Embed Size (px)
Citation preview

Endothelial function and sleep: associations of flow-mediateddilation with perceived sleep quality and rapid eye movement(REM) sleep
DEN I SE C . COOPER 1 , M I CHAEL G . Z I EGLER 2 , M I LOS S . M I L I C 2 ,SON I A ANCOL I - I SRAE L 3 , P AUL J . M I L L S 3 , J OS �E S . LOREDO 2 ,ROLAND VON KÄNEL 4 and JOE L E . D IMSDALE 3
1Health Services Research and Development, VA Puget Sound Health Care System, Seattle, WA, USA, 2Department of Medicine, University ofCalifornia-San Diego, La Jolla, CA, USA, 3Department of Psychiatry, University of California-San Diego, La Jolla, CA, USA and 4Division ofPsychosomatic Medicine, Department of General Internal Medicine, Inselspital, Bern University Hospital and University of Bern, Bern,Switzerland
Keywordsendothelial function, polysomnography, sleep,subjective sleep quality, vasodilation
CorrespondenceDenise C. Cooper, PhD, Health ServicesResearch and Development, VA Puget SoundHealth Care System, 1100 Olive Way, Suite1400, Seattle, WA 98101, USA.Tel.: 206-277-4185;fax: 206-764-2935;e-mails: [email protected] [email protected]
Accepted in revised form 13 July 2013; received3 January 2013
DOI: 10.1111/jsr.12083
SUMMARYEndothelial function typically precedes clinical manifestations of cardio-vascular disease and provides a potential mechanism for the associa-tions observed between cardiovascular disease and sleep quality. Thisstudy examined how subjective and objective indicators of sleep qualityrelate to endothelial function, as measured by brachial artery flow-mediated dilation (FMD). In a clinical research centre, 100 non-shiftworking adults (mean age: 36 years) completed FMD testing and thePittsburgh Sleep Quality Index, along with a polysomnography assess-ment to obtain the following measures: slow wave sleep, percentagerapid eye movement (REM) sleep, REM sleep latency, total arousalindex, total sleep time, wake after sleep onset, sleep efficiency andapnea–hypopnea index. Bivariate correlations and follow-up multipleregressions examined how FMD related to subjective (i.e. PittsburghSleep Quality Index scores) and objective (i.e. polysomnography-derived) indicators of sleep quality. After FMD showed bivariate corre-lations with Pittsburgh Sleep Quality Index scores, percentage REMsleep and REM latency, further examination with separate regressionmodels indicated that these associations remained significant afteradjustments for sex, age, race, hypertension, body mass index, apnea–hypopnea index, smoking and income (Ps < 0.05). Specifically, as FMDdecreased, scores on the Pittsburgh Sleep Quality Index increased(indicating decreased subjective sleep quality) and percentage REMsleep decreased, while REM sleep latency increased (Ps < 0.05). Poorersubjective sleep quality and adverse changes in REM sleep wereassociated with diminished vasodilation, which could link sleepdisturbances to cardiovascular disease.
INTRODUCTION
Research has linked poor sleep quality (e.g. insufficient sleepduration, self-reported low sleep quality) to the incidence ofcardiovascular disease (CVD), primarily systemic hyperten-sion and possibly myocardial infarction, congestive heartfailure and stroke (Hoevenaar-Blom et al., 2011; Wolk et al.,2005). While the physiological underpinnings of the sleep and
CVD relationship are not yet well defined, one plausiblemechanism may be endothelial dysfunction, which is found inthe early stages of atherosclerosis (Wolk et al., 2005).Circulating markers of endothelial cell activation and damage(e.g. von Willebrand factor, endothelin-1) are increasedamong patients with obstructive sleep apnea (OSA) com-pared to healthy controls (El Solh et al., 2008; Phillipset al.,1999; Zamarr�on-Sanz et al., 2006) and among
ª 2013 European Sleep Research Society 1
J Sleep Res. (2013) Regular Research Paper

relatively healthy adults with increased sleep disturbance,according to both self-reports (von K€anel et al., 2010) andpolysomnography derived indices of sleep (e.g. latency inrapid eye movement or REM sleep) (von K€anel et al., 2007,2010; Mills et al., 2007).Although circulating biomarkers are useful indicators of
endothelial conditions, flow-mediated dilation (FMD) offers amore direct way to assess endothelial dysfunction (Moenset al., 2005). FMD refers to endothelium-dependent vasodi-lation following a short period of increased shear stressgenerated by reactive hyperaemia (Corretti et al., 2002). Inendothelial dysfunction, the endothelium responds to reactivehyperaemia with decreased FMD, mainly suggesting dimin-ished availability of endothelium-derived nitric oxide(Celermajer et al., 1992; Corretti et al., 2002). FMD ispredictive of adverse cardiovascular outcomes and is relatedinversely to cardiovascular risk (Yeboah et al., 2007).Studies suggest that certain populations known to have
disrupted sleep, such as patients with diagnosed OSA andworkers with night shift jobs, not only have higher risk forCVD (Wang et al., 2011; Wolk et al., 2005), but have alsoreduced endothelial function (Amir et al., 2004; Patt et al.,2010). However, little is known about how endothelialfunction, as measured by FMD, relates to sleep qualityamong the general population of adults. Self-reported poorsleep quality and polysomnographic-assessed sleep distur-bances (e.g. OSA) have been linked with cardiovascularoutcomes (Chien et al., 2010; Hoevenaar-Blom et al., 2011;Wolk et al., 2005; Young et al., 2008), but it is unclearwhether such subjective and objective measures of sleepquality also exhibit links to endothelial function in adultssampled from the general population.The aim of this study was to assess how subjective and
objective indices of sleep quality relate to endothelial function(as measured by FMD) among relatively healthy, employed(non-shift work) adults. We hypothesized that lower FMD (i.e.poorer endothelial function) would be associated with lowerself-reported sleep quality and greater objectively assessedsleep disturbance as measured by polysomnography.
METHODS
Participants
The sample included 100 employed (30+ h week; non-shiftwork) adults of upper, middle and lower socioeconomicstatus, who were recruited via community advertisements orreferrals between 2005 and 2010 to participate in a largercardiovascular investigation. Excluded were participants withsecondary hypertension, diabetes (or a fasting glucose>120 mg/dL), known sleep disorders, current drug or alcoholabuse, ongoing psychiatric treatment, creatinine levels>1.4 mg/dL, proteinuria or haematuria by dipstick analysis,or renal bruit upon examination. For women, additionalexclusions were current pregnancy, postmenopausal status,oral contraceptive use and premenopausal syndrome. Vol-
unteers were eligible if the assessment (i.e. physical exam-ination and medical history) by the study’s physicianindicated that they were ostensibly healthy with no prescrip-tion medication use and no major medical/conditions. Thesample included 12 non-medicated individuals with hyper-tension, who had either not been taking antihypertensivemedications (n = 10) or had undergone a 3-week closelymonitored drug-tapering programme during which their non-medicated blood pressure had remained <180/110 mmHg toqualify for participation in the study (n = 2). In addition, thesample included eight light smokers (smoked less than onepack per day). Written informed consent was obtained fromall participants in accordance with the Institutional ReviewBoard of the University of California San Diego.
Procedures
The study procedures for the larger study have beenreported previously (von K€anel et al., 2007). To summarizeaspects of the protocol relevant to the current analyses,demographic and psychosocial data were collected, alongwith measures of resting blood pressure (BP) and bodymass index (BMI), during the initial visit. Later, participantsunderwent a 17:00 hours admission to the University ofCalifornia San Diego’s General Clinical Research Center fora 2-night stay at the Gillin Laboratory of Sleep andChronobiology. Set-up for sleep monitoring with standardpolysomnography (von K€anel et al., 2007) took placebetween 20:00 and 21:00 hours, then lights out at22:00 hours for an adaptation sleep study during the firstnight that ended with awakening at 06:00 hours andcompletion of psychosocial questionnaires. Upon the par-ticipants’ return to the unit that evening at 17:00 hours,overnight sleep monitoring with polysomnography wasrepeated from 22:00 to 06:00 hours for data collection.After a light (low fat, no caffeine) standard breakfast, thesubjects underwent FMD testing at 09:00 hours. Prior to theFMD testing session, participants had been on the unit formore than 12 hours and had refrained from smoking,exercise and consumption of caffeine, alcohol and foodscontaining high fat or nitrates.
Measures
Endothelial function
Flow-mediated dilation. A single examiner blinded to thehypotheses conducted non-invasive assessments of endo-thelial functioning using the guidelines for FMD testing, asdescribed by Celermajer and colleagues (Celermajer et al.,1992). The study’s examiner (co-author MSM) has exten-sive experience in brachial artery imaging and providingreliable measurements (e.g. intra-observer reliability basedon two blinded evaluations of 20 randomly selected record-ings: intraclass correlation 0.96; 95% confidence interval:0.89–0.98; coefficient of baseline values was 16%). Prior to
ª 2013 European Sleep Research Society
2 D. C. Cooper et al.

testing, participants relaxed quietly in the supine position for30 min in a dimmed, temperature-controlled room (22–25 °C) to limit the potential influence of mental or environ-mental stress on vasodilator responses. The right brachialartery was visualized in longitudinal section 2–8 cm prox-imal to the antecubital fossa with a high-resolution 5–12-MHz broadband linear array transducer (ATL HDI5000SonoCT System; Philips, Andover, MA, USA). Arterialdiameter was measured from the anterior to the posteriorintima line at end diastole, synchronous with electrocardio-graph (ECG) R wave. Baseline diameter was determined byaveraging three measurements taken immediately beforeinflation of the cuff on the upper arm. Then, the cuff wasinflated to 50 mmHg pressure above the systolic BP. After5 min, the cuff was deflated and ultrasound scans wereacquired for post-occlusion diameter measurements at 15-sintervals for 1 min and then at 30-s intervals for anadditional 9 min. FMD was calculated using followingformula: FMD =[(D(max)∕D(baseline)–1) 9 100], where FMD ismaximum percentage change in diameter, D(max) is maxi-mum post-occlusion diameter in centimeters and D(baseline)
is average pre-occlusion diameter in centimeters.
Sleep quality: subjective measure
Pittsburgh Sleep Quality Index (PSQI). Subjective sleepquality was measured with the PSQI (Buysse et al., 1989).The PSQI includes 19 items (e.g. ‘wake up in the middle ofthe night or early morning’) that assess perceived sleepdisturbance over the preceding 4 weeks. Seven componentscores (i.e. sleep quality, sleep latency, sleep duration,habitual sleep efficiency, sleep disturbances, use of sleepmedication, daytime dysfunction) are summed to derive aPSQI global score of subjective sleep quality (range 0–21points). Higher scores on the PSQI indicate poorer sleepquality.
Sleep quality: objective measures
Polysomnography. Sleep was recorded using the GrassHeritage (model PSG36-2; Astro-Med Inc., West Warwick,RI, USA) sleep recording system, which recorded central andoccipital electroencephalogram, bilateral electro-oculogram,submental and tibialis anterior electromyogram, ECG, nasalairflow (nasal cannula and pressure transducer), oral airflow(thermistor), respiratory effort (chest and abdominal piezo-electric belts) and oxyhaemoglobin saturation. Sleep stagingwas scored according to the criteria of Rechtshaffen andKales (1968) by technicians with inter-rater reliabilities above90%. Apneas were defined as decrements in airflow ≥90%from baseline for a period ≥10 s. Hypopneas were definedas decrements in airflow ≥50% but <90% from baseline for aperiod ≥10 s. Airflow was measured using a pressuretransducer and thermistor simultaneously. The pressuretransducer was used as the primary channel to score apneasand hypopneas. The thermistor was used primarily to detect
oral breathing, and served as a confirmatory adjunct to thepressure transducer measurement.Based on previous studies (von K€anel et al., 2007, 2010;
Mills et al., 2007), we selected a panel of eight sleepparameters that reflect the different domains of sleep thatmight reasonably be expected to show associations withendothelial function. They were slow wave sleep (SWS) (i.e.Stage 3 plus Stage 4 sleep), percentage rapid eye movement(%REM) sleep, REM sleep latency, total arousal index (TAI),total sleep time (TST), wake after sleep onset (WASO), sleepefficiency (TST/time in bed 9 100) and apnea–hypopneaindex (AHI). (Given the potential confounding of undiagnosedsleep apnea, AHI also was included as a covariate in theanalyses of FMD and other sleep quality measures.)
Covariate measures
The relationship of endothelial function to subjective andobjective sleep quality has a variety of potential confounders,including socioeconomic status (Mezick et al., 2008).Accordingly, in addition to adjusting the analyses for age,sex, race, BMI, hypertension status, AHI and smoking (self-reported current smoker: yes/no), we also accounted forsocioeconomic status (i.e. self-reported annual income).Exploratory analyses will additionally consider perceivedstress as a potential confounder.
Hypertension status. Hypertensive participants (systolic BP>140 mmHg and/or a diastolic BP >90 mmHg) were identi-fied based on the average of three BP measures [Dinamap1846x monitor (Critikon, Tampa, FL, USA)] obtained after5 min of seated rest.
Income. Participants answered the following question inreference to their employment: ‘What is your total annualwage or salary from this job?’.
Stress (exploratory analyses). Analyses explored theimpact of adjusting for perceived stress, because of theliterature suggesting that stress may influence both sleep andendothelial function (�Akerstedt, 2006; Toda and Nakanishi-Toda, 2011). Self-reported stress levels in the past 30 dayswere measured with the Perceived Stress Scale (PSS)(Cohen et al., 1983). The PSS asks respondents to indicateon a five-point Likert scale [0 (never) to 4 (very often)] howoften they have experienced each of the 10 items (e.g. ‘Howoften have you felt difficulties were piling up so high that youcould not overcome them?’) during the past month. Totalscores may range from 0 to 40, with higher scores indicatinghigher levels of perceived stress.
Data analysis
The relationships of FMD to subjective sleep quality (PSQI–global) and to objective sleep measures (i.e. SWS,%REMsleep, REM sleep latency, TAI, TST, WASO, sleep efficiency,
ª 2013 European Sleep Research Society
Endothelial function and sleep 3

AHI) were analysed with correlational and multiple regressionanalyses using PASW/SPSS version 18.0 software (IBM,Armonk, NY, USA). After examining FMD for bivariatecorrelations (P ≤ 0.05) with subjective and objective sleepmeasures, these noted correlations were examined furtherwith separate multiple regressions that tested the signifi-cance of the respective association after adjustment for astandard set of covariates: sex, age, race, BMI, hypertension,AHI, smoking and income. Covariates were selected basedon prior literature (Mezick et al., 2008; Moens et al., 2005)and/or simple correlations with the variables of interest.In the adjusted regression models, covariates were
entered on the first step, followed by the sleep measure ofinterest entered on the last step. Exploratory regressionanalyses were conducted to assess whether the previouslydescribed adjusted regression models remained significantafter further adjusting for the potential psychosocial con-founder of perceived stress, as measured by the PSS.The scores for PSQI–global, REM latency, FMD and
income were log10-transformed to reduce skew. Continuousscores were used to represent all variables, with theexception of categorical variables for sex, race, smokingand hypertension. One extreme outlier (standardized residual>�4.5; Cook’s distance more than eight times the 4/nthreshold) was excluded from the analyses, resulting in asample size of 100. However, three missing PSQI–globalscores reduced the sample size to 97 for analyses ofsubjective sleep quality and FMD.
RESULTS
Sample characteristics
As shown in Table 1, the sample included more men thanwomen (57 versus 43%) and a greater proportion ofCaucasians than African Americans (63 versus 37%).Participants were predominantly normotensive and non-smoking. On average, the sample exhibited a 14% changein brachial artery diameter. The mean PSQI score was 4.9,falling slightly below the cutoff of 5, which is used toscreen for sleep disturbance (approximately 36% of partic-ipants had PSQI scores of ≥6). Even though this was anostensibly healthy sample from the general population, wefound the mean AHI was somewhat high (meanAHI = 8.1).
Bivariate correlations
As indicated by the simple correlations provided in Table 2,decreasing FMD was associated with decreasing %REMsleep (P < 0.01) and with increasing REM latency(P < 0.05). FMD did not show bivariate associations withany other objective sleep measure derived from polysom-nography. However, decreasing endothelial function alsoshowed a correlation with poorer subjective sleep quality,such that FMD was associated inversely with PSQI–global
scores (P = 0.05). Higher PSQI–global scores (indicatingpoorer sleep quality) were correlated with lower SWS(P = 0.05), higher perceived stress (P < 0.01), hypertension(P < 0.01) and African American race (P < 0.05). LowerSWS and lower sleep efficiency were both correlated withAfrican American race (Ps < 0.01). Other simple correlationsrevealed that increased %REM sleep was associated withincreasing income and age (Ps < 0.05) in this young tomiddle-aged sample.
Table 1 Sample characteristics (n = 100)
VariableMean (SD)or% Range
Flow-mediated dilation% 13.50% (5.89%) 2.70–28.6Sex (% male:% female) 57%: 43%Age (years) 35.66 (9.54) 19–53Race (% Caucasian:African American) %
63%: 37%
BMI (kg/m2) 26.24 (4.11) 18.92–42.44Obesity: BMI ≥30kg/m2
19%
Hypertension(% normotensive:% hypertensive)
88%: 12%
Systolic bloodpressure (mmHg)
120.75 (14.09) (91.33–153.67)
Diastolic bloodpressure (mmHg)
71.70 (9.94) (53.67–102.67)
Smoking (% non-smokers:% smokers)
92%: 8%
Annual income (dollars) $31 519 (19 067) $300–100 000Perceived stress scale 13.42 (6.11) 0–28Pittsburgh Sleep QualityInventory global score
4.88 (2.89) 0–16
Total sleep time (min) 395.77 (49.46) 241.3–557.4Wake after sleeponset (min)
23.31 (20.87) 2.5–117.0
REM sleep% 22.73 (5.79) 8.58–39.19REM sleep latency fromsleep onset (min)
87.50 (48.50) 3.5–271.0
Slow wave sleep (min) 80.27 (39.91) 0–182.0Sleep efficiency% 91.89 (6.20) 70.04–99.12Total arousal index(events h)
8.09 (5.43) 0–33.70
Apnea–hypopneaindex(AHI) (events h)
8.09 (8.35) 0.17–38.64
No OSA: AHI 0–4.9) (48%)Undiagnosedmild OSA:AHI 5.0–14.9
(36%)
Undiagnosedmoderate OSA:AHI 15.0–29.9
(12%)
Undiagnosedmoderate OSA:AHI 15.0–29.9
(4%)
BMI, body mass index; REM, rapid eye movement; OSA,obstructive sleep apnea; SD, standard deviation.
ª 2013 European Sleep Research Society
4 D. C. Cooper et al.

Table2
Sim
pleco
rrelations
(r)am
ongva
riables
Variable
12
34
56
78
910
1112
1314
1516
1718
1.FMD
–0.36
**0.20
*�0
.17
0.04
0.09
0.02
0.04
�0.09
�0.20†
0.03
0.02
0.27
**�0
.21*
�0.18
�0.05
�0.02
�0.01
2.Sex
–�0
.04
0.04
0.03
0.05
�0.11
�0.07
�0.06
�0.08
0.03
�0.15
0.06
0.05
0.21
*0.13
�0.14
�0.08
3.Age
–�0
.28**
0.40
**0.24
*0.09
0.16
0.02
0.16
�0.15
0.34
**0.43
**�0
.10
0.52
**�0
.36**
0.32
**0.24
*4.
Rac
e–
�0.38**
�0.23*
�0.16
�0.03
�0.14
�0.21*
0.09
�0.14
�0.14
�0.05
0.42
**0.28
**�0
.02
�0.13
5.BMI
–0.49
**�0
.10
0.17
0.14
0.13
0.01
0.25
*0.18
�0.05
�0.30**
�0.19†
0.10
0.21
*6.
Hyp
ertens
ion
–0.01
0.01
0.02
0.29
**�0
.04
0.11
�0.04
0.08
0.24
*�0
.18
0.03
0.15
7.Smok
ing
–�0
.03
0.17
0.13
�0.17
0.12
0.13
0.02
�0.26**
�0.12
0.14
�0.03
8.Inco
me
–�0
.02
0.02
0.12
�0.06
0.22
*�0
.18
�0.10
0.07
0.10
0.22
*9.
Perce
ived
stress
–0.40
**�0
.07
0.11
0.03
0.08
�0.17
�0.15
�0.01
�0.08
10.PSQI–glob
al–
�0.12
0.17
�0.10
�0.02
�0.20†
�0.13
0.07
0.11
11.TST
–�0
.35**
0.08
�0.08
0.17
0.55
**�0
.15
0.18
12.WASO
–0.09
�0.02
�0.27**
�0.83**
0.26
*0.08
13.%
REM
slee
p–
�0.39**
�0.45**
�0.15
0.28
**0.38
**
14.REM
latenc
y–
0.14
�0.11
�0.26**
�0.16
15.SWS
–0.34
**�0
.28**
�0.16
16.Sleep
efficien
cy–
�0.12
�0.07
17.TAI
–0.33
**18
.AHI
–
FMD,flow
-med
iateddilatio
n;BMI,bo
dymas
sinde
x;PSQI–glob
al,Pittsb
urgh
Sleep
Qua
lityInve
ntoryglob
alsc
ore;
TST,totals
leep
time;
WASO,wak
eafterslee
pon
set;REM,rapidey
emov
emen
t;SWS,slow
wav
eslee
p;TAI,totala
rous
alinde
x;AHI,ap
nea–
hypo
pnea
inde
x.**P
<0.01
.*P
<0.05
.†P
=0.05
(two-tailed).
ª 2013 European Sleep Research Society
Endothelial function and sleep 5

Regression analyses: subjective sleep quality and FMD
The simple correlation found between poorer subjectivesleep quality (i.e. increasing PSQI–global scores) andpoorer endothelial function (i.e. decreasing FMD) wasexamined further with a regression of PSQI–global onFMD (see Table 3). After adjustment for sex, age, race,BMI, hypertension, AHI, smoking and income, the inverseassociation between PSQI–global scores and FMDremained significant (P < 0.05). PSQI–global scoresaccounted for 4% of the variance in FMD explained bythe final adjusted model (F(9,87) = 4.05; P < 0.001,R2 = 0.30).To understand these findings more clearly, the association
between PSQI–global and FMD was deconstructed byassessing the bivariate correlations of FMD with the PSQI’sseven components/subscales (data not shown). Only thePSQI’s daytime dysfunction component/subscale (e.g. ‘Dur-ing the past month, how often have you had trouble stayingawake while driving, eating meals, or engaging in socialactivity?’) was correlated with FMD (r = �0.26, P < 0.05),which suggests that subjective daytime dysfunction was
driving the relationship found between PSQI–global andFMD.
Regression analyses: objective sleep quality and FMD
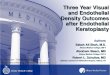
Regression analyses were conducted to examine further theobserved simple correlations of FMD with the objective sleepmeasures of %REM sleep and REM latency. In a multipleregression adjusted for sex, age, race, BMI, hypertension,AHI, smoking and income (Table 4), a significant associationwas observed between decreased FMD and decreased%REM sleep (P < 0.05). Approximately 4% of the variance inFMD was explained by %REM sleep in the final adjustedmodel (F(9,90) = 4.22; P < 0.001, R2 = 0.30). The relation-ship between FMD and %REM sleep is illustrated in Fig. 1.The results of multiple regression analyses indicated that
decreases in FMD were accompanied by significantincreases in REM latency (P < 0.05), after adjustment forsex, age, race, BMI, hypertension, AHI, smoking and income(Table 5). REM latency explained 4% of the variance in FMDaccounted for by the full model (F(9,90) = 4.09; P < 0.001,R2 = 0.29).
Table 4 Regression (final step) of REM Sleep% on FMD (n = 100): lower % REM correlated with lower endothelial funtion
Predictors MR2 MFMFP-value B (SE)
StandardBeta
BetaP-value
Step 1: Covariates 0.25 30.88 0.001(a) Sex 0.153 (0.04) 00.37 0.000(b) Age 0.002 (0.00) 00.10 0.368(c) Race �0.051 (0.02) �00.24 0.016(d) Hypertension 0.100 (0.07) 00.16 0.132(e) Body mass index �0.010 (0.01) �00.21 0.078(f) Apnea–hypopnea index �0.004 (0.00) �00.15 0.143(g) Income 0.031 (0.05) 00.06 0.541(h) Current smoker 0.053 (0.07) �00.07 0.454
Step 2:%REM sleep 0.04 50.42 0.022 0.009 (0.00) 00.25 0.022
REM, rapid eye movement; FMD, flow-mediated dilation; SE, standard error.
Table 3 Regression (final step) of the Pittsburgh Sleep Quality Index–global on flow-mediated dilation (n = 97): poorer subjective sleepquality correlated with poorer vasodilation
Predictors MR2 MFMFP-value B (SE)
StandardBeta
BetaP-value
Step 1: Covariates 0.25 3.72 0.001(a) Sex 0.160 (0.04) 0.39 0.000(b) Age 0.004 (0.00) 0.21 0.047(c) Race �0.056 (0.02) �0.26 0.012(d) Hypertension 0.107 (0.07) 0.17 0.115(e) Body mass index �0.010 (0.01) �0.20 0.096(f) Apnea–hypopnea index �0.002 (0.00) �0.06 0.507(g) Income 0.043 (0.05) 0.08 0.405(h) Current smoker �0.010 (0.07) �0.01 0.883
Step 2: Pittsburgh Sleep Quality Index–global 0.04 5.26 0.024 �0.164 (0.07) �0.22 0.024
ª 2013 European Sleep Research Society
6 D. C. Cooper et al.

Exploratory regression analyses
A series of exploratory regressions were conducted to testwhether adjustments for PSS scores, obesity (i.e. BMI<30 kg/m2 versus ≥30 kg/m2), levels of undiagnosedOSA severity or oxygen saturation measures would attenu-ate the observed associations of FMD with PSQI–globalscores, %REM sleep and REM sleep latency. Levels ofundiagnosed OSA severity were assessed by an AHIvariable categorizing OSA as: none (0–4.9); mild (5.0–14.9); moderate (15.0–29.9); and severe (≥30.0). Measuresof oxygen saturation included mean, lowest and percentageof time in bed with oxyhaemoglobin saturation (Spo2) <90%.None of these exploratory covariates were significant in themodels and none of them altered the significant associationsfound for FMD with PSQI, %REM sleep or REM sleeplatency.
DISCUSSION
Data showed that as FMD decreased, self-reported sleepquality (PSQI–global) worsened, %REM sleep decreased
and REM latency increased, after adjusting for sex, age,race, BMI, hypertension, AHI, smoking and income. Thus,diminished endothelial function was associated with bothsubjective and objective indicators of poor sleep quality afteradjustment for confounders.No other studies were found in the literature that investi-
gated how FMD relates to either subjective sleep quality or tothe objective sleep measures examined in the current study.Thus, it is challenging to integrate our findings with theexisting literature. Several studies suggest that FMD may bereduced among groups with disrupted sleep, such as adultsworking night shifts and patients with confirmed OSA (Amiret al., 2004; Patt et al., 2010) and with other work reportingthat patients with OSA who were treated with continuouspositive airway pressure (CPAP) showed increased FMD(Panoutsopoulos et al., 2012). The current study extendsthose findings by finding associations between sleep qualityand FMD among non-shift-working adults sampled from thegeneral population, who did not have a previously diagnosedsleep disorder. To our knowledge, this is the first study thathas linked reduced FMD to poorer subjective sleep qualityand to objective indicators of poorer REM sleep quality.Diminished endothelial function could be a mechanismunderlying the observed associations between poor sleepquality and adverse cardiovascular health (Chien et al.,2010; Wolk et al., 2005; Young et al., 2008).While the literature has no comparable studies of
subjective sleep quality and endothelial function, asmeasured by FMD, a previous study by our group (vonK€anel et al., 2010) found that poorer subjective sleep qualitywas associated with endothelial dysfunction, as measured byvon Willebrand factor, in a sample of chronically stressedolder adults and controls. The earlier study (von K€anel et al.,2010) noted that poor subjective sleep quality could be asurrogate marker for stress, but similar to the current study, itfound that adjustment for psychosocial stress did not atten-uate the relationship observed between poorer perceivedsleep quality and poorer endothelial function. Althoughmental stress is related to both perceived sleep quality and
Table 5 Regression (final step) of REM latency on FMD (n = 100): greater REM latency correlated with lower endothelial function
Predictors MR2 MFMFP-value B (SE)
StandardBeta
BetaP-value
Step 1: Covariates 0.25 30.88 0.001(a) Sex 0.168 (0.04) 0.41 0.000(b) Age 0.004 (0.00) 0.17 0.095(c) Race �0.055 (0.02) �0.26 0.010(d) Hypertension 0.084 (0.07) 0.13 0.202(e) Body mass index �0.010 (0.01) �0.20 0.084(f) Apnea–hypopnea index �0.002 (0.00) �0.10 0.312(g) Income 0.031 (0.05) 0.06 0.553(h) Current smoker �0.029 (0.07) �0.39 0.674
Step 2: REM sleep latency 0.04 40.53 0.036 �0.115 (0.05) �0.20 0.036
REM, rapid eye movement; FMD, flow-mediated dilation; SE, standard error.
Figure 1. Flow-mediated dilation and rapid eye movement (REM)sleep percentage: as endothelial functioning increased, percentagesof REM sleep increased.
ª 2013 European Sleep Research Society
Endothelial function and sleep 7

endothelial function (Toda and Nakanishi-Toda, 2011), theseresults suggest that perceived sleep quality is associatedwith endothelial function independent of psychosocial stress.This association also seems to be independent of AHI, whichshowed no bivariate correlation with PSQI and did notattenuate the relationship between PSQI–global scores onFMD in the regression analyses in the present study. Poorersubjective sleep quality showed a significant bivariate corre-lation with higher diastolic BP in the current sample (data notshown). Autonomic dysfunction may be a mechanism linkingsubjective sleep disturbances to poor cardiovascular health(von K€anel et al., 2010; Wolk et al., 2005). Given thatautonomic changes also are associated with REM sleep(Dang-Vu et al., 2010; Wolk et al., 2005), further research isneeded to understand more clearly how autonomic function-ing may relate to subjective sleep quality, particularly daytimedysfunction, as well as REM sleep.It is intriguing that not only was decreased FMD associated
with poorer subjective sleep quality, particularly subjectivedaytime dysfunction, but that it also was associated withdecreased %REM sleep and with increased latency of REMsleep. Although no direct investigations of its potential associ-ations with cardiovascular risk have been reported, REM sleephas been shown to be important in optimal learning andmemory, as well as daytime functioning (Dang-Vu et al.,2010). While nitric oxide in the brain facilitates REM sleep(Cespuglio et al., 2012), FMD is a functional measure of nitricoxide-mediated vasodilation (Corretti et al., 2002). In ourprevious study (Mills et al., 2007), increased REM latencyamong healthy adults was associated with increased endo-thelin-1,which is anothermarker of endothelial dysfunctionandnitricoxidedysregulation.ResearchhasfoundthatpatientswithOSA exhibit diminished nitric oxide and FMD (Wolk et al.,2005). However, given that the current analyseswere adjustedfor AHI, the findings for endothelial function and REM sleepmeasures are probably independent of undiagnosedOSA. It isunclearwhyFMDshowedassociationswith theREMindicatorsbut not with any of the other objective sleep measures in thecurrent study. However, FMD had a marginal bivariate associ-ation with SWS, which may have become significant if morestatistical power was available. Interestingly, SWS and REMare both partially facilitated by nitric oxide (Cespuglio et al.,2012). Additional research is needed to elucidate the linksbetween endothelial function, REM sleep, SWS and nitricoxide-mediated pathways.Systemic low-grade inflammation that is predictive of CVD
might be another important mechanism linking REM sleep toendothelial dysfunction. Inflammatory processes contributeto and are also affected by endothelial dysfunction (Trepelset al., 2006). Greater REM latency has been associated withelevated plasma levels of the proinflammatory cytokineinterleukin (IL)-6 (Mills et al., 2007). Subcutaneous admin-istration of low-dose recombinant IL-6 was found todecrease REM sleep (Spath-Schwalbe et al., 1998). FMDand IL-6 have shown an inverse correlation (Esteve et al.,2007). IL-6 might induce endothelial dysfunction through
impairment of the vasodilating effects of insulin mediated bythe endothelial nitric oxide synthase (eNOS) pathway andby directly inhibiting eNOS expression (Andersen andPedersen, 2008).One of the strengths of this study is that it assessed both
subjective and objective measures of sleep to provide abroader picture of relations between FMD and sleep quality.Moreover, it appears that this is the first investigation of theserelations in a relatively healthy sample from the generalpopulation. Another strength is the study’s limiting of thepotential effect of confounders on the results throughrelatively strict exclusion criteria, physician confirmation ofhealth status and testing in a controlled inpatient setting.Other strengths include adjustments for varying levels ofseveral traditional and psychosocial risk factors for CVD.Nevertheless, our results should be interpreted within the
limitations of the study design and sample. Our findingsshould be replicated with larger samples. The current studyexamined a sample from the general population that wasostensibly healthy. However, the findings may be limited bythe sample’s relatively high mean level of AHI. Althoughroughly 4% of this sample had an AHI ≥30 (suggestingsevere sleep-disordered breathing), this prevalence is similarto samples of other population-based studies (Young et al.,2008). We did not exclude participants with high AHI levelsdue to sample size considerations. The significant findingsreported were based on primary analyses adjusted for AHI(continuous scores) and exploratory analyses adjusted forAHI categorized according to AHI levels of OSA severity.Further, AHI did not reach significance as a covariate in anyof the regression models for PSQI, %REM sleep or REMlatency on FMD. However, it is possible that undiagnosedOSA is influencing our findings and that the high levels of AHIin the current sample will limit the generalizability of ourfindings to non-OSA samples.Similarly, we did not exclude hypertensive participants,
but they all were unmedicated and we adjusted forhypertension status in the regression analysis. The samplealso included several smokers, but this was addressed withan adjustment in the analyses and participant restrictionfrom smoking in the hours before FMD testing. Approxi-mately 19% of the sample had BMI ≥30 kg/m2. However,our analyses were adjusted for BMI and exploratoryanalyses that included obesity as a alterative covariatedid not alter the results. Like other samples (Moens et al.,2005; Yeboah et al., 2007), FMD in the current samplewas greater among women than men. Although theanalyses included an adjustment for sex, the findingscould be limited by our inability to account for possiblevariations in endothelial function or sleep that might havebeen related to hormonal changes (e.g. oestradiol) asso-ciated with the menstrual cycle in premenopausal women.While the inclusion/exclusion criteria probably reducedvariance in this otherwise healthy, unmedicated, young tomiddle-aged sample, these findings might have limitedgeneralizability to other age groups and to populations in
ª 2013 European Sleep Research Society
8 D. C. Cooper et al.

which comorbidity/medication use is prevalent. Ourpolysomnography data were obtained during a single night(after an adaptation night), as is common in the literature,but an assessment involving several nights of recordingsmight have produced different results. In addition, asindicated in Fig. 1, participants’ %REM sleep values variednotably, ranging from relatively low values (8–11%) to arelatively high value (39%). Given that none of thesevalues were statistical outliers and that their omission fromthe sample in exploratory regressions (data not shown) didnot change the results substantially, we retained theseparticipants in the sample to maintain statistical power.Finally, no causal or temporal determinations can be madefrom this cross-sectional, correlational study.In summary, reduced endothelial function was related to
poor subjective sleep quality and to potentially adversedecreases in %REM sleep and increases in REM latency.These findings suggest that endothelial dysfunction could bea pathway linking subjective and objective measures of poorsleep quality to CVD.
ACKNOWLEDGEMENTS
This study was supported by National Institutes of HealthGrants HL36005, RR00827, AG08415 and P60 MD00220.
DISCLAIMER
The views expressed in this paper are solely those of theauthors and do not necessarily reflect the position or policy ofthe Department of Veterans Affairs, the University of Califor-nia San Diego or the University of Bern.
CONFLICT OF INTEREST
No conflicts of interest declared.
REFERENCES
�Akerstedt, T. Psychosocial stress and impaired sleep. Scand.J. Work Environ. Health, 2006, 32: 493–501.
Amir, O., Alroy, S., Schliamser, J. E. et al. Brachial artery endothelialfunction in residents and fellows working night shifts. Am.J. Cardiol., 2004, 93: 947–949.
Andersen, K. and Pedersen, B. K. The role of inflammation invascular insulin resistance with focus on IL-6. Horm. Metab. Res.,2008, 40: 635–639.
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R. andKupfer, D. J. Pittsburgh Sleep Quality Index: a new instrument forpsychiatric practice and research. Psychiatry Res., 1989, 28: 193–213.
Celermajer, D. S., Sorensen, K. E. and Gooch, V. M. Non-invasivedetection of endothelial dysfunction in children and adults at risk ofatherosclerosis. Lancet, 1992, 340: 1111–1115.
Cespuglio, R., Amrouni, D., Meiller, A., Buguet, A. and Gautier-Sauvign�e, S. Nitric oxide in the regulation of the sleep–wakestates. Sleep Med. Rev., 2012, 16: 265–279.
Chien, K. L., Chen, P. C., Hsu, H. C. et al. Habitual sleep durationand insomnia and the risk of cardiovascular events and all-cause
death: report from a community-based cohort. Sleep, 2010, 33:177–184.
Cohen, S., Kamarck, T. and Mermelstein, R. A global measure ofperceived stress. J. Health Soc. Behav., 1983, 24: 385–396.
Corretti, M. C., Anderson, T. J., Benjamin, E. J. et al. InternationalBrachial Artery Reactivity Task Force. Guidelines for the ultra-sound assessment of endothelial-dependent flow-mediated vaso-dilation of the brachial artery: a report of the International BrachialArtery Reactivity Task Force. J. Am. Coll. Cardiol., 2002, 39:257–265.
Dang-Vu, T. T., Schabus, M. and Desseilles, M. Functional neuroi-maging insights into the physiology of human sleep. Sleep, 2010,33: 1589–1603.
El Solh, A. A., Akinnusi, M. E., Berim, I. G., Peter, A. M., Paasch, L. L.and Szarpa, K. R. Hemostatic implications of endothelial cellapoptosis in obstructive sleep apnea. Sleep Breath., 2008, 12:331–337.
Esteve, E., Castro, A., Lopez-Bermejo, A., Vendrell, J., Ricart, W.and Fernandez-Real, J. M. Serum interleukin-6 correlates withendothelial dysfunction in healthy men independently of insulinsensitivity. Diabetes Care, 2007, 30: 939–945.
Hoevenaar-Blom, M. P., Spijkerman, A. M., Kromhout, D., van denBerg, J. F. and Verschuren, W. M. Sleep duration and sleep qualityin relation to 12-year cardiovascular disease incidence: theMORGEN study. Sleep, 2011, 34: 1487–1492.
von K€anel, R., Loredo, J. S., Ancoli-Israel, S., Mills, P. J., Natarajan,L. and Dimsdale, J. E. Association between polysomnographicmeasures of disrupted sleep and prothrombotic factors. Chest,2007, 131: 733–739.
von K€anel, R., Ancoli-Israel, S., Dimsdale, J. E. et al. Sleep andbiomarkers of atherosclerosis in elderly Alzheimer caregivers andcontrols. Gerontology, 2010, 56: 41–50.
Mezick, E. J., Matthews, K. A., Hall, M. et al. Influence of race andsocioeconomic status on sleep: Pittsburgh Sleep SCORE project.Psychosom. Med., 2008, 70: 410–416.
Mills, P. J., von K€anel, R., Norman, D., Natarajan, L., Ziegler, M. G.and Dimsdale, J. E. Inflammation and sleep in healthy individuals.Sleep, 2007, 30: 729–735.
Moens, A. L., Goovaerts, I., Claeys, M. J. and Vrints, C. J. Flow-mediated vasodilation: a diagnostic instrument, or an experimentaltool? Chest, 2005, 127: 2254–2263.
Panoutsopoulos,A.,Kallianos,A.,Kostopoulos,K.et al.EffectofCPAPtreatment on endothelial function and plasmaCRP levels in patientswith sleep apnea.Med. Sci. Monit., 2012, 18: CR747–CR751.
Patt, B. T., Jarjoura, D., Haddad, D. N. et al. Endothelial dysfunctionin the microcirculation of patients with obstructive sleep apnea.Am. J. Respir. Crit. Care Med., 2010, 182: 1540–1545.
Phillips, B. G., Narkiewicz, K., Pesek, C. A., Haynes, W. G.,Dyken, M. E. and Somers, V. K. Effects of obstructive sleepapnea on endothelin-1 and blood pressure. J. Hypertens., 1999,17: 61–66.
Rechtshaffen, A. and Kales, A. A Manual of Standardized Terminol-ogy, Techniques, and Scoring System for Sleep Stages of HumanSubjects. National Institutes of Health, Publication no. 204. USGovernment Printing Office, Washington DC, 1968.
Spath-Schwalbe, E., Hansen, K., Schmidt, F. et al. Acute effects ofrecombinant human interleukin-6 on endocrine and central ner-vous sleep functions in healthy men. J. Clin. Endocrinol. Metab.,1998, 83: 1573–1579.
Toda, N. and Nakanishi-Toda, M. How mental stress affectsendothelial function. Pflugers Arch., 2011, 462: 779–794.
Trepels, T., Zeiher, A. M. and Fichtlscherer, S. The endothelium andinflammation. Endothelium, 2006, 13: 423–429.
Wang, X. S., Armstrong, M. E., Cairns, B. J., Key, T. J. and Travis, R.C. Shift work and chronic disease: the epidemiological evidence.Occup. Med. (Lond.), 2011, 61: 78–89.
ª 2013 European Sleep Research Society
Endothelial function and sleep 9

Wolk, R., Gami, A. S., Garcia-Touchard, A. and Somers, V. K. Sleepand cardiovascular disease. Curr. Prob. Cardiol., 2005, 30: 625–662.
Yeboah, J., Crouse, J. R., Hsu, F. C., Burke, G. L. and Herrington, D.M. Brachial flow-mediated dilation predicts incident cardiovascularevents in older adults: the Cardiovascular Health Study. Circula-tion, 2007, 115: 2390–2397.
Young, T., Finn, L., Peppard, P. E. et al. Sleep disordered breathingand mortality: eighteen-year follow-up of the Wisconsin sleepcohort. Sleep, 2008, 31: 1071–1078.
Zamarr�on-Sanz, C., Ricoy-Galbaldon, J., Gude-Sampedro, F. andRiveiro-Riveiro, A. Plasma levels of vascular endothelial markers inobstructive sleep apnea. Arch. Med. Res., 2006, 37: 552–555.
ª 2013 European Sleep Research Society
10 D. C. Cooper et al.