Embed Size (px)
Citation preview

بسم الله الرحمن الرحيمWorking Length Determination, Endodontic Radiology
Today we will talk about working length determination , radiology in endodontic , why we need to have working length and why it’s important.
We will know all of these things in today’s lecture.
We will not be able to do any proper work in endodontic if you don’t know 1- where you are working 2- how long you need to go deep into the canal
S0 at first we need to have a reference point to measure the distance , the reference point should be stable.
Stable reference point means that it doesn’t have undermined caries which may affect this point so it will be lost in the next visit [ so you will lose it and you have to start again ] .
USUALLY , the reference point for : anterior teeth is the incisal edge
Posterior teeth is tip of the cusp
*You should record your reference point location and mark the working length on the file.
•Optimal length
Usually , the opening or the orifice of the canal doesn’t locate exactly at the tip of the root , so if you have a radiograph you measure the length of the tooth from the incsial edge to the radiographic apex [ anatomical apex ] this will be the length of the tooth .
1 | P a g e

If we calculate the location of the orifice where it locates , usually it is up to 2mm from the anatomical apex.
SO >> if we find out that our working length is 22mm when measure it on the radiograph , we should subtract 2mm and we will work on 20mm.
The length that we should work on it = working length – 2mm
There are some terms that you will get in contact while you are working in root canal .
FIRST The apical foramen : as we said before it isn’t always on the tip of the root so it could be on the side.
THEN Anatomical apex : which is the final end of the root or the tip of the root.
Apical construction : you will see what do we mean by apical construction
As you see in fallowing picture :
Anatomical apex
2 | P a g e

If we said that our working length will start from the anatomical apex this will be mistaken ; because when we insert our files into the canal we will be pushing infected materials and necrotic tissues beyond the true apex , so we should confined our instrumentation into the canal space only.
Theoretically we said that we need to end our preparation to the apical constriction but it is not always present , however we need to finish our opturation at this point to get safety distance not to push infected material beyond the apex.
First of all as we said before , we should have a pre-operative radiograph which one of its uses to estimate the working length and as we said we should subtract 2mm ( 1mm for apical constriction and the other 1mm for magnification error )
Once you measure the length of this tooth , you take a file which can go easily into the canal passively and you mark the length that you measured using the ruler.
( ●ex : if you measure the length of central incisor and it was 22mm ,so you need to : • mark the file using a rubber stopper which comes with the file [ yellow in color ]. • slide the rubber stopper down to 20mm length.• insert the file into the canal.• let the rubber stopper seat physically on your reference point [ to be in touch physically with your reference point ].
3 | P a g e

This is film hogar [sry I’m not sure of the spelling ] which especially used in endodontic , it has empty pops inside.
Rubber stopper
To obtain accurate measurements of your working length , we need to take radio graph after inserting the file into the tooth to make sure of our measurements.
for our measurements on the x-ray film to be reliable we should use the minimum file size .
•the minimum size of the file for working length determination should be 20 ( because the tip of the file beyond or smaller than this will not appear in the radio graph specially in anterior teeth ) .
We said before that we have to place the rubber dam on the tooth before inserting any file.
It is imperative that the rubber dam be left in place during working length determination to ensure an aseptic environment and to protect the patient from swallowing or aspirating instruments.
4 | P a g e

●There is something called paralleling technique in taking radio graphs we use it in endodontic to make the length of the tooth near accurate on the film and to make everything on the tooth clear.
In order to see the whole structure or all root length , the film should cross or beyond the opposite of the midline of the map.**(I couldn’t understand this point , go back to the record may you understand it !!)**
The beam should strike the long access of the tooth in a right angle (90 degrees )
If we place the film near to the tooth not beyond the midline , the palatal root will not appear on the film , so we want the film to be after the midline
After we took the estimated working length , inserted the file into the canal & took a radio graph we need to look and measure and see where does the tip locate.
• If it’s longer than apical constriction we need to estimate or calculate how much it’s longer and correct it.
[ we need to calculate and measure how much the difference from the anatomical apex , If it’s 1mm for example we add or subtract according to the condition )
• If the difference more than 3mm , we need to take another radio graph.
5 | P a g e

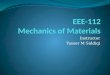
This picture shows the variations in the calculations of corrected working length according to the condition of the apical area
So , if we have any kind of bone resorption but there is no apical resotption => we subtract 1.5 instead of 1
But if there is bone resorption as well as apical resorption=>we subtract 2
sometimes we have some causes that prevent us from taking a radio graph and we can’t proceed doing RCT without knowing the working length , So what we have to do ?
There is something called apex locator this is a new technology that was found to tell us where is the apex of that canal and most of the time it is really accurate , but we can’t rely on this device only.
So , however you took the reading by the apex locator , you need to confirm it with radio graph.
6 | P a g e

They say that there are some contraindications of using the apex locator because it uses electrical signals that may affect patients with cardiac pacemakers. [ it’s not true all the time ]
IMPORTANCE OF RADIOGRAPHY IN ENDODONTI
endodontic radiology needs kind of modification or manipulation of instruments or the beam .
Radiographs perform essential functions in three areas. However, they have limitations that require special approaches.
A single radiograph is a 2-dimensional shadow of a 3-dimensional object.
For maximum information, the third dimension must be visualized and interpreted.
The three general areas of application are :
- diagnosis ( Root and pulp anatomy , Identifying Pathosis & Characterizing normal structures. )
-treatment ( Determinig working length , Moving superimposed structure Locating canals & Evaluating obturation )
- recall ( Identifying new pathosis & Evaluating Healing )
7 | P a g e

In the two pictures above :Pic (A) this radio graph was taken in 90 degrees , so you will see two canals but there is a shadow for another root .
Pic (B) this is when we took another radio graph with mesial angulations 20 degrees , we saw the mesiobuccal canal which is arrowed by red.
A this is a premolar where you can see a large radiolucency in the center which refers to ( pulp tissue ) and then suddenly this radiolucency will break and become narrow which means a bifurcation area at that part (another root) So >> you need to take another radio graph with an angulations in order to separate these two objects from each other and to measure them.
8 | P a g e

Bthe same tooth but the x-ray was taken from the mesial side but in the patient’s mouth we can’t take it mesial because there is another tooth.So this radio graph to show the deference between radio graph according to the side the it was taken from it.
when two objects and the film are in a fixed position and the radiation source (cone) is moved, images of both objects move in the opposite direction.
So , they discover a rule which is called Slob Rule
Slob Rule means when you see the two canals in the film [ assuming that the tooth is upper and the radio graph was taken mesially ] The mesial canal on the film is the lingual canal on the tooth The opposite one will be buccal
In the above picture : Central (x-ray) beam passing directly through a root containing two canals
will superimpose the canals on the film. When the cone is shifted to the mesial or distal aspect, the lingual object
will move in the same direction as the cone; the buccal object will move in the opposite direction (SLOB rule).
9 | P a g e

A here we can’t see separated apex , but when we shift it mesially it appears as two different tips
In the lower we always do distal shift *but anterior of the lower we do mesial shift
In the upper we always do mesial shift
Canine right angle Premolars mesial shift (20 degrees)Molars distal shift (20 degrees)
10 | P a g e

THE HAPPY END
PLEAS GO BACK TO THE SLIDES.
for give me for any mistake
Done By :
11 | P a g e

GaYda’a Kana’an
12 | P a g e