Embed Size (px)
Citation preview

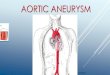
Endovascular Management
of Cerebral Aneurysms
Shao-Pow Lin, MD, PhD
Neurointerventional Radiology
Lambert Radiology Medical Group

Cerebral Aneurysms
Weak point in vessel wall that “balloons out” over time
Propensity for hemorrhage
Adapted from Chalouhi et al, Stroke. 2013;44:3613-3622

Risk Factors
For aneurysms:
• Smoking, HTN,
Hyperlipidemia
• Age > 40, Female
• Family history,
congenital disorders
• CNS infection,
Trauma, AVM
For rupture:
• Prior rupture
• Smoking, HTN,
cocaine, meth
• African Americans &
Hispanics > White

Statistics
Statistics
~1 in 50 people have an aneurysm, ~1 in 20 over 50
• Common disease
Ruptures ~30k/yr in US (less than 5% of all stroke)
• Low risk of rupture (1%/yr – most never rupture)
~50% of ruptures are fatal (15% never reach hospital)
~50% of non-fatal ruptures result in permanent
neurological deficit
• High risk of bad outcome

Intracranial Hemorrhage
Epidural
• Trauma, usually fracture
Subdural
• Trauma, spontaneous
(elderly/blood thinners)
Intraparenchymal
(intracerebral)
• HTN, AVM, tumor, trauma
Subarachnoid
• Aneurysm, trauma

SAH Evaluation
SAH = ruptured aneurysm
until proven otherwise
Imaging
• CTA or MRA at minimum
• If negative, catheter
angiography still
recommended
• Up to 20% can be
negative on catheter
angiogram
• Depending on clinical
suspicion, repeat CTA or
angiogram after 1-2 weeks

Aneurysm Work-up
MRA
Non-emergent
screening
CTA
Workhorse for
emergent work-up
Catheter angio
Work-up known
aneurysm/SAH

Ok I found an aneurysm,
now what?
Incidental aneurysm
• Non-emergent consult,
outpatient ok
Symptomatic aneurysm
• New, worsening,
persistent HA or cranial
nerve palsy
• ED, Urgent consult
Subarachnoid hemorrhage
• Emergent consult

Emergent Consult
Why isn’t time critical?
• Brain is not ischemic
• Usually no active
bleeding
• Aneurysm treatment
doesn’t improve status,
but hydrocephalus
treatment can
Why is time still important?
• Highest risk of re-bleed
in first 48 hrs
• Our goal is to treat
within 24 hrs, usually
within 12

Acute Management
Imaging: Non-con CT, CTA
Labs: Coags, BMP, CBC
Control BP
• Nicardipine drip
• SBP < 140
Manage ICP
• Mannitol, Hypertonic saline
• Ventriculostomy
Treat
• Clip (craniotomy)
• Coil (endovascular)

Treatment: Clip or Coil?
CLIP COIL
Approach Craniotomy Endovascular
Anesthesia General General
Goal Exclude aneurysm by
placing clip across neck
Exclude aneurysm by packing the
inside with coils
Preferred
Characteristics
MCA bifurcation,
Complex or wide neck
Basilar tip,
Narrow neck
Follow-up Usually 1 angiogram F/u angiography for several years

What is a “Coil”?
Platinum (mostly) wire:
0.002-0.003 in
Secondary shape “coil”:
0.010 to 0.015 in
Tertiary shape helix,
sphere, etc. 1 mm – 3 cm
Attach to pusher wire with
detachment mechanism
MR Conditional
• Field < 3T
• Gradient < 2500 G/cm
• SAR < 2W/kg in 15 min
Ok for immediate
scanning

41 M
In town for wedding
Acute onset severe HA
with R facial droop

Catheter Angio, LICA

Primary Coiling, ACOM
AP LAT

Subtracted Image
AP LAT

1 Lobe Left…
AP LAT

Complete Occlusion
AP LAT

Outcome
No new neurologic deficits
No vasospasm
D/c home

66 F
In town on vacation
Sudden onset:
• HA
• Neck pain
• LOC, likely seizure
while taking shower
Now awake, oriented

Catheter Angiogram, LICA
AP LAT

Wide Neck PCOM aneurysm

Balloon-Assisted Coiling

Outcome
No new neurologic deficits
No vasospasm
D/c home

39 F
Acute onset HA
SAH dx at OSH
No aneurysm found on
CTA, patient transferred
for higher level of care

CTA
Missed basilar
tip aneurysm
No neck
Wider at base
than dome

What Now?
Clip – not for basilar tip
Primary coiling
• Unlikely to work
Balloon assisted coiling
• Temporary scaffold
Stent assisted coiling
• Permanent scaffold
• Non-ideal because patient has
acute rupture
• Pre-medicated with
ASA/Plavix overnight and
treated first case in AM

Aneurysm Scaffold Devices
Laser cut stents
• Cut from Nitinol, with
tantalum or platinum
markers
• Neuroform, Enterprise
Braided stents
• Nitinol wires with tantalum
markers
• LVIS, Leo
Pulserider
• Nitinol with platinum/iridium
markers

Catheter Angio, Vertebral
AP LAT

“Y” Stent Assistance
Stent to L PCA Stent to R PCA Finish coiling

Outcome
No new neurological deficit
No vasospasm
D/c home
Small recurrence at 6 months,
added coils

51 F
HA
Hypertensive urgency
No hemorrhage
Incidental aneurysm (HA resolved with
lower BP)

Catheter Angio, LICA

Very Wide Neck Aneurysm
Primary coiling – unlikely to work
Balloon assisted coiling – might work
Stent assisted coiling – reasonable option
Flow diversion
• Latest and greatest treatment

What is a Flow Diverter?
Braided stent-like device
Typical (Neuroform/Enterprise) stent
provides approximately 6% coverage
Pipeline, Surpass, Silk and other flow
diverters provide 30+% coverage
Low porosity “diverts” blood away
from aneurysm without need for coils

Pipeline Flow Diverter
48-strand braided mesh
75% Co-Cr, 25% Pt-W
CT: easily visible
MRI safety:
• Conditional up to 3T,
720 G/cm, SAR 4
W/kg
• Ok for immediate
scanning

PED Placed Over Aneurysm
Immediate stasis 6 month f/u

58 F
Acute onset HA,
R sided weakness
SAH Dx at OSH,
transfer for higher
level of care
Awake, oriented

Catheter Angio, LICA
AP LAT

Fusiform MCA Aneurysm
Clip – generally best
option for complex
MCA aneurysm
Primary or balloon
assisted coil – no
Stent assisted coil or
Pipeline embolization
• Need ASA/Plavix
• Would consider if not
ruptured

Post Clipping
AP LAT

Outcome
No new neurological deficit
Full recovery
D/c home

8 Months Later…
Recurrent HA and R sided weakness

What Now?
Parent artery not normal
Re-clip not a good option
Need vessel
reconstruction
Patient pre-medicated
with ASA/Plavix a few
hours prior to Pipeline
assisted coiling

Pipeline and Coils

Outcome
No new neurological deficit
Full recovery
D/c home
3 Month f/u

Take Home Points
Aneurysms are common
Aneurysm rupture
• Low probability, high risk event
Aneurysm treatment depends on:
• Rupture status
• Complexity of aneurysm
• Neck size
• Branch vessels
• Location
GDC coil FDA approved in 1995.
Neurointervention is still a new field!

What’s Coming Soon…

Stay Connected with PIH Health
@PIHHealth
Facebook.com/PIHHealth
@PIHHealth
Sign up for our patient portal:
PIHHealth.org/MyPIHHEALTH
Free Health & Wellness Programs: Visit PIHHealth.org/Calendar
PIHHealth.org


















![Thrombosed Large Middle Cerebral Artery Aneurysm Mimicking … · 2015-05-05 · Intracranial aneurysms are common and affecting approxi-mately 5% of the population [4]. And MCA aneurysms](https://img.pdfslide.net/doc/110x75/5ed573adc0b3156ac4174ccc/thrombosed-large-middle-cerebral-artery-aneurysm-mimicking-2015-05-05-intracranial.jpg)