Embed Size (px)
Citation preview


Endodontic clinical seminar 91/10/05
By: Dr. somayyeh dehghan

Case 1

• A 22 years-old female
Chief complaint:
• my tooth fell out due to trauma.
Medical history:
• Non-contributory

• Dental history:
• Avulsion of left maxillary lateral incisor(90/07/28).
• 3 hours dry time.
• Immersed in doxycycline for 15 min.
• Replanted and sutured.
• Referred after 10 days (90/08/08).

Pulpal tests:
Right Maxillary
central incisor
11
Left Maxillary
central incisor
21
Left Maxillary
lateral incisor
22
Left Maxillary
canine
23
cold + + - +
Heat + + - +
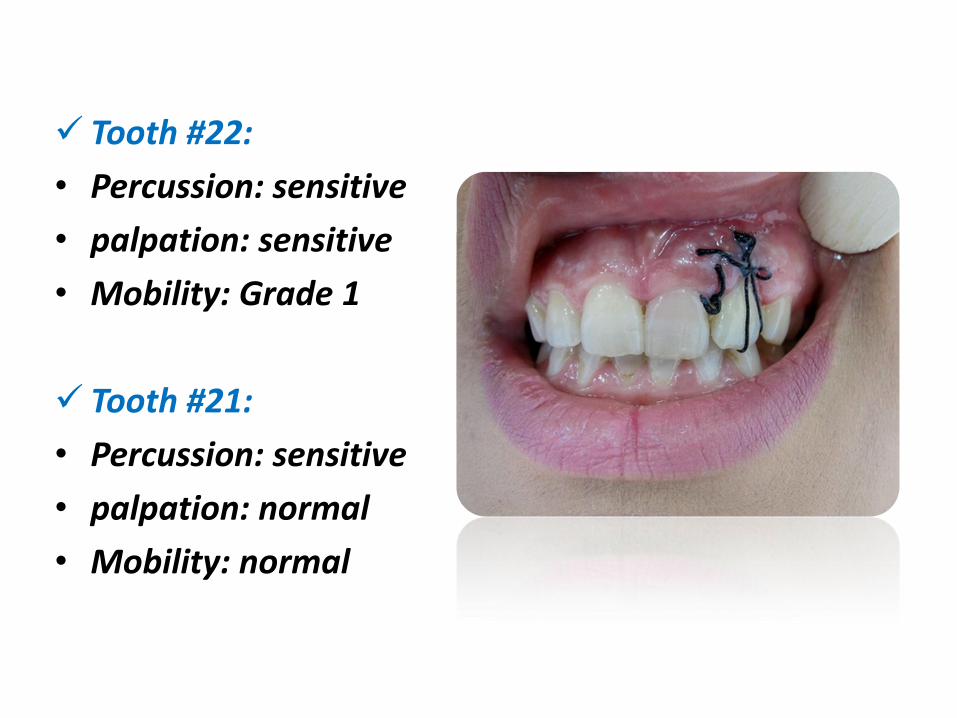
Tooth #22:
• Percussion: sensitive
• palpation: sensitive
• Mobility: Grade 1
Tooth #21:
• Percussion: sensitive
• palpation: normal
• Mobility: normal

1390/08/08: Radiographs with different angles

Treatment plan?

• Which factors determine the avulsed tooth prognosis?
1. Maturity of the tooth (mature/immature)
2. Dry time of the tooth (less than 60min/more than 60 min)

Favorable responses (new cementum)
Unfavorable responses
*osseous replacement resorption
*inflammatory resorption

Storage medium
HBSS(Hanks Balanced Salt Solution)
milk
saliva
Saline
Water(hypotonic)

Chamorro et al , Dental Traumatology 2008;24:11–16
• Overall, cells treated on ice showed significantly lower levels of apoptosis when compared with treatments at room temperature
• Milk and HBSS had a low percentage of apoptotic cells and no significant difference (P > 0.05)

*

Replantation
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min

Replantation
* Rinse with saline & replant.
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min

Replantation
* Rinse with saline
* Topical antibiotics
Enhance revascularization
*Replant
* Rinse with saline & replant.
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min

Replantation
*Place in acid
*Remove nonviable cells with gauze
*2% stannous fluoride
*Replant
* Rinse with saline
* Topical antibiotics
Enhance revascularization
*Replant
* Rinse with saline & replant.
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min

Replantation
*Not replant
*Remove nonviable cells with gauze
*2% stannous fluoride
*RCT & replant
*Place in acid
*Remove nonviable cells with gauze
*2% stannous fluoride
*Replant
* Rinse with saline
* Topical antibiotics
Enhance revascularization
*Replant
* Rinse with saline & replant.
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min
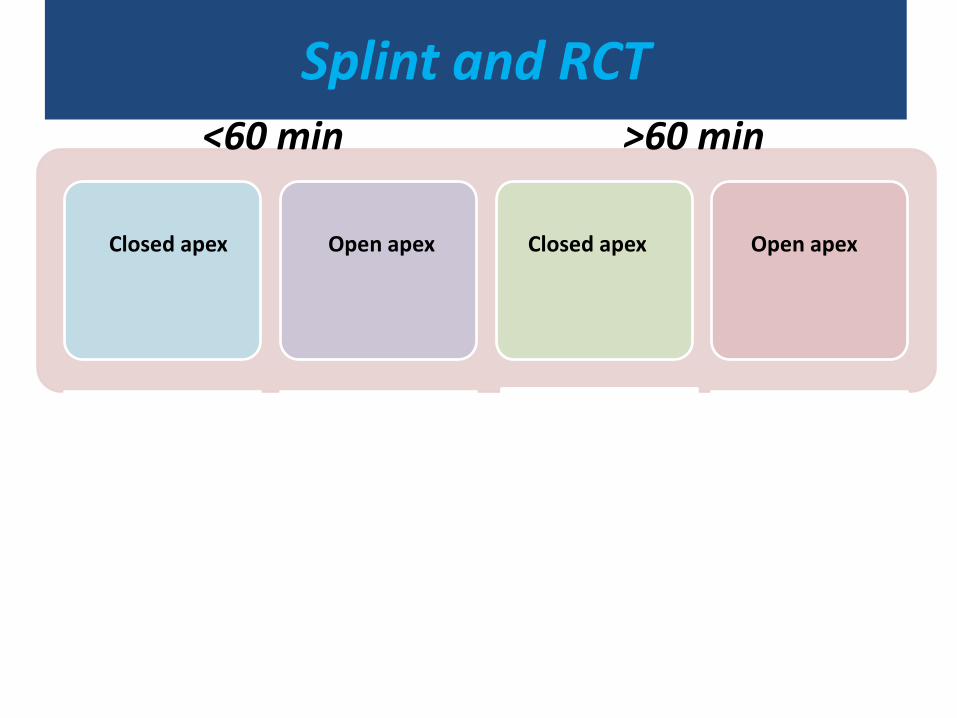
Splint and RCT
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min

Splint and RCT
*flexible splint for 2w.
*RCT 7-10 days later
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min

Splint and RCT
*flexible splint for 2w.
*follow up
*flexible splint for 2w.
*RCT 7-10 days later
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min

Splint and RCT
*flexible splint for 4w.
*RCT 7-10 days later
*flexible splint for 2w.
*follow up
*flexible splint for 2w.
*RCT 7-10 days later
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min

Splint and RCT
*flexible splint for 4w.
*RCT extraorally
*flexible splint for 4w.
*RCT 7-10 days later
*flexible splint for 2w.
*follow up
*flexible splint for 2w.
*RCT 7-10 days later
Closed apex Open apex Closed apex
Open apex
<60 min
>60 min

How to manage the closed apex avulsed tooth with extra oral
dry time>60 minutes?
• Placing in acid for 5 minutes.
• Soaking in 2%stannous fluoride.
• splinting for 1-2 weeks(4week)
Is splinting duration important or not??

*
- 138 replanted avulsed permanent teeth - both short-term splinting (14 days or less) and long term-splinting (over 14 days) - successful periodontal healing after replantation is unaffected by splinting duration.

*
Petrovic et al.
low survival: •Delayed replantation •Unphysiological storage •Incisors with open apices •Required prolonged treatment with calcium hydroxide

flexible splints with physiologic movement of the tooth1
(TTS, suture2).
1. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dental Traumatology 2012; 28: 88–96. 2. Management of tooth avulsion, review and case report. Int journal of contemporary dentistry, 2011

what about traumatic occlusion?
Traumatic occlusion SP expression increases significantly in human dental pulp/PDL
inflammatory responses in pulpal and periapical tissues1.
1. Effect of Experimentally Induced Occlusal Trauma on Substance P Expression in Human Dental Pulp and Periodontal Ligament.
J Endod 2011;37:627–630.

What about antibiotic administration?
• systemic administration :
• clinical studies:
Not demonstrated.
• Experimental studies :
Limiting infection-related resorption:
Tetracycline
Penicillin V
amoxicillin
• Local administration :
Intracanal Ledermix
Topical application before replantation
Andreasen et al. The role of antibiotics in preventing healing complications after traumatic dental injuries: a literature review. Endodontic Topics 2006, 14, 80–92

1390/08/08 (first visit):
• Tooth #22 (lateral incisor) :
Suture was removed.
Root canal therapy was initiated for #22 (lateral) and treated with long-term calcium hydroxide therapy.

1390/09/26 (second visit):
• tooth #21:
Crown discoloration
Vitality: negative
Percussion: sensitive
Mobility: normal

1390/09/26 (second visit):
• tooth #21: Root canal therapy was initiated
Irrigated with NaOCl 5.25%
obturated with gutta-percha/AH26.
• Tooth #22: Ca(OH)2 was removed.
obturated with gutta-percha/AH26.

1391/03/30(6-month follow up):
• tooth #21:
No clinical and radiographic signs.
• Tooth #22:
Metallic-like percussion sound.
Possibly inflammatory and replacement resorption.

1391/04/10: 6-month follow up

1391/08/10 9-month follow up:

Diagnosis and treatment plan?

How to control root resorption?
MTA
Calcium hydroxide / MTA
Long- term calcium hydroxide

Andreasen et al.
fracture resistance: 1- MTA 2- CH(short-term,30 days)+ MTA (not significant) 3-saline 4- CH(long-term,100days) (significant) *

Witherspoon et al. *Clinical & RA evaluation 93.5% of teeth treated in 1 visit healed( MTA obturation) 90.5% of teeth treated in 2 visits healed. (3 weeks calcium hydroxide ) ( not significant)
*

Kafman et al. • teeth with root treatment
with MTA showed the highest fracture resistance at 1 year.
• MTA induced the expression of TIMP-2 in the dentin matrix and prevented destruction of the collagen matrix. *

Calcium hydroxide therapy
advantages: disadvantages:
High pH
No bacteria-tight seal*
Antimicrobial activity

Calcium hydroxide therapy
advantages: disadvantages:
High pH
No bacteria-tight seal*
Antimicrobial activity
detrimental effect on periodontal tissues when used as an intracanal medicament1.
1. Biocompatibility of dental materials used in contemporary endodontic therapy: a review. Part 1. Intracanal drugs and substances. IEJ,36, 75–85.
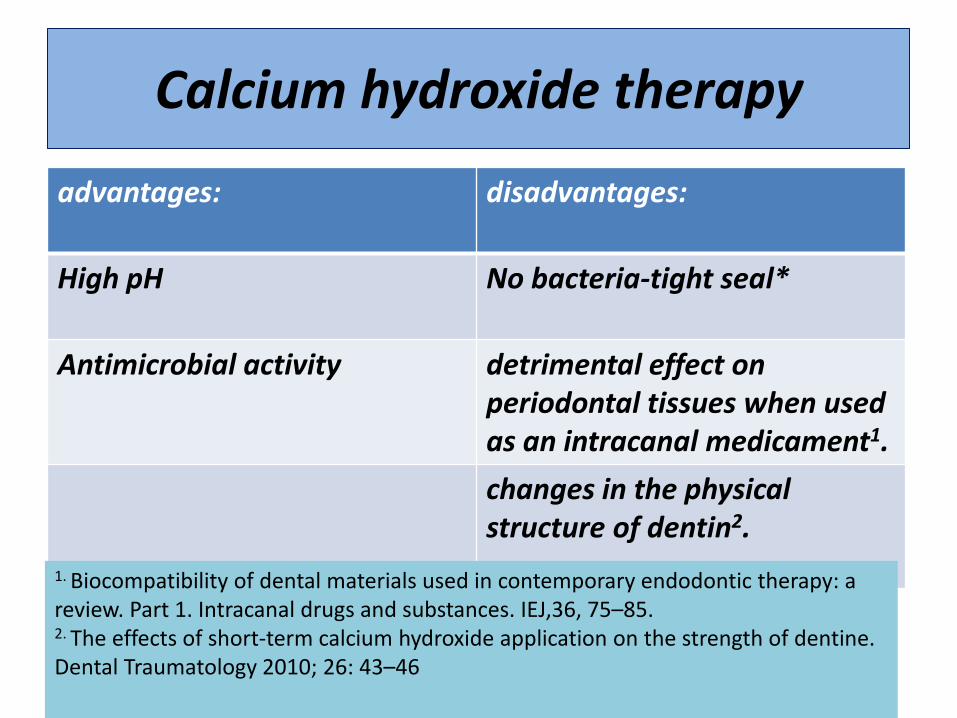
Calcium hydroxide therapy
advantages: disadvantages:
High pH
No bacteria-tight seal*
Antimicrobial activity
detrimental effect on periodontal tissues when used as an intracanal medicament1.
changes in the physical structure of dentin2.
1. Biocompatibility of dental materials used in contemporary endodontic therapy: a review. Part 1. Intracanal drugs and substances. IEJ,36, 75–85. 2. The effects of short-term calcium hydroxide application on the strength of dentine. Dental Traumatology 2010; 26: 43–46

MTA Advantages:
Antimicrobial activity
Sustained alkaline pH
bacterial-tight seal
Activates proliferation and differentiation of cells
Inhibits osteoclastic activity by high PH and inhibition of MMPs1.
1. Fracture resistance and histological findings of immature teeth treated with mineral trioxide aggregate. dental traumatol 2008.

Is chloroform contraindicated or not?
• Decreases Human Periodontal Ligament Fibroblasts growth1.
• Significantly reduces intracanal levels of E. faecalis2.
1.Chloroform Biocompatibility on Human Periodontal Ligament Fibroblasts.2010
2. The antimicrobial effect of chloroform on Enterococcus faecalis after gutta-percha removal. J Endod,2006

the use of chloroform during endodontic retreatment significantly reduced intracanal levels of cultivatable E. faecalis
*

What are Causes of central discoloration?
Causes of tooth
discoloration
Intrapulpal hemorrhage
Pulp necrosis

Is internal bleaching contraindicated in traumatized teeth or not?
Heat
bacteria
Previous trauma
external cervical
root resorption

Is internal bleaching contraindicated in traumatized
teeth or not?

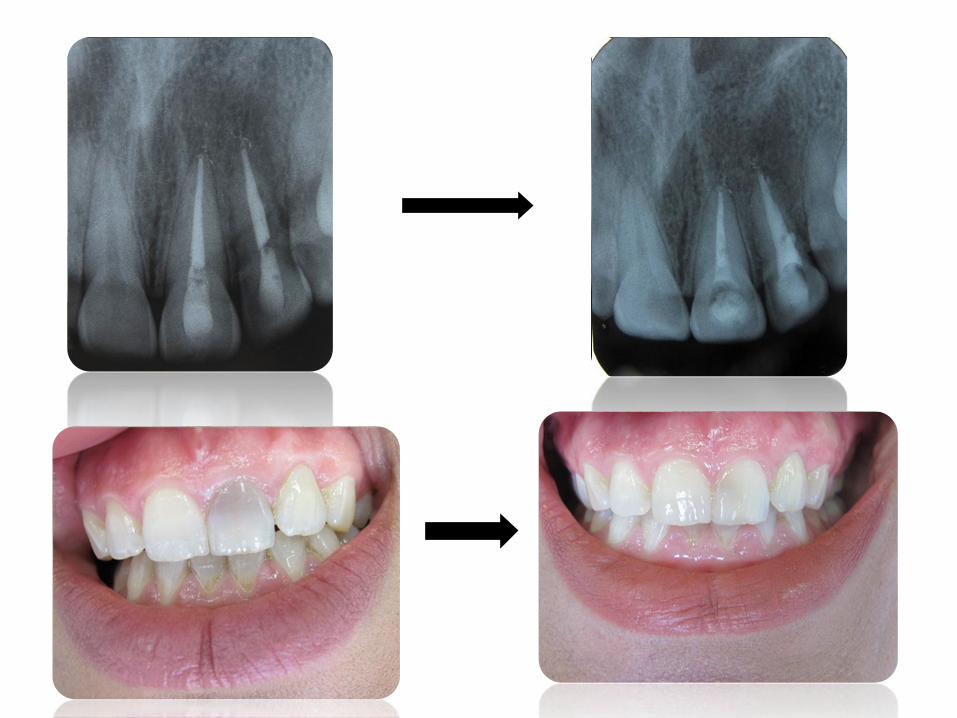
1391/08/10:
• Tooth #22:
Retreatment and obturation with MTA.
• Tooth #21:
Internal bleaching with sodium perborate.

Thanks for your attention





























