Embed Size (px)
Citation preview
Endoscopy Reprocessing:
Manual versus Automated
7th GCC Conference on Infection
Prevention and Control
December 2, 2013
Kuwait City, Kuwait
William R. Jarvis, M.D.
Jason and Jarvis Associates, LLC
www.jasonandjarvis.com
Brief History of Endoscopy
• In the early 1900s, the first attempts to view inside the body with lighted telescopes were made. These initial devices were often fully rigid.
• In the 1930s, semi-flexible endoscopes, called gastroscopes, were developed to view inside of the stomach.
• Fiber-optic endoscopy was pioneered by South African-born physician Basil Hirschowitz at the University of Michigan in 1957. Widespread use of fiber optic endoscopes began in the 1960s.
• A fiber optic cable is simply a bundle of microscopic glass or plastic fibers that literally allows light and images to be transmitted through curved structures.
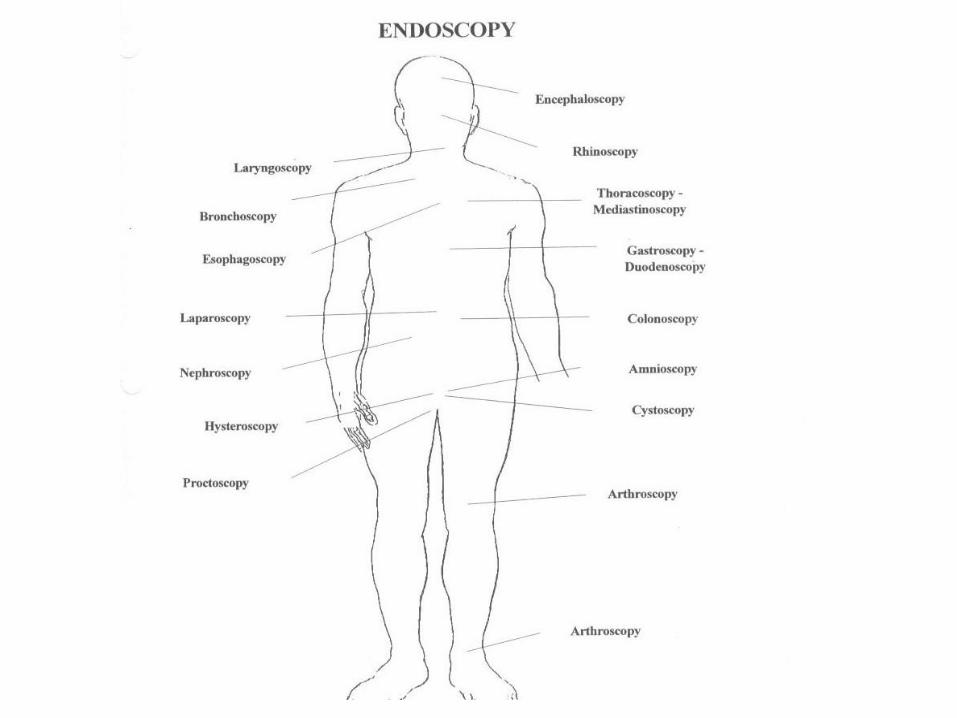
ENDOSCOPY
FLEXIBLE ENDOSCOPY
SURGICAL ENDOSCOPY
RIGID ENDOSCOPY
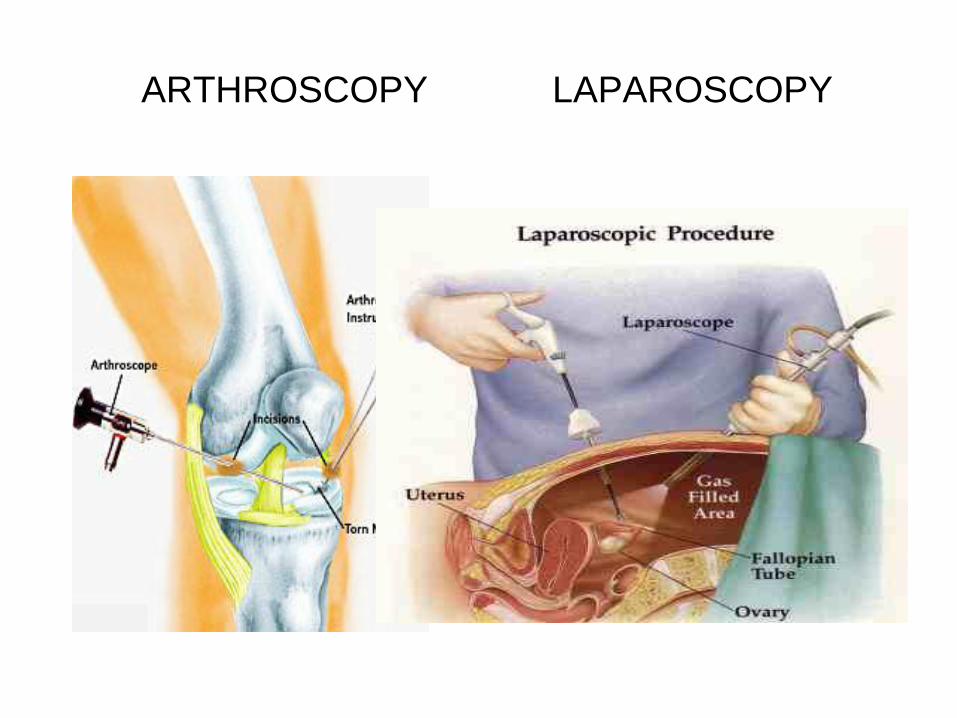
ARTHROSCOPY LAPAROSCOPY
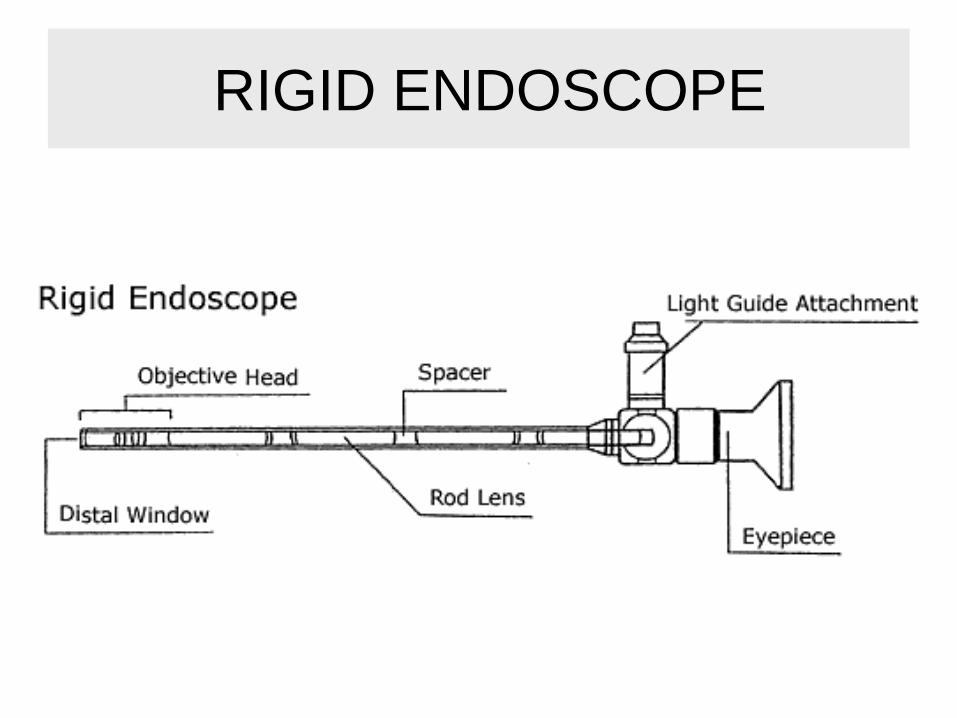
RIGID ENDOSCOPE
FLEXIBLE ENDOSCOPY
Upper Gastrointestinal Endoscopy
Gastroscopy
Duodenoscopy (ERCP)
Enteroscopy
Lower Gastrointestinal Endoscopy
Colonoscopy
Sigmoidoscopy
Respiratory Endoscopy
Bronchoscopy
Laryngoscopy
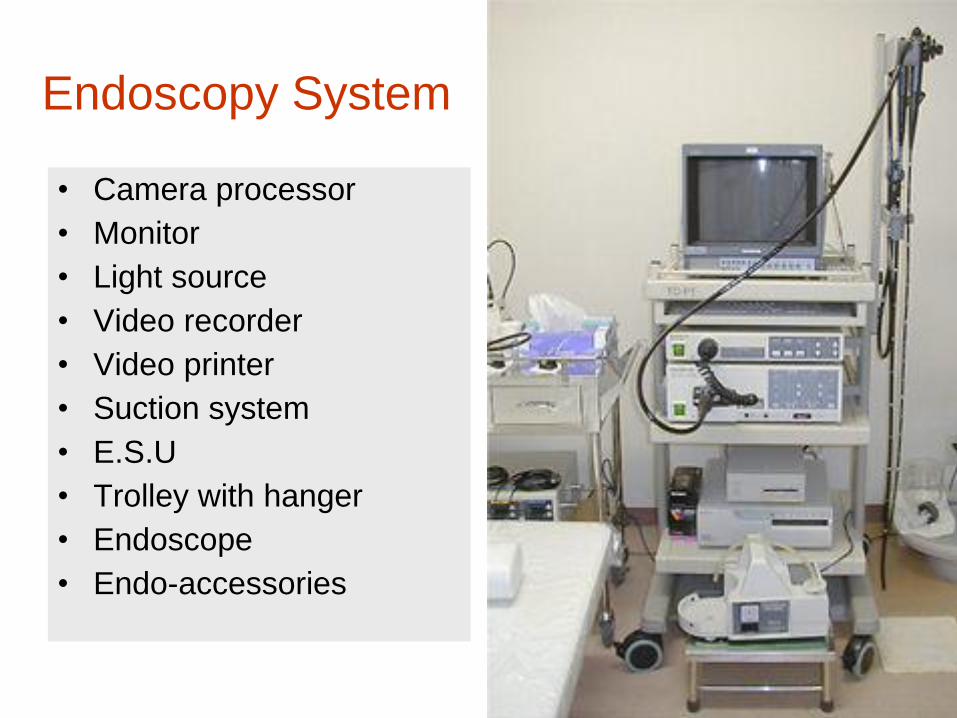
Endoscopy System
• Camera processor
• Monitor
• Light source
• Video recorder
• Video printer
• Suction system
• E.S.U
• Trolley with hanger
• Endoscope
• Endo-accessories
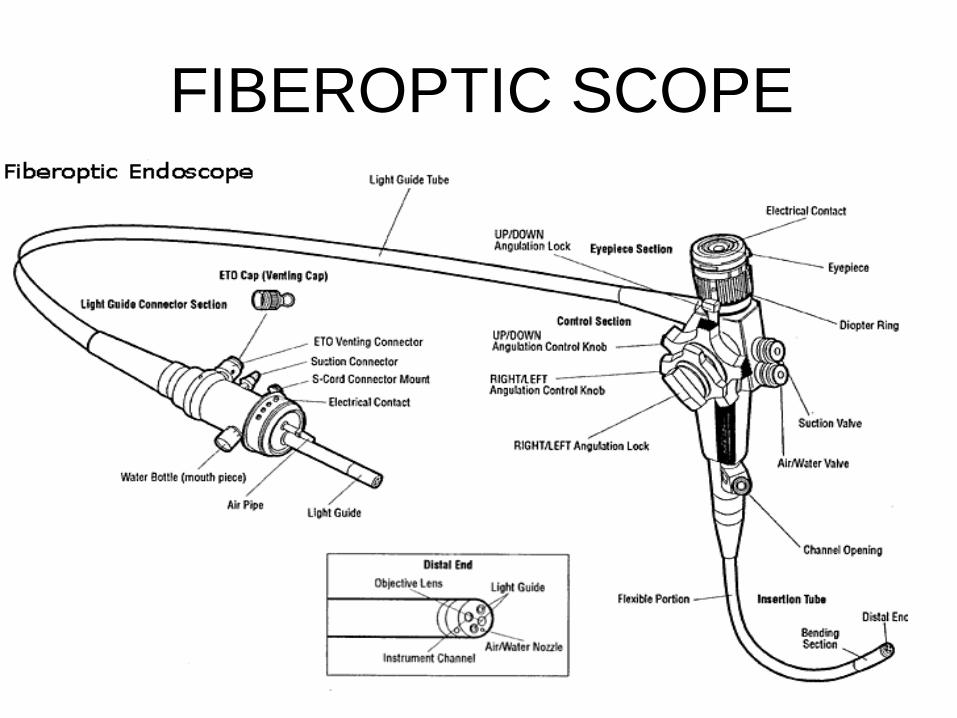
FIBEROPTIC SCOPE
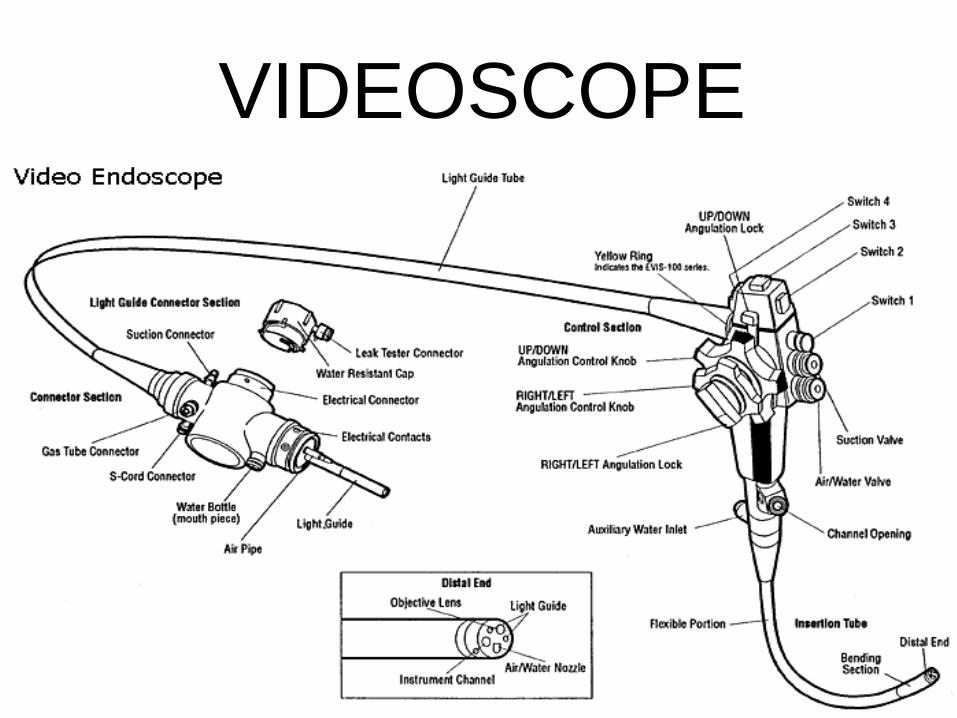
VIDEOSCOPE
Construction of Flexible
Endoscope
• Control Body
• Insertion Tube
• Light Guide Tube
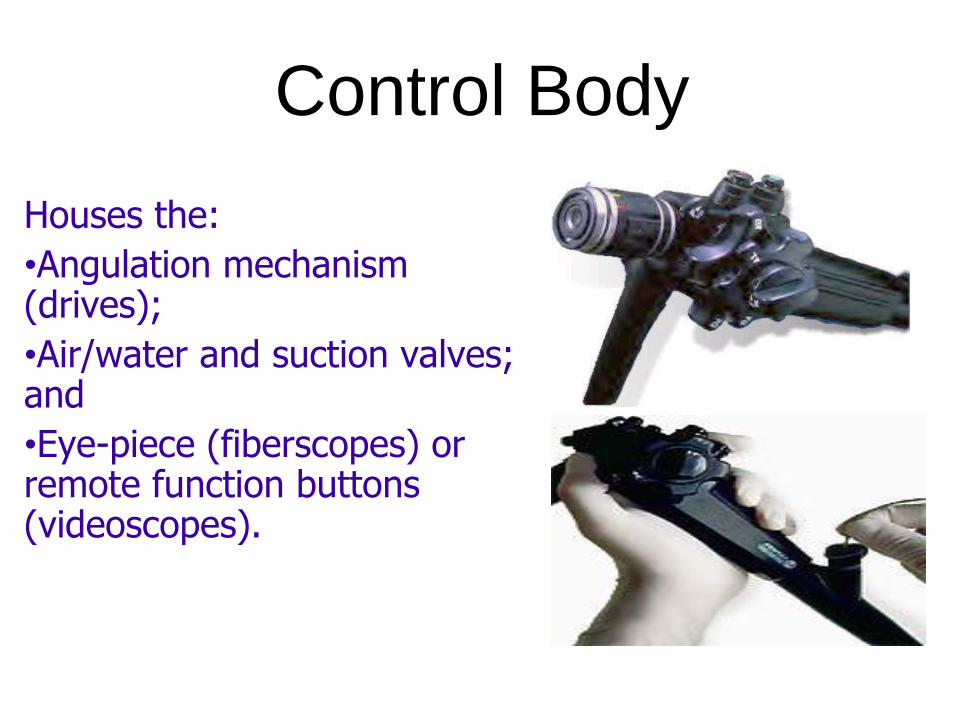
Control Body
Houses the:
•Angulation mechanism (drives);
•Air/water and suction valves; and
•Eye-piece (fiberscopes) or remote function buttons (videoscopes).
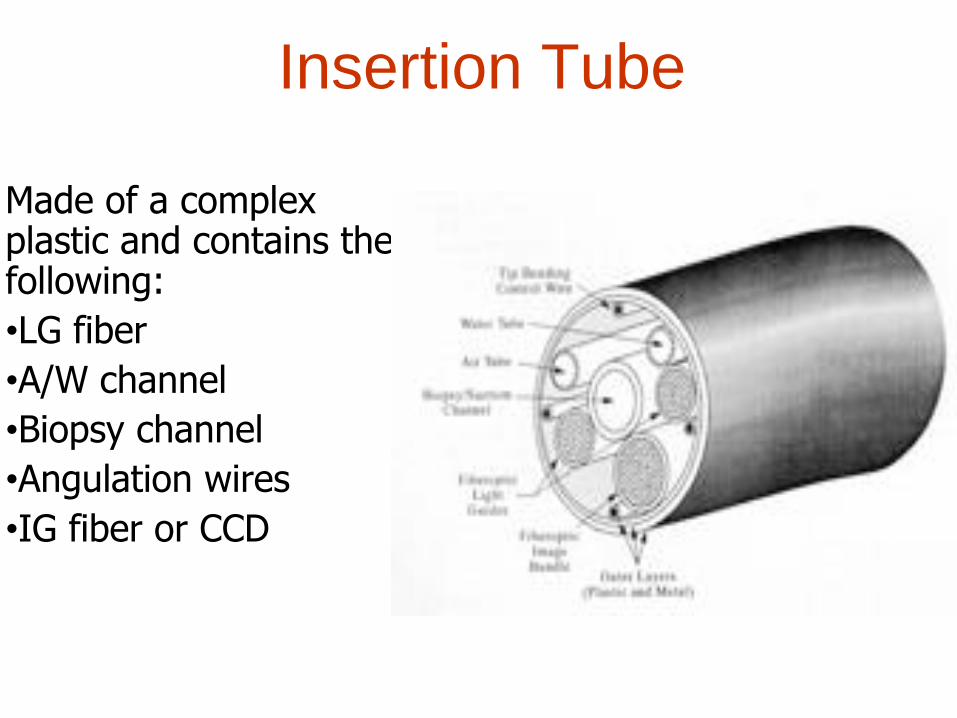
Insertion Tube
Made of a complex plastic and contains the following:
•LG fiber
•A/W channel
•Biopsy channel
•Angulation wires
•IG fiber or CCD
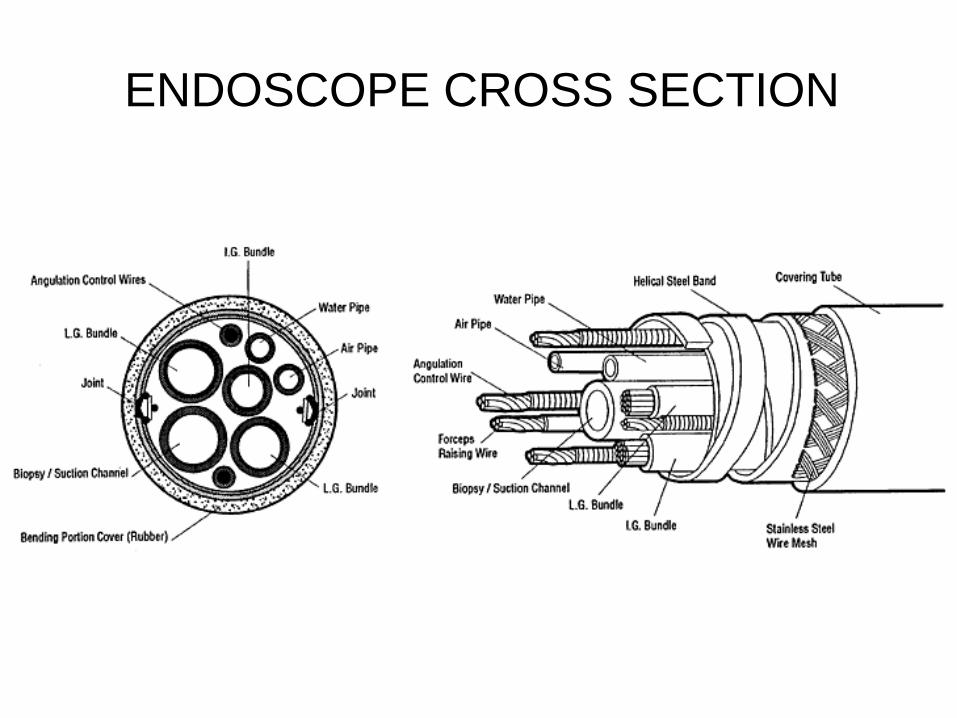
ENDOSCOPE CROSS SECTION
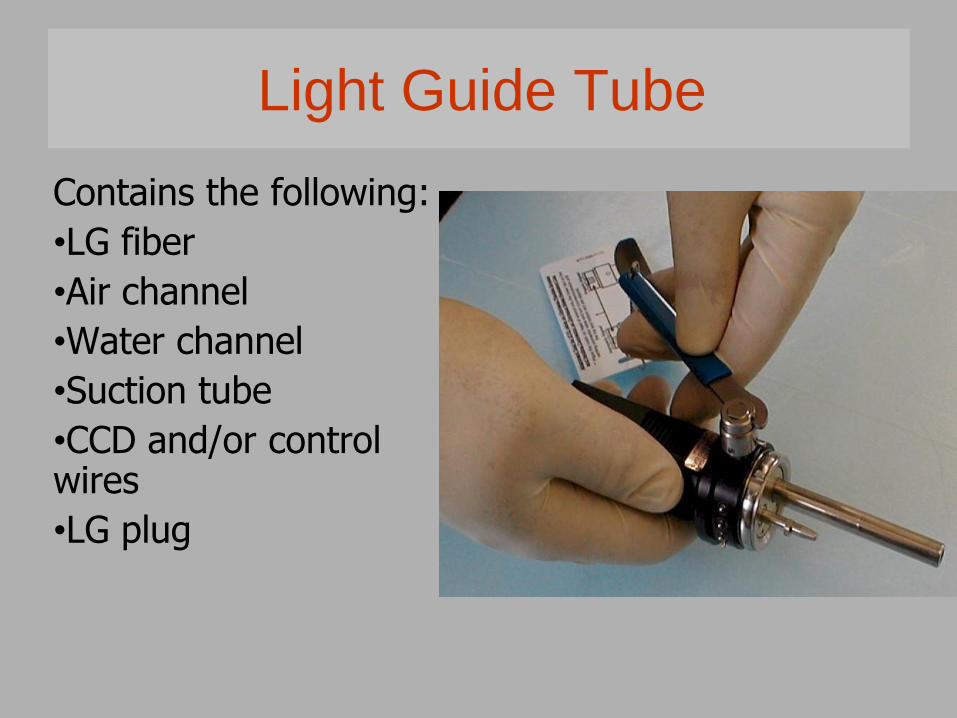
Light Guide Tube
Contains the following:
•LG fiber
•Air channel
•Water channel
•Suction tube
•CCD and/or control wires
•LG plug
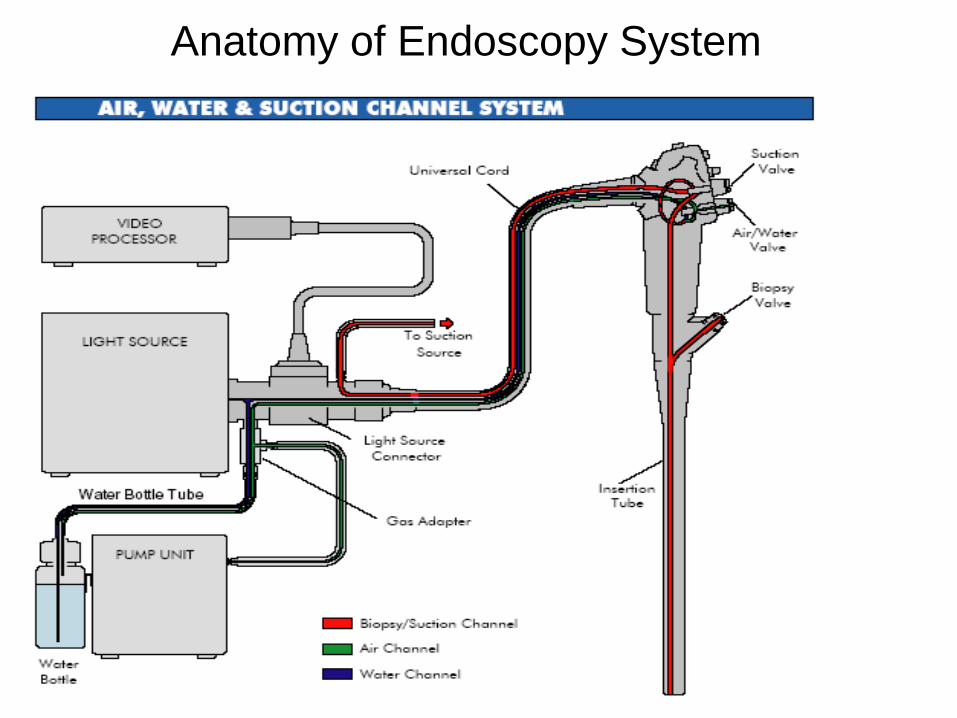
Anatomy of Endoscopy System

Endoscopic Accessories
• Biopsy forceps
• Graspers
• Baskets
• Injectors
• Dilators
• Knives
• HF endo-therapy accessories
• . . .And too many types of accessories.
PROCESSING OF ENDOSCOPES
• Mechanical Cleaning (wiping
tubes and channel brushing in a detergent
solution)
• Disinfection
• Rinsing
Endoscope Reprocessing
Device Classification
Manual Cleaning
Personal Protective Equipment
Biofilms within GI Endoscopy
Reprocessing Room Standards
Endoscope Reprocessing Protocols
Leakage Testing
Endoscope Handling
Endoscope Reprocessing
Endoscope ReprocessingTwo classifications of Endoscopes
Critical Endoscope:
• Endoscopes used in the examination of critical spaces such as joints and sterile cavities. Many of these endoscopes are rigid with no lumen. Examples of critical endoscopes are arthroscopes and laproscopes
Semi-critical Endoscope:
• Fiberoptic or video endoscopes used in the examination of the hollow viscera. These endoscopes generally invade only semicritical spaces, although some of their components might enter tissue or other critical spaces i.e., forceps. Examples of semi-critical endoscopes are colonoscopes, gastroscopes, duodenoscopes, sigmoidoscopes, laryngoscopes, nasopharangeal endoscopes and enteroscopes.
• Opinions differ regarding the reprocessing requirements of bronchoscopes; a minimum of high level disinfection is required.
Medical Device Classification
Spaulding Classification
Determines the degree of disinfection or sterilization required for various medical devices.
•Critical: A device that enters normally sterile tissue, including the vascular system. These devices should be sterilized.
•Semi-critical: A device that comes into contact with intact mucous membranes and does not ordinarily penetrate sterile tissue. These devices are cleaned followed by High Level Disinfection.
•Non-critical: Devices that do not ordinarily touch the patient or touch only intact skin. These devices may be cleaned by low-level disinfection.
Manual CleaningThorough and meticulous manual cleaning of all instruments must precede exposure to any high-level disinfectant or sterilant. This process significantly reduces the organic and microbial challenge to the high-level disinfectant or sterilant. An item that has not been cleaned cannot be assuredly disinfected or sterilized.
Refer to endoscope manufacturers’ guidelines for design features unique to a particular instrument.
Personal Protective Equipment
Should be used when reprocessing endoscopes. Gowns, gloves and protective eyewear are recommended when handling any high-level disinfectant/sterilant.
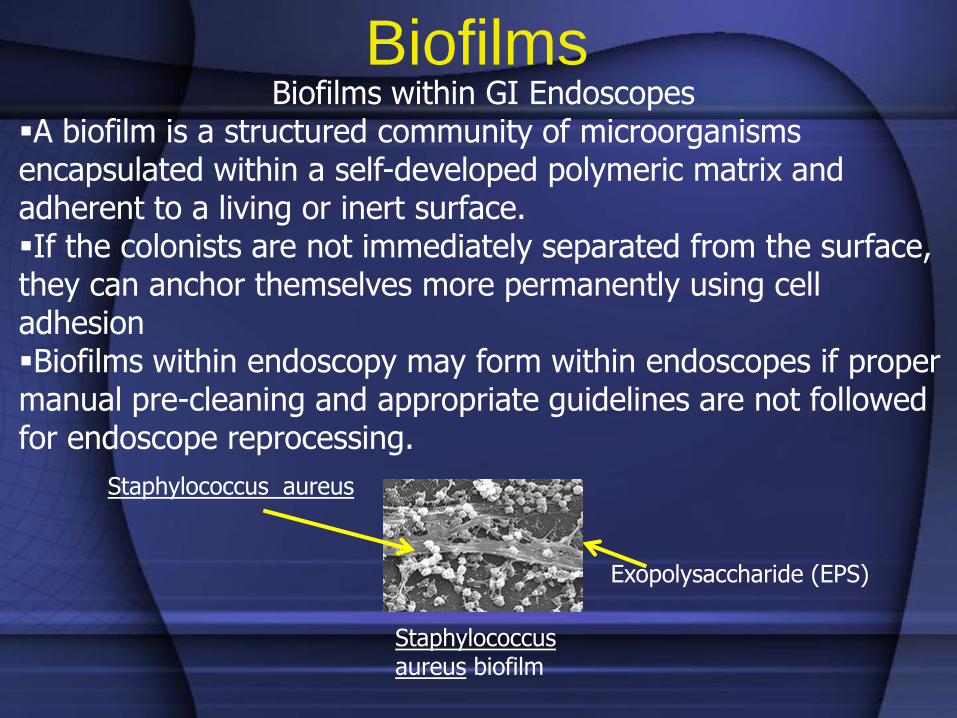
BiofilmsBiofilms within GI Endoscopes
A biofilm is a structured community of microorganisms encapsulated within a self-developed polymeric matrix and adherent to a living or inert surface.If the colonists are not immediately separated from the surface, they can anchor themselves more permanently using cell adhesionBiofilms within endoscopy may form within endoscopes if proper manual pre-cleaning and appropriate guidelines are not followed for endoscope reprocessing.
Staphylococcus aureus biofilm
Exopolysaccharide (EPS)
Staphylococcus aureus
Reprocessing Room Standards
• The process and products used for cleaning, disinfection and/or sterilization of endoscopes must be compatible with the equipment being used.
• Each healthcare setting in which endoscopic procedures are performed should have written detailed standard operating procedures (SOPs) for the cleaning and handling of endoscopes.
• Reprocessing of contaminated patient equipment should be done in an area designated and dedicated for this function.
• This room should be separate from where endoscopic procedures are performed.
• Ventilation must be capable of removing toxic vapors generated by, or emitted from, cleaning or disinfectant agents – the vapor concentration of the chemical disinfectant being used should not exceed allowable limits (e.g., 0.05 ppm for glutaraldehyde).
Reprocessing Room Standards
• Minimum of 10-12 air exchanges per hour in the reprocessing area.
• Tap water and/or water that has been filtered by passage through a 0.2 micron filter--or water of equivalent quality--should be available in the reprocessing area.
• Manual cleaning should include a medical grade, low-foaming, neutral pH enzymatic solution formulated for endoscopes that contain enzymes to digest all components of bioburden; including, blood, fat, carbohydrate, uric acid, starch.
Accessories
• Accessories which are classified as critical devices (e.g., biopsy forceps) require sterilization. Critical items labeled for single-use should not be reprocessed and/or re-used.
Transportation and Handling of
Contaminated Endoscopes• Covered containers with easily cleanable surfaces
should be used for handling and transporting soiled endoscopes.
• Soiled endoscopes should be transported by direct routes to where cleaning will be performed.
• Containers used to transport soiled endoscopes should be cleaned after each use.
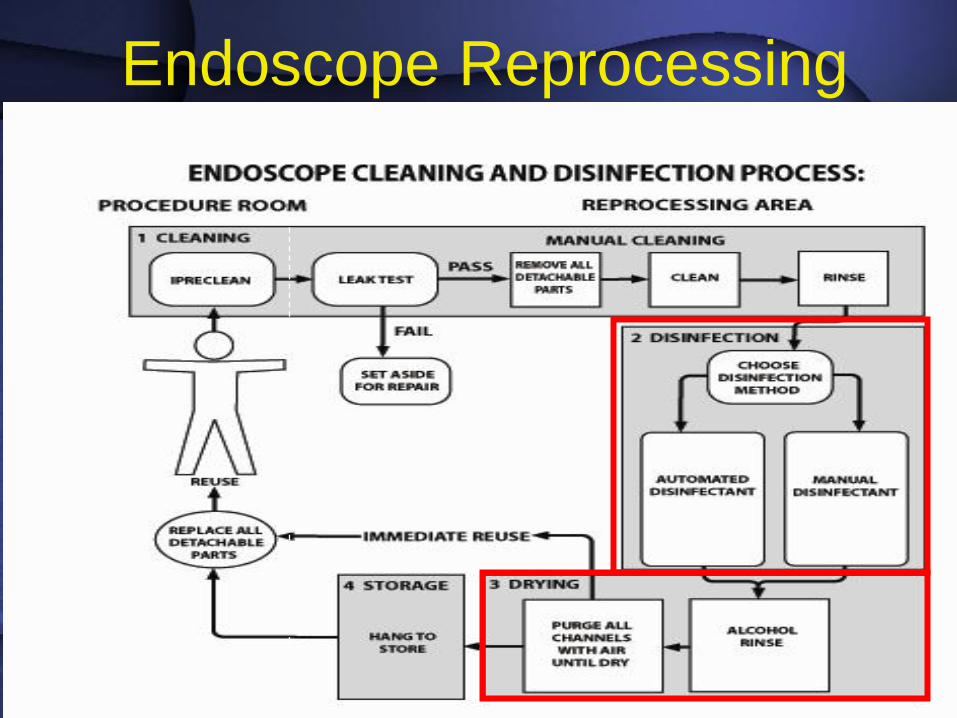
Endoscope Reprocessing Protocols
Basic steps to clean and perform high-level disinfection of gastrointestinal
endoscopes
1) Pre-cleaning
2) Leakage testing
3) Cleaning
4) Rinsing
5) Disinfection
6) Rinsing
7) Drying
8) Storage
Endoscope Reprocessing ProtocolsA. Pre-cleaning
1) Immediately after removal of the insertion tube from the patient and before disconnecting the endoscope from the power source
Prepare for bedside cleaning:
Personnel Protective Equipment (PPE)
Container with enzymatic solution
Sponge or lint-free cloth
Air and water channel cleaning adapters, per manufacturer’s instruction
Protective video cap2) Wipe the insertion tube with the wet cloth or sponge soaked
in the freshly prepared enzymatic solution. Note that the cloth/sponge should be disposed of between cases.
Endoscope Reprocessing Protocols
A. Pre-cleaning
3) Place the distal end of the endoscope into the enzymatic solution. Suction the solution through the biopsy/suction channel, alternate suctioning enzymatic solution and air several times until the solution is visibly clean – Finish by suctioning air.
Note: Alternate suctioning of fluid and air is more effective than suctioning fluid alone in the removal of debris from lumens –immediate flushing of the biopsy/suction and air/water channels precludes drying of debris on lumen surfaces.
Endoscope Reprocessing Protocols
A. Pre-cleaning
4) Flush or blow-out air and water channels in accordance with the endoscope manufacturer’s instructions.
5) Flush the auxiliary water channel.
6) Detach the endoscope from the light source and suction pump.
7) Attach the protective video cap, if using a video endoscope.
8) Transport the Endoscope to the reprocessing area in an enclosed container.
Note: Containers, sinks, and basins should be large enough that the endoscope will not be damaged by being coiled too tightly.
Endoscope Reprocessing ProtocolsB. Cleaning the Endoscope in the Reprocessing Area
Prepare the following:
PPE
Leakage testing equipment
Channel cleaning adapters
Large basin of endoscope detergent solution
Channel cleaning brushes
Sponge or lint-free cloth
C. Leak Testing
Leak testing detects damage to the interior or exterior of the endoscope.
The leak test is done before immersion of the endoscope in reprocessing solutions to minimize damage to parts of the endoscope not designed for fluid exposure.
Endoscope Reprocessing Protocols
C. Leak Testing
1. Manual Leak Testing
Remove suction valves, air water valves, and biopsy valves.
Attach the leak tester and pressurize the endoscope before submerging it in water.
With the pressurized insertion tube completely submerged, flex the distal portion of the scope in all directions, observing for bubbles.
Submerge the entire endoscope and, observing the control head of the scope, depress the freeze and release buttons.
Check the insertion tube and distal bending section as well as the universal cord for bubbles coming from the interior of the scope.
Endoscope Reprocessing Protocols
C. Leak Testing
1. Computerized leak testing: Remove suction valves, air water valves, and biopsy valves. Attach the leak tester to the computer unit. Input data, including scope ID and user. Move knobs and depress the freeze and release buttons
when indicated. Reprocess when test is complete.
Follow the endoscope manufacturer’s instructions if a leak or high humidity is detected or if the endoscope appearsdamaged.
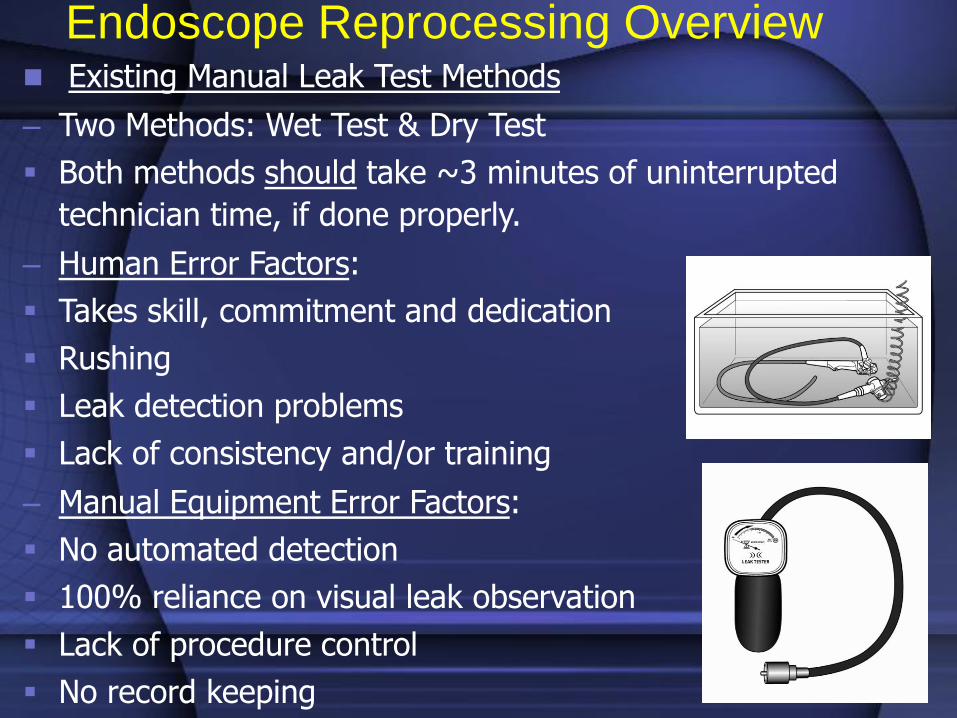
Existing Manual Leak Test Methods
– Two Methods: Wet Test & Dry Test
Both methods should take ~3 minutes of uninterrupted
technician time, if done properly.
– Human Error Factors:
Takes skill, commitment and dedication
Rushing
Leak detection problems
Lack of consistency and/or training
– Manual Equipment Error Factors:
No automated detection
100% reliance on visual leak observation
Lack of procedure control
No record keeping
Endoscope Reprocessing Overview
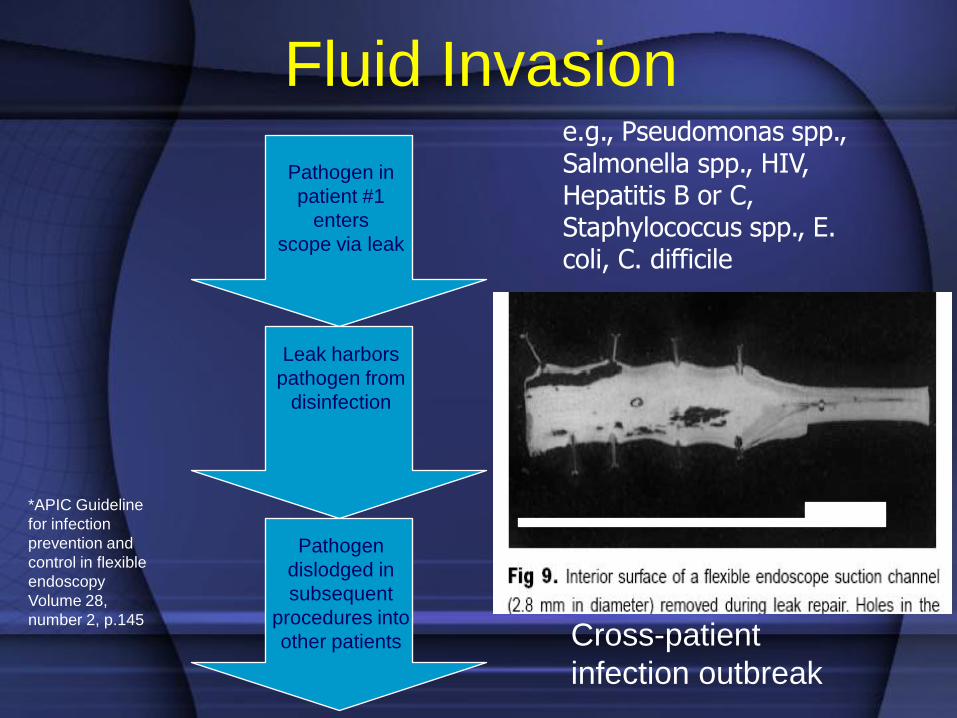
Fluid Invasion
Pathogen in
patient #1
enters
scope via leak
Cross-patient
infection outbreak
e.g., Pseudomonas spp., Salmonella spp., HIV, Hepatitis B or C, Staphylococcus spp., E. coli, C. difficile
Leak harbors
pathogen from
disinfection
Pathogen
dislodged in
subsequent
procedures into
other patients
*APIC Guideline
for infection
prevention and
control in flexible
endoscopy
Volume 28,
number 2, p.145
Endoscope Reprocessing Study Results
– 1% of endoscopy procedures result in the endoscope
developing a leak
– 65% of leaks are currently detected (35% undetected) and
undetected leaks lead to fluid invasion
– 60% of endoscope repair costs are fluid invasion-related
– .2% of endoscopy procedures result in fluid invasion
without a leak present (usually due to poor handling such as
cleaning cap left off or poorly sealed)
– 10-15% of patient-ready endoscopes possess a leak
Endoscope Reprocessing Overview
Endoscope Reprocessing Protocols
D. Cleaning Solutions
Composition of soil found on endoscopes includes, proteins, fats, carbohydrates and the various chemical salts that exist in blood and other body fluids.
Ideally, a cleaning solution should have a broad spectrum of effectiveness against these various contaminants and not harm the device being cleaned.
i) Enzymatic cleaning solutions use surfactants to breakdown and digest bioburden. They are specifically selected to have a negligible effect on surface tension while still suspending soil particles. This feature provides easy rinsibility.
Endoscope Reprocessing Protocols
E. Cleaning
Manual cleaning of endoscopes is necessary immediately after removing the endoscope from the patient and BEFORE automated or manual disinfection
Performed as the first and most important step in removing the microbial burden from an endoscope.
Retained debris may inactivate or interfere with the capability of the active ingredient of the chemical solution to effectively kill and/or inactivate microorganisms.
Endoscope Reprocessing Protocols
E. Cleaning (cont)
1. Fill a sink with freshly prepared solution of water and a medical grade, low-foaming, neutral pH detergent formulated for endoscopes – Enzymatic detergent must be discarded after each use.
2. Dilute and use according to the detergent manufacturer’s instructions.
3. Immerse the endoscope.
4. Wash all the debris from the exterior of the endoscope by brushing and wiping the instrument while submerged in the detergent solution. Note that the instrument should be left under water during the cleaning process to prevent splashing of contaminated fluid and aerosolization of bioburden.
Endoscope Reprocessing ProtocolsE. Cleaning (cont)
5. Use a small, soft brush to clean all removable parts, including inside and under the suction valve, air/water valve, and biopsy port cover and openings.
6. Brush all accessible endoscope channels including the body, insertion tube and the umbilicus of the endoscope – brushes used for cleaning lumens should be of an appropriate size, inspected before and after use and discarded or cleaned, high-level disinfected and dried following use.
7. After each passage, rinse the brush in enzymatic solution, removing any visible debris before retracting and reinserting it.
8. Continue brushing until there is no debris visible on the brush.
9. Cleaning items should be disposable or thoroughly cleaned and minimum of high-level disinfected between cases.
Endoscope Reprocessing ProtocolsE. Cleaning (cont)
10. Attach the endoscope cleaning adapters for suction, biopsy, air, and water channels.
Note: Automated pumps are available for this step that eliminate the manual flush
11. Attach the manufacturer’s cleaning adapters for special endoscope channels (i.e., dual channel, elevator channel, auxilliary channel)
i. To achieve adequate flow through all lumens, various adapters or channel restrictors may be required.
ii. The elevator channel of a duodenoscope is a small lumen, this channel requires manual reprocessing using a 2-5mm syringe.
12. Flush all channels with the detergent solution to remove debris.
13. Soak the endoscope and its internal channels for the period of time specified by the label.
14. If immediate reprocessing is not possible the endoscope should be leak-tested, flushed, brushed, and allowed to soak in a enzymatic solution until it can be thoroughly reprocessed.
Endoscope Reprocessing ProtocolsF. Rinse After Cleaning
Thoroughly rinse the endoscope and all removable parts with clean water.
Purge water from all channels using forced air. Dry the exterior of the endoscope with a soft, lint-free cloth to prevent dilution of the liquid chemical germicide used in subsequent steps.
G. High Level Disinfection (Recognized as the standard of reprocessing for endoscopes by:
Multi-Society Guideline, 11 professional organizations, 2003; Society of Gastroenterology Nurses and Associates (SGNA), 2000; European Society of Gastrointestinal Endoscopy, 2000; British Society of Gastroenterology Endoscopy, 1998; Gastroenterological Society of Australia, 1999; Gastroenterological Nurses Society of Australia, 1999; American Society for Gastrointestinal Endoscopy, 1996; Association for Professional in Infection Control and Epidemiology, 2000; Centers for Disease Control and Prevention, 2008.
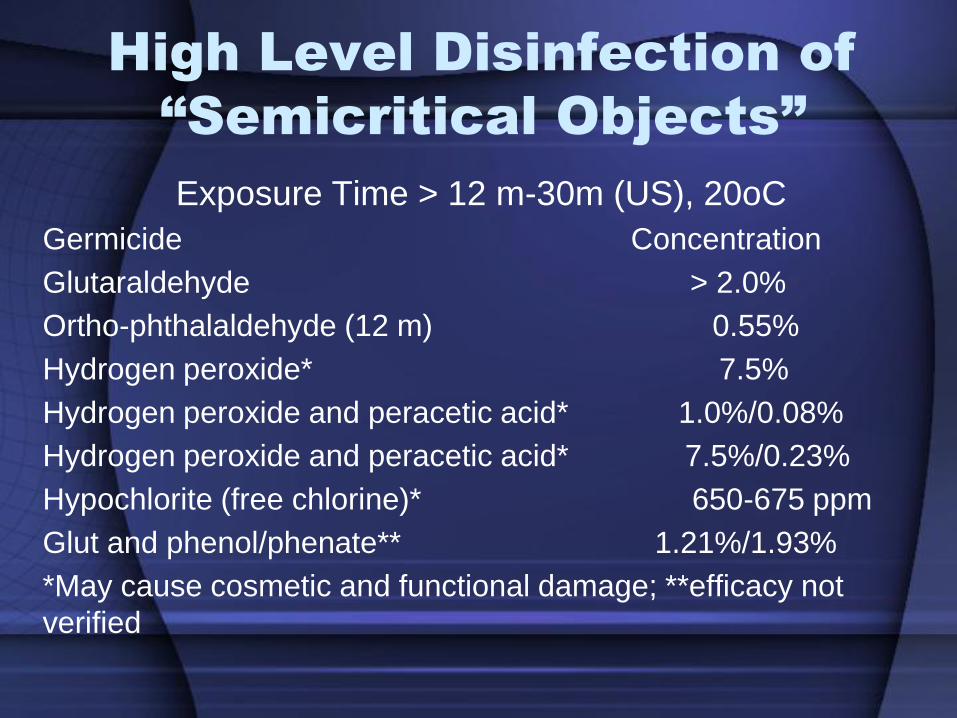
High Level Disinfection of
“Semicritical Objects”
Exposure Time > 12 m-30m (US), 20oC
Germicide Concentration
Glutaraldehyde > 2.0%
Ortho-phthalaldehyde (12 m) 0.55%
Hydrogen peroxide* 7.5%
Hydrogen peroxide and peracetic acid* 1.0%/0.08%
Hydrogen peroxide and peracetic acid* 7.5%/0.23%
Hypochlorite (free chlorine)* 650-675 ppm
Glut and phenol/phenate** 1.21%/1.93%
*May cause cosmetic and functional damage; **efficacy not
verified
New FDA-Cleared Sterilants/HLD
• “Older”
• > 2% Glut, 7.5% HP, 1.0% HP and 0.08% PA
• Newer
• 0.55% ortho-phthalaldehyde (HLD- 5 m
worldwide, 12 m in US)
• 0.95% glut and 1.64% phenol/phenate (HLD-
20 m at 25oC)
• 7.5% HP and 0.23% PA (HLD-15 m)
• 2.5% Glut (HLD-5 m at 35oC)
• Ensure antimicrobial activity and material
compatibility
Automated Endoscope Reprocessing
• Ensure that the endoscope and endoscope components are compatible with the automated endoscope reprocessor (AER).
• Follow the OEM instructions for use in the AER.
• AERs provide a method by which a permanent record of endoscope use and reprocessing can be monitored and validated.
• Some AERs have a system capable of tracking endoscopes and patients. For each procedure, the patients name and record number, the date and time of procedure, type of procedure, the endoscopist and the serial number of the endoscope are recorded and stored to assist in outbreak investigation.
Endoscope Reprocessing Protocols
F. DRYING
Purge all channels with air until dry.
Flush all channels, including accessory channels, with alcohol until the alcohol can be seen exiting the opposite end of each channel.
i. 70% isopropyl alcohol is used to assist in drying the interior channel surfaces.
ii. Use alcohol that has been properly stored in a closed container between uses – alcohol, when exposed to air, rapidly evaporates, and if below the recommended percentage level, cannot be relied upon to assist in the drying process.
iii. Alcohol flushes should be used even when sterile water is used for rinsing.
Endoscope Reprocessing Protocols
F. DRYING (cont)
• Purge all channels with air. Alcohol mixes with the remaining water on the channel surfaces and acts to encourage evaporation of the residual water as air flows through the channel.
• Remove all channel adapters.
• Dry the exterior of the endoscope with a soft, clean lint-free towel.
• Thoroughly rinse and dry all removable parts. Do not attach removable parts to the endoscope during storage as this lowers the risk of trapping liquid inside the instrument.
Endoscope Reprocessing ProtocolsF. DRYING (cont)
Drying the endoscope after every reprocessing cycle, both between patient procedures and before storage is a requisite practice crucial to the prevention of bacterial transmission. Drying is as important to the prevention of disease transmission as cleaning and high level disinfection.
Endoscope Reprocessing Protocols
G. STORAGE
• Hang the endoscope vertically, with the distal tip hanging freely in a clean, well-ventilated dust-free area.
• A storage area with good ventilation will encourage continued air drying of the surfaces, and prevent undue moisture build-up, thus discouraging any microbial contamination.
• Caps, valves and other detachable components should be removed during storage and reassembled before use.
• Colonoscopes have a minimum shelf life of 7 days, if stored dry.
Gastrointestinal Endoscopes
• Widely used diagnostic and therapeutic procedures. Endoscope contamination during use (109 colony forming unit/ml [CFU/ML] in/105 CFU/ml out). Semi-critical items require high-level disinfection minimally. Inappropriate cleaning and disinfection has lead to cross-transmission. In the inanimate environment, although the incidence remains very low, endoscopes represent a risk of disease transmission.
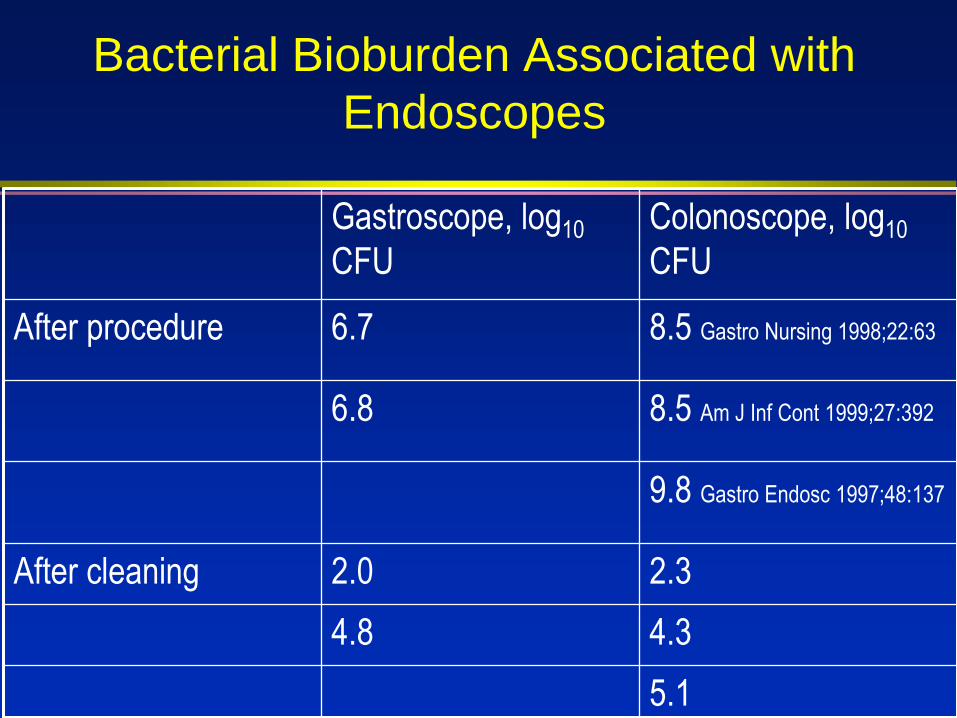
Bacterial Bioburden Associated with
Endoscopes
Gastroscope, log10
CFU
Colonoscope, log10
CFU
After procedure 6.7 8.5 Gastro Nursing 1998;22:63
6.8 8.5 Am J Inf Cont 1999;27:392
9.8 Gastro Endosc 1997;48:137
After cleaning 2.0 2.3
4.8 4.3
5.1
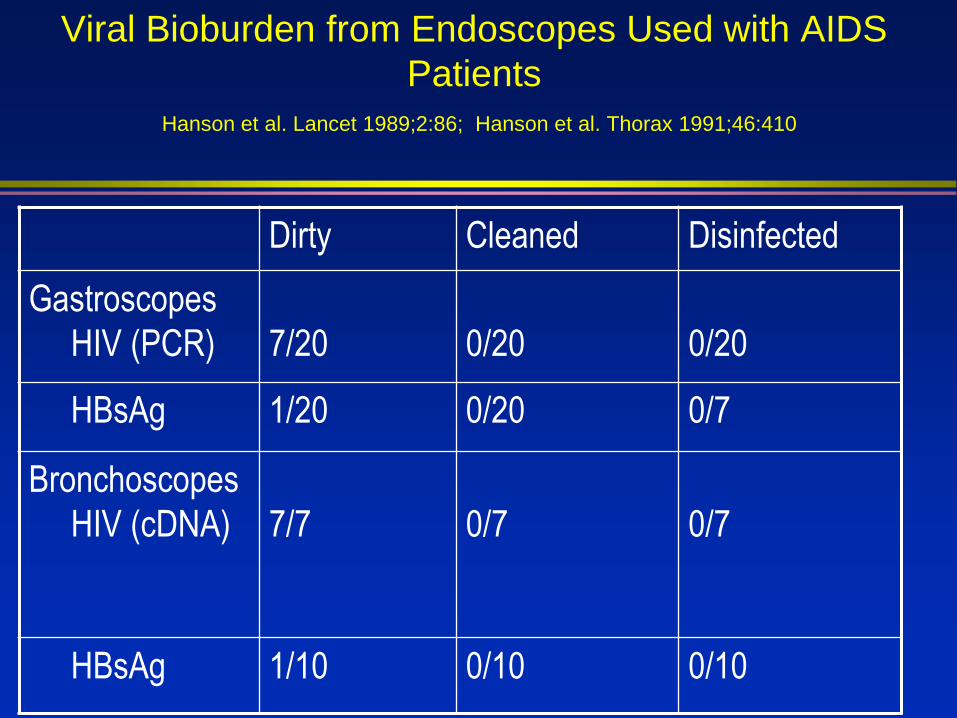
Viral Bioburden from Endoscopes Used with AIDS
Patients
Hanson et al. Lancet 1989;2:86; Hanson et al. Thorax 1991;46:410
Dirty Cleaned Disinfected
Gastroscopes
HIV (PCR) 7/20 0/20 0/20
HBsAg 1/20 0/20 0/7
Bronchoscopes
HIV (cDNA) 7/7 0/7 0/7
HBsAg 1/10 0/10 0/10
Endoscopy Pathogen Transmission
Gastrointestinal Endoscopy: >300 infections transmitted 70% agents were Salmonella spp. or P. aeruginosa. Clinical spectrum ranged from colonization to death (~4%)
Bronchoscopy: 90 infections transmitted M. tuberculosis, atypical Mycobacteria, P. aeruginosa.
Spach DH et al Ann Intern Med 1993: 118:117-128 and Weber DJ, Rutala WA Gastroint Dis 2002
Healthcare-associated Infections
Transmission via GI Endoscopes
The number of reported infections reported is small, suggesting a very low incidence. Endemic transmission may go unrecognized (e.g., inadequate surveillance, low frequency, asymptomatic infections).
Infections traced to deficient practices:
1. Inadequate cleaning (clean all channels).
2. Inappropriate/ineffective disinfection (e.g., time exposure, perfuse channels, test concentration, ineffective disinfectant, inappropriate disinfectant).
3. Failure to follow recommended disinfection practices (i.e., tapwater rinse)
4. Flaws is design of endoscopes or AERs.
Spach DH. Ann Int Med 1993;118:117 and Weber DJ, Rutala, WA. Gastroint Dis 2002
Endoscope Reprocessing,
Worldwide
Worldwide, endoscopy reprocessing varies greatly.
India, of 133 endoscopy centers, only 1/3 performed even a minimum disinfection (1% glut for 2 min).
Brazil, “a high standard …occur only exceptionally”.
Western Europe, >30% did not adequately disinfect.
Japan, found “exceedingly poor” disinfection protocols.
In the United Sates, 25% of endoscopes revealed >100,000 bacteria.
Schembre DB. Gastroint Endoscopy 2000;10:215
Healthcare-associated Infections
Transmission via GI Endoscopes
Source of contamination for infections (36
outbreaks) transmitted by GI endoscopes from
1974-2001:
Cleaning-3 (12%)
Disinfection-19 (73%)
Rinse, Dry, Store-3 (12%)
Etiology unknown-11
Endoscope Reprocessing
• High level disinfection is the standard of care for reprocessing GI endoscopes and bronchoscopes.
• The process can be completed manually or with an automatic endoscope reprocessor (AER).
• Until recently no AER substitutes for manual cleaning.
• For manual disinfection, immerse the endoscope completely in high level disinfectant (HLD) and fill each channel with the HLD.
• Cover the basin to prevent vaporization and use a timer.
• Flush the channels with air before removing the scope from the HLD.
Automatic Endoscope Reprocessors (AERs)
• Advantages: automate and standardize reprocessing
steps, reduce personnel exposure to chemicals, filtered
tap water.
• Disadvantages: failure of AERs linked to outbreaks, does
not eliminate pre-cleaning, does not monitor HLD
concentration.
• Problems: incompatible AER (side-viewing
duodenoscope); biofilm build-up; contaminated AER;
inadequate channel connectors.
• Wrong set-up or connector used (CDC MMWR
1999;48:557).
• Must ensure exposure of internal surfaces with
HLD/sterilant.
EVOTECH with Cleaning ClaimProduct Definition:
FDA-cleared claim
Integrated double-bay AER
Eliminates manual cleaning
Uses New High-Level Disinfectant
(HLD) with IP protection
Single-shot HLD
Automated testing of endoscope
channels and minimum effective
concentration of HLD
Incorporates additional features
(LAN, LCD display) Automated cleaning comparable to manual cleaning. All residual data for cleaning of the internal channels as well as external insertion tube surfaces were below the limit of <8.5ug/cm2
Reliance™ EPSEndoscope Processing System
Requires a minimal number of
connections to the endoscope channels
and uses a control boot (housing
apparatus the creates pressure
differentials to ensure connectorless fluid
flow through all channels that are
accessible through the endoscope’s
control handle channel ports). Data
demonstrate that the soil and microbial
removal effected by Reliance washing
phase was equivalent to that achieved by
optimal manual cleaning.
(Alfa, Olson, DeGagne. AJIC 2006;34:561).

Thank you