Embed Size (px)
Citation preview

lACC Vol. 10, No.5November 1987:1113-21
1113
End-Systolic Radius to Thickness Ratio: An Echocardiographic Indexof Regional Performance During Reversible Myocardial Ischemia inthe Conscious Dog
WILLIAM A. ZOGHBI, MD, FACC, MARTIN L. CHARLAT, MD, ROBERTO BOLLI, MD, FACC,
HELEN KOPELEN, LVN, CRAIG J. HARTLEY, PHD, ROBERT ROBERTS, MD, FACC,
MIGUEL A. QUINONES, MD, FACC
Houston. Texas
Regional myocardial dysfunction induced by ischemia isassociated with less thickening and a larger ventricularradius at end-systole. Thus, end-systolic radius to thickness ratio measured by echocardiography may providean accurate index of regional left ventricular functionthat is totally independent of cardiac motion. To test thishypothesis, a total of 14 transient (~10 minutes) coronary artery occlusions (8 left anterior descending, 6 leftcircumflex) followed by up to 24 hours of reperfusionwere performed in six chronically instrumented conscious dogs providing multiple grades of regional ventricular dysfunction. Regional myocardial thickeningfraction was determined with epicardial pulsed Dopplerprobes and served as an independent standard for comparison with simultaneous echocardiographic measurements. End-systolic radius to thickness ratio and radialshortening fraction were derived from the two-dimensional echocardiographic short-axis view along 12 equidistant radii.
In the ischemic zone, percent thickening fraction averaged 22 ± 5% during baseline, decreased to -4 ±4% during occlusion with gradual return to baseline
Accurate quantitation of regional myocardial function iscrucial for the assessment of the extent of myocardial dysfunction and the evaluation of the effects of interventionson the ischemic myocardium, Two-dimensional echocardi-
From the Section of Cardiology. Department of Medicine, Baylor College of Medicine, Houston, Texas. Computational assistance was providedby the CLiNFO Project funded by Grant RR-00350 from the Division ofResearch Resources, National Institutes of Health, Bethesda, Maryland.This paper was presented in part at the 58th Annual Session of the AmericanHeart Association, November 1985. Washington, D.C.
Manuscript received December 23, 1996; revised manuscript receivedApril 29, 1987, accepted May IS. 1987.
Address for reprints: William A. Zoghbi, MD, Section of Cardiology,Baylor College of Medicine, 6535 Fannin, MS, F-IOOl, Houston. Texas77030.
© 1987 by the American College of Cardiology
after reperfusion. End-systolic radius to thickness ratioaveraged 1.39 ± 0.25 before coronary occlusion andincreased to 2.97 ± 0.48 during occlusion with a gradualreturn to baseline values. A significant correlation wasfound between Doppler-determined thickening fractionmeasurements and echocardiographic end-systolic radius to thickness ratio as well as radial shortening fraction for absolute values (r = - 0.83 and 0.75, respectively; n = 65) and percent change from baseline (r =-0.86 and 0.78, respectively). Using 95% confidencelimits, the sensitivity and specificity of end-systolic radius to thickness ratio for detecting regional thickeningabnormalities were 81 and 79%, respectively, and forthe radial shortening method were 89 and 71%, respectively.
Thus, measurements of end-systolic radius to thickness ratio provide an alternative echocardiographicmethod for quantitating regional left ventricular function that compares well with an independent standardand, in contrast to existing methods, is not affected byexternal cardiac motion.
(J Am Coil CardioI1987;LO:1l13-21)
ography has been shown, in experimental animals and clinical studies, to be a sensitive and specific technique for thedetection of regional wall motion abnormalities (1-17). Todate, methods quantitating regional function from the shortaxis view have predominantly involved measurements ofmyocardial thickening or shortening of intracavitary radiior areas during contraction from end-diastole to end-systole,Consequently, these methods depend on the reference system used to correct for cardiac translation and rotation(S-I4,I6-19). Furthermore, the accuracy of these methodsduring various grades of regional dysfunction has never beenevaluated against an independent quantitative standard.
The left ventricular radius to wall thickness ratio is amajor determinant of systolic wall stress and has been used
0735-1097/87/$3.50

1114 ZOGHBI ET AL.END-SYSTOLIC RADI US TO TIIiCKNESS RAno
lACC Vol. 10. No.5November 1987:1113-21
clinically to characterize the response of the left ventricleto chronic pressure or volume overload (20 ,21) . More recently, Osakada et al. (22) demonstrated in a closed chestdog model of progressive ischemia a significant decrease inend-systolic wall thickness with a concomitant increase inend-systolic dimension and wall stress in the ischemic region . Thus, it is conceivable that regional end-systolic radiusto thickness ratio may provide an index of regional functionsensitive to alterations induced by ischemia. The presentinvestigation was undertaken in a conscious canine modelof reversible ischemia to explore this hypothesis. If validated, measurements of end-systolic radius to thickness ratiowould have the advantage of requiring only a single endsystolic frame and thus eliminating the problems of cardiactranslation and rotation. A recently developed epicardialDoppler probe (23) that measures regional myocardial thickening was used as an independent standard for comparisonof echocardiographic measurements .
MethodsExperimental preparation. Eight mongrel dogs of either
sex weighing between 15 and 30 kg were anesthetized withsodium pentobarbital (30 mg/kg body weight intravenously) , intubated and ventilated with room air. A left thoracotomy was performed through the fifth intercostal spaceand the heart suspended in a pericardial cradle. The leftanterior descending coronary artery just distal to the firstdiagonal branch or the proximal circumflex coronary arterywas isolated from surrounding tissue and encircled with ahydraulic balloon occluder. A Doppler ultrasound flow probewas placed around the artery to be occluded just distal tothe occlusion site. A high fidelity micromanometer (Konigsberg P7) was inserted into the left ventricular cavity througha stab incision at the apex. The first derivative of left ventricular pressure (dP/dt) was obtained by electronic differentiation. Two 10 MHz pulsed Doppler probes were usedfor measurement of regional wall thickening (23) and weresutured to the epicardium overlying the anterior as well asthe posterior left ventricular walls at the level of the midpapillary muscles.
The position of the two Doppler probes in relation tointernal ventricular landmarks was established in vivo withthe use of intraoperative echocardiography as follows: Atwo-dimensional phased array 3.5 MHz transducer was placedinside a sterile Tekna Med Surgiprobe drape (Biosound Inc.)filled with Aquasonic gel and positioned directly on theanterior wall of the heart so as to obtain a short-axis imageof the left ventricle at the level of the midpapillary muscles .The Doppler probes were frequently not seen but their position was noted by visualizing on the image a straighthemostat that was manually placed directly over the probesperpendicular to the external wall of the heart. Care wastaken to avoid placement of the probes directly over the
papillary muscles. The position of the probes was furtherconfirmed at postmortem study by direct examination (seelater). Following instrumentation , the chest was closed, thewires and catheters were tunneled under the skin and exteriorized at the back of the neck . The dogs were allowedat least 10 postoperative days for recovery.
The dogs were trained to lie in the right lateral decubitusposition on a table specially designed with a center cut toallow two-dimensional echocardiographic imaging from theright parasternal window . The experimental design allowedsimultaneous performance of echocardiographic studies andrecording of the following variables on an eight channel,direct writing oscillograph (Gould Brush, System 200): electrocardiogram (ECG), left ventricular pressure and dP/dt,blood flow velocity in the coronary artery to be occludedand wall thickening and range gate depth in the zones to berendered ischemic and nonischemic . No interference between the Doppler signals and echocardiographic imagingwas seen .
Experimental protocol. Light sedation was induced withintravenous diazepam, I to 2 mg/kg, given 30 minute s before each experiment. Each dog underwent up to a total ofthree transient coronary occlu sions (one/week for three consecutive weeks) with random occlusion times of 2.5, 5 or10 minutes followed by reperfusion. The variable durationof coronary occlusion resulted in multiple grades of regionalventricular dysfunction occurring at variable times after reperfusion in accordance with the phenomenon of " myocardial stunning" (24-26) . This protocol , therefore , allowed the investigator measuring the echocardiographicimages to be further blinded as to the level of recovery offunction at a given time after reperfusion.
Recordings of two-dimensional echocardiographic images, regional myocardial thickening with the Doppler probesand hemodynamic variables were obtained at baseline, continuously during occlusion and during the first 5 minutesafter reperfusion. In addition, similar recordings were obtained at the following times after reperfusion: 10, 15, 30,45 and 60 minutes; 1.5 , 2, 3, 4 and 24 hours. At the endof the third coronary occlu sion, the dog was killed and theheart was excised and sectioned in a plane parallel to theatrioventricular groove . The position of the Doppler thickening probes on the epicardium was marked and examinedin relation to internal ventricular landmarks. Myocardialstaining with triphenyltetrazolium chloride demonstrated theabsence of myocardial necrosi s. The myocardial section swere preserved in a 10% buffered formalin solution for laterinspection.
Measurement of wall thickening by the Dopplermethod. Regional wall thickening was measured by thepulsed Doppler epicardial probe method as previously described (23,27,28). In brief, the pulsed Doppler techniqueutilizes a single epicardial ultrasonic crystal to determinemyocardial wall displacement by digitally integrating the

lACC Vol. 10, No.5November 1987:1113-21
ZOGHBI ET AI..END-SYSTOLIC RADIUS TO THICKNESS RATIO
1115
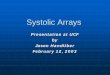
velocity of myocardial layers passing through the range gatesample volume, In contrast to transit time ultrasonic crystals, the Doppler probes are virtually atraumatic becausethey are sutured to the epicardial surface with four 6-0Prolene stitches penetrating 0,5 to I mm in depth, A representative example of simultaneous recording of ECG, leftventricular pressure and dP/dt, mean coronary flow, therange gate depth at the endocardial level and changes inwall thickness in an anterior wall segment is shown in FigureI , End-diastole was defined at the onset of the rapid upstrokeof left ventricular pressure and end-systole at the time ofmaximal myocardial thickening occurring at or within 20ms before peak negative dP/dt (29). Percent myocardialthickening fraction (%TF) was determined as
~Th%TF = -- x 100,
Thed
where ~Th is the change in wall thickness from end-diastoleto end-systole and Thed is the end-diastolic wall thicknessestimated from the Doppler range gate depth (23,27,28). Anegative thickening fraction indicates systolic wall thinning.
Analysis of the Doppler data was performed by one ofthe investigators (M.L.C) before analysis of the echocardiographic images. Measurements were made at baseline,after 2 minutes of coronary occlusion and serially duringreperfusion in five consecutive cardiac cycles showing asignal of good quality and stable sinus rhythm, Results wereexpressed as the average of five cardiac cycles,
Two-dimensional echocardiographic studies and measurements. The studies were performed using a HewlettPackard sector scanner equipped with a 3.5 MHz transducer.Short-axis views at the level of the midpapillary muscleswere obtained from the right parasternal window in the rightlateral decubitus position and recorded on '12 in, (1,27 em)
videotape (VHS format, Panasonic NV 8200). The studieswere later reviewed on an off-line station equipped with asearch module for frame by frame bidirectional playbackand interfaced with an X-Y digitizer (Digisonics EC200),
Echocardiographic measurements were performed by oneof the investigators (W .A.Z.) during baseline, occlusion andreperfusion at specific times assigned by the investigatormeasuring the Doppler recordings (M. L.C) but withoutknowledge of his results. This was performed to match intime the data obtained from both techniques and to reducethe echocardiographic analysis time from what otherwisewould have been overwhelming. During the entire protocol,the time interval between cycles chosen for the determination of thickening fraction and those selected for echocardiographic measurements was <5 seconds. Two echocardiographic variables of regional ventricular function weremeasured from the same cardiac cycles: end-systolic radiusto thickness ratio and radial shortening fraction.
A, End-systolic radius to thickness ratio, End-systolewas defined as the frame showing the smallest left ventricular cavity during frame by frame playback of the selectedcycles, This usually occurred after the peak of the ECG T
ECG
REPERFUSION
i ~
i\i .~ _il }1• ~ I~ - ~- -' .
I- ,. . . .~
t
, .
LAD OCCLUSIONBASELINE
+LV dP /dl 0
RANGE lOtGATE
DEPTH 5(mm) 0
200
tLVP 100(mmHg)
o
CF
(ml /mln)
CHANGE IN tWALL
THICKNESS i(mm) t
ANTERIORWALL
Figure l. Recordings of electrocardiogram(ECG), left ventricular pressure (LVP), meancoronary flow (CF), first derivative of left ventricular pressure (LV dP/dl), range gate depthof the epicardial pulsed Doppler probe positioned at the endocardial level and changes inwall thickness in an anterior wall segment.Systolic wall thickening during baseline is replaced by systolic wall thinning during a 2,5minute left anterior descending (LAD) arteryocclusion followed by reduced thickening lOminutes after reperfusion. The vertical linesin the three panels represent end-diastole andend-systole.

1116 ZOGHBI ET AL.END-SYSTOLIC RADIUS TO THICKNESS RATIO
lACC Vol. 10. No.5November 1987:1113-21
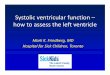
Figure 2. Short-axis end-systolicechocardiographic frames at the levelof the midpapillary muscles duringbaseline (left) and after left anteriordescending (LAD) coronary artery occlusion (right). Theepicardial andendocardial contours used for the determination of radius to thickness ratioare shown. The position of the epicardial (open circle) and endocardial(open triangle) centroids is almostidentical at baseline, whereas duringcoronary occlusion, the endocardialcentroid is shifted towards the thinnerischemic myocardium.
wave. The epicardial contour including the right side of theinterventricular septum and the endocardial contour excluding the papillary muscles were digitized (Fig. 2). The papillary muscles were excluded by extrapolation from the papillary muscle-endocardialjunction in a rather circular outlineparallel to the epicardial border. Twelve equidistant radiiwere derived by computer from the epicardial center ofgeometry or centroid to the digitized endocardial and epicardial contours with the first radius starting at the anterolateral papillary muscle (Fig. 3). The epicardial rather thanthe endocardial centroid was used as reference because it isthe center of gravity of the total cardiac structure at thatparticular short axis level and is less influenced by regionalendocardial motion. Figure 3 illustrates the near identicalposition of the epicardial and endocardial centroids at endsystole during normal myocardial function. However, in thepresence of regional myocardial dysfunction, the endocardial centroid is shifted toward the ischemic and thinnermyocardium, therefore underestimating the change in intracavitary radii in the ischemic zone and overestimatingthe change in radii in the control zone. The ratio of intra-
cavitary radius to wall thickness at end-systole was calculated by computer along each radius.
8 . Radial shortening fraction . The same cardiac cyclesused for the determinationof end-systolic radius to thicknessratio were used to measure intracavitary radial shorteningfraction. The endocardial contour excluding the papillarymuscles was traced at end-diastole in addition to the endocardial contour traced at end-systole. End-diastole wasdefined at the peak of the ECG R wave. Although the reference system for the determination of radial shorteningremains an issue of controversy, recent studies (10,17,30)have demonstrated the superiority of fixed over floatingreferences in the identification of regional ventricular dysfunction. More recently, the endocardial centroid fixed atend-systole was suggested as a better reference and wasused in this study (31). Twelve equidistant radii were derived from the end-systolic endocardial centroid with thefirst radius starting at the anterolateral papillary muscle forboth end-diastole and end-systole. Radial shortening fraction (RSF) was derived along each radius as
Red - ResRSF (%) = d x 100,
ReFigure 3, Schematic end-systolic echocardiographic frames during baseline and left anterior descending (LAD) coronary arteryocclusion. Theepicardial andendocardial left ventricular contoursused for radius to thickness ratio measurements areoutlined. Twelveequidistant radii using the epicardial centroid (open circle) asreference andnumbered clockwise starting at theanterolateral papillary muscle areshown. Notice the larger intracavitary radius (R).reduced myocardial thickness (Th) andthus larger radius to thickness ratio in the ischemic zone during left anterior descendingcoronary occlusion when compared with baseline. Ant = anterior;Lat = lateral; Post = posterior: Sept = septum. Open triangle= endocardial centroid.
BASELINE LAD OCCLUSION
S~POSI
epl
R / -
\ Lat1
Ant
where Red and Res are the radii at end-diastole and endsystole, respectively.
Data analysis. Measurements of end-systolic radius tothickness ratio and radial shortening fraction were performed along all 12 radii. However, only values from radiicorresponding to the position of the Doppler probes in theischemic and nonischemic zones were used for comparisonwith individual thickening fraction determination by theDoppler probes. The location of the two Doppler probesand corresponding radii (one for each probe) was determinedlaterby reviewing the intraoperative echocardiographic studiesand myocardial sections.
To test the ability of echocardiographic variables to differentiate various grades of regional function, the severityof regional dysfunction was classified according to percentchange in Doppler-determined thickening fraction from
lACC Vol. 10, NO.5November 1987:1113-21
ZOGHBI ET AL.END-SYSTOLIC RADIUS TO THICKNESS RATIO
1117
baseline values as: akinesia/dyskinesia (S - 100%), severehypokinesia ( - 99 to -70%), moderate hypokinesia ( - 69to - 40%), mild hypokinesia ( - 39 to - 10%) and recovery(2: - 9%), The results observed within each functional classification were expressed as mean ± SD. Analysis of variance was used to compare results within groups. If the Fvalue was significant, a paired Student's t test was used tocompare results with control values adjusted for the numberof comparisons by the Bonferroni method (32). Correlationbetween echocardiographic and Doppler measurements wasperformed using linear regression analysis.
Interobserver reproducibility. To assess the interobserver reproducibility in the determination of end-systolicradius to thickness ratio and radial shortening fraction, atotal of II cardiac cycles during baseline, occlusion andreperfusion were reanalyzed by an independent experiencedechocardiographer (M.A.Q.). This provided 132 pairedmeasurements of each echocardiographic variable duringvarious states of regional ventricular function. Interobservervariability was expressed as the absolute difference betweenmeasurements by the two observers along the same radius.To permit comparison of the interobserver variability of thetwo echocardiographic variables, a mean percent error ofthe measurements was determined as the absolute differencebetween the two determinations divided by the mean valueof the two observations. This was performed only duringnormal ventricular function (n = 60), that is, baseline andrecovery stages, because during regional dysfunction, radialshortening approaches zero and thus the differences betweenobservations, when expressed as percentage, are magnified (9).
ResultsEight mongrel dogs were chronically instrumented for
occlusion of the left anterior descending or circumflex coronary artery. One dog died 4 days postoperatively and another
was excluded because of malfunctioning epicardial Dopplerprobes. A total of 14 transient coronary artery occlusions(8 left anterior descending, 6 left circumflex) followed byreperfusion were performed in the remaining 6 dogs, resulting in 65 paired echocardiographic and Doppler observations available for comparison. Of these, 14 were obtainedduring baseline, 13 during akinesia/dyskinesia, 4 duringsevere hypokinesia, 10 during moderate hypokinesia, 10during mild hypokinesia and 14 after recovery. After the2.5, 5 and 10 minutes of coronary occlusion, recovery offunction, as defined by the Doppler probes, was achievedat a mean duration of 1.4 ± 0.8, 89.3 ± 73.4 and 169.8± 105.3 minutes after reperfusion, respectively.
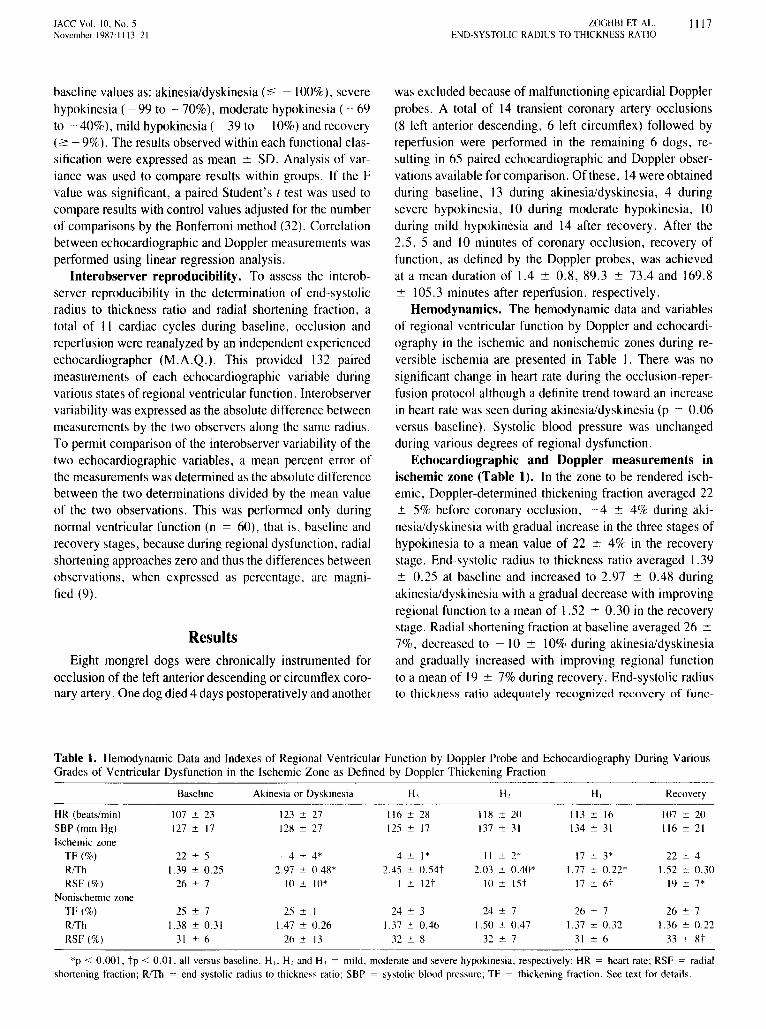
Hemodynamics. The hemodynamic data and variablesof regional ventricular function by Doppler and echocardiography in the ischemic and nonischemic zones during reversible ischemia are presented in Table I. There was nosignificant change in heart rate during the occlusion-reperfusion protocol although a definite trend toward an increasein heart rate was seen during akinesia/dyskinesia (p = 0.06versus baseline). Systolic blood pressure was unchangedduring various degrees of regional dysfunction.
Echocardiographic and Doppler measurements inischemic zone (Table 1). In the zone to be rendered ischemic, Doppler-determined thickening fraction averaged 22± 5% before coronary occlusion, - 4 ± 4% during akinesia/dyskinesia with gradual increase in the three stages ofhypokinesia to a mean value of 22 ± 4% in the recoverystage. End-systolic radius to thickness ratio averaged 1.39± 0.25 at baseline and increased to 2.97 ± 0.48 duringakinesia/dyskinesia with a gradual decrease with improvingregional function to a mean of 1.52 ± 0.30 in the recoverystage. Radial shortening fraction at baseline averaged 26 ±7%, decreased to - 10 ± 10% during akinesia/dyskinesiaand gradually increased with improving regional functionto a mean of 19 ± 7% during recovery. End-systolic radiusto thickness ratio adequately recognized recovery of func-
Table 1. Hemodynamic Data and Indexes of Regional Ventricular Function by Doppler Probe and Echocardiography During VariousGrades of Ventricular Dysfunction in the Ischemic Zone as Defined by Doppler Thickening Fraction
Baseline Akinesia or Dyskinesia H, H, H, Recovery
HR (beats/min) 107 ± 23 123 ± 27 116 ± 28 118 ± 20 113 ± 16 107 ± 20SBP (mm Hg) 127 ± 17 128 ± 27 125 ± 17 137 ± 31 134 ± 31 116 ± 21Ischemic zone
TF(%) 22 ± 5 -4 ± 4* 4 ± 1* II ± 2* 17 ± 3* 22 ± 4R/Th 1.39 ± 0.25 2.97 ± 0.48* 2.45 ± 0.54t 2.03 ± 0.40* 1.77 ± 0.22* 1.52 ± 0.30RSF(%) 26 ± 7 -10 ± 10* 1 ± 12t 10 ± 15t 17 ± 6t 19 ± 7*
Nonischemic zoneTF(%) 25 ± 7 25 ± I 24 ± 3 24 ± 7 26 ± 7 26 ± 7R/Th 1.38 ± 0.31 1.47 ± 0.26 1.37 ± 0.46 1.50 ± 0.47 1.37 ± 0.32 1.36 ± 0.22
RSF(%) 31 ± 6 26 ± 13 32 ± 8 32 ± 7 31 ± 6 33 ± 8t
*p < 0.001, tp < 0.01, all versus baseline. H,; H, and H, = mild, moderate and severe hypokinesia, respectively; HR = heart rate; RSF = radialshortening fraction; R/Th = end-systolic radius to thickness ratio; SBP = systolic blood pressure; TF = thickening fraction. See text for details.

1118 ZOGHBI ET AL.END-SYSTOLIC RADIUS TO THICKNESS RATIO
lACC Vol. 10. NO.5November 1987:1113-21
Figure 4. Correlations in the ischemic zone duringreversible myocardial ischemia among percent thickening fraction bytheDoppler probe, echocardiographicend-systolic radius to thickness (RlTh) ratioand radialshortening fraction. Absolute values are shown in theupper panels and percent change from baseline measurements (% Il) in the lower panels. The solid linerepresents the lineof regression and the dashed linesrepresent the 95% confidence limits. The dotted linerepresents the inverse identity linein theleft panel andthe line of identity in the right panel. Closed circles= left anterior descending artery occlusion; open circles = circumflex artery occlusion .
•
40,......----------,
30
20
10
o-10
- 20 L...-..........&..........--l.--'''--.L--............
-30-20-10 0 10 20 30 40 50Radial Shortening Fraction (%)
-200 '---'--......--''--.......-~-.I-250-200-150-100 -50 0 50% 4 Radial Shortening Fraction
50
o-50
-100
-150
• y:-13. + 39,:-.83; SEE:6%
1.5 2 2.5 3 3.5 4 4.5End-systolic R/Th
............ y:-.88. - 5o ......... ':-.86: SEE:25%
a.......Cl ......
... ...o ............
:'"
o 50 100 150% 4 End-systolic R/Th
•<,..............
<,Ii? ."?..... 0
'-'...... -;
<, .
;f. 40e 30.2U 20III..~ 10enc 0'cGI -10~ez -20~
.5
c.2U 50III..~
0ene
-50'cGI~ -100u:c~ -150<I
;f.-200
-50
tion in contrast to radial shortening measurements, whichremained significantly decreased in the recovery stage whencompared with baseline values (p < 0.001).
In the ischemic zone, a significant linear correlation wasobserved between thickening fraction measurements by theDoppler probe and echocardiographic determinations of endsystolic radius to thickness ratio and radial shortening fraction (r = -0.83 and 0.75 respectively; n = 65) (Fig. 4).More importantly, percent change in thickening fractionfrom baseline values correlated significantly with percentchange in radius to thickness ratio (r = - 0.86) better thanwith percent change in radial shortening fraction (r = 0.78)with a regression equation closer to the respective identityline (Fig. 4). Similar correlations were observed when thedata obtained after occlusion and reperfusion of the left
anterior descending and left circumflex coronary arterieswere analyzed separately.
Measurements in the nonischemic zone (Table 1).Thickening fraction by the Doppler probe, end-systolic radius to thickness ratio and radial shortening fraction averaged 25 ± 7, 1.38 ± 0.31 and 31 ± 6%, respectively atbaseline. No significant change occurred in Doppler-determined thickening fraction or end-systolic radius to thicknessratio during reversible ischemia of the opposite region.However, a significant increase in radial shortening fractionoccurred during the recovery stage compared with baseline.
Sensitivity and specificity of method (Table 2). Toassess the sensitivity and specificity of end-systolic radiusto thickness ratio and radial shortening as indexes of regionalfunction, a 95% confidence interval was constructed for each
Table 2. Comparative Echocardiographic Assessment of Regional Left Ventricular Function byEnd-Systolic Radius to Thickness Ratio and Radial Shortening Fraction
Akinesia or Dyskinesia H3 H2 H, Recovery
End-systolic R/ThNo. of radii*
Range 4 to 9 2 to8 2 to 7 I to5 I to 3Mean 5.8 4.3 4.0 2.8 1.7
Sensitivity (%) 13 of 13 (100) 4 of4 (100) 8 of 10 (80) 5 of 10 (50)Specificity (%) II of 14 (79)
Radial shorteningfraction
No. of radiitRange 5 to 8 4 to6 I to6 1 to4 I to 2Mean 6.6 5.5 3.5 2.4 1.5
Sensitivity (%) 13 of 13 (100) 4 of4 (100) 9 of 10 (90) 7 of 10 (70)Specificity (%) 10 of 14 (71)
*Number of abnormal radii above the normal 95% confidence limits of end-systolic radius to thickness(RlTh) ratio. tNumber ofabnormal radii below the normal 95% confidence limits ofradial shortening fraction.Abbreviations as in Table I.

lACC Vol. 10, No.5November 1987:1113-21
ZOGHBI ET AL.END-SYSTOLIC RADIUS TO THICKNESS RATIO
1119
Figure 5. Exampleof the changes in end-systolic radius to thicknessratioalongall 12radiiafter transientocclusionof a leftanteriordescendingor a left circumflex coronary artery. The normal 95%confidence limits for end-systolic radius to thickness ratio (R/Th)along the 12 equidistant radii are shown in the shaded area.Regional function is assessed by the Doppler probes (see text). Asignificant increase in radius to thickness ratio occurred in theischemic zone during occlusion (ace). Note the gradual decreasein magnitude of end-systolicradius to thicknessratio and concomitant decrease in the number of radii above the 95% confidencelimits in the ischemic zone occurring with gradual improvementin regional ventricular function. HI = mild hypokinesia; H3 =severe hypokinesia; R = recovery. Other abbreviations as in Figure 3.
echocardiographic method from baseline measurements alongeach of the 12 radii. Analysis of variance demonstrated asignificant heterogeneity in end-systolic radius to thicknessratio and radial shortening among the 12 radii (p < 0.01).An example of the changes in end-systolic radius to thickness ratio along all radii after occlusion and reperfusion ofa left anterior descending and a left circumflex coronaryartery is shown in Figure 5. For the end-systolic radius tothickness ratio, regional function was considered abnormalif at least one end-systolic radius to thickness ratio measurement exceeded the 95% confidence limit. Similarly,regional function was considered abnormal if at least oneradial shortening fraction measurement was below its 95%confidence limit. During periods of akinesia or dyskinesiaas measured by the Doppler probes, the number of abnormalradii in the ischemic region identified by the end-systolicradius to thickness ratio and radial shortening fraction averaged 5.8 and 6.6 radii, respectively. A gradual decreasein the number of abnormal radii was seen with both methodsduring recovery of function after reperfusion. For all cardiaccycles studied, the sensitivity of both methods was 100%for akinetic, dyskinetic or severely hypokinetic segments asassessed by the Doppler probes. The sensitivity of the radiusto thickness ratio method for moderate and mild hypokinesiawas 80 and 50%, respectively, whereas it was 90 and 70%.respectively, for the radial shortening method. The overallsensitivity and specificity of end-systolic radius to thickness
1 2 3 4 5 6 7 8 9101112 1 2 3 4 5 6 7 8 9101112
Radius Number
Discussion
Current methodology: advantages and limitations.Quantitation of regional myocardial function has generallyinvolved measurements of either endocardial excursion ormyocardial thickening from end-diastole to end-systole. Eachof these approaches has its advantages and limitations. Although the endocardial border is more easily defined thanthe epicardial border, measurements of endocardial motionare limited by the influence of cardiac translation, rotationand respiratory movements and the need for a yet unsettledreference system (8-10,14,16-19). In contrast, measurements of myocardial thickening are less dependent on cardiac motion but their accuracy depends on having excellentepicardial and endocardial definition during both diastoleand systole.
Evaluation of echocardiographic methods for the quantitation of regional ventricular function has been predominantly performed using models of severe or total coronaryocclusion resulting in severe dysfunction of the involvedsegments, that is, akinesia or dyskinesia (8,11,12,16). Thus,the accuracy of these methods has not been adequately testedin lesser degrees of regional dysfunction. Furthermore, thesemethods have rarely been validated against an independentquantitative standard for the determination of regional myocardial performance (11,12).
The present study demonstrates that regional end-systolicradius to thickness ratio is an index of regional function thatadequately differentiates grades of dysfunction produced byreversible ischemia. Although the sensitivity and specificityof this index for regional dysfunction were similar to thoseof radial shortening, the index more accurately quantitated
ratio for detecting regional dysfunction was 81 and 79%,respectively and 89 and 71%, respectively, for the radialshortening method.
Hyperkinesia was defined as a measurement below the95% confidence limit for radius to thickness ratio or abovethe 95% confidence limits for radial shortening fraction.Using the radius to thickness ratio, hyperkinesia was seenin only three cardiac beats during occlusion and reperfusioninvolving a maximum of two radii only in the control regionas opposed to six cardiac beats involving up to six radiiusing the radial shortening method.
Interobserver reproducibility. The interobserver reproducibility in 132 determinations of end-systolic radiusto thickness ratio and radial shortening fraction during various stages of regional dysfunction expressed as the absolutedifference between observations was (mean ± SO) 0.24 ±0.19 and 6 ± 6%, respectively. The mean percent errorbetween the two observers for measurements of end-systolicradius to thickness ratio and radial shortening fraction duringnormal ventricular function (n = 60) was 16 ± II and 17± 15%, respectively.
H,R
H,
Oee
CIRCUMFLEX
Ant Sep Post LatAnt Sep Post Lat
3.5 Oce
.5
LEFT ANTERIOR DESCENDING
s:I-~,2 2.5
:2III>IIII 1.5
"CI<::W

1120 ZOGHBI ET AL.END-SYSTOLIC RADIUS TO THICKNESS RATIO
lACC Vol. 10. No.5November 1987:1113-2\
the change in regional function as assessed by the Dopplerprobes and thus may be better suited for the serial assessmentof regional ventricular performance. Measurements of radialshortening in this preparation overestimated the change inregional function in the ischemic zone and did not accuratelyrecognize complete recovery of function. This is likely secondary to the inability of radial shortening to correct forcardiac motion so that function is overestimated in the nonischemic zone and underestimated in the ischemic zone.
Advantages and limitations of the end-systolic radiusto thickness ratiomethod. The end-systolic radius to thickness ratio offers several potential advantages over otherechocardiographic methods for assessing regional function.Because this index involves end-systolic measurements froma single frame only, it obviates the need for correction ofcardiac translation and rotation, which has limited otherquantitative methods requiring end-diastolic and end-systolic measurements. In addition, two-dimensional echocardiographic frames during systole frequently have better qualityof epicardial and endocardial definition and less echo dropout than do diastolic frames. Moreover, only two contoursare needed for measurements (epicardial and endocardial atend-systole) as opposed to four ventricular contours requiredfor the determination of thickening fraction, thus reducingthe opportunity for errors during measurements. The predominant sources of error arise from tracing the epicardialand endocardial contours because the epicardial center ofgeometry and radius to thickness measurements are derivedautomatically by the computer.
Determination of left ventricular wall stress, using amodification of the Laplace equation, usually involves multiple geometric assumptions and is proportional to the product of ventricular pressure and the ratio of ventricular radiusto wall thickness (22,33-36). The end-systolic radius tothickness ratio described in this study, when combined withdetermination of ventricular pressure, may provide an indexproportional to end-systolic regional wall stress. Becausesystolic ventricular pressure was not significantly alteredduring the occlusion-reperfusion protocol, the serial endsystolic radius to thickness ratio plots shown in Figure 5may be proportional to changes in regional end-systolicstress. However, the major difference between this and previous methods is that the radii arise from the epicardialcentroid and may be different from measurements of minorsemiaxes of the ventricle, especially in situations of regionaldysfunction. Further studies are required to determine whetherend-systolic regional wall stress can be derived with theradius to thickness ratio as measured in this study.
A potential limitation of regional end-systolic radius tothickness ratio resides with the definition ofend-systole. Weelected to use a global definition based on the smallest leftventricular cavity size because it allowed selection of onlyone frame for measurements and obviated the limitationsimposed by cardiac motion on the reference system. Because
of temporal heterogeneity in regional contraction which maybecome accentuated during ischemia, it is likely that maximal systolic thickening occurred in some ventricular segments at a time different from the frame showing the smallest cavity size. This problem probably limited the correlationbetween end-systolic radius to thickness ratio and Dopplerthickening fraction because maximal reduction in cavity sizeechocardiographically may have been off by a few milliseconds in time from end-systole as defined with the Dopplermethod. A more accurate measurement of regional endsystolic radius to thickness ratio requires frame by framemeasurements throughout systole to plot the time course ofregional thickening and intracavitary radial shortening fromwhich maximal regional contraction could be identified.Such an approach, although theoretically more accurate,would be clinically less appealing because it would bringback the limitations discussed previously for measurementsof regional thickening and endocardial motion. The resultsobserved with the simplified "one-frame" end-systolic methodin our model of reversible ischemia appear to be accurateenough to warrant clinical trial.
We acknowledge the expertise of Almanubia Cespedes in the preparation
of the manuscript.
Referencesl. Kisslo lA, Robertson D, Gilbert BW, vonRamm 0, Behar VS. A
comparison of real-time, two-dimensional echocardiography and cineangiography in detecting left ventricular asynergy. Circulation 1977;55:134-41.
2. Heger JJ, Weyman AE, Wann LS, Dillon lC, Feigenbaum H. Crosssectional echocardiography in acute myocardial infarction: detectionand localization of regional left ventricular asynergy. Circulation 1979;60:531-8.
3. Heger JJ, Weyman AE, Wann LS, Rogers EW, Dillon lC, Feigenbaum H. Cross-sectional echocardiographic analysis of the extent ofleft ventricular asynergy in acute myocardial infarction. Circulation1980;61: 1113-8.
4. Nixon lV, Narahara KA, Smitherman TC. Estimation of myocardialinvolvement in patients with acute myocardial infarction by two-dimensional echocardiography. Circulation 1980;62: 1248-55.
5. Visser CA, Lie KI, Kan G, Meltzer R, Durrer D. Detection andquantification of acute, isolated myocardial infarction by two dimensional echocardiography. Am 1 Cardiol 1981;47:1020-5.
6. Wyatt HL, Meerbaum S, Heng MK, Rit r, Gueret P, Corday E.Experimental evaluation of the extent of myocardial dyssynergy andinfarct size by two-dimensional echocardiography. Circulation 1981;63:607-14.
7. Horowitz RS, Morganroth J, Parrotto C, Chen CC, Soffer 1, PauleItoFl. Immediate diagnosis of acute myocardial infarction by two-dimensional echocardiography. Circulation 1982;65:323-9.
8. Lieberman AN, Weiss JL, Jugdutt BI, et at. Two-dimensional echocardiography and infarct size: relationship of regional wall motion andthickening to the extent of myocardial infarction in the dog. Circulation1981;63:739-46.
9. Moynihan PF, Parisi AF, Feldman CL. Quantitative detection of regional left ventricular contraction abnormalities by two-dimensionalechocardiography. I. Analysis of methods. Circulation 1981;63:752-60.

JACC Vol. 10, NO.5November 1987:1 J 13-21
ZOGHBI ET AL.END-SYSTOLIC RADtUS TO THICKNESS RATIO
1121
10. Parisi AF, Moynihan PF, Folland ED, Feldman CL. Quantitativedetection of regional left ventricular contraction abnormalities by twodimensional echocardiography. II. Accuracy in coronary artery disease. Circulation 1981;63:761-7.
II. Pandian NG, Kerber RE. Two-dimensional echocardiography in experimental coronary stenosis. I. Sensitivity and specificity in detectingtransient myocardial dyskinesia: comparison with sonomicrorneters.Circulation 1982;66:597-602.
12. Pandian NG, Kieso RA, Kerber RE. Two-dimensional echocardiography in experimental coronary stenosis. II. Relationship betweensystolic wall thinning and regional myocardial perfusion in severecoronary stenosis. Circulation 1982;66:603-11.
13. Nieminen M, Parisi AF, O'Boyle JE. Folland ED. Khuri S. KlonerRA. Serial evaluation of myocardial thickening and thinning in acuteexperimental infarction: identification and quantification using twodimensional echocardiography. Circulation 1982;66: 174-80.
14. O'Boyle lE, Parisi AF, Nieminen M. Kloner RA. Khuri S. Quantitative detection of regional left ventricular contraction abnormalitiesby 2-dimensional echocardiography: comparison of myocardial thickening and thinning and endocardial motion in a canine model. Am JCardiol 1983;51: 1732-8.
15. VanReet RE, Quinones MA. Poliner LR. et al. Comparison of twodimensional echocardiography with gated radionuclide ventriculography in the evaluation of global and regional left ventricular functionin acute myocardial infarction. J Am Coli Cardiol 1984:3:243-52.
16. Gillam LD, Hogan RD, Foale RA, et al. A comparison of quantitativeechocardiographic methods for delineating infarct-induced abnormalwall motion. Circulation 1984;70: 113-22.
17. Schnittger I, Fitzgerald PJ, Gordon EP, Alderman EL, Popp RL.Computerized quantitative analysis of left ventricular wall motion bytwo-dimensional echocardiography. Circulation 1984;70:242-54.
18. Haendchen RV, Wyatt HL, Maurer G, et al. Quantitation of regionalcardiac function by two-dimensional echocardiography. I. Patterns ofcontraction in the normal left ventricle, Circulation 1983:67: 1235-45.
19. Pandian NG, Skorton DJ, Collins SM, Falsetti HL. Burke ER, KerberRE, Heterogeneity of left ventricular segmental wall thickening andexcursion in 2-dimensional echocardiograms of normal human subjects. Am J CardioI1983;51:1667-73.
20, Gaasch WHo Left ventricular radius to wall thickness ratio. Am JCardiol 1979;43: 1189-94,
21. Kurnpuris AG, Quinones MA, Waggoner AD, et al. Importance ofpreoperative hypertrophy, wall stress and end-systolic dimension asechocardiographic predictors of normalization of left ventricular dilatation after valve replacement in chronic aortic insufficiency. Am JCardiol 1982;49: 1091-100.
22. Osakada G, Hess OM, Gallagher KP, Kemper WS. Ross J Jr. Endsystolic dimension-wall thickness relations during myocardial isch-
ernia in conscious dogs, A new approach for defining regional function. Am J Cardiol 1983;51:1750-8,
23. Hartley CJ, Latson LA. Michael LH, Seidel CL, Lewis RM, EntmanML. Doppler measurement of myocardial thickening with a singleepicardial transducer. Am J Physiol 1983;245:H 1066-72.
24. Braunwald E. Kloner RA. The stunned myocardium: prolonged. postischemic ventricular dysfunction, Circulation 1982;66: 1146-9.
25. Heyndrickx GR. Millard RW. McRitchie RJ, Maroko PR, Vatner SF.Regional myocardial functional and electrophysiologic alterations afterbrief coronary occlusion in conscious dogs, J Clin Invest 1975;56:978-85,
26, Theroux P, Ross J, Franklin 0, Kemper WS, Sasayama S. Regionalmyocardial function in the conscious dog during acute coronary occlusion and responses to morphine. propranolol, nitroglycerin andlidocaine. Circulation 1976;53:302-14.
27. lhu WX, Myers ML, Hartley CJ. Roberts R, Bolli R. Validation ofa single crystal for measurement of transmural and epicardial thickening. Am J Physiol 1986;251:HI045-55.
28. Myers ML. Bolli R. Lekich RF. Hartley CJ. Roberts R. Enhancementof recovery of myocardial function by oxygen free-radical scavengersafter reversible regional ischemia. Circulation 1985;72:915-21.
29. Gallagher KP. Kumada T. Koziol JA. McKown MD, Kemper WS.Ross J Jr. Significance of regional wall thickening abnormalities relative to transmural myocardial perfusion in anesthetized dogs. Circulation 1980;62: 1266-74.
30. Fujii 1, Sawada H, Aizawa T. Kato K, Onoe M. Kuno Y. Computeranalysis of cross sectional echocardiogram for quantitative evaluationof left ventricular asynergy in myocardial infarction. Br Heart J 1984;51:139-41.
31. Wiske PS. Gillam LD. Hogan RD, ct al. Two-dimensional echocardiographic definition of the systolic left ventricular centroid (abstr). JAm Coli Cardiol 1985;5:424.
32. Wallenstein S, Zucker CL. Fleiss JL. Some statistical methods usefulin circulation research. Circ Res 1980;47: 1-9.
33. Sandler H, Dodge HT. Left ventricular tension and stress in man. CircRes 1963;13:91-104.
34. Hood WP. Rackley CEo Rolett EL. Wall stress in the normal andhypertrophied human left ventricle. Am J Cardiol 1968;22:550-8.
35. Bums JW. Covell JW. Myers R. Ross J Jr. Comparison of directlymeasured lett ventricular wall stress and stress calculated from geometric reference figures. Circ Res 1971;28:611-21.
36. Quinones MA. Mokotoff OM. Nouri S. Winters WL Jr. Miller RR.Noninvasive quantification of left ventricular wall stress: validationof method and application to assessment of chronic pressure overload.Am J Cardio! 1980;45:782-90.