Embed Size (px)
DESCRIPTION
endocryn system
Citation preview

10
The Endocrine System 87
The Endocrine SystemThe endocrine system provides long-term regula-tion and adjustment of homeostatic mechanismsand a variety of body functions. For example, theendocrine system is responsible for the regulationof fluid and electrolyte balance, cell and tissuemetabolism, growth and development, and repro-ductive functions. The endocrine system alsoassists the nervous system in responding to stress-ful stimuli.
The endocrine system is composed of ninemajor endocrine glands and several other organs,such as the heart and kidneys, that have otherimportant functions. The hormones secreted bythese endocrine organs are distributed by the circu-latory system to target tissues throughout the body.Each hormone affects a specific set of target tissuesthat may differ from that of other hormones. Theselectivity is based on the presence or absence ofhormone-specific receptors in the cell membrane,cytoplasm, or nucleus of the target cells.
Homeostatic regulation of circulating hormonelevels primarily involves negative feedback controlmechanisms. The feedback loop involves an inter-play between the endocrine organ and its target tis-sues. Release of a particular hormone by anendocrine gland may occur in response to one ofthree different types of stimuli:
1. Some hormones are released in response tovariations in the concentrations of specific sub-stances in the body fluids. Parathyroid hor-mone, for example, is released when calciumlevels decline.
2. Some hormones are released only when thegland cells receive hormonal instructions fromother endocrine organs. For example, the rateof production and release of T3 and T4 by thethyroid gland is controlled by thyroid stimulat-ing hormone (TSH) from the anterior pituitarygland. The secretion of TSH is in turn regulatedby the release of thyrotropic releasing hormone(TRH) from the hypothalamus.
3. Some hormones are released in response toneural stimulation. The release of epinephrineand norepinephrine from the adrenal medulladuring sympathetic activation is an example.
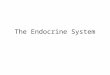
Endocrine disorders can therefore develop due toabnormalities in (a) the endocrine gland, (b) theendocrine or neural regulatory mechanisms, or (c) thetarget tissues. Figure A-33 provides an overview ofthe major classes of endocrine disorders. In the dis-cussion that follows, we will use the thyroid glandas an example because the text introduces majortypes of thyroid gland disorders. These primary dis-orders may result in overproduction (hypersecre-tion) or underproduction (hyposecretion ofhormones. For example, clinicians may categorize athyroid disorder as primary hyperthyroidism or pri-mary hypothyroidism if the problem originates with-in the thyroid gland.
1. Many endocrine disorders are the result ofproblems within the endocrine gland itself.Causes of hyposecretion include the following:
• Metabolic factors: Hyposecretion may resultfrom a deficiency in some key substrateneeded to synthesize that hormone. Forexample, hypothyroidism can be caused byinadequate dietary iodine levels or exposureto drugs that inhibit iodine transport orutilization at the thyroid gland.
• Physical damage: Any condition that inter-rupts the normal circulatory supply orthat physically damages the endocrinecells in some other way will suppress hor-mone production temporarily. If the dam-age is severe, the condition may bepermanent. Examples of problems thatmay cause temporary or permanenthypothyroidism include infection orinflammation of the gland (thyroiditis),interruption of normal circulation, andexposure to radiation as part of treatmentfor cancer of the thyroid or adjacent tis-sues. The thyroid may also be damaged inan autoimmune disorder that results in theproduction of antibodies that attack anddestroy normal follicle cells.
• Congenital disorders: The individual may beunable to produce normal amounts of aparticular hormone because (a) the glanditself is too small, (b) the required enzymesare abnormal in some way, or (c) the glandcells lack the receptors normally involved instimulating secretory activity.
2. Endocrine disorders can also result from prob-lems with other endocrine organs involved inthe negative feedback control mechanism. Forexample:
• Secondary hypothyroidism can be causedby inadequate TSH production at the pitu-itary gland or by inadequate TRH secretionat the hypothalamus.
• Secondary hyperthyroidism can be causedby excessive TRH or TSH production; sec-ondary hyperthyroidism may develop inindividuals with tumors of the pituitarygland.
3. Endocrine abnormalities can also be caused bythe presence of abnormal hormonal receptors intarget tissues. In this case the gland and theregulatory mechanisms may be normal, but theperipheral cells are unable to respond to the cir-culating hormone. The best example of this typeof abnormality is type 2 diabetes (maturity-onset, NIDDM), where peripheral cells do notrespond normally to insulin. (Maturity-onsetdiabetes is discussed further on p. 92.)
Endocrine.eap3am 8/20/02 3:41 PM Page 87

10
88 The Body Systems: Clinical and Applied Topics
THE SYMPTOMS OFENDOCRINE DISORDERSKnowledge of the individual endocrine organs andtheir functions makes predictions possible aboutthe symptoms of specific endocrine disorders. Forexample, thyroid hormones increase basal meta-bolic rate, body heat production, perspiration, rest-lessness, and heart rate. An elevated metabolicrate, increased body temperature, weight loss, ner-vousness, excessive perspiration, and an increasedor irregular heartbeat are common symptoms ofhyperthyroidism. On the other hand, a low meta-bolic rate, decreased body temperature, weightgain, lethargy, dry skin, and a reduced heart rateoften accompany hypothyroidism. The symptomsassociated with over- and under-production ofmajor hormones are summarized in Table A-19.
The Diagnosis of Endocrine DisordersThe first step in the diagnosis of an endocrine dis-order is the physical examination. Several disor-ders produce characteristic physical signs thatreflect abnormal hormone activities. Several exam-ples were introduced in the text:
• Cushing’s disease results from an oversecre-tion of glucocorticoids by the adrenal cortex. Asthe condition progresses there is a shift awayfrom the normal pattern of fat distribution inthe body. Adipose tissue accumulates in theabdominal area, the lower cervical area (caus-ing a “humpback”), and in the face, but theextremities become relatively thin.
• Acromegaly results from oversecretion ofgrowth hormone in the adult. In this conditionthe facial features become distorted due toexcessive cartilage growth, and the lower jawprotrudes, a sign known as prognathism. Thehands and feet also become enlarged.
• Adrenogenital syndrome results from the over-secretion of androgens by the adrenal glands ofa female. Hair growth patterns change, and thecondition of hirsutism (p. 45) develops.
• Hypothyroidism due to iodine deficiency pro-duces a distinctively enlarged thyroid gland, orgoiter.
• Hyperthyroidism can produce protrusion of theeyes, or exophthalmos.
GigantismAcromegalyPituitary growth failure
Primary effects on metabolism
Primary effects on growth
Primary effects on reproductive function
Precocious pubertyAdrenogenital syndromeGynecomastia
Primary effects on fluid and electrolyte balance
Addison’s diseaseHypoaldosteronismDiabetes insipidusSyndrome of inappropriate ADH secretion (SIADH)HyperparathyroidismHypoparathyroidism
Effects on cardiovascular function
Addison’s disease (produces hypotension)Hyperthyroidism (increases heart rate; arrhythmias)Pheochromocytoma (produces hypertension)Diabetes mellitus
ENDOCRINEDISORDERS
Glucose metabolism: Addison’s disease Cushing’s disease Diabetes mellitus
Metabolic rate abnormalities: Hyperthyroidism Hypothyroidism Cretinism
Figure A-33 Disorders of the Endocrine System
Endocrine.eap3am 8/20/02 3:41 PM Page 88

10
The Endocrine System 89
Table A-19 Clinical Implications of Endocrine Malfunctions
Under- Over-production Principal production Principal
Hormone Syndrome Signs & Symptoms Syndrome Signs & Symptoms
Growth hormone Pituitary Retarded growth, Gigantism, Excessive growth(GH) growth abnormal fat acromegaly
failure distribution, low (pituitary blood glucose dwarfism) hours after a meal
Antidiuretic Diabetes Polyuria, dehydration, SIADH (syndrome Increased body hormone (ADH) insipidus thirst of inappropriate weight and
ADH secretion) water contentThyroxine (T4), Myxedema, Low metabolic rate and Hyperthyroidism, High metabolic
triiodothyronine cretinism body temperature; Graves’ disease rate and body (T3) impaired physical temperature
and mental development
Parathyroid Hypopara- Muscular weakness, Hyperparathyroidism Neurological, mental, hormone (PTH) thyroidism neurological muscular problems
problems, formation due to high blood of dense bones, calcium concen-tetany due to low trations; weak and blood calcium brittle bonesconcentrations
Insulin Diabetes High blood glucose, Excess insulin Low blood glucose mellitus impaired glucose production levels, possibly (type 1) utilization, dependence or administration causing coma and death
on lipids for energy; glycosuria, possiblycausing coma and death
Mineralocorticoids Hypoaldo- Polyuria, low blood Aldosteronism Increased body (MC) steronism volume, high blood weight due to sodium
potassium and low and water retention; sodium concentrations low blood
potassium concentration
Glucocorticoids Addison’s Inability to tolerate Cushing’s disease Excessive breakdown (GC) disease stress, mobilize energy of tissue proteins
reserves, or maintain and lipid reserves; normal blood glucose impaired glucose concentrations metabolism
Epinephrine (E), None identified Pheochromocytoma High metabolic rate, norepinephrine body temperature, (NE) blood pressure
and heart rate Estrogens Hypogonadism Sterility, lack of Adrenogenital Overproduction of
(females) secondary sexual syndrome androgens by characteristics innermost adrenal
cortex leads tomasculinization
Menopause Cessation of Precocious Premature sexualovulation puberty maturation and
related behavioral changes
Androgens Hypogonadism Sterility, lack of Adrenogenital Abnormal production (males) (male) secondary sexual syndrome of estrogen, some-
characteristics (gynecomastia) times due to adrenal or interstitial cell tumors; leads to breast enlargement
Precocious Premature sexualpuberty maturation and
related behavioral changes
Endocrine.eap3am 8/20/02 3:41 PM Page 89

10
90 The Body Systems: Clinical and Applied Topics
These signs are very useful, but many othersigns and symptoms related to endocrine disordersare less definitive. For example, the condition ofpolyuria, or increased urine production, may be theresult of hyposecretion of ADH (diabetes insipidus) ora form of diabetes mellitus, and a symptom such ashypertension (high blood pressure) can be caused bya variety of cardiovascular or endocrine problems. Inthese instances diagnostic decisions are often basedon blood tests, which can confirm the presence of anendocrine disorder by detecting abnormal levels ofcirculating hormones, followed by procedures thatdetermine whether the primary cause of the problemlies within the endocrine gland, the regulatory mech-anism(s), or the target tissues.
Thyroid Gland Disorders EAP p. 323
Hypothyroidism typically results from some prob-lem involving the thyroid gland rather than withpituitary production of TSH. In primary hypothy-roidism TSH levels are elevated because the pitu-itary gland attempts to stimulate thyroid activity,but levels of T3 (triiodothyronine) and T4 (tetra-iodothyronine or thyroxine) are depressed. One formof hypothyroidism results from a mutation thataffects the structure of the G-proteins at TSH recep-tors. The structural change reduces the receptors’sensitivity to TSH and depresses thyroid activity.Treatment of chronic hypothyroidism, such as thehypothyroidism that follows radiation exposure,usually involves the administration of synthetic thy-roid hormones (thyroxine) to maintain normal bloodconcentrations.
A goiter is an enlargement of the thyroidgland. The enlargement usually indicates increasedfollicular size, despite a decrease in the rate of thy-roid hormone production. A goiter usually developswhen the thyroid gland is unable to synthesize andrelease adequate amounts of thyroid hormones.Under continuing TSH stimulation, thyroglobulinproduction accelerates and the thyroid folliclesenlarge. One type of goiter occurs if the thyroidfails to obtain enough iodine to meet its syntheticrequirements. (This condition is now rare in theU.S. due to the use of iodized table salt.) Withtreatment, over time the resting thyroid may returnto its normal size.
Hyperthyroidism, also known as thyrotoxico-sis, occurs when thyroid hormones are produced inexcessive quantities. In Graves’ disease excessivethyroid activity leads to goiter and the symptoms ofhyperthyroidism. Protrusion of the eyes, or exoph-thalmos (eks-ahf-THAL-m|s), may also appear, forunknown reasons. Graves’ disease has a geneticautoimmune basis and affects many more womenthan men. Treatment may involve the use ofantithyroid drugs, the surgical removal of portionsof the glandular mass, or destruction of part of thegland by exposure to radioactive iodine.
Hyperthyroidism may also result from inflam-mation or, rarely, thyroid tumors. In extreme cases
the individual’s metabolic processes accelerate outof control. During a thyrotoxic crisis, or “thyroidstorm,” the subject experiences an extremely highfever, rapid heart rate, and the dangerous malfunc-tioning of a variety of physiological systems.
Disorders of Parathyroid FunctionEAP p. 325
When the parathyroid gland secretes inadequate orexcessive amounts of parathyroid hormone, calci-um concentrations move outside of normal homeo-static limits. Hypoparathyroidism may developafter neck surgery, especially a thyroidectomy, ifthe blood supply to the parathyroid glands isrestricted. In other cases the primary cause of thecondition is uncertain. PTH is extremely costly, andbecause supplies are very limited, PTH administra-tion is not used to treat this condition, despite itsprobable effectiveness. As an alternative, a dietarycombination of vitamin D3 and calcium can beused to elevate body fluid calcium concentrations.(As noted in Chapter 6 of the text, vitamin D3 stim-ulates the absorption of calcium ions across thelining of the digestive tract.)
In hyperparathyroidism, calcium concentra-tions become abnormally high. Calcium salts in theskeleton are mobilized, and bones are weakened.On X-rays the bones have a light, airy appearancebecause the dense calcium salts no longer domi-nate the tissue. CNS function is depressed, think-ing slows, memory is impaired, and the individualoften experiences emotional swings and depres-sion. Nausea and vomiting occur, and in severecases the patient may become comatose. Musclefunction deteriorates, and skeletal muscles becomeweak. Other tissues are often affected as calciumsalts crystallize in joints, tendons, and the dermis,and calcium deposits may produce masses, calledkidney stones, that block filtration and conductionpassages in the kidney.
Hyperparathyroidism most commonly resultsfrom a tumor of the parathyroid gland. Treatmentinvolves the surgical removal of the overactive tis-sue. Fortunately there are four parathyroids, andthe secretion of even a portion of one gland canmaintain normal calcium concentrations.
Disorders of the Adrenal CortexEAP p. 326
Clinical problems related to the adrenal gland varydepending on which groups of adrenal cells becomeinvolved. The conditions may result from changesin the functional capabilities of the adrenal cells(primary conditions) or disorders affecting the reg-ulatory mechanisms (secondary conditions). Inhypoaldosteronism, adrenal cells fail to produceenough aldosterone, usually either as an early signof adrenal insufficiency or because the kidneys arenot releasing adequate amounts of renin. Low
Endocrine.eap3am 8/20/02 3:41 PM Page 90

10
The Endocrine System 91
aldosterone levels lead to excessive losses of waterand sodium ions at the kidneys, and the water lossin turn leads to low blood volume and a fall inblood pressure. The resulting changes in electrolyteconcentrations, including hyperkalemia (highextracellular K+ levels) affect transmembranepotentials, eventually causing dysfunctions inneural and muscular tissues.
Hypersecretion of aldosterone results in thecondition of aldosteronism, or hyperaldosteronism.Under continued aldosterone stimulation, the kid-neys retain sodium ions in exchange for potassiumions that are lost in the urine. Hypertension andhypokalemia occur as extracellular potassium lev-els decline. Aldosteronism increases the concentra-tion gradient for potassium ions across cellmembranes. This leads to an acceleration in therate of potassium diffusion out of the cells and intothe interstitial fluids. The reduction in intracellularand extracellular potassium levels eventually inter-feres with the function of excitable membranes,especially cardiac muscle cells and neurons, andkidney cells.
Addison’s disease may result from inadequatestimulation of the adrenal cells by ACTH or fromtheir inability to synthesize the necessary hor-mones usually due to autoimmune problems orinfection. Affected individuals become weak andlose weight, due to a combination of appetite loss,hypotension, and hypovolemia. They cannot ade-quately mobilize energy reserves, and their bloodglucose concentrations fall sharply within hoursafter a meal. Stresses cannot be tolerated, and aminor infection or injury may lead to a sharp andfatal decline in blood pressure. A particularly inter-esting symptom is the increased melanin pigmen-tation in the skin. The ACTH molecule and theMSH molecule are similar in structure, and at highconcentrations ACTH stimulates the MSH recep-tors on melanocytes. President John F. Kennedysuffered from this disorder.
Cushing’s disease results from overproductionof glucocorticoids. The symptoms resemble those ofa protracted and exaggerated response to stress.(The stress response is discussed in the text on p.334.) Glucose metabolism is suppressed, lipidreserves are mobilized, and peripheral proteins arebroken down. Lipids and amino acids are mobilizedin excess of the existing demand. The energyreserves are shuffled around, and the distributionof body fat changes. Adipose tissues in the cheeksand around the base of the neck become enlargedat the expense of other areas, producing a “moon-faced” appearance. The demand for amino acidsfalls most heavily on the skeletal muscles, whichrespond by breaking down their contractile pro-teins. This response reduces muscular power andendurance. The skin becomes thin and may devel-op stria, or stretch marks.
If the primary cause is ACTH oversecretion at theanterior pituitary gland, the most common source isa pituitary adenoma (a benign tumor of glandular
origin). Microsurgery can be performed through thesphenoid bone to remove the adenomatous tissue.Some oncology centers use pituitary radiation ratherthan surgery. Several drug therapies act at the hypo-thalamus, rather than the pituitary gland, to preventthe release of corticotropin-releasing hormone (CRH).Alternatively, the adrenal glands can be surgicallyremoved (a bilateral adrenalectomy), but furthercomplications can arise as the adenoma enlarges.
The chronic administration of large doses ofsteroids is required in some cases to treat severeasthma and some cancers and to prevent organtransplant rejection. Prolonged use of such largedoses can produce symptoms similar to those ofCushing’s disease, but such treatment is usuallyavoided.
Disorders of the Adrenal MedullaeEAP p. 328
The overproduction of epinephrine by the adrenalmedullae may reflect chronic sympathetic activation.A pheochromocytoma (fƒ-|-kr|-m|-sª-T«-muh) is atumor that produces epinephrine and norepineph-rine in massive quantities. The tumor usually devel-ops within the adrenal medullae, but it may alsoinvolve other sympathetic ganglia. The most danger-ous symptoms are rapid and irregular heartbeat andhigh blood pressure; other symptoms include uneasi-ness, sweating, blurred vision, and headaches. Thiscondition is rare, and surgical removal of the tumoris the most effective treatment.
Light and Behavior EAP p. 328
Exposure to sunlight can do more than stimulate atan or promote the formation of vitamin D3. Thereis evidence that daily light-dark cycles have wide-spread effects on the central nervous system, withmelatonin playing a key role. Several studies haveindicated that residents of temperate and higherlatitudes in the Northern Hemisphere undergo sea-sonal changes in mood and activity patterns. Thesepeople feel most energetic from June throughSeptember, whereas the period of Decemberthrough March finds them with relatively low spir-its. (The situation in the Southern Hemisphere,where the winter and summer seasons arereversed, is just the opposite.) The degree of sea-sonal variation differs from individual to individual;some people are affected so severely that they seekmedical attention. The observed symptoms haverecently been termed seasonal affective disorder,or SAD. Individuals with SAD experience depres-sion and lethargy and find it difficult to concen-trate. Often they sleep for long periods, perhaps 10hours or more per day. They may also go on eatingbinges and have a craving for carbohydrates.
Melatonin secretion appears to be regulated bysunlight exposure, not simply by light exposure.Normal interior lights are apparently not strong
Endocrine.eap3am 8/20/02 3:41 PM Page 91

10
92 The Body Systems: Clinical and Applied Topics
enough or do not release the right mixture of lightwavelengths to depress melatonin production.Because many people spend very little time out-doors in the winter, melatonin production increasesduring that season, and the depression, lethargy,and concentration problems appear to be linked toelevated melatonin levels in the blood. Comparablesymptoms can be produced in a normal experimen-tal subject by an injection of melatonin.
Many SAD patients may be successfully treatedby exposure to sun lamps that produce full-spectrumlight. Experiments are under way to define exactlyhow intense the light must be and determine theminimal effective time of exposure.
Diabetes Mellitus EAP p. 330
There are two major types of diabetes mellitus:insulin-dependent (type 1) diabetes and non-insulin-dependent (type 2) diabetes.
The primary cause of insulin-dependent dia-betes mellitus (IDDM), or type 1 diabetes, isinadequate insulin production by the beta cells ofthe pancreatic islets. In this condition insulin pro-duction declines due to a drop in the number ofbeta cells. Glucose transport in most cells cannotoccur in the absence of insulin. When insulin con-centrations decline, cells can no longer absorb glu-cose from their surroundings. Under theseconditions peripheral tissues remain glucose-starved despite the presence of adequate or evenexcessive amounts of glucose in the circulation.
After a meal rich in glucose, blood concentra-tions may become so elevated that the kidney cellscannot reclaim all of the glucose molecules enter-ing the urine. The high urinary concentration ofglucose limits the ability of the kidney to conservewater, so the individual urinates frequently andmay become dehydrated. The chronic dehydrationleads to disturbances of neural function (blurredvision, tingling sensations, disorientation, fatigue)and muscle weakness.
Despite the high blood concentrations, glucosecannot enter endocrine tissues, and the endocrinesystem responds as if glucose were in short supply.Alpha cells release glucagon, and glucocorticoidproduction accelerates. Peripheral tissues thenbreakdown lipids and proteins to obtain energy.The breakdown of large numbers of fatty acids gen-erates molecules called ketone bodies. The accu-mulation of large numbers of these acids can causea dangerous reduction in blood pH. This condition,called ketoacidosis, commonly triggers vomiting. Insevere cases, it can precede a fatal coma.
Long-term treatment involves a combination ofdietary control, monitoring blood glucose levels upto several times a day, and administration ofinsulin, either by periodic injection or throughmore continual subcutaneous delivery with aninsulin pump. The treatment is complicated by thefact that tissue glucose demands cycle up anddown, depending on physical activity, emotional
state, stress, and other factors that are hard toassess or predict. It is therefore difficult to main-tain stable and normal blood glucose levels overlong periods of time.
Type 1 diabetes most often appears in individu-als under 40 years of age. Because it frequentlyappears in childhood, it has been called juvenile-onset diabetes. Most people with this type of dia-betes (roughly 80 percent) have circulatingantibodies that target the surfaces of beta cells.The disease may therefore be an example of anautoimmune disorder, a condition that results whenthe immune system attacks normal body cells.(Autoimmune disorders are discussed in the text, p.446.) Consequently, attempts have been made toprevent the appearance of type 1 diabetes with aza-thioprine (Imuran®), a drug that suppresses theimmune system. This procedure is somewhat dan-gerous, however, because compromising immunefunction increases the risk of acquiring seriousinfections or developing cancer.
Non-insulin-dependent diabetes mellitus(NIDDM), or type 2 diabetes, typically affects obeseindividuals over 40 years of age. Because of the agefactor, this condition was called maturity-onsetdiabetes. Unfortunately, with increased childhoodobesity more teenagers are developing Type 2 dia-betes mellitus. Insulin levels are normal or elevat-ed, but peripheral tissues no longer respondnormally, often due to a reduction in the number ofinsulin receptors. Treatment consists of weight lossand dietary restrictions that may elevate insulinproduction and tissue response. The drug met-formin (Glucophage®) lowers blood glucose concen-trations, primarily by reducing glucose synthesisand release at the liver. The use of metformin incombination with other drugs that affect glucosemetabolism promises to improve the quality of lifefor many type 2 diabetes patients.
Up to 6 percent of the U.S. population has dia-betes mellitus, over 90% with the type 2 form.Diagnosis is based on high fasting blood glucose,symptoms of diabetes plus a high random bloodglucose, and an inability to reduce elevated bloodglucose levels 2 hours after drinking a fixedamount of glucose. These criteria have largelyreplaced the 6 hour glucose tolerance test thatinvolved drinking glucose and testing the bloodglucose level multiple times over 4 to 6 hours.Probably because glucose levels cannot be stabi-lized adequately, even with treatment, patientswith long-term diabetes mellitus often developchronic medical problems. In general, these prob-lems are related to cardiovascular abnormalities.The most common examples include the following:
1. Vascular changes at the retina, including pro-liferation of capillaries and hemorrhaging, oftencause disturbances of vision. This condition iscalled diabetic retinopathy.
2. Changes occur in the clarity of the lens, pro-ducing cataracts.
Endocrine.eap3am 8/22/02 11:04 AM Page 92

10
The Endocrine System 93
3. Small hemorrhages and inflammation at thekidneys cause degenerative changes that canlead to kidney failure. This condition is calleddiabetic nephropathy.
4. A variety of neural problems appear, includingnerve palsies, paresthesias and pain, and auto-nomic dysfunction. These disorders, collectivelytermed diabetic neuropathy, are probablyrelated to disturbances in the blood supply toneural tissues, since neurons do not requireinsulin to absorb and utilize glucose.
5. Degenerative changes in cardiac circulationcan lead to early heart attacks. For a given agegroup, heart attacks are 3–5 times more likelyin diabetic individuals.
6. Other peripheral changes in the vascular sys-tem can disrupt normal circulation to theextremities. For example, a reduction in bloodflow to the feet can lead to tissue death, ulcera-tion, infection, and loss of toes or a major por-tion of one or both feet.
Endocrinology and AthleticPerformance EAP p. 332
One of the first endocrinological “mass experi-ments” on humans occurred early in World War II,when the German government administered testos-terone to Nazi SS officers in an attempt to makethem more aggressive. (There is no evidence thatthe experiment succeeded.) Nowadays, such prac-tices are universally deplored in all civilized soci-eties, and medical research involving humans isgenerally subject to tight ethical constraints andmeticulous scientific scrutiny. Yet a clandestine,unscientific, and potentially quite dangerous pro-gram of “experimentation” with hormones is todaybeing pursued by athletes in many countries.Despite being banned by the International OlympicCommittee, the United States Olympic Committee,the NCAA, and the NFL, and condemned by theAmerican Medical Association and the AmericanCollege of Sports Medicine, a significant number ofamateur and professional athletes continue to usehormones to improve their performance at the riskof damaging their health. Although synthetic formsof testosterone are used most often, young athletesmay use any combination of testosterone, growthhormone, and a variety of synthetic hormones.
Androgen AbuseThe use of androgens, or “anabolic steroids,” hasbecome common with many athletes, both amateurand professional. The goal of steroid use is toincrease muscle mass, endurance, and “competi-tive spirit.” It has been suggested that as many as30 percent of college and professional athletes and10–20 percent of male high school athletes may beusing anabolic steroids (with or without growthhormone) to improve their performance. Among
bodybuilders, the proportion using steroids in thiscountry may be as high as 80 percent.
Black market sales of anabolic steroids proba-bly exceed $100 million annually. The compoundsare administered orally or by injection, typically indoses 10–1000 times higher than those normallyprescribed in medical treatment. (Legitimate rea-sons for androgen use include the generalizedwasting and debilitation of cancer or AIDS andtreatment of hypogonadism.)
One supposed justification for this practicehas been the unfounded opinion that compoundsmanufactured in the body are not only safe but“good for you.” In reality the administration of nat-ural or synthetic androgens in abnormal amountscarries unacceptable health risks. Androgensaffect many tissues in a variety of ways. Knowncomplications include (1) premature epiphysealclosure; (2) various liver problems (including jaun-dice and hepatic tumors); (3) prostate enlargementand urinary tract obstruction; (4) testicular atro-phy and infertility; and, (5) severe acne. A link toheart attacks, impaired cardiac function, andstrokes has also been suggested. Moreover, thenormal regulation of androgen production involvesa feedback mechanism comparable to thatdescribed for adrenal steroids earlier in this chap-ter. A releasing hormone stimulates the produc-tion of LH, and LH in turn stimulates the secretionof testosterone and other androgens by the inter-stitial cells of the testes. The circulating androgensthen inhibit the production of both the releasinghormone and LH, as indicated in Figure 10-7a, p.320. Thus when synthetic androgens are adminis-tered in high doses, they can (1) suppress the nor-mal production of testosterone, and (2) depress themanufacture of the associated releasing hormoneby the hypothalamus. This suppression may bepermanent.
The use of androgenic “bulking agents” byfemale bodybuilders may not only add musclemass but alter muscular proportions and sec-ondary sexual characteristics. For example,women taking steroids can develop irregular men-strual periods and changes in body-hair distribu-tion (including baldness). Finally, androgen abusemay cause a generalized depression of the immunesystem.
EPO AbuseBecause it is now being synthesized using recombi-nant DNA techniques, erythropoietin, or EPO, isreadily available. Athletes engaged in endurancesports, such as cycling or marathon running, mayuse it to boost the number of oxygen-carrying redblood cells in circulation. Although this improvesthe oxygen content of the blood, it also makes theblood more dense, and the heart must work harderto push it around the circulatory system. Between1991 and 1994, the deaths of 18 young, otherwisehealthy European cyclists were attributed to heartfailure related to EPO abuse.
Endocrine.eap3am 8/20/02 3:41 PM Page 93

94 The Body Systems: Clinical and Applied Topics
GHB and ClenbuterolAndrogens and EPO are known hormones with rea-sonably well understood effects. Because drug test-ing is now widespread in amateur and professionalsports, people interested in “getting an edge” areexperimenting with other drugs whose long-termand short-term effects are difficult to predict. Twoexamples are the recent use of GHB and clen-buterol by amateur athletes.
Gamma-hydroxybutyrate, or GHB, was testedfor use as an anaesthetic 30 years ago and rejectedin part because it was linked to epileptic seizures.In 1990 this drug appeared in health-food stores,where it was sold as an anabolic agent and dietaid. During a 5-month period in 1990, 16 cases ofsevere reaction to GHB were treated in San
Francisco alone. Symptoms experienced includedconfusion, hallucination, seizures, and coma atdoses from 0.25 teaspoons to 4 tablespoons.
Clenbuterol abuse is reportedly widespread,although exact numbers are difficult to obtain.Clenbuterol, sometimes used to treat asthma,mimics epinephrine by increasing the diameter ofthe respiratory passageways and accelerating bloodflow through active skeletal muscles. Although it isalso rumored to have anabolic properties, there isno evidence to support this. Heavy usage cancause severe headaches, tremors, insomnia, andpotentially dangerous abnormal heartbeats. Duringthe 1992 Olympics in Barcelona, Spain, twoAmerican athletes were disqualified because theytested positive for this drug.
CRITICAL-THINKING QUESTIONS5-1. Pheochromocytomas are tumors of the
adrenal medullae that cause hypersecretion of thehormones produced by this region of the adrenalgland. What symptoms would you associate with aperson who suffers from this condition?
a. hypertension
b. sweating
c. nervousness
d. elevated metabolic rate
e. all of the above
5-2. Fifty-year-old Barbara B. reports to theemergency room with heart palpitations (rapid,irregular heart beat). EKG recording shows atrialfibrillation. Barbara’s medical history includesrecent weight loss of 10 pounds and complaints ofincreased irritability and nervousness within thelast month. Some of Barbara’s abnormal diagnosticand lab test results are as follows:
Radioactive iodine uptake test (RAIU) at 2 hours: 20% absorption (normal: 1-13%)
Serum thyroxine (T4) test: 13 ng/dl
Serum triiodothyronine (T3) test: 210 ng/dl
Serum TSH: <0.1
What is the probable diagnosis?
a. hypothyroidism
b. hyperthyroidism
c. myxedema
d. goiter
5-3. Bill develops a benign tumor of theparathyroid glands that causes the level ofparathyroid hormone in his blood to be higher thannormal. Which of the following would you expect tooccur as a result of this condition?
a. decreases in the blood levels of calcium
b. convulsions
c. decreased muscle strength
d. increased bone density
e. all of the above
5-4. Sixteen-year-old John is a promising ath-lete who is below the average height for his age. Hewants to play football in college but is convincedthat he needs to be taller and stronger in order toaccomplish his dream. He persuades his parents tovisit a doctor and inquire about GH treatments. Ifyou were his physician, what would you tell himabout the potential risks and benefits of suchtreatments?
5-5. Angie is diagnosed with abnormal periph-eral vision. After performing several tests, herphysician decides to remove a tumor of her pitu-itary gland. Shortly after the surgery, her eyesightreturns to normal. What was the apparent cause ofAngie’s problem?
5-6. A patient is suffering from secondaryhypothyroidism. Assuming you had available allthe modern testing materials, how could you deter-mine if the problem was due to hypothalamic orpituitary dysfunction?
Endocrine.eap3am 8/20/02 3:41 PM Page 94

The Endocrine System 95
NOTES
Endocrine.eap3am 8/20/02 3:41 PM Page 95