying effects of oxygen and radiation quality on tumour growth delay and on cell survival in vitro (after irradiation in vivo) were different. More recently (McNally and Sheldon, 1977) he has shown that for a murine tumour neither the cell survival assay nor the growth delay agreed with the TCDso (dose to cure 50% of the animals) when investigating the effect of the hypoxic cell sensitiser misonidazole. Clearly there is considerable variation from one animal tumour to another, let alone any extra- polation to man, and Steel (1977) has highlighted as a deficiency in our knowledge the relationship between clonogenic cell survival and the gross end- points of growth delay and tumour cure. In fact, the 'Quantitation of Tumour Response' has been selected as the theme of the next L. H. Gray Conference to be held here in a year's time, so clinicians may obtain some solace from knowing that the subject is far from being tied up, even at the laboratory level.
E N D - P O I N T S I N C A N C E R T H E R A P Y 125
TIlE CLINICAL EVALUATION OF TUMOUR RESPONSE
The objective evaluation of tumour response in an i~dividual patient depends of course on clinical observations, imaging techniques, and biochemical determinations, and these must be viewed in context to obtain a clinically meaningful appraisal. Apart from the very special instances of intra-ocular tumours, those of the skin (both primary and meta- static) provide opportunities for the greatest accuracy of physical measurement, as shown by the elegance of Thomlinson's studies (Thomlinson, 1977)based on r~any thousands of caliper readings; and even these reveal that what is being measured is usually the clinical tip of a pathological iceberg. Squamous carcinoma of the upper respiratory tract is also accessible, and when turnouts are small a fairly high degree of accuracy is possible in their measurement. Once the carcinomas have become large and diffusely infiltrating there is however little precision in the assessment, and it is well to note that many studies of chemotherapy are of necessity based on such material. If responses of accessible lymph node masses are difficult to quantitate, how much more difficult is the situation with abdominal and pelvic nodes.
When we clinically observe ovarian cancer and infiltrating carcinoma of the colon and rectum the accuracy of physical measurement is often least, and these again are two important diseases which are the subject of many clinical trials.
In this context, Moertel of the Mayo Clinic (Moertel and Hanley, 1976) has reported on the effect of measuring error on the results of therapeutic trials in advanced cancer. Sixteen experienced oncolo- gists each measured 12 simulated tumour masses (some of which were identical in size); the lesions varied from about 2 to 15 cm in diameter and were covered with foam rubber ½-1½in thick to mimic subcutaneous tissue or the abdominal wall. The oncologists were asked to measure each sphere using the technique usually used in practice. They found the 'placebo response rate' in unchanged masses to be 25% if a 25% regression was employed, and 7% if a 50% criterion was taken. Moertel points out that when an oncologist is measuring a deep-seated irregular mass through the muscle guarding of an uncomfortable patient, the error of his measurement will undoubtedly be far greater than that recorded in this study. 'Certainly under real life circumstances a 25% regression must be considered meaningless, and even a 50% regression is questionable.'
Such critical approaches to determination of tumour size should not of course be construed as observational nihilism, for it is important that clinical observations should be pursued to the limit of
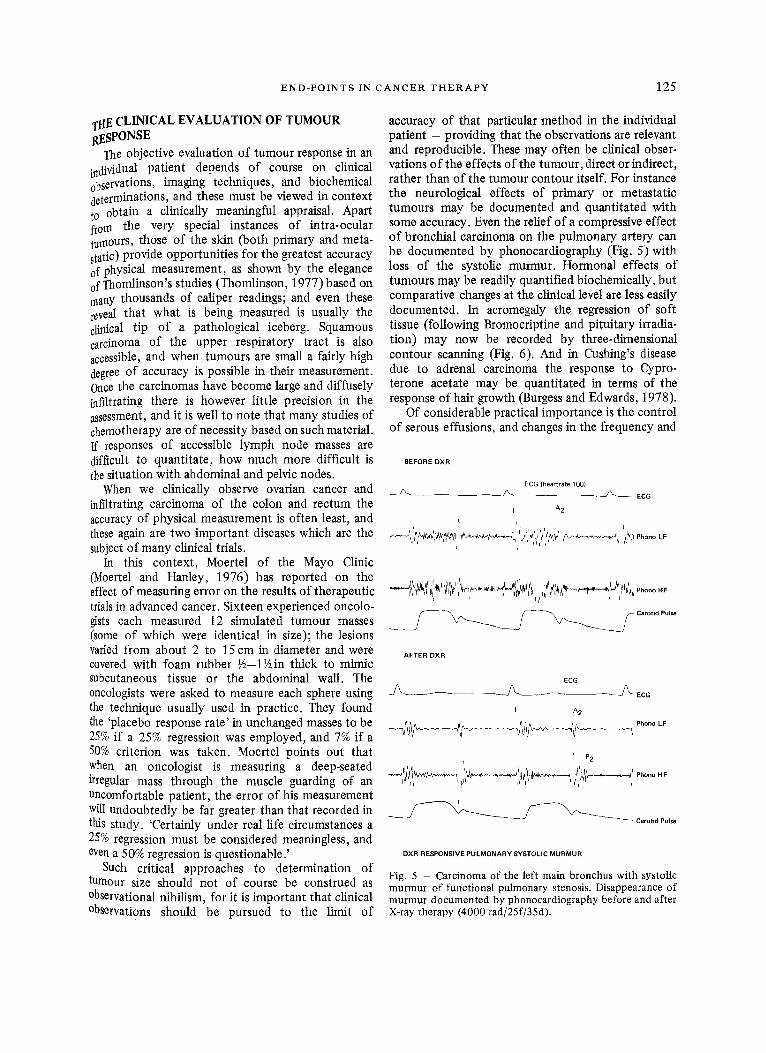
accuracy of that particular method in the individual patient - providing that the observations are relevant and reproducible. These may often be clinical obser- vations of the effects of the turnout, direct or indirect, rather than of the tumour contour itself. For instance the neurological effects of primary or metastatic tumours may be documented and quantitated with some accuracy. Even the relief of a compressive effect of bronchial carcinoma on the pulmonary artery can be documented by phonocardiography (Fig. 5)with loss of the systolic murmur. Hormonal effects of tumours may be readily quantified biochemically, but comparative changes at the clinical level are less easily documented. In acromegaly the regression of soft tissue (following Bromocriptine and pituitary irradia- tion) may now be recorded by three-dimensional contour scanning (Fig. 6). And in Cushing's disease due to adrenal carcinoma the response to Cypro- terone acetate may be quantitated in terms of the response of hair growth (Burgess and Edwards, 1978).
Of considerable practical importance is the control of serous effusions, and changes in the frequency and
BEFORE D X R
ECG (heartrate 100)
~ - - ~ ECG I A 2
L i
. . . . . !L&tL'l"ri/I,~ l JlrhJJr'z, . . . . . ,I,,. ~ L j ! r r . u ' ~ r tr~,g ,L.. ~ .i~r~* L L ' ,
I t i • ,t r ii '
A F T E R O X R
ECG
J ~ ~ -J~ EcG I A 2
~l~__~.~_.4~15~__~,~. . '~P~°n°'F
' P2 x
~ Carottd Pulse
D X R R E S P O N S I V E P U L M O N A R Y S Y S T O L I C M U R M U R
Fig. 5 - Carcinoma of the left main bronchus with systolic murmur of functional pulmonary stenosis. Disappearance of murmur documented by phonocardiography before and after X-ray therapy (4000 rad/25f/35d).
126 CLINICAL RADIOLOGY
B E F O R E T R E A T M E N T
711. 63c.,-
B R O M O C R I P T I N E F O R T H R E E M O N T H S
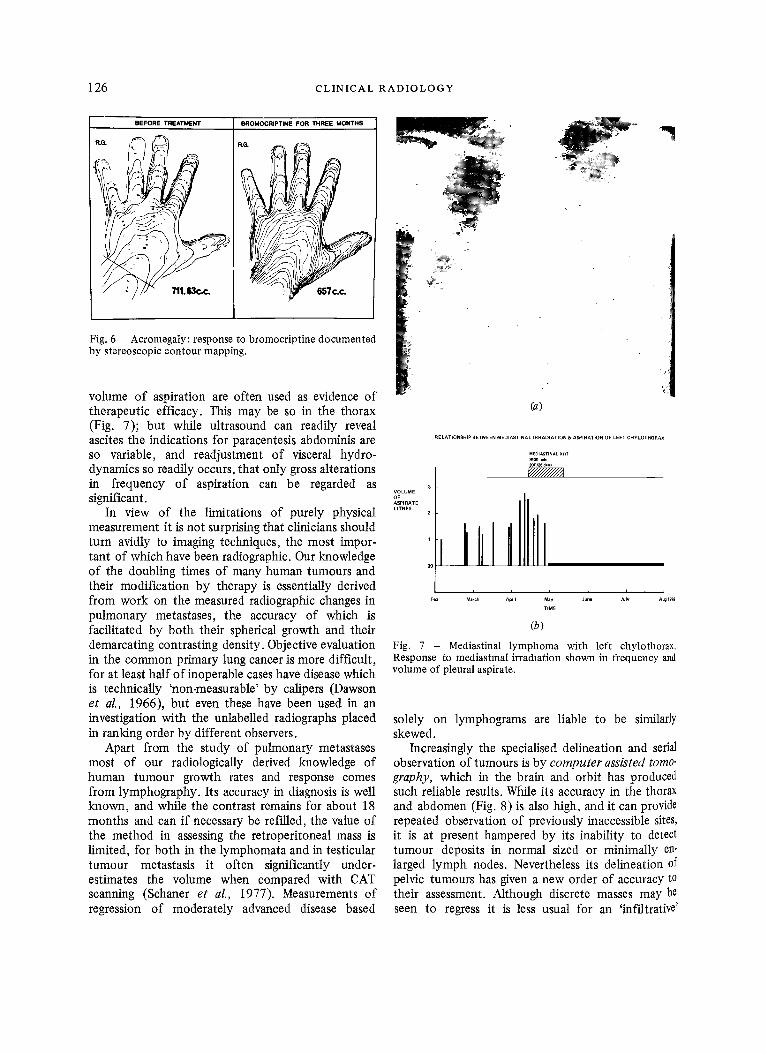
Fig. 6 Acromegaly: response to bromocriptine documented by stereoscopic contour mapping.
volume of aspiration are often used as evidence of therapeutic efficacy. This may be so in the thorax (Fig. 7); but while ultrasound can readily reveal ascites the indications for paracentesis abdominis are so variable, and readjustment of visceral hydro- dynamics so readily occurs, that only gross alterations in frequency of aspiration can be regarded as significant.
In view of the limitations of purely physical measurement it is not surprising that clinicians should turn avidly to imaging techniques, the most impor- tant of which have been radiographic. Our knowledge of the doubling times of many human tumours and their modification by therapy is essentially derived from work on the measured radiographic changes in pulmonary metastases, the accuracy of which is facilitated by both their spherical growth and their demarcating contrasting density. Objective evaluation in the common primary lung cancer is more difficult, for at least half of inoperable cases have disease which is technically 'non-measurable' by calipers (Dawson et al., 1966), but even these have been used in an investigation with the unlabelled radiographs placed in ranking order by different observers.
Apart from the study of pulmonary metastases most of our radiologically derived knowledge of human tumour growth rates and response comes from lymphography. Its accuracy in diagnosis is well known, and while the contrast remains for about 18 months and can if necessary be refilled, the value of the method in assessing the retroperitoneal mass is limited, for both in the lymphomata and in testicular tumour metastasis it often significantly under- estimates the volume when compared with CAT scanning (Schaner et al., 1977). Measurements of regression of moderately advanced disease based
k (a)
RE LATIONSHIP BETWEEN MEDIASTINAL IRRADIATION & ASPIRATION OF LEFT CHYLOTHORAX
MEDIASTINA L XRT
3 VOLUME
ASPIRATE LITRES 2
]llllll i i i I i i
Feb March Apt I May Ju~ July Aug 1970
TIME
(b)
Fig. 7 - Mediastinal lymphoma with left chylothorax. Response to mediastmal irradiation shown in frequency and volume of pleural aspirate.
solely on lymphograms are liable to be similarly skewed.
Increasingly the specialised delineation and serial observation of tumours is by computer assisted tomo- graphy, which in the brain and orbit has produced such reliable results. While its accuracy in the thorax and abdomen (Fig. 8) is also high, .and it can provide repeated observation of previously inaccessible sites, it is at present hampered by its inability to detect tumour deposits in normal sized or minimally en- larged lymph nodes. Nevertheless its delineation of pelvic tumours has given a new order of accuracy to their assessment. Although discrete masses may be seen to regress it is less usual for an 'infiltrative'
E N D - P O I N T S IN C A N C E R T H E R A P Y 127
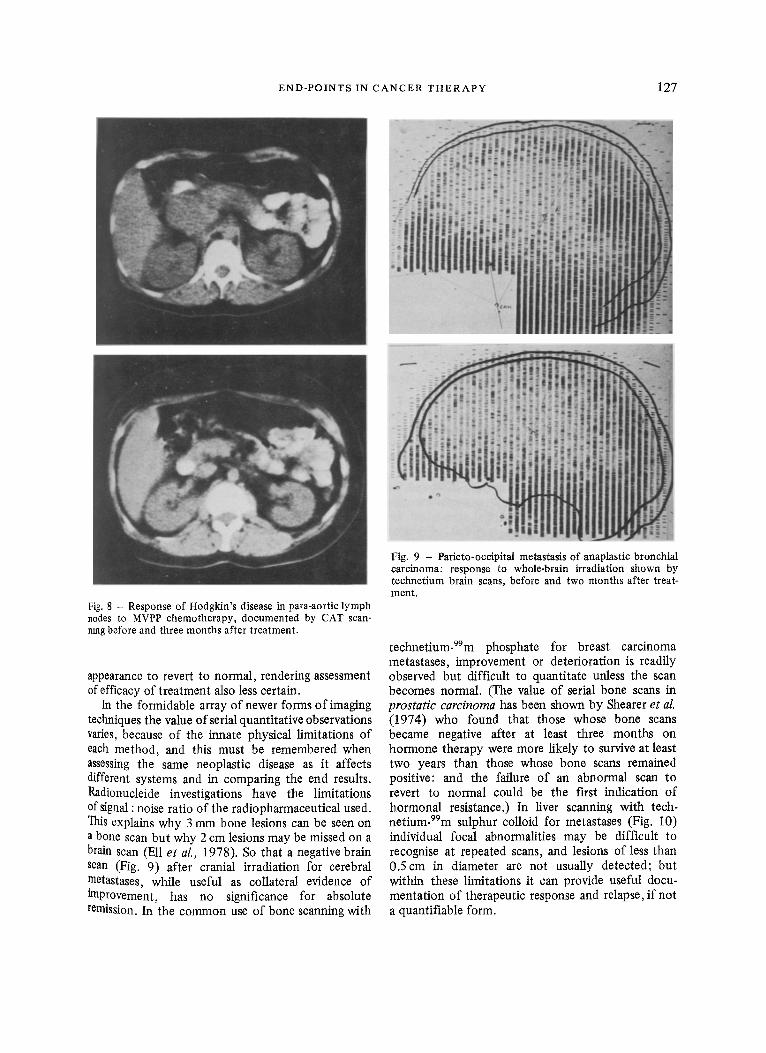
Fig. 8 - Response of Hodgkir~'s disease in para-aortic lymph nodes to MVPP chemotherapy, documented by CAT scan- nmg before and three months after treatment.
appearance to revert to normal, rendering assessment of efficacy of treatment also less certain.
In the formidable array of newer forms of imaging techniques the value of serial quantitative observations varies, because of the innate physical limitations of each method, and this must be remembered when assessing the same neoplastic disease as it affects different systems and in comparing the end results. Radionucleide investigations have the limitations of signal : noise ratio of the radiopharmaceutical used. This explains why 3 mm bone lesions can be seen on a bone scan but why 2 cm lesions may be missed on a brain scan (Ell et al., 1978). So that a negative brain scan (Fig. 9) after cranial irradiation for cerebral .metastases, while useful as collateral evidence of tmprovement, has no significance for absolute remission. In the common use of bone scanning with
Fig. 9 - Parieto-occipital metastasis of anaplastic bronchial carcinoma: response to whole-brain irradiation shown by technetium brain scans, before and two months after treat- ment.
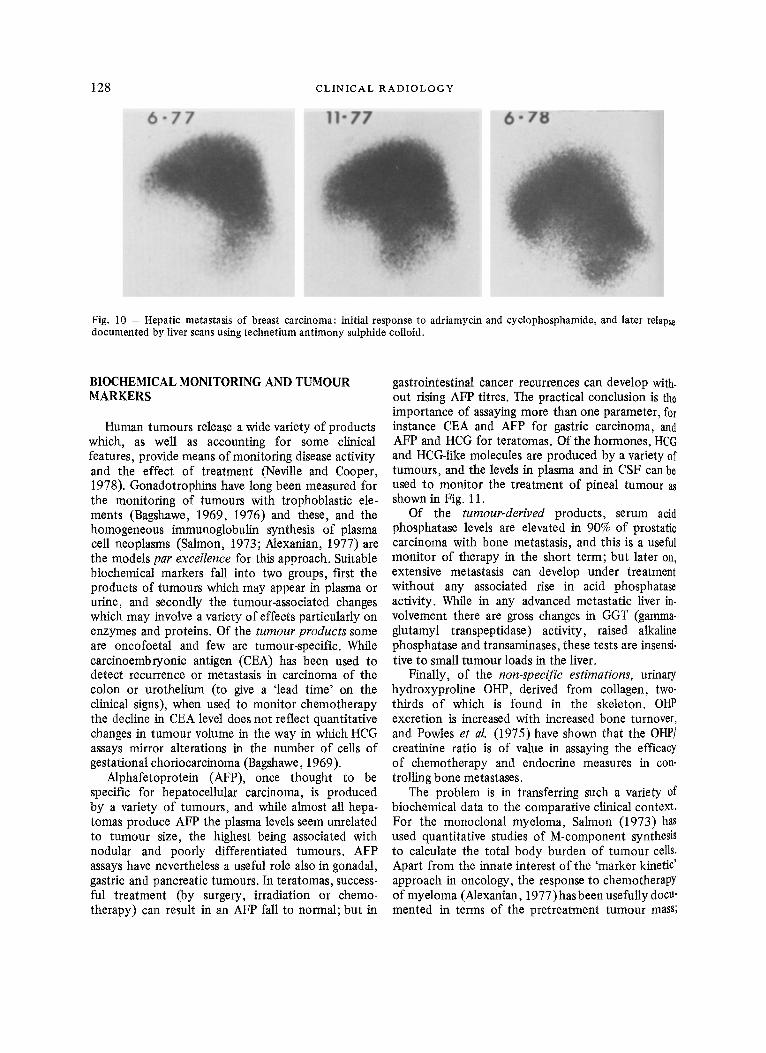
tectmetium-99m phosphate for breast carcinoma metastases, improvement or deterioration is readily observed but difficult to quantitate unless the scan becomes normal. (The value of serial bone scans in prostatic carcinoma has been shown by Shearer et al. (1974) who found that those whose bone scans became negative after at least three months on hormone therapy were more likely to survive at least two years than those whose bone scans remained positive: and the failure of an abnormal scan to revert to normal could be the first indication of hormonal resistance.) In liver scanning with tech- netium-99m sulphur colloid for metastases (Fig. 10) individual focal abnormalities may be difficult to recognise at repeated scans, and lesions of less than 0.5cm in diameter are not usually detected; but within these limitations it can provide useful docu- mentation of therapeutic response and relapse, if not a quantifiable form.
128
6 " 7 7
C L I N I C A L R A D I O L O G Y
11"77 6 - 7 8
Fig. 10 - Hepatic metastasis of breast carcinoma: initial response to adriamycin and cyclophosphamide, and later relapse documented by liver scans using technetium antimony sulphide colloid.
BIOCHEMICAL MONITORING AND TUMOUR MARKERS
Human tumours release a wide variety of products which, as well as accounting for some clinical features, provide means of monitoring disease activity and the effect of treatment (Neville and Cooper, 1978). Gonadotrophins have long been measured for the monitoring of tumours with trophoblastic ele- ments (Bagshawe, 1969, 1976) and these, and the homogeneous irnmunoglobulin synthesis of plasma cell neoplasms (Salmon, 1973; Alexanian, 1977) are the models par excellence for this approach. Suitable biochemical markers fall into two groups, first the products of tumours which may appear in plasma or urine, and secondly the tumour-associated changes which may involve a variety of effects particularly on enzymes and proteins. Of the tumour products some are oncofoetal and few are tumour-specific. While carcinoembryonic antigen (CEA) has been used to detect recurrence or metastasis in carcinoma of the colon or urothelium (to give a 'lead time' on the clinical signs), when used to monitor chemotherapy the decline in CEA level does not reflect quantitative changes in tumour volume in the way in which HCG assays mirror alterations in the number of cells of gestational choriocarcinoma (Bagshawe, 1969).
Alphafetoprotein (AFP), once thought to be specific for hepatocellular carcinoma, is produced by a variety of tumours, and while almost all hepa- tomas produce AFP the plasma levels seem unrelated to tumour size, the highest being associated with nodular and poorly differentiated tumours. AFP assays have nevertheless a useful role also in gonadal, gastric and pancreatic turnouts. In teratomas, success- ful treatment (by surgery, irradiation or chemo- therapy) can result in an AFP fall to normal; but in
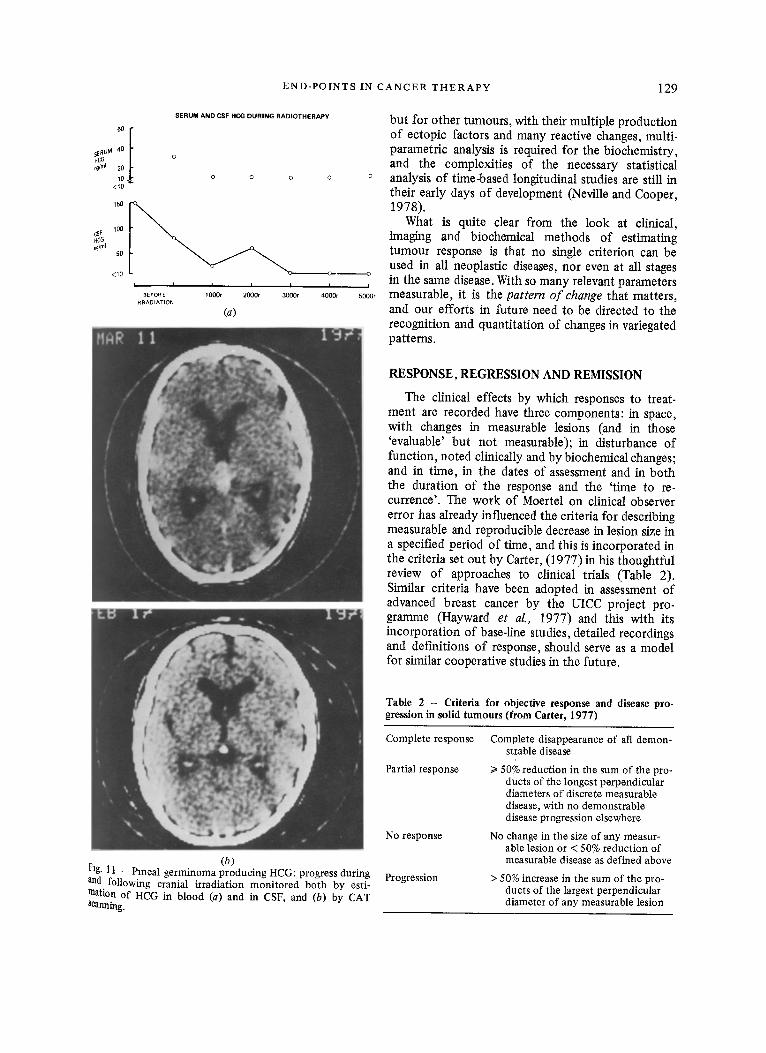
gastrointestinal cancer recurrences can develop with. out rising AFP titres. The practical conclusion is the importance of assaying more than one parameter, for instance CEA and AFP for gastric carcinoma, and AFP and HCG for teratomas. Of the hormones, HCG and HCG-like molecules are produced by a variety of tumours, and the levels in plasma and in CSF can be used to monitor the treatment of pineal tumour as shown in Fig. 11.
Of the tumour-derived products, serum acid phosphatase levels are elevated in 90% of prostatic carcinoma with bone metastasis, and this is a useful monitor of therapy in the short term; but later on, extensive metastasis can develop under treatment without any associated rise in acid phosphatase activity. While in any advanced metastatic liver in. volvement there are gross changes in GGT (gamma- glutamyl transpeptidase) activity, raised alkaline phosphatase and transaminases, these tests are insensi- tive to small tumour loads in the liver.
Finally, of the non-specific estimations, urinary hydroxyproline OHP, derived from collagen, two- thirds of which is found in the skeleton. OHP excretion is increased with increased bone turnover, and Powles et al. (1975) have shown that the OHP/ creatinine ratio is of value in assaying the efficacy of chemotherapy and endocrine measures in con- trolling bone metastases.
The problem is in transferring such a variety of biochemical data to the comparative clinical context. For the monoclonal myeloma, Salmon (1973) has used quantitative studies of M-component synthesis to calculate the total body burden of tumour cells. Apart from the innate interest of the 'marker kinetic' approach in oncology, the response to chemotherapy of myeloma (Alexanian, 1977)hasbeen usefully docu- mented in terms of the pretreatment turnout mass;
END-POINTS IN CANCER THERAPY 129
HC6 ~fnl
<10
CSF HCG ng/rn I
SERUM AND CSFHCG DURING RADIOTHERAPY
O O O O
100
5O
< 1 0
• I I I I
BEFORE lO00r 2000r 30GOt tRRADIATION
(a)
, O
I
4 0 0 0 r
but for other tumours, with their multiple production o f ectopic factors and many reactive changes, multi- parametric analysis is required for the biochemistry, and the complexities of the necessary statistical
° analysis o f time-based longitudinal studies are still in their early days o f development (Neville and Cooper, 1978).
What is quite clear from the look at clinical, imaging and biochemical methods of estimating tumour response is that no single criterion can be used in all neoplastic diseases, nor even at all stages in the same disease. With so many relevant parameters
5000, measurable, it is the pattern o f change that matters, and our efforts in future need to be directed to the recognition and quantitation of changes in variegated patterns.
RESPONSE, REGRESSION AND REMISSION
The clinical effects by which responses to treat- ment are recorded have three components: in space, with changes in measurable lesions (and in those 'evaluable' but not measurable); in disturbance of function, noted clinically and by biochemical changes; and in time, in the dates of assessment and in both the duration of the response and the 'time to re- currence'. The work of Moertel on clinical observer error has already influenced the criteria for describing measurable and reproducible decrease in lesion size in a specified period of time, and this is incorporated in the criteria set out by Carter, (1977) in his thoughtful review of approaches to clinical trials (Table 2). Similar criteria have been adopted in assessment of advanced breast cancer by the UICC project pro- gramme (Hayward et al., 1977) and this with its incorporation of base-line studies, detailed recordings and definitions o f response, should serve as a model for similar cooperative studies in the future.
(b) Fig. 11 - Pineal germinoma producing HCG: progress during and following cranial irradiation monitored both by esti- mation of HCG in blood (a) and in CSF, and (b) by CAT Scanning.
Table 2 - Criteria for objective response and disease pro- gression in solid tumours (from Carter, 1977)
Complete response
Partial response
No response
Progression
Complete disappearance of all demon- strable disease
I> 50% reduction in the sum of the pro- ducts of the longest perpendicular diameters of discrete measurable disease, with no demonstrable disease progression elsewhere
No change in the size of any measur- able lesion or < 50% reduction of measurable disease as defined above
> 50% increase in the sum of the pro- ducts of the largest perpendicular diameter of any measurable lesion
130 C L I N I C A L R A D I O L O G Y
There is clearly such a need, for in practice there have been vast differences in usage between the various subspecialties of ontology, so that a cursory look at published results may mislead those not involved in that particular type of study. For instance, the EORTC Clinical Screening Group (1973), reporting the 'oncostatic effect' of epipodo- phyllotoxin VP16213 in leukaemia and solid tumours defined remission as the 'apparent disappearance of the disease', regression as the 'apparent complete disappearance of tumour ' ; both remission and regression could be complete or incomplete, and whether each was more or tess than 50% was 'necessarily subjective'. Again, the term 'remission' has come to have specific import in the leukaemias and in lymphoma, but it has been extended less substantially to, for instance, myeloma when Salmon (Alberts et al., 1976) defines 'complete remission' as greater than 75% reduction in tumour cell mass, with relief of pain and increase in haemoglobin and serum albumen.
In Hodgkin's disease patients are considered to be in complete clinical remission (Sutcliffe et al., 1978a) when there are no symptoms or signs of the disease, chest X-ray and lymphography are normal, and routine blood tests have become normal. The prog- nostic significance of such remission at one year is highly correlated with survival, and it has important implications for continuing chemotherapy. So it is of particular interest that in the recent investigation by Sutcliffe et al. (1978b) of post-treatment taparo- tomies after chemotherapy, they showed that 4 to 19 cases, considered to be free of abdominal disease on the strict criteria given, had residual active Hodgkin's disease, and that they were able to define the three histological categories negative, active, and healed disease. In most otber diseases it is unusual for patients labelled 'in remission' to be subjected to such searching checks of disease status, but one may surmise on the possible implications. The common usage of 'remission' in medical oncology having been defined, it is perplexing to find it used in CNS tumours in a quite different sense. Rosenblum et al. (1973) in describing their use of CCNU in malignant brain tumours developed a staging system depending on both symptoms and signs, and 'if a patient improves in disease stage he was considered a "Remission" '. By this criterion their initial clinical response to CCNU was 'a 37% remission rate' but this is liable to misinterpretation when reported briefly and out of context.
The concept of 'disease stasis' has had a vogue in describing the unmeasurable, particularly in abdominal tumours, but Wiltshaw and Kroner (1976) pertinently state that in their experience of ovarian
carcinoma so-called 'no change' usually represent ~ advancing disease. The methods for assessing tt~s tumour are probably the least sophisticated in the oncological spectrum, and this is unfortunate in viev¢ of its interest for immunotherapy and particularly for the recently reported predictive tests for cancer chemotherapy (Salmon et al., 1978).
With increased specialisation in oncology and the mass of reports it becomes increasingly difficult for physicians to critically evaluate each study, and Carter (1977) has stressed the need for guide-lines for study design and data reports 'to bring some e0. herence to the chaos now found in the oncological literature'. The first steps out of a semantic rnor~ are being taken by strict def'mition of terms, but it Is clearly important that those who use them should be aware of the usages of others who may have more than a marginal interest in their study.
EFFECTS ON NORMAL TISSUES
When we turn to the other side of the therapeutic equation, to assessing the effect on normal tissues,it is important that we compare like with like. The tumour process is assessed by its main function -that of unbridled reproduction - so that normal tissue effects should also be assessed in terms of function rather than on any static histological appearances This gives us a diverse series of end-points depending on bodily systems, but in addition to specialised function in the limit the important end-point is the ability to cope with stress. Examples are seen in the haemopoietic reserve after chemotherapy, or the ability of connective tissue to respond to physical or ischaemic stress after irradiation. The quantitati0n of normal tissue responses has of course to be by the methods of the 'system specialty', and as these become progressively more sophisticated it follows that the evidence for levels of tissue damage has to be re-examined every few years; but the end-point chosen should be directly relevant to dose-response, and not some trivial side effect seized upon by the organ specialist: for what can be measured will be measured. In the case of late effects it is clearly desirable to have exact knowledge of the original patient pool, and adequate numbers of patients surviving long enough for latency and 'at risk' factors to be elucidated. Then not only may frequency diagrams be produced, but 'probit analysis' can pro. duce curves predicting the probability of developing the late complication (e.g. Wara et al. (1975) for thoracic radiation myelopathy) and this is of course what the clinician really wants to know.
The real difficulties arise in the quantitation of combined radiation and chemotherapy effects in
END-POINTS IN CANCER THERAPY 131
critical tissues of the antibiotic agents which enhance radiation reaction, and of those drugs such as Adria- roycin arid Methotrexate which themselves damage the tissues (the heart or CNS) directly. These effects are particularly important in paediatric ontology. As the 'dose effect factor ' (Phillips and Fu, 1976)varies from 1.1 to 1.8 there is considerable urgency in acquiring further information from experimental models and clinical data.
Finally, with increased survival, the problem of late carcinogenesis, exemplified in our recent experience by such bizarre tumours as mesothelioma and fibrosarcoma of the uterine cervix following prolonged alkylating therapy for Hodgkin's disease. Again we need data on incidence and latency in relation to the degree of exposure, and then on the probability of tumour induction; now the urgency is of course the need for guidance in matters o f adjuvant chemotherapy for curable conditions.
10
08
06
04 PROBABILITy OF SURVIVING
02
01 12 24 36
TIMEIN MONTHS
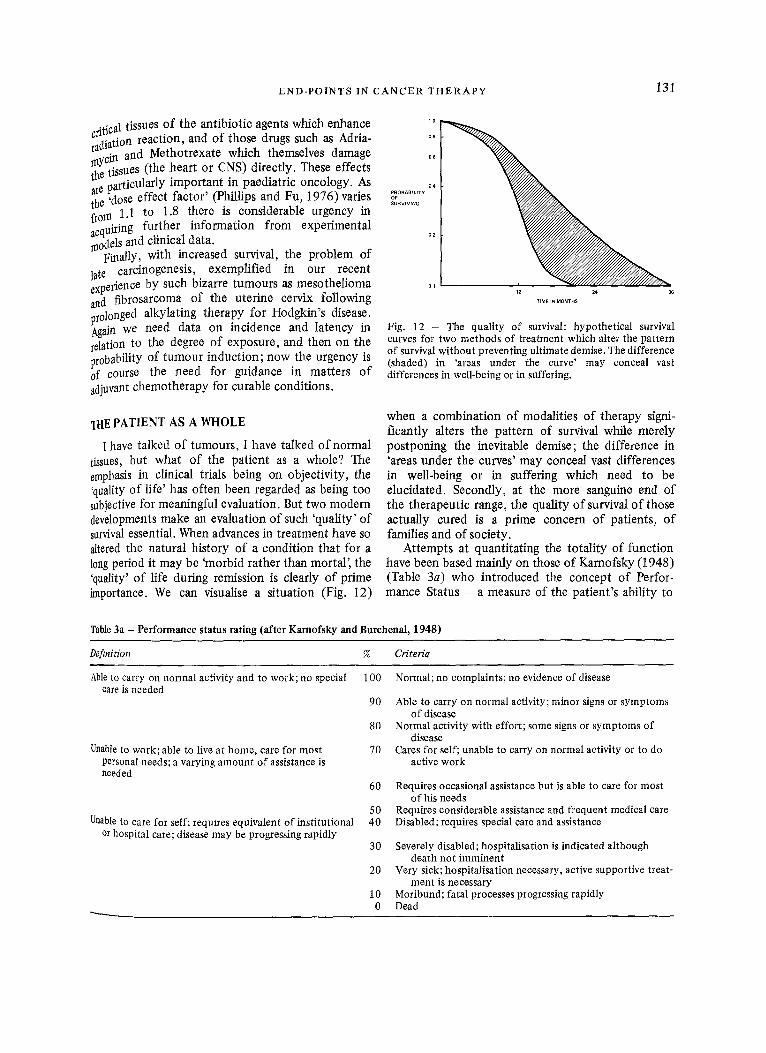
Fig. 12 - The quality of survival: hypothetical survival curves for two methods of treatment which alter the pattern of survival without preventing ultimate demise. The difference (shaded) in 'areas under the curve' may conceal vast differences in well-being or in suffering.
THE PATIENT AS A WHOLE
I have talked of tumours, I have talked of normal tissues, but what o f the patient as a whole? The emphasis in clinical trials being on objectivity, the 'quality of life' has often been regarded as being too subjective for meaningful evaluation. But two modern developments make an evaluation of such 'quality' of survival essential. When advances in treatment have so altered the natural history of a condition that for a 10ng period it may be 'morbid rather than mortal', the 'quality' o f life during remission is clearly o f prime importance. We can visualise a situation (Fig. 12)
when a combination of modalities of therapy signi- ficantly alters the pattern of survival while merely postponing the inevitable demise; the difference in 'areas under the curves' may conceal vast differences in well-being or in suffering which need to be elucidated. Secondly, at the more sanguine end of the therapeutic range, the quality o f survival o f those actually cured is a prime concern of patients, o f families and of society.
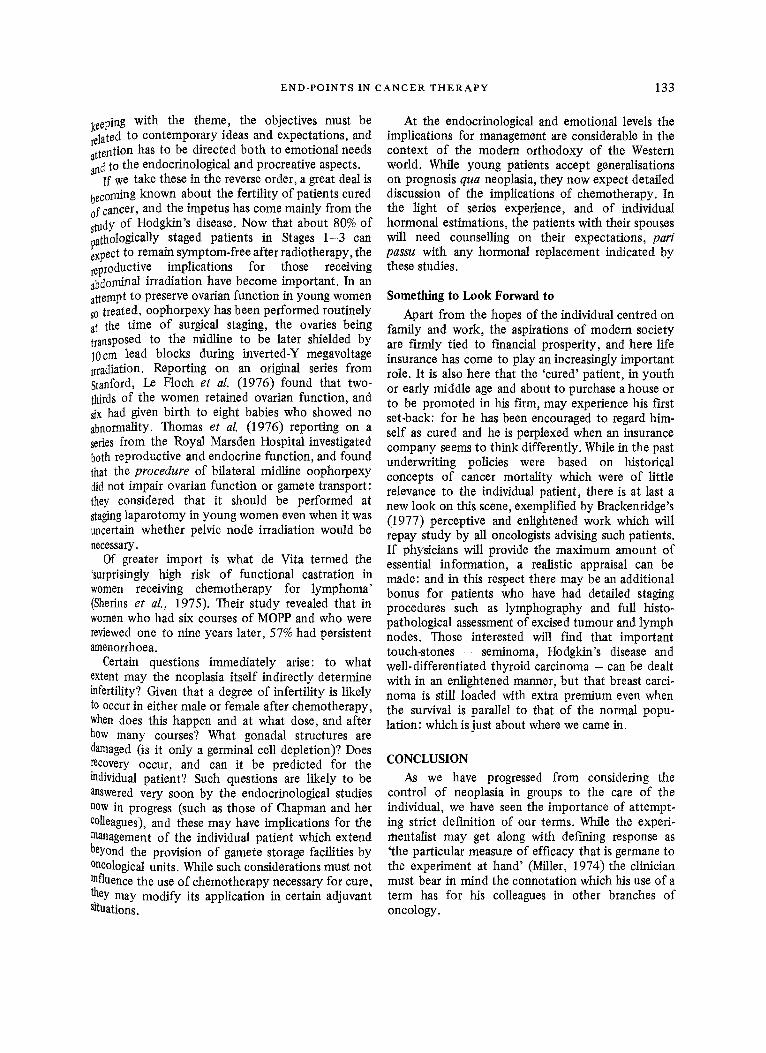
Attempts at quantitating the totality of function have been based mainly on those of Karnofsky (1948) (Table 3a) who introduced the concept of Perfor- mance Status - a measure of the patient's ability to
Table 3a - Performance status rating (after Karnofsky and Burchenal, 1948)
Defmition % Criteria
Able to carry on normal activity and to work; no special 100 Normal; no complaints; no evidence of disease care is needed
90
80
7O Unable to work; able to live at home, care for most personal needs; a varying amount of assistance is needed
Unable to care for self; requtres equivalent of institutional or hospital care; disease may be progressing rapidly
60
50 40
30
20
10 0
Able to carry on normal activity; minor signs or symptoms of disease
Normal activity with effort; some signs or symptoms of disease
Cares for self; unable to carry on normal activity or to do active work
Requires occasional assistance but is able to care for most of his needs
Requires considerable assistance and frequent medical care Disabled;requires special care and assistance
Severely disabled; hospitalisation is indicated although death not imminent
Very sick; hospitalisation necessary, active supportive treat- ment is necessary
Moribund; fatal processes progressing rapidly Dead

132 CLINICAL RADIOLOGY
Table 3b - MRC 5-point scale of perfor- mance status
1. Normal activity 2. Fully active but not working 3. Out and about but restricted activity 4. Confined at home or hospital 5. Bedridden
continue useful work and to care for his own needs, or his dependence on nursing or hospital care. Its use is exemplified by Hyde's study (1973) of inoperable lung cancer, with a consistent linear correlation between log-survival and initial Kamofsky rating which is not entirely surprising in this extensive disease group. In this country the categories are usually reduced to five, as in the MRC performance scale (Table 3b).
The problems of function and quality evaluation are never more difficult than following the prolon- gation of life in patients with malignant brain tumours. Rosenblum and Walker (Rosenblum et al., 1973; Sklansky et al., 1974) have elaborated the Kamofsky system to take into account both neuro- logical signs and symptoms (Table 4) and have described a Central Nervous System Disease Staging System in which a patient is placed in one or four disease stages based on a combined evaluation of symptoms, signs and function. Their criterion of therapeutic effect was, as already mentioned, improvement by one or more disease stages maintained at least until the end of a course of chemotherapy. 'Quality' of survival for such patients still eludes definition, and the philosophical overtones are revealed in Penman and Smith's (1954) term of 'useful survival', meaning that in their view 'a sensible on-looker, knowing and bearing in mind the sort of person the patient was before his illness, would on the whole be glad he was still alive'. The affective
Table 4 - CNS disease staging system of Rosenblum and Walker (from Sklansky et al., 1974)
A. Signs
Mental status Speech Visual fields Intracranial hypertension Cranial nerves Motor Sensory Cerebellar Other
B. Symptoms and function
Graded from 1 (normal) to 4 (severe deficit)
Disease stage = highest number in either category A or B.
changes which are part of the neurological defici t usually prevent such patients from themselves taking part in a subjective assessment; but in advanced breast cancer this is not so, and Priestman and Baum (1976) have pioneered the technique of 'linear analogue self. assessment' (LASA) to measure the subjective effeet~ of treatment. LASA is a standard form of psyche. logical testing which they adapted using indices SUch as well-being, activity, pain (and including the question 'is treatment helping?') so as to produce a numerical score. Applied to both response and toxi. city it gave in their hands reliable and reproducible results, and while it gives of necessity a superficial view, it is a first step towards recognising and quanti. tating the supreme importance of quality of life in assessing the overall response to chemotherapy.
PERSONAL END-POINTS
What of the quality of life of patients who are regarded as 'cured', and have been told so by their physician? Each will have his or her own 'end-point' of hopes and aspirations, even of assumptions, which it is the place of the physician to support. But with any evaluation of 'quality' we pass straight into the realm of philosophy. It has been said that for a life of fulfilment a person needs three things: something to do, someone to love and something to look forward to: and perhaps I may be forgiven for looking at these in the present context. As by modern standards mere survival is quite inadequate as an end-point, any criterion for quality must also be set in contemporary terms.
Something to Do
The employability of those cured of cancer has been examined several times, most recently by a large New York organisation, the Metropolitan Life Insurance Company (Wheatley et aL, 1974); it has found that about 50% of applicants with a cancer history (and who had had a wide variety of tumours) could be medically accepted for employment, and that their subsequent employment record was saris. factory. Community and industrial health physicians have their part to play in ensuring that patients ha this category are not placed at a disadvantage when being considered for employment, for even the NHS itself has been known to show reluctance to take on what the uninformed regard as 'yet another lame duck'.
Someone to Love As we have been exploring quantitation I hasten
to reassure you, Mr President, that it is no part of this lecture to try to quantify amatory pursuits. But ha
E N D - P O I N T S IN C A N C E R T H E R A P Y 133
keeping with the theme, the objectives must be related to contemporary ideas and expectations, and attention has to be directed both to emotional needs ~ad to the endocrinological and procreative aspects.
If we take these in the reverse order, a great deal is becoming known about the fertility of patients cured of cancer, and the impetus has come mainly from the studY of Hodgkin's disease. Now that about 80% of pathologically staged patients in Stages 1-3 can expect to remain symptom-free after radiotherapy, the reproductive implications for those receiving abdominal irradiation have become important. In an attempt to preserve ovarian function in young women so treated, oophorpexy has been performed routinely at the time of surgical staging, the ovaries being transposed to the midline to be later shielded by 10cm lead blocks during inverted-Y megavoltage irradiation. Reporting on an original series from Stanford, Le Floch et al. (1976) found that two- thirds of the women retained ovarian function, and six had given birth to eight babies who showed no abnormality. Thomas et al. (1976) reporting on a series from the Royal Marsden Hospital investigated both reproductive and endocrine function, and found that the procedure of bilateral midline oophorpexy did not impair ovarian function or gamete transport: they considered that it should be performed at staging laparotomy in young women even when it was uncertain whether pelvic node irradiation would be necessary.
Of greater import is what de Vita termed the 'surprisingly high risk of functional castration in women receiving chemotherapy for lymphoma' (Sherins et al., 1975). Their study revealed that in women who had six courses of MOPP and who were reviewed one to nine years later, 57% had persistent amenorrhoea.
Certain questions immediately arise: to what extent may the neoplasia itself indirectly determine infertility? Given that a degree of infertility is likely to occur in either male or female after chemotherapy, when does this happen and at what dose, and after how many courses? What gonadal structures are damaged (is it only a germinal cell depletion)? Does recovery occur, and can it be predicted for the individual patient? Such questions are likely to be answered very soon by the endocrinological studies now in progress (such as those of Chapman and her colleagues), and these may have implications for the management of the individual patient which extend beyond the provision of gamete storage facilities by 0ncological units. While such considerations must not tnfluence the use of chemotherapy necessary for cure, they may modify its application in certain adjuvant situations.
At the endocrinological and emotional levels the implications for management are considerable in the context of the modern orthodoxy of the Western world. While young patients accept generalisations on prognosis qua neoplasia, they now expect detailed discussion of the implications of chemotherapy. In the light of series experience, and of individual hormonal estimations, the patients with their spouses will need counselling on their expectations, pari passu with any hormonal replacement indicated by these studies.
Something to Look Forward to
Apart from the hopes of the individual centred on family and work, the aspirations of modern society are firmly tied to financial prosperity, and here life insurance has come to play an increasingly important role. It is also here that the 'cured' patient, in youth or early middle age and about to purchase a house or to be promoted in his firm, may experience his first set-back: for he has been encouraged to regard him- self as cured and he is perplexed when an insurance company seems to think differently. While in the past underwriting policies were based on historical concepts of cancer mortality which were of little relevance to the individual patient, there is at last a new look on this scene, exemplified by Brackenridge's (1977) perceptive and enlightened work which will repay study by all oncologists advising such patients. If physicians will provide the maximum amount of essential information, a realistic appraisal can be made: and in this respect there may be an additional bonus for patients who have had detailed staging procedures such as lymphography and full histo- pathological assessment of excised tumour and lymph nodes. Those interested will Fred that important touch-stones - seminoma, Hodgkin's disease and well-differentiated thyroid carcinoma - can be dealt with in an enlightened manner, but that breast carci- noma is still loaded with extra premium even when the survival is parallel to that of the normal popu- lation: which is just about where we came in.
CONCLUSION As we have progressed from considering the
control of neoplasia in groups to the care of the individual, we have seen the importance of attempt- ing strict definition of our terms. While the experi- mentalist may get along with defining response as 'the particular measure of efficacy that is germane to the experiment at hand' (Miller, 1974) the clinician must bear in mind the connotation which his use of a term has for his colleagues in other branches of oncology.

134 CLINICAL RADIOLOGY
Concepts of 'cure' were originally devised so as to reassure patients, but one may suspect that some recent extrapolations have been derived equally to reassure the oncologists themselves. If they are not on sure ground when communicating within clinical science the issues may rebound, for there are those who, in relation to the funding of cancer research, do not hesitate to point out that it was 'the cancer researchers who actually originated the numbers game'.
We have seen that there is no single criterion of response which can be used in all neoplastic diseases, nor at all stages of the same disease, and the important feature is the change in pattern of relevant parameters. Pattern recognition, both conscious and subliminal, has probably always been the basic method of clinical medicine, and in evaluating the results of cancer treatment we are, with all modern aids, just extending this basic medical expertise.
The natural history of many cancers has been so modified by treatment as to require a change in end- points, and with fuller control of neoplasia we are now concerned with matters which even a decade ago would have seemed academic. Undoubtedly the quality o f survival is of a different order of impor- tance from the effects which are measurable, and it is equally the most difficult to evaluate. The energies of clinical oncologists will in future be increasingly devoted to considering this paramount feature of any therapeutic equation, and if it is not assessable in comparative statistical terms, this is a characteristic shared with all the highest activities of man.
Acknowledgements. I wish to express my thanks to the following for kindly permitting reproduction of illustrations: Dr Ray Bush for Figs 1 and 2; Drs Brinkley and Haybittle for Fig. 3; Dr E. D. Thomas for Fig. 4; and Professor G. M. Besser and Dr J. Wass for the use of unpublished data in Figs 6 and 11 respectively.
REFERENCES
Alberts, D. S., Durie, B. G. M. & Salmon, S. E. (1976). Doxorubicin/BCNU chemotherapy for multiple myeloma in relapse. Lancet, 1,926-928.
Alexanian, R. (1977) Plasma cell neoplasms. Medicine, 2nd Series, ed. Malpas, J. S. & Weatherall, D. J., 30, 1700- 1712.
Bagshawe, K. D. (1969). Choriocarcinoma. Arnold, London. Bagshawe, K. D. (1976). In Cancer Related Antigens, ed.
Franchirmont, P., p. 251. Elsevier Amsterdam. Barendsen, G. W. & Broerse, J. J. (1969). Effects of 15 MeV
neutrons and 300 kV X-rays on a rat rhabdomyosarcoma. European Journal of Cancer, 5,373-391.
Brackenridge, R. D. (1977). Medical Selection of Life Risks, p. 486. Undershaft Press, London.
Brinkley, D. & Haybittle, J. L. (1975). The curability of breast cancer. Lancet, 2, 95-97.
Burgess, C. A. & Edwards, C. R. W. (1978). Hirsutography British Journal of Photography, 125,770-772.
Bush, R. S., Gospodarowicz, M., Sturgeon, J. & Alison, 1~ (1977). Radiation therapy of localised non-Hodgkt~, lymphoma. Cancer Treatment Reports, 61, 1129-1136
Bush, R. S. (1979). Malignancies of the ovary, uterus and cervix. In The Management o f Malignant Disease Sene~ ed. Peckham, M. J. & Carter, R. L. Edward Arnold, London.
Carter, S. K. (1977). Clinical trials in cancer chemotherapy Cancer, Suppl., 40, 544-557.
Dawson, J. M., Hall, T. C., Schneiderman, M. A., Schnider, I., Owens, A. H., Anderws, J. R., Baxter, D. H., Brenner S., Hunter, C., Levene, M. B., Sheenan, F. R. &White, Gi (1966). Objective evaluation of change in turnout size aq lung cancer patients with non-measurable disease. Cancer, 19,415-420.
Easson, E. C. (1966). Possibilities for the cure of Hodgkin's disease. Cancer, 19, 345-350.
Easson, E. C. & Russell, M. H. (1963). The cure of Hodgkin's disease. British Medical Journal, 1, 1704 - 1707.
Ell, P. J., Williams, E. S. & Todd-Pokropek, E. E. (1978). ~e clinical use of diagnostic imaging. British Journal o[ Hospital Medicine, 20, 119-127.
Engstrom, J. E. & Austin, D. F. (1977). Interpreting cancer survival rares. Science, 195, 847-851.
EORTC Chnical Screening Group (1973). Epipodophyll0. toxin VP 16213 in treatment of acute leukaemias, haerna. tosarcomas, and solid tumours. British Medical Journal, 30, 199-202.
Frei, E. & Gehan, E. A. (1971). Definition of cure for Hodgkin's disease. Cancer Research, 31, 1828-1833.
Gehan, E. A. & Freireich, E. J. (1974) Non-randomised controls in cancer clinical trials. New England Journal of Medicine, 290, 198-203.
Greenwood, M. (1926) A report on the natural duration of cancer. Ministry of Health Report No. 33 HM Stationery Office, London.
Hayward, J. L., Rubens, R. D., Carbone, P. P., Heuson. J. C, Kumaoka, S. & Segaloff, A. (1977). Assessment of response to therapy in advanced breast cancer. British Journal of Cancer, 35,292-298.
Hill, R. P. & Bush, R. S. (1969). A lung-colony assay to determine the radiosensitivity of the cells of a solid tumour. International Journal of Radiation Biology, 15, 435-444.
Hyde, L. Wolf, McCracken, S. & Yenser, R. (1973). Natural course of inoperable lung cancer. Chest, 64, 309-312
Karnofsky, D. A. & Burchenal, J. H. (1948). In Evaluation of Chemotherapeutic Agents, ed. MacLeod, C. M., London.
Le Floch, O., Donaldson, S. S. & Kaplan, H. S. (1976) Pregnancy following oophoropexy and total nodal lrradla. tion in women with Hodgkin's disease. Cancer, 38, 2263- 2268.
Leiberman, D. P. (1978). CRC Breast Study Annual Meeting Report (personal communication).
McNally, N. J. & Sheldon, P. W. (1977). The effect of radia- tion on tumour growth, cell survival and cure of the animal using a single tumour system. British Journal of Radiology. 50, 321-328.
McNally, N. J. (1975). The effect of an hypoxic cell sens~tlser on tumour growth delay and cell survival. British Journal of Cancer, 32,610-618.
Miller, I. (1974). Statistical design for experiments in conabl" nation therapy. Cancer Chemotherapy Reports, 4, 151- 156.
Moertel, G. C. & Hanley, J. A. (1976). The effect of measur"
END-POINTS IN CANCER T H E R A P Y 135
l~g error on the results of therapeutic trials in advanced cancer- Cancer, 38, 388-394.
g,rraY J' G. (1974). Cancer Research Campaign Breast ~studY' British Journal of Surgery, 61,772-774.
Neville, A. M. & Cooper, E. H. (1978). Biochemical moni- toring of cancer. Annals of Clinical Biochemistry, 13, 283-305.
po~man, J. & Smith, M. C. (1954). Intracranial gliomata. ~l~edical Research Council Special Report Series, No. 284,
p. 66. Feto, R., Pike, M. C., Armitage, P., Breslow, N. E., Cox, D.
R., Howard, S. V., Mantel, N., McPherson, K., Peo, J. & smith, P. G. (1976). Design and analysis of randomised clinical trials requiring prolonged observation of each patient. I. Analysis and design. British Journal of Cancer, 34,585-612.
peto, R., Pike, M. C., Armitage, P., Breslow, N. E., Cox, D. R., Howard, S. V., Mantel, N., McPherson, K., Peo, J. & smith, P. G. (1977). Design and analysis of randomised clinical trials requiring prolonged observation of each patient. II. Analysis and examples. British Journal of Cancer, 35, 1-39.
phillips, T. L. & Fu, K. K. (1976). Quantitation of combined radiation therapy and chemotherapy effects on critical normal tissues. Cancer, 37, Suppl. 2, 1186-1200.
powles, T. J., Leese, C. L. & Bondy, P. K. (1975). Hydroxy- proline excretion in patients with breast cancer and response to treatment. British Medical Journal, 2, 164- 166.
Pnestman, T. J. & Baum, M. (1976). Evaluation of quality of life in patients receiving treatment for advanced breast cancer. Lancet, 1,899--902.
Puck, T. T. & Marcus, P. I. (1956). Action of X-rays on mammalian cells. Journal of Experimental Medicine, 103, 653 -667.
Rosenblum, M. L., Reynolds, A. F., Smith, K. A., Bumack, B. H. & Walker, M. D. (1973). CCNU in the treatment of malignant brain tumours. Journal of Neurosurgery, 39, 306 -314.
Russell, M. H. (1958). Contribution to Symposium on Presentation of Results of Cancer Treatment, London. 7th International Cancer Congress.
Salmon, S. E. (1973). Immunoglobulin synthesis and tumour kinetics of multiple myeloma. Seminars in Haematology, 10,135 147.
Salmon, S. E., Hamburger, A. W., Soehnlen, B., Durie, B. G. M., Alberts, D. S. & Moon, T. E. (1978). Quantita- tion of differential sensitivity of human turnout cells to anticancer drugs. New England Journal of Medicine, 298, 1321-1327.
Schaner, E. G., Head, G. L., Doppman, J. L. & Young, R. C. (1977). Computed tomography in the diagnosis, staging
and management of abdominal lymphoma. Journal of Computer Assisted Tomography, 1, 176-180.
Shearer, R. J., Constable, A. R., Girling, M., Hendry, W. P. & Fergusson, J. D. (1974) Radioisotopic bone scinto- graphy with the gamma camera in the investigation of prostatic cancer. British Medical Journal, 2, 362-366.
Sherins, R., Winokur, S. & De Vita, V. T. (1975). Surpri- singly high risk of functional castration in women receiv- ing chemotherapy for lymphoma. Clinical Research, 23, 343A.
Skipper, H. E., Schabel, F. M., Jr & Wilcox, W. S. (1964). Experimental evaluation of potential anti-cancer agents. XIII. On the criteria and kinetics associated with 'cur- ability' of experimental leukemias. Cancer Chemotherapy Reports, 35, 1-111.
Sklansky, B. D., Mann-Kaplan, R. S., Reynolds, A. F., Rosen- blum, M. L. & Walker, M. D. (1974). 4'-Dimethyl-epipo- dophylotoxin-#-D-thenylidene glucoside (PT6) in the treatment of malignant intracranial neoplasms. Cancer, 33,460-467 .
Steel, G. G. (1977). Growth Kinetics of Tumours, p. 307. Oxford.
Sutcliffe, S. B., Wrigley, P. F. M., Peto, J., Lister, T. A., Stansfeld, A. G., Whitehouse, J. M. A., Crowther, D. & Malpas, J. S. (1978a). MVPP chemotherapy regimen for advanced Hodgkin's disease. British Medical Journal, 1, 679-683.
Sutcliffe, S. B., Stansfeld, A. G., Wrigley, P. F. M., Katz, D., Shand, W. S. & Malpas, J. S. (1978b). Post-treatment laparotomy in the management of Hodgkin's disease. Lancet, 1, 57-60.
Thomas, E. D., Flournoy, N., Buckner, C. D., Clift, R. A., Fefer, A., Neiman, P. E. & Storb, R. (1977). Cure of leukaemia by marrow transplantation. Leukaemia Research, 1, 67-70.
Thomas, P. R. M., Winstanly, D., Peckham, M. J., Austin, D. E., Murray, M. A. F. & Jacobs, H. S. (1976). Repro- ductive and endocrine function in patients with Hodgkin's disease: effects of oophoropexy and irradiation. British Journal of Cancer, 33, 226-231.
Thomlinson, R. H. (1977). Implications of the changing size of tumours. British Institute of Radiology Symposium, December 1977 ; and personal communication.
Wara, W. M., Phillips, T. L., Sheline, G. E. & Schwade, J. G. (1975). Radiation tolerance of the spinal cord. Cancer, 35, 1558-1562.
Wheatley, G. M., Cunnick, W. R., Wright, B. P. & van Keuren, D. (1974). The employment of persons with a history of treatment for cancer. Cancer, 33,441-446.
Wiltshaw, E. & Kroner, T. (1976). Phase II study of cis- dichlorodiammineplatinum II (NSC-119875) in advanced adenocarcinoma of the ovary. Cancer Treatment Reports, 60, 55-60.