Embed Size (px)
Citation preview

Eur J Vasc Endovasc Surg 16, 164-168 (1998)
ENDOVASCULAR AND SURGICAL TECHNIQUES
Obturator Bypass to the Distal Profunda Femoris Artery Using a Medial Approach - Long-term Results
G, Plate ~1, P, Qvarfordt 1, S. Oredsson 1 and L. Stigsson z
Departments of 1Surgery and 2Radiology, Central Hospital, S-251 87 Helsingborg, Sweden
Key Words: Obturator foramen; Bypass; Deep femoral artery.
Introduction Patients
Bypass via the obturator foramen was first described by Shaw and Baue in 19631 and has since been used for iliofemoral arterial reconstruction in the presence of a hostile groin or graft infection. The long-term outcome has been compromised by a high failure rate especially in patients who require graft extension to the popliteal or tibial vessels. 2-5 There are also a few case reports of thigh ischaemia despite adequate lower leg perfusion provided by an obturator bypass ex- tended to below the knee level, s'6 These problems emphasise the importance of perfusing the profunda fernoris artery, which may be excluded with con- ventional obturator bypass. The proximity to an in- fected groin increases the risk of secondary graft infection if the bypass is anastomosed to the profunda femoris artery exposed in a conventional manner.
Influenced by a communication by Nunez et al. 7 describing exposure of the third portion of the pro- funda femoris artery using a posteromedial approach between the adductor muscles, we have performed obturator bypass using this exposure in six patients. The plane between the adductor longus and adductor magnus muscles leads directly to the obturator chan- nel, which simplifies the tunnelling procedure. Only two single case reports using this technique have been found in the literature, s'9 both only providing short- term follow-up. Others have used the profunda femoris artery as an outflow vessel for obturator by- pass,10 12 but technical details were not described.
* Please address all correspondence to: G. Plate, Department of Surgery, Central Hospital, S-251 87 Helsingborg, Sweden.
Six non-diabetic male smokers with a median age of 66 (50-79) had previously undergone aortobifemoral bypass and several other vascular procedures (Table 1). Four of the patients had culture-proven or sus- pected graft infection, whereas the indication for ob- turator bypass was a hostile groin following repeated vascular procedures in two patients with severe limb ischaemia. All had occlusive lesions of the femo- ropopliteal arteries precluding conventional obturator bypass to the superficial femoris artery. Two had severe ischaemia and three had claudication. The ankle-bra- chial index was 0.0-0.7 (median 0.5).
Operative Technique
The patients were draped with adhesive plastic on the abdomen and the affected thigh proximally and medially. The hip was flexed and rotated outwards. Using a longitudinal incision at least 10 cm from the groin, the plane between the adductor longus and adductor magnus muscles was explored without dis- section of the superficial femoris artery. The third portion of the profunda femoris artery was exposed between the deep fascial insertions of these muscles. Using the same plane, the outside of the obturator fascia was palpated. In cases of distal graft limb in- fection (four patients), the obturator foramen and the proximal ipsilateral graft limb was exposed trans- peritoneally using a low mid-line abdominal incision. The graft limb was divided and the distal portion was
1078-5884/98/080164+05 $12.00/0 © 1998 W.B. Saunders Company Ltd.

Obturator Bypass 165
Table 1. Previous vascular procedures, present problem, and bacterial cultures in six patients operated with obturator bypass.
Pat no. Previous vascular procedures Present problem Culture involving the same groin
1 Aortobifemoral bypass Draining groin sinus Graft limb infected
2 Groin infection Recent thrombectomy
Aortobifemoral bypass Femoropopliteal bypass Thrombectomy x 3
3 Thromboendar terectomy Aortobifemoral bypass Thrombectomy ÷ patch
4 Aortobifemoral bypass Femorofemoral bypass Thrombectomy Thromboendarterectomy
5 Femorofemoral bypass Thrombectomy Aortobifemoral bypass
6 Aortobifemoral bypass
Occluded graft limb Repeated procedures
fJ-streptococcus (type G) Staphylococcus epidermidis (multiresistant) Not done
Occluded graft limb Not done
Pseudoaneurysm
Pseudoaneurysm Fever
Staphylococcus epidermidis (multiresistant) Negative
c o v e r e d b y s u r r o u n d i n g t issue in the r e t r o p e r i t o n e u m . A n ex te rna l ly r e in fo rced p o l y t e t r a f l u o r o e t h y l e n e graf t (Gore- tex ®) w a s a n a s t o m o s e d e n d - t o - e n d to the p rox- ima l graf t l imb a n d tunne l l ed t h r o u g h the o b t u r a t o r f o r a m e n , w h i c h w a s p e n e t r a t e d u n d e r d i rec t vision.
In the two cases w i t h graf t l imb occlus ion and a host i le groin , the p ros thes i s w a s a n a s t o m o s e d end- to - s ide to the cont ra la te ra l graf t l imb (Fig. 1). All dis ta l ana- s t omoses w e r e p e r f o r m e d end- to - s ide to the p r o f u n d a f emor i s a r t e ry u s ing a ve in cuff in th ree cases (Fig. 2).
"D.
Fig. 1. Artist's concept of obturator bypass to the profunda femoris artery. Left: crossover bypass from the contralateral aortofemoral graft limb in case of graft limb occlusion and a hostile groin. Right: proximal anastomosis to divided ipsilateral aortofemoral graft limb in case of groin infection.
Eur J Vasc Endovasc Surg Vol 16, August 1998

166 G. Plate et aL
k, -{ " -
J
!1,
t
\
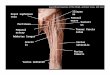
Fig. 2. Artist's concept of obturator bypass (arrow) to the profunda femoris artery (arrow-head), and it's relationship to the surrounding tissues.
In t w o p a t i e n t s w h o h a d s eve re i s c h a e m i a a n d in one p a t i e n t w h o h a d a p r e v i o u s f e m o r o p o p l i t e a l b y p a s s tha t h a d to be d i s c o n n e c t e d f r o m its inf low, an ex- t en s iona l b y p a s s to the p o p l i t e a l a r t e r y w a s p e r f o r m e d u s i n g in - s i tu v e i n graf t s in t w o cases a n d a p o l y - t e t r a f l u o r o e t h y l e n e (Gore-Tex ®) graf t in one case. The inc is ions w e r e c losed in l aye r s a n d cove red , w h e r e - u p o n the p r o b l e m in the g r o i n w a s d e a l t w i t h as r equ i r ed .
Fig. 3. Intravenous digital subtraction angiography performed 3 years after obturator bypass. The initial operation was performed with an end-to-side anastomosis to the contralateral aortofemoral graft limb and an end-to-side anastomosis to the profunda femoris artery. The infected graft limb was excised to the groin where the femoral arteries were divided. Following graft occlusion after 3 months, which was treated with thrombectomy, anticoagulation, and jump-graft extension to the popliteal artery, the reconstruction has remained patent for 5 years (patient 3).
Eur J Vasc Endovasc Surg Vol 16, August 1998

Obturator Bypass 167
Results
There was no operative mortality, no injury to the obturator nerve or vein, and no serious early morbidity related to the obturator bypass. The peripheral per- fusion was sufficient in all patients (ankle-brachial index=0.6-0.9), despite immediate occlusion of the graft extension to the popliteal artery in two patients. No prosthesis has become infected during a median follow-up of 5 (range 3-7) years. Two early obturator graft occlusions occurred after 2 and 3 months, re- spectively. These were treated with thrombectomy, graft extension to the popliteal artery, and oral anti- coagulation, but only one of these two grafts remained patent (Fig. 3). The other early graft occlusion resulted in below-knee amputation. Three patients have died from unrelated causes after 10, 20 and 82 months, respectively. The primary patency was 67% (four of six grafts), 60% (three of five grafts), and 25% (one of four grafts) after 1, 3, and 5 years respectively, and the secondary patency was 83% (five of six grafts), 80% (four of five grafts), and 75% (three of four grafts) at the same time intervals.
occlusion, a crossover bypass is readily accomplished. This has been described previously 13'~4 but only Atnip s used the present technique with anastomosis to the profunda femoris artery.
The primary patency may improve if postoperative anticoagulation is routinely employed. We used ex- ternally reinforced vascular prostheses as vascular conduits due to the risk of graft kinking or compression with passage of the narrow obturator channel. 4'5'11 However, others have used autogenous vein grafts with good results. 1°'15 Addition of a jump-graft ex- tension to the popliteal artery was not successful in this small series. Only two out of five (three initial and two post-thrombectomy) extensions have remained patent. Although these occlusions may be due to tech- nical problems, their failure did not seem to com- promise peripheral perfusion or decrease patency of the obturator bypass graft per se. When compared to other series of conventional obturator bypass, 3'4'16 we have demonstrated an equally good or superior early and late graft patency. Since the operative morbidity has been minimal by using this technique of obturator bypass, it is recommended especially in patients with obstructive lesions of the superficial femoris and pop- liteal arteries.
Discussion
The advantage with this procedure is the preservation of thigh perfusion without risking infection of the new graft. In this series, no secondary graft infection occurred and perfusion of the thigh and lower leg was sufficient as long as the obturator bypass stayed patent. Bypass to the superficial femoral artery or the above- knee popliteal artery probably have the same chance of success as with this technique, provided arterial perfusion of the thigh is maintained. This is not always possible if the femoral arteries have to be ligated in the groin to control infection and if obstructive lesions in the femoropopliteal arteries prohibit sufficient ret- rograde flow up the superficial femoris artery. 5 In addition, the chance of long-term patency is reduced if the obturator bypass is carried down to the below- knee vessels. 3'4
With the described technique, the long-term results seem acceptable, and peripheral perfusion was ad- equate except in one patient where the graft per- manently occluded. This provided a secondary graft patency rate of around 75% after 3 years. A short graft length and a high blood flow are crucial for maintained patency of prosthetic vascular grafts. Our technique provides the shortest possible distance to bypass and a good outflow via the profunda femoris artery which is usually less diseased. In case of ipsilateral graft limb
References
1 SHAW RS, BAUE AE. Management of sepsis complicating arterial reconstructive procedures. Surgery 1963; 53: 75-86.
2 KRETSCItMER G, NIEDERLE B, HUK I, KARNER J, PIzA-KATZER H, POLTERAUER PI WALZER LR. Groin infections following vascular surgery: obturator bypass (BYP) versus "biologic coverage" (TRP) - a comparative analysis. Eur ] Vasc Surg 1989; 3: 25-29.
3 NEVELSTEEN A1 MEES U, DELEERSNIJDER J, SUY R. Obturator bypass: a 16 year experience with 55 cases. Ann Vasc Surg 1987; 1: 558-563.
4 PEARCE WH, RICCO J-B, YAO JST, FLINN WR, BERGAN JJ. Modified technique of obturator bypass in failed or infected grafts. Ann Surg 1983; 197: 344-347.
5 SAUTNER T I NIEDERLE B, HERBST F~ KRETSCHMER G, POLTERAUER Pr RENDL KH, PRENNER K. The value of obturator canal bypass. A review. Arch Surg 1994; 129: 718-722.
6 RUDICH M, GUTIERREZ IZ, GAGE AA. Obturator foramen bypass in the management of infected vascular prostheses. Am J Surg 1979; 137: 657-660.
7 NUNEZ AA, VEITH FJ, COLLIER Pt ASCER E, WHITE FLORES S, GUPTA SK. Direct approaches to the distal portions of the deep femoral artery for limb salvage bypasses. J Vasc Surg 1988; 8: 576-581.
8 ATNIP RG. Crossover ilioprofunda reconstruction: an expanded role for obturator foramen bypass. Surgery 1991; 110: 106-108.
9 MILLIS J~V[, AHN SS. Transobturator aorto-profunda femoral artery bypass using the direct medial thigh approach. Ann Vasc Surg 1993; 7: 384-390.
10 ERATH HG, GALE SS, SMITH BM, DEAN RH. Obturator foramen grafts: the preferable alternate route? Am Surg 1982; 48: 65-69.
11 GEROULAKOS G, PARVIN SD, BELL PRE Obturator foramen bypass - the alternative route for sepsis in the femoral triangle. Acta Chir Scand 1988; 154: 111-112.
Eur J Vasc Eudovasc Surg Vol 16, August 1998

168 G. Plate et aL
12 ROYSTER TS, LYNN Ry MULCARE RJ, STELZER PE. Dacron grafting from the aorta to the distal profunda femoris arteries via the obturator foramina. Arch Surg 1977; 112: 316-317.
13 JOFFE B, LANKOVSKY Z, MORDECHAY I. Cross over iliopopliteal bypass through the obturator foramen: an additional route for extra-anatomic limb blood supply. Int Surg 1985; 70: 345-347.
14 KIEFFER E. Pontage iliofemoral crois6 par le trou obturator. La NouveIle Presse mfdicale 1975; 4: 1487-1488.
15 TILSON MD, SWE~NEY T, GUSBERG RJ, STANSEL HC. Obturator canal bypass grafts for septic lesions of the femoral artery. Arch Surg 1979; 114: 1031-1033.
16 VAN DET RJ, BRANDS LC. The obturator foramen bypass: an alternative procedure in iliofemoral artery revascularization. Surgery 1981; 89: 543-547.
Accepted 24 March 1998
Eur J Vasc Endovasc Surg Vol 16, August 1998