Embed Size (px)
Citation preview

AT
TC
CD
J
A
1E
PEER-REVIEW REPORTS
Endoscopic Surgery for Intraventricular Hemorrhage (IVH) Caused by ThalamicHemorrhage: Comparisons of Endoscopic Surgery and External VentricularDrainage (EVD) SurgeryChun-Chung Chen1,2, Chun-Lin Liu1, Ying-Nan Tung3, Han-Chung Lee1, Hao-Che Chuang1,
Shinn-Zong Lin1, Der-Yang Cho1
aa(h
efke
INTRODUCTION
Hypertensive intracerebral hemorrhage (ICH)is a neurosurgical emergency frequentlyencountered in clinical practice. Approxi-mately 10% to 15% of cases of ICH involvethalamic hemorrhage (1, 22). Evacuation ofa thalamic hematoma by craniotomy is gen-erally considered controversial because ofthe high rates of mortality and morbidityobserved after this procedure. Thalamichemorrhages are clinically significant asthey are located close to the internal capsuleand the ventricular system. They have beenclassified into medial, posterolateral, ante-rior and dorsal types according to the vesselinvolved and subsequent clinical picture(10). Many studies had found that ICH vol-ume, intraventricular hemorrhage (IVH),
Key words� Endoscopic surgery� External ventricular drainage� Intraventricular hemorrhage� Thalamic hemorrhage
Abbreviations and AcronymsCSF: Cerebrospinal fluidETV: Endoscopic third ventriculostomyEVD: External ventricular drainageGCS: Glasgow Coma ScaleICU: Intensive care unitICH: Intracerebral hemorrhageIVF: Intraventricular fibrinolysisIVH: Intraventricular hemorrhageVP: Ventriculoperitoneal
From the 1Department of Neurosurgery, 2ChinaMedical University, and 3Department of
nesthesiology, China Medical University Hospital,aichung, Taiwan, Republic of China
o whom correspondence should be addressed:hun-Chung Chen M.D. [E-mail: [email protected]]
itation: World Neurosurg. (2011) 75, 2:264-268.OI: 10.1016/j.wneu.2010.07.041
ournal homepage: www.WORLDNEUROSURGERY.org
vailable online: www.sciencedirect.com
878-8750/$ - see front matter © 2011 Published bylsevier Inc.
hydrocephalus, Glasgow Coma Scale (GCS) n
264 www.SCIENCEDIRECT.com
nd age are the best predictors for mortalitynd functional outcome after thalamic ICH10, 11, 15, 20). IVH caused by thalamicemorrhage is generally treated with exter-
� BACKGROUND: Intraventricular heorrhage has high mortality and morbidithe efficacy and the results of endoscaused by thalamic hemorrhage comdrainage (EVD) surgery.
� METHODS: From January 2006 to Deby thalamic hemorrhage were enrollewith IVH caused by thalamic hemorrhaalus were indicated for surgery; the padivided into an EVD group and anevaluation data included the Glasgow(ICU) stay, age, intracerebral hemorrhwas measured using the 30-day and 9(VP) shunt dependent rate, and Glasgo
� RESULTS: The clinical features ofsignificant differences in age or GlasgThere was also no significant differenGraeb score between the endoscopic gstay was 11 � 5 days in the endoscopicgroup. The endoscopic surgery group hwith the EVD group. The 30-day and 90in the endoscopic surgery group anrespectively. The mean Glasgow Outcendoscopic surgery group and 3.33 �cantly correlated with initial conscioinfluence the outcome in all of the casmortality rate or outcome between theVP shunt rates were 47.62% in the enEVD group. Endoscopic surgery group0.002; odds rate � 9.8) compared with
� CONCLUSIONS: Endoscopic surgershunt-dependent hydrocephalus, andEVD surgery. This can decrease the nwith IVH caused by thalamic hemorrh
al ventricular drainage (EVD) (2). How- r
WORLD NEUROSURGE
ver, although appropriate treatment is of-ered, the clinical response to EVD is notnown in detail. We used endoscopy tovacuate IVH caused by thalamic hemor-
hage (IVH) caused by thalamic hem-he aim of this study was to investigateic surgery for the evacuation of IVHed with that of external ventricular
ber 2008, 48 patients with IVH causedd treated in our department. Patientsho also resulted in acute hydroceph-
ts who were included were randomlyscopic surgery group. The clinicala Scale, length of intensive care unit
volume, and severity of IVH. Outcomey mortality rate, ventriculoperitonealutcome Scale after three months.
4 patients in each group showed nooma Scale assessment on admission.intracerebral hemorrhage volume orand the EVD group. The length of ICU
gery group and 18 � 7 days in the EVDshorter ICU stay (P � 0.04) comparedmortality rates were 12.5% and 20.8%2.5% and 16.6% in the EVD group,
Scale score was 3.08 � 1.38 in the0 in the EVD group. Outcome signifi-ss level; the severity of IVH did nothere was no significant difference in
oscopic group and the EVD group. Theopic surgery group and 90.48% in the
significant lower VP shunt rate (P �EVD group.
as found to have significantly lowerICU stay was shorter compared withfor permanent VP shunts in patients
morrty. Tcoppar
cemd ange wtienendoCom
age0-daw O
the 2ow Cce inroupsur
ad a-dayd 1ome1.4
usnees. Tend
doschad a
the
y wtheeedage.
hage (3). The results were promising with
RY, DOI:10.1016/j.wneu.2010.07.041

Bi
Gtmm(t
OAassfOmd
SAipsd�p
IAhsmcrtcm
PEER-REVIEW REPORTS
CHUN-CHUNG CHEN ET AL. ENDOSCOPIC SURGERY FOR IVH CAUSED BY THALAMIC HEMORRHAGE
respect to the prevention of shunt-depen-dent hydrocephalus. The aim of this studywas to investigate the efficacy and the re-sults of endoscopic surgery for IVH fromthalamic hemorrhage and compare themwith those from EVD surgery.
MATERIAL AND METHODS
PatientsFrom January 2006 to December 2008, 72patients with thalamic hemorrhage weretreated in our department. All patients werescreened and the surgical indication waspatients with IVH from thalamic hemor-rhage that caused acute hydrocephalus. Pa-tients with thalamic hemorrhage not asso-ciated with IVH, patients with bleedingtendency, or secondary parenchymal hem-orrhage were excluded. This study was pro-spective and randomized. The selected pa-tients were randomly divided into twogroups: an EVD group and an endoscopicsurgery group.
OperationIn the EVD group, traditional EVDs wereperformed on patients in the supine posi-tion under local anesthesia. Patients withventricular blood received continuousdrainage at 10 cm H2O until there was nofurther reduction in cerebrospinal fluid(CSF) blood content. The EVD catheter wasthen sequentially weaned in daily incre-ments of 5 cm H2O and removed. Patientswere considered as having failed catheter“weaning” if they developed hydrocepha-lus, or if their level of conscious worsenedas a result of the weaning process. Perma-nent ventriculoperitoneal (VP) shunt sur-
Table 1. Clinical Data for the Patients wi
Data EVD (n � 24)
Age 62.17 � 10.74
Initial GCS (range) 9.83 � 3.09 (4–13)
ICH volume (mL) 11.5 � 9.56 (4–20)
Graeb Score 4.54 � 3.11 (2–8)
ICU length of stay 18 � 7
EVD, external ventricular drainage; GCS, Glasgow Coma Scintraventricular hemorrhage.
gery was performed if patients failed EVD a
WORLD NEUROSURGERY 75 [2]: 264-268
weaning. No intraventricular injection of ananticoagulant (eg, urokinase) was givenduring the procedure.
In the endoscopic surgery group, the sur-gical procedure was performed with the pa-tient in the supine position with a pillowunder the shoulder and the head turned ap-proximately 60° away, while under generalanesthesia. A 3-cm incision was made in theparietal-occipital scalp ipsilateral to IVHand the thalamic hematoma. A burr hole (1cm in diameter) was drilled using the navi-gator system guide. A transcortical trans-ventricular puncture was made with a 7-mmrigid endoscope sheath. When the ventriclewas reached, the stylet was removed and a2.7-mm, 0° endoscope (Storz) and a suctiontube were inserted through this tube, per-mitting the simultaneous removal of in-traventricular and thalamic hematomas.When a bleeding vessel was encountered,the suction tube was replaced with a 3-mmunipolar suction, coagulation tube to cau-terize the vessel. When all procedures werecomplete, an EVD was left in the ventriclefor 3 � 2 days until there was no furtherreduction in CSF blood content after whichit was removed. Permanent VP shunt sur-gery was performed if patients failed the“weaning” of the EVD. No urokinase wasgiven during this procedure.
Clinical EvaluationThe clinical evaluation data included theGlasgow Coma Scale (GCS), age, ICH vol-ume, length of ICU stay, and severity ofIVH. The volume of ICH was calculated us-ing the simplified equation 1/2A � B � C,where A is the maximum width measured,
is the length, and C is the height (9). Sever-ty of IVH was graded according to the
alamic ICH with IVH
Endoscopic (n � 24) P Value
65.54 � 11.70 0.30
8.54 � 2.78 (4–12) 0.13
10.5 � 10.74 (4–25) 0.42
6.9 � 2.98 (2–10) 0.47
11 � 5 0.04
H, intracerebral hemorrhage; ICU, intensive care unit; IVH,
mount of blood in each ventricle using the
, FEBRUARY 2011 ww
raeb score of 0 to 12, which is the sum ofhe score in each ventricle; 4 is the maxi-
um in each lateral ventricle, and 2 is theaximum in the third and fourth ventricles
6). The clinical data of the patients withhalamic ICH with IVH are listed in Table 1.
utcome Analysistelephone interview was conducted with
ll surviving patients at the time of thetudy, and the outcome at 90 days after on-et of the disease was determined. Patientunction was evaluated using the Glasgowutcome Scale. The 30-day and 90-dayortality rate and 90-day VP shunt depen-
ent rates were also evaluated.
tatistical Analysisll statistical analyses were performed us-
ng the SPSS 16.0 Statistics program. Arobability value of less than 0.05 was con-idered statistically significant. Normallyistributed data are expressed as the means
the standard deviations and were com-ared using the unpaired t test.
llustrative Case71-year-old woman was admitted to our
ospital because of an altered level of con-ciousness and left hemiparesis. On ad-ission, she was drowsy (GCS score, 9). A
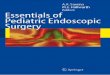
omputed tomographic scan revealed aight-sided thalamic hemorrhage with rup-ure into the ventricle and acute hydro-ephalus (Figure 1). The volume of the he-atoma was estimated to be 40 mL. As
Figure 1. Preoperative axial computedtomographic scan revealing the rupture of a
th Th
ale; IC
thalamic hematoma into the ventricle.
w.WORLDNEUROSURGERY.org 265

aitp
ws
Egi1iltncE4asrwiswo
D
TfelrtCaonlpho1adprpo
lsbndpntds(
PEER-REVIEW REPORTS
CHUN-CHUNG CHEN ET AL. ENDOSCOPIC SURGERY FOR IVH CAUSED BY THALAMIC HEMORRHAGE
previously described, the patient was intu-bated and underwent endoscopic surgeryto evacuate the hematoma. Postoperativecomputed tomographic scanning revealedcomplete removal of the thalamic hema-toma (Figure 2). A ventricular drain waskept in place for three days after the opera-tion. No intraventricular injection of an an-ticoagulant (eg, urokinase) was needed forthis patient. She regained consciousness 1week later and displayed a left-sided hemi-paresis; three months later she had a Glas-gow Outcome Scale of 3.
RESULTS
From January 2006 to December 2008, 48patients with thalamic hemorrhage andIVH were enrolled and treated in our depart-ment. All the patients had hypertensivehemorrhaging. These patients were ran-domly divided into an EVD group and anendoscopic surgery group. The clinical fea-tures of each group are shown in Table 1.No significant differences in age or GCSassessment on admission were found be-tween the two groups. There was no signif-icant differences in ICH volume or Graebscore between the endoscopic group andthe EVD group. The length of ICU stay was11 � 5 days in the endoscopic surgery group
nd 18 � 7 days in the EVD group. Patientsn the endoscopic surgery group stayed inhe ICU for a shorter time (P � 0.04) com-ared with EVD group (Table 1).
The 30-day and 90-day mortality ratesere 12.5% and 20.8% in the endoscopic
Figure 2. Postoperative axial computedtomographic scan revealing completeevacuation of the hematoma.
urgery group and 12.5% and 16.6% in the
266 www.SCIENCEDIRECT.com
VD group, respectively. The mean Glas-ow Outcome Scale score was 3.08 � 1.38
n the endoscopic surgery group and 3.33 �.40 in the EVD group. Outcome was signif-cantly correlated with initial consciousnessevel, the severity of IVH did not influencehe outcome in all cases. There was no sig-ificant difference in mortality rate or out-ome between the endoscopic group andVD group. The VP shunt rates were7.62% in the endoscopic surgery groupnd 90.48 in the EVD group. The endo-copic surgery group had lower VP shuntate (P � 0.002; odds rate � 9.8) comparedith the EVD group (Table 2). There was no
ntracranial infection and re-bleeding afterurgery in any cases, and of the total thereere 10 cases in which there was an increasef hematoma observed.
ISCUSSION
halamic hemorrhage can be divided intoour types: posterior-lateral, anterior-lat-ral, medial, and dorsal (10). The posterior-ateral type is the type of hemorrhage thatuptures into the trigone of the lateral ven-ricle. This causes obstruction of normalSF flow and also caused acute hydroceph-lus. EVD was frequently used for the relieff hydrocephalus (2). But an EVD drain canot prevent shunt-dependent hydrocepha-
ous. Hydrocephalus is associated withoor outcome, and VP shunt surgery isampered by several problems, includingbstruction, infection, and malfunction (5,2). From the literature review, both IVHnd thalamic hemorrhagic were strong pre-ictors for a permanent VP shunt, and ap-roximately 66% of all thalamic hemor-hagic patients need a shunt (14). Inatients with IVH caused by thalamic hem-rrhage, the shunt-dependent hydrocepha-
Table 2. Results for Patients with Thalam
DataEVD
(n � 24)
30-day mortality rate (%) 12.5
90-day mortality rate (%) 16.6
GOS 3.33 � 1.40
VP shunt rate (%) 90.48
CI, confidence interval; EVD, external ventricular drainage
GOS, Glasgow Outcome Scale; VP, ventriculoperitoneal.WORLD NEUROSURGE
us rate was higher than 66%. In our presenttudy, 33 patients of the 48 with IVH causedy thalamic hemorrhage needed a perma-ent VP shunt. The shunt-dependent hy-rocephalus rate was 68%, but only 47.62%atients in the endoscopic surgery groupeeded a VP shunt, whereas 90.48% of
hose in the EVD group needed shunts. En-oscopic surgery had a significantly lowerhunt-dependent hydrocephalus outcomeP � 0.002; odds ratio 9.8).
Several strategies to prevent hydrocepha-lus have been reported (7, 8, 12, 16, 17, 19,21, 24). Huttner and colleagues (8) have re-cently reported success in reducing VPshunt rates after ICH by using temporarylumbar drainage. Oertel and coworkers (19)addressed the value of the endoscopic thirdventriculostomy (ETV) in the treatment ofpatients who had suffered intracranialhemorrhage with obstructive hydrocepha-lus. They present data on 34 ETVs in 34patients who suffered from acute obstruc-tive hydrocephalus caused by intracranialhemorrhage with intraventricular exten-sion. They observed clinical and radiologi-cal improvement without intraoperativecomplications. Only two patients (5.9%)underwent VP shunt placement in their se-ries. They concluded that ETV is a safe treat-ment option in intraventricular hemor-rhage-related obstructive hydrocephalus,with similar results to external drainage,but with less risk of infection and a very lowsubsequent shunt placement rate. Otherstrategies aim to mobilize sedentary bloodand enhance CSF clearance through intra-ventricular fibrinolysis (IVF) (16, 21, 25).EVD combined with urokinase offers a sim-ple operation technique with less injury tocerebral cortex. Staykov et al. (21) investi-gated the feasibility and safety of IVF fol-lowed by early lumbar drainage (LD) for the
H with IVH
scopic24) P Value
Odds Ratio(95% CI)
2.5 1.0
0.8 0.71
� 1.38 0.54
7.62 0.002 9.8 (2.28 � 42.06)
ntracerebral hemorrhage; IVH, intraventricular fibrinolysis;
ic IC
Endo(n �
1
2
3.08
4
; ICH, i
RY, DOI:10.1016/j.wneu.2010.07.041

pbwsflemstvgsdrsdbEcmrba
cfvtIpi1ssbtta
PEER-REVIEW REPORTS
CHUN-CHUNG CHEN ET AL. ENDOSCOPIC SURGERY FOR IVH CAUSED BY THALAMIC HEMORRHAGE
treatment of posthemorrhagic hydrocepha-lus. They concluded that IVF is safe and fea-sible for posthemorrhagic hydrocephalusand may markedly reduce the need forshunt surgery. In our study, we did not per-form ETV during endoscopic surgery, be-cause our endoscopic surgery is not suitablefor removing third and fourth ventricle he-matomas. Therefore, ETV can not be doneat the end of the operation. We also did notperform IVF to hasten IVH resolution, be-cause secondary infection and re-bleedingmay result from a less accurate setting of thecatheter and drainage time is longer. In ourendoscopic surgery, we immediately andaggressive removed the thalamus hema-toma and IVH, because hematoma volumeand IVH are the prognostic factors in thethalamus ICH (10, 11, 15, 20). To avoid re-bleeding, we only removed the IVH and softthalamus clot, leaving the hard clot in thehematoma cavity (no complete evacuationof the hematoma). Our present study showsthat endoscopic surgery can decrease shunt-dependent hydrocephalus from 90.48% to47.62% in IVH caused by thalamic hemor-rhage. This may be due to the fact that endo-scopic surgery can remove intraventricularblood fast and also rapidly reverse ventriculardilatation and normalize intracranial pres-sure. Fast removal of IVH and rapid reversalof ventricle dilatation can prevent hydroceph-alus from developing. These goals can beachieved with our endoscopic procedure andthe complications often observed with othertraditional approaches are minimized. How-ever, in our endoscopic surgery group therewere 11 patients (47.62%) that had shunt-de-pendant hydrocephalus and most also hadhigher Graeb scores. Because our endoscopicprocedure can evacuate lateral ventricle he-matomas, but can not evacuate those in thethird and fourth ventricle, there were stillsome severe IVH patients that needed perma-nent VP shunts.
Among the prognostic factors associatedwith negative outcome in patients with IVH,the volume of intraventricular blood is cer-tainly one of the most relevant (18). There-fore, efficient and rapid removal of intra-ventricular blood is the primary goal in themanagement of IVH, because it will reduceventricular dilation and a allow re-equili-bration of the CSF circulation. IVH severityinfluences the occurrence of acute hydro-cephalus and the initial level of conscious-
ness, which is significantly associated withWORLD NEUROSURGERY 75 [2]: 264-268
rognosis. Priority treatment of IVH shoulde given to those ICH patients with IVHith Graeb score of 6 or more (18). Animal
tudies have demonstrated IVH causes in-ammatory response in epidermal and sub-pidermal tissue layers, as well as inflam-ation and fibrosis of the arachnoidal villi
urface (13). Therefore, fast removal of ven-ricular and subarachnoid blood may pre-ent prolonged irritation of the Pacchioniranulations and ongoing inflammatory re-ponse caused by the blood and its break-own products. This may result in fasterecovery of the granulation and avoid per-istent hydrocephalus. In our series, the en-oscopic group had higher Graeb scores,ut the VP shunt rate is lower than in theVD group. This may have occurred be-ause our endoscopic procedure can re-ove the intraventricular blood faster,
educe ventricular dilatation, and re-equili-rate the CSF circulation, resulting in thevoidance of persistent hydrocephalus.
Thalamic hemorrhage is a severe clinicalondition with an in-hospital mortality raterom 12% to 37% (4, 15), and even 52% inentricular extensive hemorrhage (22). Al-ered consciousness, IVH, hydrocephalus,CH volume, and advanced age were inde-endent predictors of in-hospital mortality
n patients with thalamic hemorrhage (10,1, 15, 20). IVH has been found to be atrong predictor of in-hospital mortality inome studies (10, 22, 23), and IVH shoulde the priority treatment in thalamic hema-
omas with ventricular extension. The mor-ality rate of thalamic hemorrhage was 12%fter 6 � 6 days after stroke and 17.3%
within 6 months in Mori et al’s. (15) series.In Chung et al’s. (4) series, the case fatalitywas 37% at the time of discharge. Steinke etal. (22) found that in-hospital mortality oc-curred in 52% of thalamic hematomas withventricular extension and that intraventric-ular extension is a powerful independentpredictor of mortality.
In this present study, the 30-day and 90-day patient mortality rates were between12.5% and 20.8% for those who had tha-lamic hemorrhage with ventricular exten-sion. The mortality rate was lower than inSteinke et al’s (22) series. However, al-though endoscopic surgery can remove tha-lamic hematoma and IVH simultaneously,our results showed that there was no differ-ence in mortality between endoscopic sur-
gery and the EVD group. Some study, FEBRUARY 2011 ww
showed that endoscopic surgery offers abetter surgical outcome than EVD in IVHtherapy (25), but in our present study, out-come was significantly correlated with ini-tial consciousness level, which did not in-fluence the severity of IVH in all patients.There was also no significant difference be-tween endoscopic surgery and EVD surgeryin IVH caused by thalamic hemorrhage.
Our study has some limitations. We didnot perform ETV and IVF to reduce the needof shunt surgery. The alternative method,first of short EVD (with lysis), and then en-doscopy, if possible with ETV, which wasintroduced by Zhang et al. (25) can perhapsreduce the need for shunt surgery and im-prove the prognosis in thalamus ICH pa-tients. Further studies are necessary for thisto be confirmed.
CONCLUSIONS
Both endoscopic surgery and EVD surgerycan decrease the mortality rate in IVHcaused by thalamic hemorrhage patients.Endoscopic surgery had a significant lowerincidence of shunt-dependent hydrocepha-lus and a shorter ICU stay compared withEVD surgery, and this can decrease the needfor permanent VP shunt in IVH caused bythalamic hemorrhage.
REFERENCES
1. Arboix A, Comes E, Garcia Eroles L, Massons J, Oli-veres M, Balcells M, Targa C: Site of bleeding andearly outcome in primary intracerebral hemorrhage.Acta Neurol Scand 105:282-288, 2002.
2. Adams RE, Diringer MN: Response to external ven-tricular drainage in spontaneous intracerebral hem-orrhage with hydrocephalus. Neurology 50:519-23,1998.
3. Chen CC, Lin HL, Cho DY: Endoscopic surgery forthalamic hemorrhage: a technical note. Surg Neurol68:438-442, 2007.
4. Chung CS, Caplan LR, Han W, Pessin MS, Lee KH,Kim JM: Thalamic hemorrhage. Brain 119:1873-1886, 1996.
5. Diringer MN, Edwards DF, Zazulia AR: Hydroceph-alus: a previously unrecognized predictor of pooroutcome from supratentorial intracerebral hemor-rhage. Stroke 29:1352-1357, 1998.
6. Graeb DA, Robertson WD, Lapointe JS, Nugent RA,Harrison PB: Computed tomographic diagnosis of
intraventricular hemorrhage. Etiology and progno-sis. Radiology 143:91-96, 1982.w.WORLDNEUROSURGERY.org 267

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
CpR
r
CD
J
A
PEER-REVIEW REPORTS
CHUN-CHUNG CHEN ET AL. ENDOSCOPIC SURGERY FOR IVH CAUSED BY THALAMIC HEMORRHAGE
7. Hamada H, Hayashi N, Kurimoto M, Umemura K,Nagai S, Kurosaki K, Kuwayama N, Endo S: Neu-roendoscopic removal of intraventricular hemor-rhage combined with hydrocephalus. Minim InvasNeurosurg 51:345-349, 2008.
8. Huttner HB, Nagel S, Tognoni E, Köhrmann M,Jüttler E, Orakcioglu B, Schellinger PD, Schwab S,Bardutzky J: Intracerebral hemorrhage with severeventricular: lumbar drainage for communicatinghydrocephalus. Stroke 38:183-187, 2007.
9. Kothari RU, Brott T, Broderick JP, Barsan WG, Sau-erbeck LR, Zuccarello M, Khoury J: The ABCsof measuring intracerebral hemorrhage volumes.Stroke 27:1304-1305, 1996.
0. Kumral E, Kocaer T, Ertubey NO, Kumral K: Tha-lamic haemorrhage—a prospective study of 100 pa-tients. Stroke 26:964-970, 1995.
1. Kwak R, Kadoya S, Suzuki T: Factors affecting theprognosis in thalamic hemorrhage. Stroke 14:493-500, 1983.
2. Longatti P, Fiorindi A, Martinuzzi A: Neuroendo-scopic aspiration of hematocephalus totails: echni-cal note. Neurosurgery 57:E409, 2005.
3. Mayfrank L, Kim Y, Kissler J, Delsing P, Gilsbach JM,Schroder JM, Weis J: Morphological changes fol-lowing experimental intraventricular hemorrhageand intraventricular fibrinolytic treatment with re-combinant tissue plasminogen activator. Acta Neu-ropathol (Berl) 100:561-567, 2000.
268 www.SCIENCEDIRECT.com
parenchymal hemorrhage. Neurocrit Care 8:235-240,2008.
5. Mori S, Sadoshima S, Ibayashi S, Fujishima M: Im-pact of thalamic hematoma on six-month mortalityand motor and cognitive outcome. Stroke 26:620-626, 1995.
6. Naff NJ, Daniel FH, Penelope MK, Stanley T, Mi-chael K, Joshua B, Ross B, Stephan AM, Eric S: In-traventricular thrombolysis speeds blood clot reso-lution: results of a pilot, prospective, randomized,double-blind, controlled trial. Neurosurgery 54:577-584, 2004.
7. Nakano T, Ohkuma H, Ebina S: Neuroenscopic sur-gery for intracerebral hemorrhage-comparison withtraditional therapies. Minim Invas Neurosurg 46:278-283, 2003.
8. Nishikawa T, Ueba T, Kajiwara M, Miyamatsu N,Yamashita K: A priority treatment of the intraven-tricular hemorrhage (IVH) should be performed inthe patients suffering intracerebral hemorrhagewith large IVH. Clinical Neurology and Neurosur-gery 111:450-453, 2009.
9. Oertel JM, Mondorf Y, Baldauf J, Schroeder HW,Gaab MR: Endoscopic third ventriculostomy for ob-structive hydrocephalus due to intracranial hemor-rhage with intraventricular extension. J Neurosurg111:1119-1126, 2009.
0. Shan SD, Kalita J, Misra UK, Mandal SK, Srivastava
WORLD NEUROSURGE
1. Staykov D, Huttner HB, Struffert T, Ganslandt O,Doerfler A, Schwab S, Bardutzky J: Intraventricularfibrinolysis and lumbar drainage for ventricularhemorrhage stroke 40:3275-3280, 2009.
2. Steinke W, Sacco RL, Mohr JP, Foulkes MA, Tatemi-chi TK, Wolf PA, Price TR, Hier DB: Thalamicstroke. Presentation and prognosis of infarcts andhemorrhages. Arch Neurol 49:703-710, 1992.
3. Weisberg LA: Thalamic hemorrhage: clinical-CTcorrelations. Neurology 36:1382-1386, 1986.
4. Yadav YR, Mukerji G, Shenoy R, Basoor A, Jain G,Nelson A: Endoscopic management of hypertensiveintraventricular haemorrhage with obstructive hy-drocephalus. BMC Neurology 7:1-9, 2007.
5. Zhang Z, Li X, Liu Y, Shao Y, Xu S, Yang Y: Applica-tion of neuroendoscopy in the treatment of intra-ventricular hemorrhage. Cerebrovasc Dis 24:91-96,2007.
onflict of interest statement: This study was supported inart by the Taiwan Department of Health Clinical Trial andesearch Center of Excellence (DOH99-TD-B-111-004).
eceived 30 March 2010; accepted 29 July 2010
itation: World Neurosurg. (2011) 75, 2:264-268.OI: 10.1016/j.wneu.2010.07.041
ournal homepage: www.WORLDNEUROSURGERY.org
vailable online: www.sciencedirect.com
4. Miller C, Tsivgoulis G, Nakaji P: Predictors of ventri-culo-peritoneal shunting after spontaneous intra-
M: Prognostic predictors of thalamic hemorrhage. JClin Neurosci 12:559-561, 2005.
1878-8750/$ - see front matter © 2011 Published by ElsevierInc.
RY, DOI:10.1016/j.wneu.2010.07.041