Embed Size (px)
Citation preview

Endocrine System
Carl B. Goodman, Ph.D.
College of Pharmacy & Pharmaceutical Sciences
Florida A&M University
308E FSH-SRC
599-3128

Endocrine System: Homeostasis
Hormone- Regulatory molecules secreted into blood stream
Endocrine Gland- Ductless glands contains secretory cells- Synthesis or produce hormones
Effector- Target cells or tissues- Contains receptors to produce some physiological response
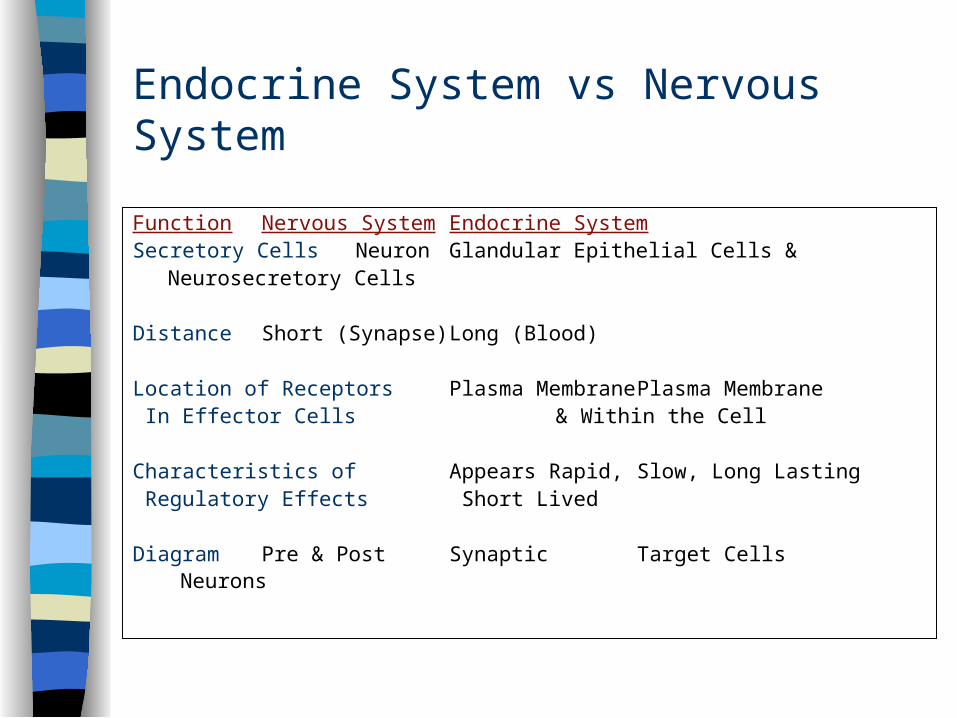
Endocrine System vs Nervous System
Function Nervous System Endocrine System
Secretory Cells Neuron Glandular Epithelial Cells &Neurosecretory Cells
Distance Short (Synapse) Long (Blood)
Location of Receptors Plasma Membrane Plasma Membrane In Effector Cells & Within the Cell
Characteristics of Appears Rapid, Slow, Long Lasting Regulatory Effects Short Lived
Diagram Pre & Post Synaptic Target Cells Neurons

Endocrine System vs Nervous System
Function Nervous System Endocrine System
Overall Function Regulate Effectors Regulate Effectors *HOMEOSTASIS *HOMEOSTASIS
Control Feedback Loop Yes (Nervous Reflex) Yes (Endocrine Reflex)
Chemical Messenger Neurotransmitter Hormone (Proteins or Steroids)
Effector Tissues Muscle & Glandular All Cell Types Tissues *Muscles, Bones,
Glandular
Effector Cells Post Synaptic Neurons Target Cells

Endocrine Action

Endocrine System
Endocrine Glands
CNS: Pituitary Gland
Periphery: Pancreas, Thyroid,
Parathyroid, Adrenal, Testes and Ovaries
Organs with Partial Endocrine Functions
Hypothalamus, Pineal Gland, Stomach, Duodenum, Liver, Thymus, Heart, Skin, Kidney, Lung and Placenta

Types of Hormones: Lipid Soluble
Steroids- Cortisol- Aldosterone- Androgens- Estrogen/Progesterone- Testosterone- Calcitrol (Kidney)
Gas- Nitric Oxide (NO)
Thyroids- Triiodothyronine (T3)
- Thyroxine (T4)

Types of Hormones: Water Soluble Glycoproteins
- Follicle Stimulating Hormone (FSH)- Luteinizing Hormone (LH)- Thyroid Stimulating Hormone (TSH)
Peptides- Anti-diuretic Hormone (ADH) (8 AA)- Oxytocin (8 AA)- Melanocyte Stimulating Hormone (MSH)- Thyroid Releasing Hormone (TRH)
Proteins- Growth Hormone (191), Calcitonin (32 AA), Prolactin, Insulin (21 & 30 AA), ACTH (39 AA), Parathyroid Hormone (84 AA)
Fatty Acids (Arachidonic acid) - Leukotrienes- Prostaglandins- Thromboxanes- Prostacyclins

Types of Hormones: Amino Acids Amines (Water Soluble)
- Norepinephrine (Tyrosine)- Epinephrine (Tyrosine)- Melatonin (Tryptophan)- Serotonin (Tryptophan)- Histamine (Histadine)
Iodinated Amino Acid - Thyroxine (T4)
- Triiodothyronine (T3)

Hormone Circulation Endocrine Action:
hormone is distributed in blood and binds to distant target cell
Paracrine Action:hormone acts locally by diffusing from its source to target cells in the neighborhood
Autocrine Action:hormone acts on the same cell that produced it

Hormone Transport in Blood
Protein hormones circulate in free form in blood
Steroid (lipid) & thyroid hormones must attach to transport proteins (Carrier Molecules) synthesized by liver– improve transport by making them water-soluble– slow loss of hormone by filtration within kidney– create reserve of hormone
• only .1 to 10% of hormone is not bound to transport protein = free fraction
Synthesis and Metabolism

General Mechanisms of Hormone Action
Hormone binds to cell surface or receptor inside target cell
Cell may then:– synthesize new molecules (Protein Synthesis)– change permeability of membrane (Ion channels)– alter rates of reactions (Enzymes)
Each target cell responds to hormone differently– Liver cells: insulin stimulates glycogen synthesis– Adipose: insulin stimulates triglyceride synthesis
Circadian Rhythm for all Hormones (Basal Level)- Ex. Cortisol: increased daytime and decreased at night

Hormone Interaction
Synergistic
Permissive- a second hormone, strengthens the effects of the firstEx. thyroid strengthens epinephrine’s effect upon lipolysis or Estrogen
and Progesterone are need for maturation of follicle
Antagonisticex. Insulin and Glucagon
Prehormone
ex. T4 converted to T3
ex. Vitamin D3 converted to 1,25 dihydroxyvitamin D3

Role of Hormone Receptors Constantly being synthesized & broken down
A range of 2,000-100,000 receptors / target cell
Down-regulation (Hypersecretion of Hormone)– excess hormone, produces a decrease in number of
receptors• receptors undergo Endocytosis and are degraded
– decreases sensitivity of target cell to hormone
Up-regulation (Hyposecretion of Hormone)– deficiency of hormone, produces an increase in the number
of receptors– target tissue more sensitive to the hormone
H + R = HR Complex

Intracellular Chemical Signal Autocrine: secreted in a local area ex. Prostaglandins
Paracrine: neighboring cell ex. Histamine, Prostaglandins
Hormone: secreted in blood… ex. Insulin, T4, and T3
Neurohormone: produced by neurons ex. Oxytocin, ADH
Neurotransmitter or Neurohumor: produced by neurons and secreted into synapse ex. Acetylcholine and Epinephrine
Pheromone: secreted in environment, modifies behavior ex. Sex pheromones

Hormone Signal Transduction Pathway
Steroids Hormone Protein Hormone

Second Messengers
cAMP cGMP Phospholipase C Ca++
Opposing 2nd Messenger System with Same Hormone Beta Adrenergic Receptors
- Relaxation/Dilation = cAMP
Alpha Adrenergic Receptors- Constriction = Phospholipase C

Feedback Control System
Negative Feedback Positive Feedback

Hypothalamic-Pituitary System
AdenohypophysisNeurohypophysis
Pituitary Gland = Hypophysis
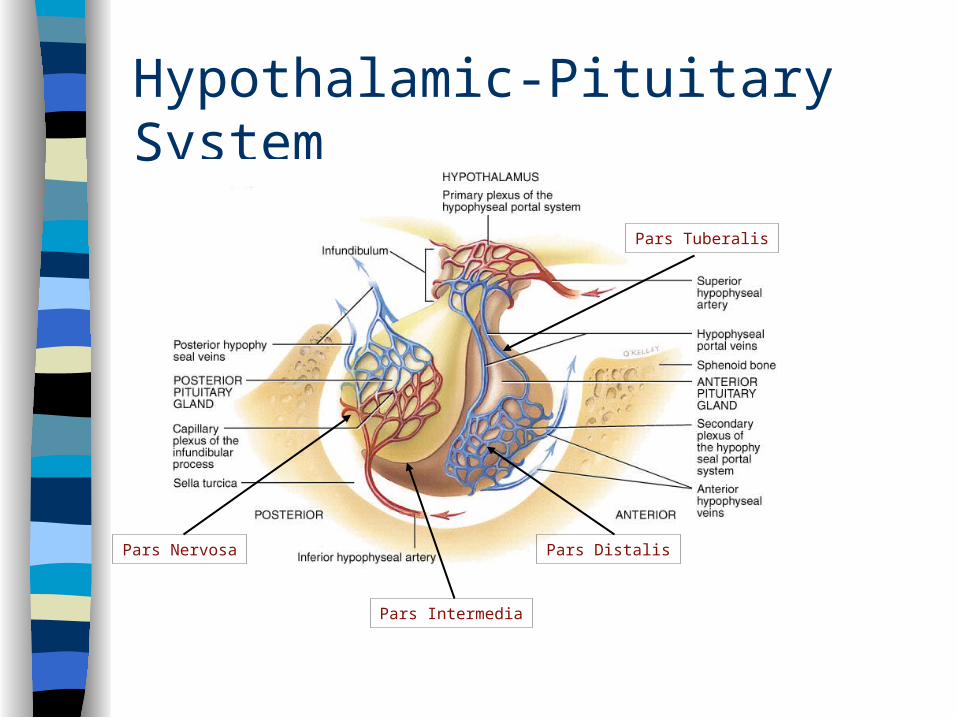
Hypothalamic-Pituitary System
Pars Nervosa Pars Distalis
Pars Tuberalis
Pars Intermedia

Posterior Pituitary Gland: Neurohormones Anti-diuretic Hormone
(ADH) or Vasopressin Osmoreceptors near Supraoptic
Nucleus (Dehydration) (Alcohol)
H2O is reabsorbed from the tubules of the kidney and returned to the blood instead of the urine (H20 is conserved)
Decrease in rate of perspiration during dehydration
Raises Blood Pressure by constricting Arterioles
Oxytocin Stimulate contraction of
uterine muscle (smooth muscle)
Initiate milk ejection from the Alveolar Cells into the ducts of the breast in lactating women

Melanocyte-Stimulating Hormone (MSH)
Pars Intermedia (Corticotroph cells)
Melanocytes - Melanin (Darkening of Skin)
Pre-proopiomelanocortin
2o Addision’s Disease (skin darkening)
Estrogen/Progesterone (skin darkening)

Anterior Pituitary Gland
Growth Hormone (Somatotrophin) Prolactin
Tropic Hormones Adenocorticotrophic Hormone (ACTH) Thyroid Stimulating Hormone (TSH) Luteinizing Hormone (LH) Follicle Stimulating Hormone (FSH)

Growth Hormone
Produced by somatotrophs (191AA)
Within target cells increases synthesis of Somatomedins and Insulin-like Growth Factors that act locally or enter bloodstream– common target cells are liver, skeletal muscle, cartilage and
bone– increases cell growth & cell division by increasing their
uptake of amino acids & synthesis of proteins– stimulate lipolysis in adipose so fatty acids used for ATP– retard use of glucose for ATP production so blood glucose
levels remain high enough to supply brain

Abnormal Levels of Growth HormoneHypersecretion of GH During the growth years before
ossification of Epiphyseal plates, causes increase in rate of skeletal growth = Gigantism
After the growth years = Acromegaly-Excess cartilage growth forming new bones.-Enlarged hands, feet, jaws, separation of teeth, -*Soft Tissue (forehead and nose)
Hyposecretion of GH During the growth years, results
in stunted body growth = Pituitary Dwarfism

Prolactin
Hypothalamus regulates lactotroph cells
Primary function is to generate/initiate milk secretion (Lactation)
1. During Pregnancy, high prolactin promote development of breast for milk secretion
2. At Birth of an Infant, suckling reduces levels of hypothalamic inhibition and prolactin levels rise along with milk production
Mammary glands are primed with E/P, Cortisol, GH, T4 and Insulin
Nursing ceases & milk production slows

Abnormal Levels of Prolactin
Hypersecretion of Prolactin
Causes lactation in non-nursing women
Disruption of the menstrual cycle
(Men) can cause impotence
Hyposecretion of Prolactin
Insignificant except in women, who want to nurse feed their babies

ACTH & TSH Hypothalamus releasing
hormones stimulate corticotrophs
Corticotrophs secrete ACTH & MSH
ACTH stimulates cells of the adrenal cortex that produce glucocorticoids
Hypothalamus regulates thyrotroph cells
Thyrotroph cells produce TSH
TSH stimulates the synthesis & secretion of T3 and T4
Metabolic rate stimulated
Luteinizing Hormone Releasing hormones from
hypothalamus stimulate gonadotrophs
Gonadotrophs produce LH In females, LH stimulates
– secretion of estrogen– ovulation of 2nd oocyte from
ovary– formation of corpus luteum– secretion of progesterone
In males, stimulates interstitial cells to secrete testosterone
Follicle Stimulating Hormone Releasing hormone from
hypothalamus controls gonadotrophs
Gonadotrophs release follicle stimulating hormone
FSH functions
– initiates the formation of follicles within the ovary
– stimulates follicle cells to secrete estrogen
– stimulates sperm production in testes
Gonadotrophins





























