-
The Egyptian Journal of Radiology and Nuclear Medicine (2013)
44, 237–243
Egyptian Society of Radiology and Nuclear Medicine
The Egyptian Journal of Radiology andNuclearMedicine
www.elsevier.com/locate/ejrnmwww.sciencedirect.com
ORIGINAL ARTICLE
Endothelial dysfunction and subclinical atherosclerosisas
evidenced by the measurement of flow mediateddilatation of brachial
artery and carotid intimamedia thickness in patients with
rheumatoid arthritis
Noha Mohamed AbdelMaboud *, Hytham Haroon Elsaid 1
Lecturer of Radiodiagnosis, Department of Radiology, College of
Medicine, Tanta University, Egypt
Received 18 September 2012; accepted 24 December 2012Available
online 6 February 2013
A
FM
in*
GE-
hy1
+
Pe
N
03
Op
KEYWORDS
Rheumatoid arthritis;
Endothelial dysfunction;
Brachial artery flow medi-
ated dilatation;
Carotid intima media
thickness
bbreviations: RA, rheumatoid
D, flow mediated dilatati
tima media thickness; ED, en
Corresponding author. Addr
harbeya, Egypt. Tel.: +20 10mail addresses: hythamharoo
[email protected] (H
Address: Tanta University H
20 1223658711.
er review under responsibility
uclear Medicine.
Production an
78-603X � 2013 Egyptian Soen access under CC BY-NC-ND li
arthritis;
on; NO,
dothelia
ess: Tant
6864399n@yaho
.H. Elsa
ospital,
of Egyp
d hostin
ciety of
httcense.
Abstract Aim of the work: The present study aimed at evaluating
the prevalence of subclinical
atherosclerosis and cardiovascular disease by means of
assessment of carotid intima media thick-
ness and endothelium dependent function through assessment of
brachial artery flow mediated
dilatation in patients with rheumatoid arthritis.
Materials and methods: Twenty six patients with rheumatoid
arthritis and 20 healthy control
subjects underwent measurement of brachial artery FMD and CIMT
using B-mode gray scale
US for evaluating cardiovascular risk.
Results: The brachial artery FMD was –96.6–6.6% in rheumatoid
arthritis (indicating ED), and
20–25% in the control group. The CIMT was 0.50–0.72 mm in
rheumatoid arthritis and
0.35–0.47 mm in the control group.
Conclusion: The results from the present study support the use
of carotid US and endothelial func-
tion assessment by means of FMD as a useful tool to predict the
increased risk of cardiovascular
CVD, cardiovascular disease;
nitric oxide; CIMT, carotid
l dysfunction.
a University Hospital, Tanta,
5.o.com (N.M. AbdelMaboud),
id).
Tanta, Gharbeya, Egypt. Tel.:
tian Society of Radiology and
g by Elsevier
Radiology and Nuclear Medicine. Production and hosting by
Elsevier B.V. All rights reserved.
p://dx.doi.org/10.1016/j.ejrnm.2012.12.009
mailto:[email protected]:[email protected]://dx.doi.org/10.1016/j.ejrnm.2012.12.009http://www.sciencedirect.com/science/journal/0378603Xhttp://creativecommons.org/licenses/by-nc-nd/4.0/
-
Table 1 The brachial artery diamet
group.
Number D1 (mm) D
5 2.5 3
7 3 3
8 3.2 4
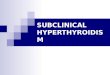
Fig. 1a T
238 N.M. AbdelMaboud, H.H. Elsaid
disease in patients with rheumatoid arthritis. We suggest that
the carotid artery US should be per-
formed for all patients with rheumatoid arthritis to establish
the risk of cardiovascular complication
which requires more aggressive therapy.
� 2013 Egyptian Society of Radiology and Nuclear Medicine.
Production and hosting by Elsevier B.V.Open access under CC
BY-NC-ND license.
1. Introduction
Rheumatoid arthritis (RA) is the most common systemic
auto-immune disease. Patients with rheumatoid arthritis are at
in-creased risk for cardiovascular diseases (CVD), one of
theearliest manifestations of CVD is endothelial
dysfunction(ED)
(1). The endothelium is the innermost lining of the
vasculatureand is responsible for maintaining vascular homeostasis
via thebalanced production of a number of vasoactive factors such
as
nitric oxide (NO) which play an important role in
vasodilata-tion and inhibiting the atherosclerotic process (2).
Damage tothe endothelium can reduce (NO) activity, causing
endothelial
dysfunction which is an early indicator of CVD (3). ED is
animportant sign of early atherosclerosis and can be assessednon
invasively by the impairment of endothelial dependantflow mediated
vasodilatation (ED-FMD) of peripheral arteries
measured by US (4). Increased carotid intima –media
thickness(CIMT), measured by US, is also regarded as an early
indica-tor of atherosclerosis and future CVD (5).
2. Patients and methods
2.1. Patients and control
The subjects in the present study were 26 RA patients (23
fe-
males and 3 males), and 20 healthy control subjects.All patients
have the following criteria: ages between 35 and
60 years, non tobacco users, did not present other
autoimmune
diseases, hypertension, diabetes mellitus, dyslipidemia,
renal
er and FMD in the control
2 (mm) FMD (%)
20
.7 23.3
25
he basal diameter of the brachia
insufficiency or received drugs affecting the
cardiovascularsystem.
20 healthy volunteers were recruited as control .Writtenconsent
was taken from all patients and the control groupand the
institutional ethics committee approved the study
protocol.
2.2. Methods: Radiological assessment by US
2.2.1. Carotid US
The subject was made to lie supine with slight hyperextensionof
the neck .Both common carotid arteries were examined
using a 7 MHz linear array transducer in a PHILIPS
HD11instrument. Carotid intima –media thickness and lumen diam-eter
were measured from end diastolic M-mode images (mini-
mum distension) of the wall of the distal common carotidartery
in a location not containing plaque. The greater distancebetween
lumen – intima and media-adventitia interface was
measured. The mean value of the two sides was taken.
2.3. Flow mediated vasodilatation of brachial artery
The procedure was performed on the same US machine andthe same
transducer as used in carotid US.
The subject lies in a supine position; the right brachial
ar-tery was scanned in longitudinal section 2–15 cm. above the
antecubital fossa with B-mode. The clearest picture of the
ar-tery at the center was obtained (the transducer was kept
con-stant throughout the procedure by noting the relation of
the
artery with the adjacent anatomical landmarks).The
luminaldiameter of the artery was measured by calculating the
dis-tance between the proximal and distal intima. Ischemia was
in-
duced with a sphygmomanometer cuff placed around theforearm
distal to the scanned region inflated to 200 mmHGfor 4 min and then
released. A second scan was taken at thisstage and the luminal
diameter was measured 60 s. after cuff
deflation .The endothelium dependant function is defined bythe
formula: D2-D1/D1x100 the higher the numeric value ofthe study ,
the better the endothelial function. ED is considered
when the FMD is
-
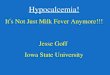
Fig. 1b The post- occlusion diameter of brachial artery in the
same person = 4 mm, FMD 25% denoting good endothelial function.
Fig. 1c The carotid intima media thickness 0.44 mm.
Table 2 The brachial artery diameter and FMD in the
rheumatoid arthritis patients.
Number D1 (mm) D2 (mm) FMD (%)
10 4.3 4.3 0
8 4.1 4.3 4.8
3 3 3.2 6.6
5 3 3.4 �96.6
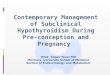
Fig. 2a The basal diameter of the brachial artery i
Endothelial dysfunction and subclinical atherosclerosisas
evidenced by the measurement of flow mediated 239
3. Results
This study included 26 patients of rheumatoid arthritis with
anage range of 35–60 years and 20 healthy control subjects with
the same age range.Table 1 shows the characteristics of the
study group in
which the diameter of the brachial artery before the
induction
of ischemia (D1) was 2.5 mm in five subjects, after the
releaseof ischemia (D2) 3 mm, the FMD was 20%.D1was 3 mm in se-ven
subjects, D2 was 3.7 mm and FMD was 23.3%.D1 was 3.2
in eight subjects, D2 was 4 mm and the FMD was 25% Fig. 1aand
b.
Table 2 shows the characteristics of the rheumatoid arthri-
tis group in which the diameter of the brachial artery beforethe
induction of ischemia (D1) was 4.3 mm in 10 subjects, afterthe
release of ischemia (D2) 4.3 mm, the FMD was 0% D1 was4.1 mm in
eight subjects, D2 was 4.3 mm and FMD was 4.8%.
D1 was 3 in three subjects, D2 was 3.2 mm and the FMD was6.6%.
D1 was 3 in five subjects, D2 was 3.4 mm and the FMDwas –96.6%
Figs. 2a and b, 3a and b, 4a and b.
So, the higher the numeric value of the FMD, the better
theendothelial function.
The CIMT in the control group was 0.44 mm in eight per-
sons, 0.47 mm in nine persons, and 0.35 mm in three personsFig.
1c Table 3.
The CIMT in the rheumatoid arthritis patients was
0.50 mm in 10 persons, 0.54 mm in nine persons, and0.56 mm in
seven persons Figs. 2c, 3c and 4c Table 4.
n a patient with rheumatoid arthritis = 4.3 mm.
-
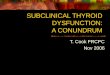
Fig. 2b The post- occlusion diameter of brachial artery in the
same person = 4.3 mm, FMD 0% denoting poor endothelial
function.
Fig. 2c The carotid intima media thickness in the same
person
0.72 mm.
240 N.M. AbdelMaboud, H.H. Elsaid
4. Discussion
Rheumatoid arthritis is associated with excessive
cardiovascu-lar mortality [6]. Almost half of all deaths in
rheumatoidarthritis results from cardiovascular causes (7).
Therefore, it
may be suggested that the main cause of mortality and morbid-ity
is ischemic heart disease in patients with RA (7). Discovery
Fig. 3a The basal diameter of brachial artery in
of early interventions in RA disease that might influence
ath-erosclerotic progression are essentials to determine
approachesthat could in turn reduce the subsequent risk of
cardiovascularmortality (8,9). CIMT is a known strong predictor of
cardio-
vascular events in the general population (10), and has
beenpredominantly reported in the literature on patients with
RA(11). The results from our study show that the CIMT has a
high predictive value for the development of CVD. Our
resultswere the same as Gonzalez–Juanatey C et al. (12) in which
thepresence of subclinical atherosclerosis, manifested by
increased
value of CIMT is consistent with the high rate of silent
ische-mic heart diseases and sudden cardiac death observed in
RApatients. Van Sijl AM et al (13) proved in their study thatCIMT
is frequently used to identify the population at elevated
cardiovascular risk. (17) The results of our study implicate
thatthe mean CIMT of the common carotid artery was signifi-cantly
higher in RA patients than in healthy subjects. Van Sijl
AM etal (13), found that the CIMT difference between RA
pa-tients and the control subject may be very small as inHigginsJP
et al. (14) and other studies such as Kumeda Y et al. (15)
& Mahajan V et al. (16) found a greater difference.
Finally,Van Sijl AM etal (13) stated that the variation in
ultrasoundprotocols for determining CIMT between all studies is
an
important observation but also complicates the interpretationof
the individual study results. Still, they think that the
differ-ences in ultrasound protocols or in other methodological
as-pects are unlikely to have caused a systematic bias toward
under - or overestimation of CIMT difference between RA
pa-tients and control. So, US scanning of CIMT has been shownto be
an accurate method for estimating cardiovascular risk
a patient with rheumatoid arthritis = 4.1 mm.
-
Fig. 3b The post- occlusion diameter of brachial artery in the
same person = 4.3 mm, FMD 4.8% denoting poor endothelial
function.
Fig. 3c The carotid intima media thickness in the same
person
0.64 mm.
Endothelial dysfunction and subclinical atherosclerosisas
evidenced by the measurement of flow mediated 241
(17). RA appears to be associated with accelerated
atheroscle-rosis, the mechanisms involved are not clear, but may
includeendothelial dysfunction mediated by systemic
inflammation(18). Our study demonstrates that patients with RA can
also
present endothelial dysfunction which may be the earliest
event
Fig. 4a The basal diameter of brachial artery in
in the atheromatous lesion, so its evaluation is a promisingtool
for the estimation of coronary affection. Castro PT
et al. (19) study mentioned that FMD allows an adequate
eval-uation of endothelial behavior and reflects the coronary
endo-thelial function and behavior inspite of that the ideal
methodfor diagnosing endothelial dysfunction has not been
estab-
lished yet. Our study coincides with those of Schroeder Set al.
(20) in which the age of the patient does not affect theendothelial
function evaluation with FMD. We have found
no significant difference in the different age groups of
patientsand the control group regarding the FMD .Like the
presentstudy, other studies like Hurlimann D et al. (21) have
found
a significant endothelial dysfunction in patients with
autoim-mune disease like RA by means of FMD .The presence of
sys-temic inflammation predisposes to atherosclerosis, affectingthe
endothelial function and decreasing the production of ni-
tric oxide by the endothelium, this decrease in the nitric
oxideproduction leads to a smaller arterial dilatation upon
inducedischemia. Quyyumi AA (22) affirms that systemic
inflamma-
tion markers like FMD, CIMT and pulse wave analysis ariseas a
method for evaluating the atherosclerosis risk .He recom-mends the
inclusion of these methods in randomized study for
screening and diagnosis of cardiovascular risk. Consideringthat
a high level of systemic inflammation affects the endothe-lial
function, inflammation markers like FMD may provide a
better evaluation for the cardiovascular risk in patients withRA
(23). In our study, we demonstrate that the FMD and
a patient with rheumatoid arthritis = 3 mm.
-
Fig. 4b The post-occlusion diameter of brachial artery in the
same person = 3.2 mm, FMD 6.6% denoting poor endothelial
function.
Table 3 CIMT in the control group.
Number CIMT (mm)
8 0.44
9 0.47
3 0.35
Table 4 CIMT in the rheumatoid arthritis patients.
Number CIMT (mm)
10 0.50
9 0.54
7 0.56
Fig. 4c The carotid intima media thickness in the same
person
0.50 mm.
242 N.M. AbdelMaboud, H.H. Elsaid
CIMT are promising methods for the evaluation of RA andare very
helpful for the prevention of vascular risk.
5. Conclusion
The results from the present study support the use of
carotid
US and endothelial function assessment by means of FMDas a
useful tool to predict the increased risk of cardiovasculrdisease
in patient with rheumatoid arthritis. We suggest that
the carotid artery US should be performed for all patients
withrheumatoid arthritis to establish the risk of
cardiovascularcomplication which requires more aggressive
therapy.
References
(1) Sandool A, Carroll D, Metsios GS, Kitas GD, Zanten VV.
The
association between microvascular and macrovascular
endothelial
function in patients with rheumatoid arthritis. Arthritis Res
Ther
2011:13.
(2) Ahluwalia A, Foster P, Scotland RS, Mclean PG, Mathur A,
Perretti M, et al. Antiinflammatory activity of soluble
guanylate
cyclase: Cgmp-dependent down–regulation of P-selection
expres-
sion and leukocyte recruitment. Proc Natl Aead Sci USA
2004;101:1386–91.
(3) Lerman A, Zeiher AM. Endothelial function: cardiac
events.
Circulation 2005;111:363–8.
(4) Gonzalez-Juanatey C, Llorca J, Martin J, Gonzalez –Gay
MA.
Carotid intima–media thickness predicts the development of
cardiovascular events in patients with rheumatoid arthritis.
Semin
Arthritis Rheum 2009;38:366–71.
(5) Adhikari MC, Guin A, Chakraborty S, Sinhamahapatra P,
Ghosh A. Subcilinical atherosclerosis and endothelial
dysfunction
in patients with early rheumatoid arthritis as evidenced by
measurement of carotid intima media thickness and flow medi-
ated vasodilatation: an observational study. Elsevier; 2011.
(6) Vaudo G, Marchesi S, Gerli R, Allegrucci R, Giordano A,
Siepi
D, et al. Endothelial dysfunction in young patients with
rheu-
matoid arthritis and low disease activity. Ann Rheum Dis
2004;63:31–5.
(7) Castro PT, Montenegro CA, Carvalho ACP, Filho JF,
Bianchi
W, Bianchi DV, et al. Brachial artery flow–mediated dilatation
in
women with rheumatoid arthritis. Radiol Bras 2007;40:4.
(8) Hannawi S, Marwick TH, Thomas R. Inflammation predicts
accelerated brachial arterial wall changes in patients with
recent-
onset rheumatoid arthritis. Arthritis Res Ther
2009;11(2):R51.
(9) Del Rincon ID, Williams K, Stern MP, Freeman GL,
Escalante
A. High incidence of cardiovascular events in a rheumatoid
arthritis cohort not explained by traditional cardiac risk
factors.
Arthritis Rheum 2001;44:2737–45.
-
Endothelial dysfunction and subclinical atherosclerosisas
evidenced by the measurement of flow mediated 243
(10) Bax L, YuLM, IkedaN, TsurutaH,MoonsKG. Development and
validation of MIX: comprehensive free software for
meta-analysis
of causal research data. BMC Med Res Methodol 2006;6(6):50.
(11) Tyrrel PN, Beyene J, Feldman BM, McCrindle BW,
Silverman
ED, Bradley JT. Rheumatic disease and carotid intima-media
thickness: a systematic review and meta-analysis. Epud May
2010;30(5):1014–26.
(12) Ciftci O, Yilmaz S, Topcu S, Cahskan M, Gullu H, Erdogan
D,
et al. Impaired coronary microvascular function and
increased
intima–media thickness in rheumatoid arthritis.
Atherosclerosis
2008;198:332–7.
(13) Van Sijl AM, Peters MJ, Knol DK, de Vet HC,
Gonzalez-Gay
MA, Smulders YM, et al. Carotid intima media thickness in
rheumatoid arthritis as compared to control subjects: a
meta-
analysis. Semin Arthritis Rheum 2011 Apr;40(5):389–97.
(14) Roman MJ, Moeller E, Davis A, Paget SA, Crow MK,
Lockshin
MD. Atherosclerosis in patients with rheumatoid arthritis.
Ann
Intern Med 2006;144(4):249–56.
(15) Kumeda Y, Inaba M, Goto H, Nagata M, Henmi Y, Furumitsu
Y. Increased thickness of the arterial intima-media detected
by
ultrasonography in patients with rheumatoid arthritis.
Arthritis
Rheum 2002;46(6):1489–97.
(16) Mahajan V, Handa R, Kumar U, Sharma S, Gulati G, Pandey
RM. Assessment of atherosclerosis by carotid intimomedial
thickness in patientswith rheumatoid arthritis. J Assoc
Physicians
India 2008;56:587–90.
(17) O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL,
Wolfson SK. Cardiovascular health study collaborative
research
group. Carotid artery intima and media thickness as a risk
factor
for myocardial infarction and stroke in older adults. N Engl
J
Med 1999;340(1):14–22.
(18) Doornum SV, McColl G, Jenkins A, Green DJ, Wicks IP.
Screening for atherosclerosis in patients with rheumatoid
arthri-
tis: comparison of two in vivo tests of vascular fubnction.
Arthritis Rheum 2003;46:862–73.
(19) Bacon PA, Stevens RJ, Carruthers DM, Young SP, Kitas
GD.
Acclerated atherogenesis in autoimmune rheumatic disease.
Review 2002;1(6):338–47.
(20) Juanatey CG, Llorca J, Martin J, Gonzalez-Gay MA.
Carotid
intima–media thickness predicts the development of
cardiovascu-
lar events in patients with rheumatoid arthritis. Semin
Arthritis
Rheum 2009;38:366–71.
(21) Schroeder S, Enderle MD, Baumbach A, Enseleit F,
Chenevard
R, Distlcr O, et al. Influence of vessel size, age and body
mass
index on the flow–mediated dilatation of the brachila artery.
Int J
Cardiol 2000;76:219–25.
(22) Hurlimann D, Forster A, Noll G. Anti tumour necrosis
factor–
alpha treatment improves endothelial function in patients
with
rheumatoid arthritis. Circulation 2002;106:2184–7.
(23) Quyyumi AA. Inflamed joints and stiff arteries: is
rheumatoid
arthritis a cardiovascular risk factor? Circulation
2006;114:
1137–9.
Endothelial dysfunction and subclinical atherosclerosis as
evidenced by the measurement of flow mediated dilatation of
brachial artery and carotid intima media thickness in patients with
rheumatoid arthr1 Introduction2 Patients and methods2.1 Patients
and control2.2 Methods: Radiological assessment by US2.2.1 Carotid
US
2.3 Flow mediated vasodilatation of brachial artery
3 Results4 Discussion5 ConclusionReferences