Embed Size (px)
Citation preview
CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 145
Endovascular Therapies for Hemodialysis Access: Case Presentations of Salvage, Surgical Maturation, and Maintenance
GUIDELINES FOR HEMODIALYSISAs life expectancy increases and the incidence of
diabetes and hypertension grows, a greater number of
patients are diagnosed with advanced chronic kidney
disease. Chronic kidney disease eventually evolves into
end-stage renal disease (ESRD) necessitating place-
ment of permanent hemodialysis access. Permanent
dialysis access of arteriovenous connection has been
introduced and implemented since the 1960s.1 Ac-
cording to the National Kidney Foundation-Kidney
Dialysis Outcomes Quality Initiative (NKF-KDOQI)
and Society of Vascular Surgery (SVS) guidelines, it is
recommended that patients be referred for permanent
vascular dialysis access when creatinine clearance is
less than 25 mL/min.2,3 Arteriovenous fistula (AVF)
access has been the dialysis modality of choice over
arteriovenous graft (AVG) placement when suitable
vascular anatomy permits.3
ACCESS FAILURE, MATURATION, MAINTENANCE, AND SALVAGE
The primary causes for dialysis access failure in-
clude poor inflow by arterial anastomotic failure, poor
outflow due to central venous stenosis, small artery
or vein preventing adequate volume of blood from
circulating through the fistula, and collateral veins
stealing blood from the primary vein. The minimal
diameter of arteries and veins for access creation is
2 mm and 2 mm to 3 mm, respectively.2 Historically,
many fistulas that have failed initial cannulation were
Yury Bak, DO; John H. Cooper, DO; Kane L. Chang, MD
From the Deborah Heart and Lung Center, Browns Mills, New Jersey.
ABSTRACT: Arteriovenous (AV) access is a field in vascular interventional surgery that has under-
gone much evolution. Today many AV access sites are carefully monitored and facilitated, main-
tained, and salvaged through endovascular techniques. This enables the physician and patient to get
significantly more use out of each access site created. This article presents the development of the
endovascular field of access surgery. We also present illustrative cases that demonstrate examples
of using such techniques in our practice.
VASCULAR DISEASE MANAGEMENT 2014;11(7):E145-E155
Key words: hemodialysis access intervention, hemodialysis, arteriovenous fistula
Copyri
ght H
MP Com
munica
tions

CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 146
either abandoned or surgically revised. This resulted
in numerous procedures throughout the lifetime of
the patient to maintain dialysis access.
As the field of access surgery has evolved to better
understand the causes for fistula and graft failures, the
methods of treating dialysis problems have become
less invasive, more aggressive, and increasingly so-
phisticated. Initiatives of access salvage, access main-
tenance, and fistula maturation have become more
common concepts in hemodialysis. Fistula salvage
refers to transforming nonmaturing or thrombosed
fistulae to functional fistulae. Surgical maturation re-
fers to decreasing the maturation time for fistulae to
become usable with endovascular therapies. Finally,
maintenance is described as prolonging patency rates
of dysfunctional but patent fistulae. Arteriovenous
fistula abandonment appears to be twice as costly as
salvage of thrombosis with potential expenses per
patient-month of $707 vs $375.4 One of the main
factors that contributes to late access failure is intimal
hyperplasia. This is caused by activation of macro-
phages and release of chemotactic agents, including
platelet-derived growth factor, transforming growth
factor beta, and angiotensin II, all of which promote
migration of smooth muscle cells.4
PERCUTANEOUS VASCULAR INTERVENTION OF FAILING ACCESS
The earliest attempts at vascular access site salvage
were described in 1984 study, where 8 of 10 balloon
angioplasties were described as outright failures and
the authors concluded that percutaneous transluminal
angioplasty had a very limited role as an access site
salvage procedure in AV grafts.5 Angioplasty was later
combined with thrombolytic infusion in completely
thrombosed AVFs and AVGs with 78% primary pa-
tency at 3 months and 36% primary patency at 9
months.6,7 In lesions that are stenosed, the median
recurrence rate is 11 months in fistulas and 5 months
in grafts, and they had a 72% patency at 6 months and
32% patency at 12 months.8 When no lesions within
the vein are visualized, then the cause of fistula failure
may be arterial stenosis. Angioplasty may be safely
performed on the brachial artery to a primary patency
rate of 83% at 1 year and 74% at 2 years. Forearm
arterial access angioplasty is to be avoided in lesions
in very distal extremities.9 Endovascular placement of
stents was implemented for lesions resistant to bal-
loon angioplasty with primary patency of 100% at
6.2 months as described by Hood et al.10 Patency of
failing AV grafts was followed for a longer timeframe
with the use of Viabahn stents by Davila Santini et
al, with 94.7% 6- and 12-month patency, and 82.1%
18-, 24- and 36-month patency.11 The combination
of performing AVF angioplasty with ligation of ac-
cessory venous side branches that can steal direct ve-
nous flow from arterialized veins can achieve access
salvage in 82.5% to 100% of fistulas that fail to develop
with 84% continued function at 3 months, 72% at 6
months, and 68% at 12 months.12,13 More recently,
salvage of cephalic vein outflow has been described,
including a totally percutaneous tunneled bypass us-
ing stent grafts in the basilic vein outflow with good
intermediate follow-up results.14
FISTULA SURVEILLANCE AND MATURATIONMonitoring the progress of fistula maturation was
traditionally clinically assessed with adequacy of thrill
Copyri
ght H
MP Com
munica
tions

CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 147
and bruit over an enlarged vein. The use of ultrasound
duplex measurement of blood flows >700-800 cc/min
may effectively predict successful AVF maturation.14,15
Another study found a significant reduction in place-
ment of central venous dialysis catheters with use of
a surveillance program based on clinical and duplex
ultrasound every 3 months, followed by fistulogram
for stenosis compared to clinical and hemodynamic
assessment in cases of dysfunction.16 Frequently access
must be serially maintained with follow-up fistulo-
grams and interventions in order to preserve patency.
Falk analyzed 154 fistulas and determined that 3.3
procedures per fistula and 1.75 procedures per year
must be performed in mature fistulas to maintain pa-
tency. These procedures included arterial and venous
angioplasty, ligation of venous side branches, throm-
bectomy, and/or banding. The primary patency rate
at 1 year was 64% while secondary patency was 68%.17
The concept of serial dilations, known as balloon
angioplasty maturation, may be used to increase the
size of AVFs. Miller et al performed thrombectomy
with angioplasty of 140 immature thrombosed fistulas.
Average maturation time, defined as from thrombec-
tomy to maturation for dialysis, was 46.4 days with an
average of 2.64 interventions per patient. Percutane-
ous salvage of fistulas costs $4,881 to $14,998 less than
the abandonment and new creation of AV access.18
De Marco Garcia et al also achieved excellent func-
tion of AVF <3 mm in ≤2 months’ duration in 96%
of patients.19 Some have advocated performing endo-
vascular interventional procedures in an office setting
under ultrasound guidance. Gorin et al describes a
93% 90-day patency rate in 55 interventions where a
fistula was failing or not maturing. The overall rate
of perifistular hematoma was 11%, with 3 cases of
thrombosis of AVF. No patient required hospitaliza-
tion or urgent surgical intervention.20
CASE PRESENTATIONSCase 1
A 62-year-old male with history of coronary artery
disease, diabetes mellitus, hypertension, peripheral ar-
tery disease, and chronic renal insufficiency predialysis
underwent left radiocephalic end-to-side arteriove-
nous fistula. Intraoperative ultrasound demonstrated
a radial artery with high take-off at the axilla. The
radial artery was densely calcified, measuring 3.5 mm
above the elbow, and was poorly visualized below the
elbow due to calcification. Exploration of the radial
artery at the wrist demonstrated a 2.0 mm calcified
artery that was deemed marginal but usable for ra-
diocephalic fistula creation. The cephalic vein, which
measured 3.0 mm on ultrasound, was dilated to 3.5
mm intraoperatively prior to AVF creation. Excellent
flow was established at the conclusion of the AVF
creation. Two months postoperatively, the proximal
fistula measured 4 mm to 5 mm by ultrasound. Good
bruit and thrill were present over proximal AVF, but
were weak in the distal AVF. A large 5 mm collateral
vein was noted at the posterior forearm that appeared
to be stealing flow from the true cephalic outflow,
which measured 3.5 mm.
Two months after initial AVF creation, surgical li-
gation of the large collateral branch was performed
to divert flow back to the primary cephalic vein. On
ultrasound, the distal cephalic vein measured 3.5 mm
to 4.0 mm. The patient was lost to follow-up thereafter
and presented 15 months later, having progressed to
Copyri
ght H
MP Com
munica
tions
CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 148
ESRD and receiving hemodialysis via a permcath. It
was determined that some form of endovascular AVF
intervention was performed at another institution.
On physical exam, AVF contained a weak bruit and
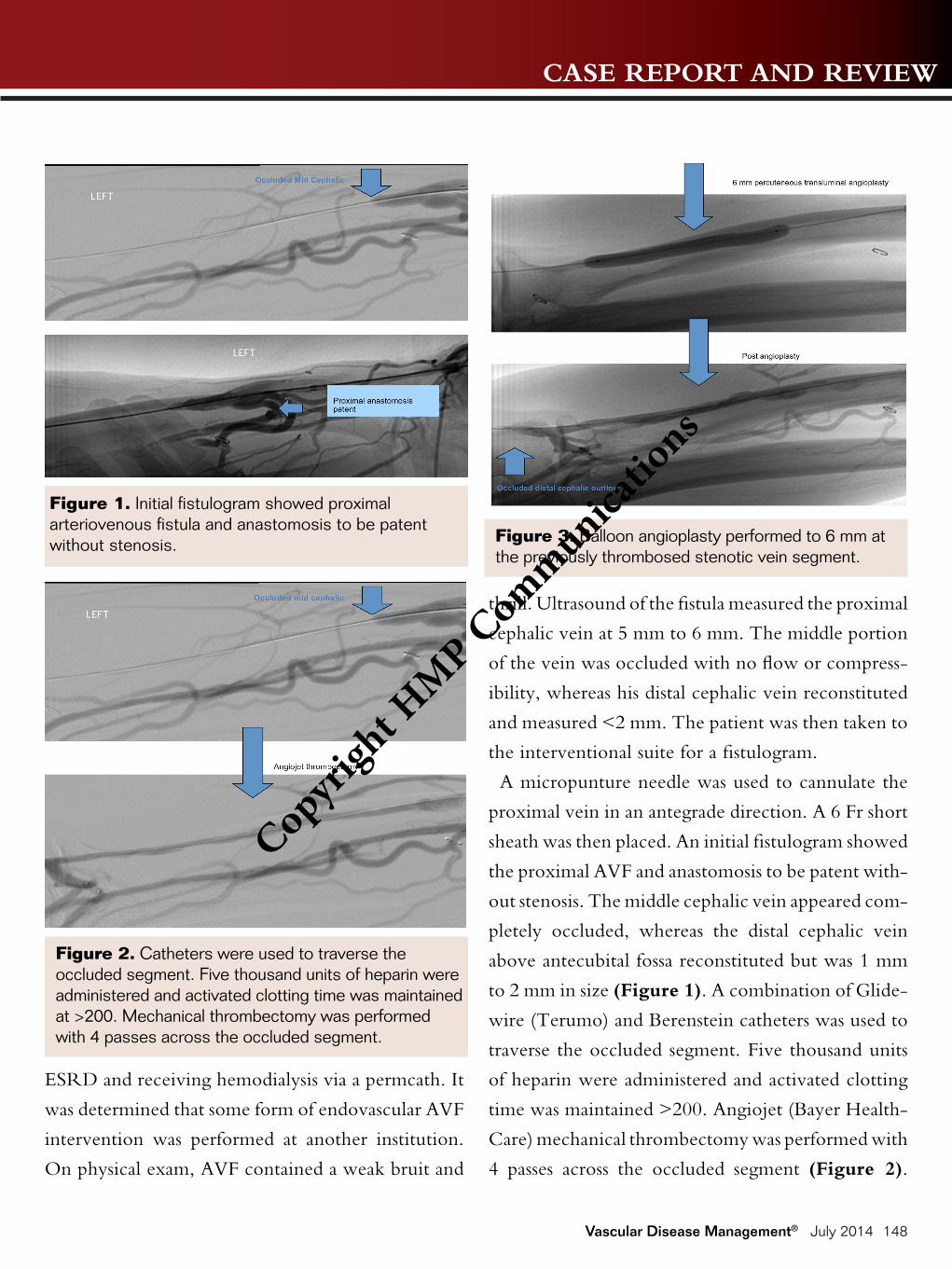
thrill. Ultrasound of the fistula measured the proximal
cephalic vein at 5 mm to 6 mm. The middle portion
of the vein was occluded with no flow or compress-
ibility, whereas his distal cephalic vein reconstituted
and measured <2 mm. The patient was then taken to
the interventional suite for a fistulogram.
A micropunture needle was used to cannulate the
proximal vein in an antegrade direction. A 6 Fr short
sheath was then placed. An initial fistulogram showed
the proximal AVF and anastomosis to be patent with-
out stenosis. The middle cephalic vein appeared com-
pletely occluded, whereas the distal cephalic vein
above antecubital fossa reconstituted but was 1 mm
to 2 mm in size (Figure 1). A combination of Glide-
wire (Terumo) and Berenstein catheters was used to
traverse the occluded segment. Five thousand units
of heparin were administered and activated clotting
time was maintained >200. Angiojet (Bayer Health-
Care) mechanical thrombectomy was performed with
4 passes across the occluded segment (Figure 2).
Figure 1. Initial fistulogram showed proximal arteriovenous fistula and anastomosis to be patent without stenosis.
Figure 2. Catheters were used to traverse the occluded segment. Five thousand units of heparin were administered and activated clotting time was maintained at >200. Mechanical thrombectomy was performed with 4 passes across the occluded segment.
Figure 3. Balloon angioplasty performed to 6 mm at the previously thrombosed stenotic vein segment.
Copyri
ght H
MP Com
munica
tions
CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 149
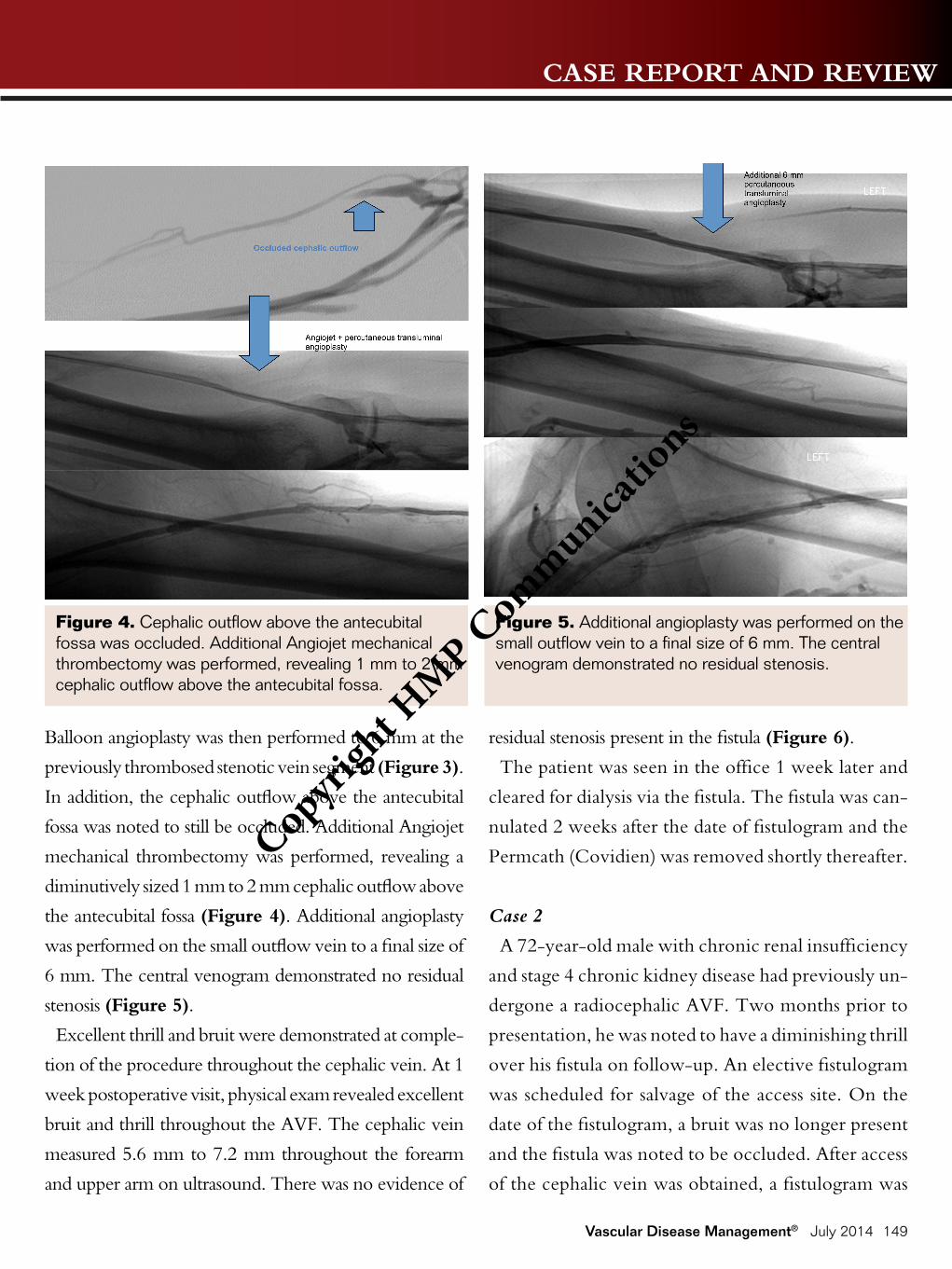
Balloon angioplasty was then performed to 6 mm at the
previously thrombosed stenotic vein segment (Figure 3).
In addition, the cephalic outflow above the antecubital
fossa was noted to still be occluded. Additional Angiojet
mechanical thrombectomy was performed, revealing a
diminutively sized 1 mm to 2 mm cephalic outflow above
the antecubital fossa (Figure 4). Additional angioplasty
was performed on the small outflow vein to a final size of
6 mm. The central venogram demonstrated no residual
stenosis (Figure 5).
Excellent thrill and bruit were demonstrated at comple-
tion of the procedure throughout the cephalic vein. At 1
week postoperative visit, physical exam revealed excellent
bruit and thrill throughout the AVF. The cephalic vein
measured 5.6 mm to 7.2 mm throughout the forearm
and upper arm on ultrasound. There was no evidence of
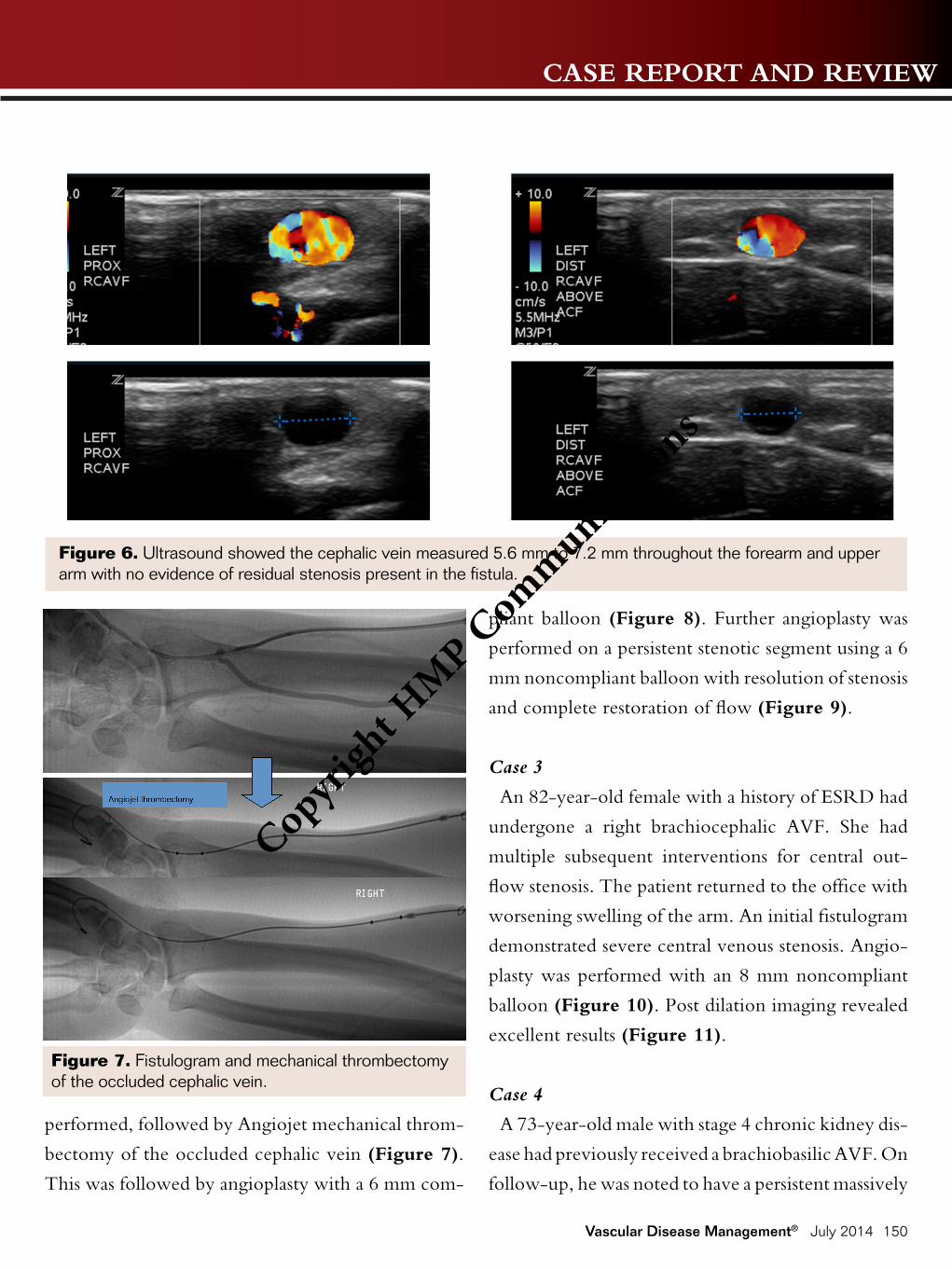
residual stenosis present in the fistula (Figure 6).
The patient was seen in the office 1 week later and
cleared for dialysis via the fistula. The fistula was can-
nulated 2 weeks after the date of fistulogram and the
Permcath (Covidien) was removed shortly thereafter.
Case 2
A 72-year-old male with chronic renal insufficiency
and stage 4 chronic kidney disease had previously un-
dergone a radiocephalic AVF. Two months prior to
presentation, he was noted to have a diminishing thrill
over his fistula on follow-up. An elective fistulogram
was scheduled for salvage of the access site. On the
date of the fistulogram, a bruit was no longer present
and the fistula was noted to be occluded. After access
of the cephalic vein was obtained, a fistulogram was
Figure 4. Cephalic outflow above the antecubital fossa was occluded. Additional Angiojet mechanical thrombectomy was performed, revealing 1 mm to 2 mm cephalic outflow above the antecubital fossa.
Figure 5. Additional angioplasty was performed on the small outflow vein to a final size of 6 mm. The central venogram demonstrated no residual stenosis.
Copyri
ght H
MP Com
munica
tions
CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 150
performed, followed by Angiojet mechanical throm-
bectomy of the occluded cephalic vein (Figure 7).
This was followed by angioplasty with a 6 mm com-
pliant balloon (Figure 8). Further angioplasty was
performed on a persistent stenotic segment using a 6
mm noncompliant balloon with resolution of stenosis
and complete restoration of flow (Figure 9).
Case 3
An 82-year-old female with a history of ESRD had
undergone a right brachiocephalic AVF. She had
multiple subsequent interventions for central out-
flow stenosis. The patient returned to the office with
worsening swelling of the arm. An initial fistulogram
demonstrated severe central venous stenosis. Angio-
plasty was performed with an 8 mm noncompliant
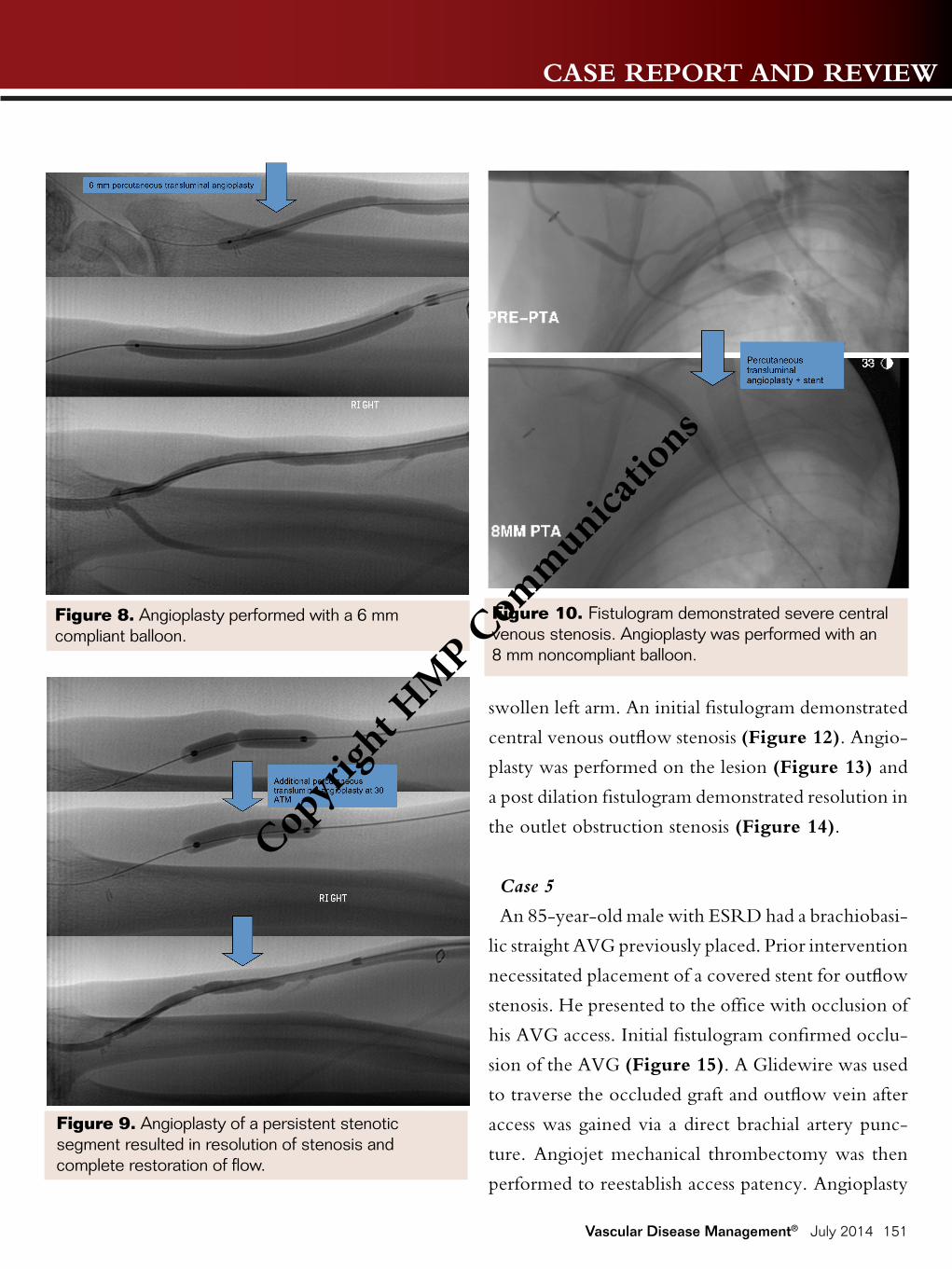
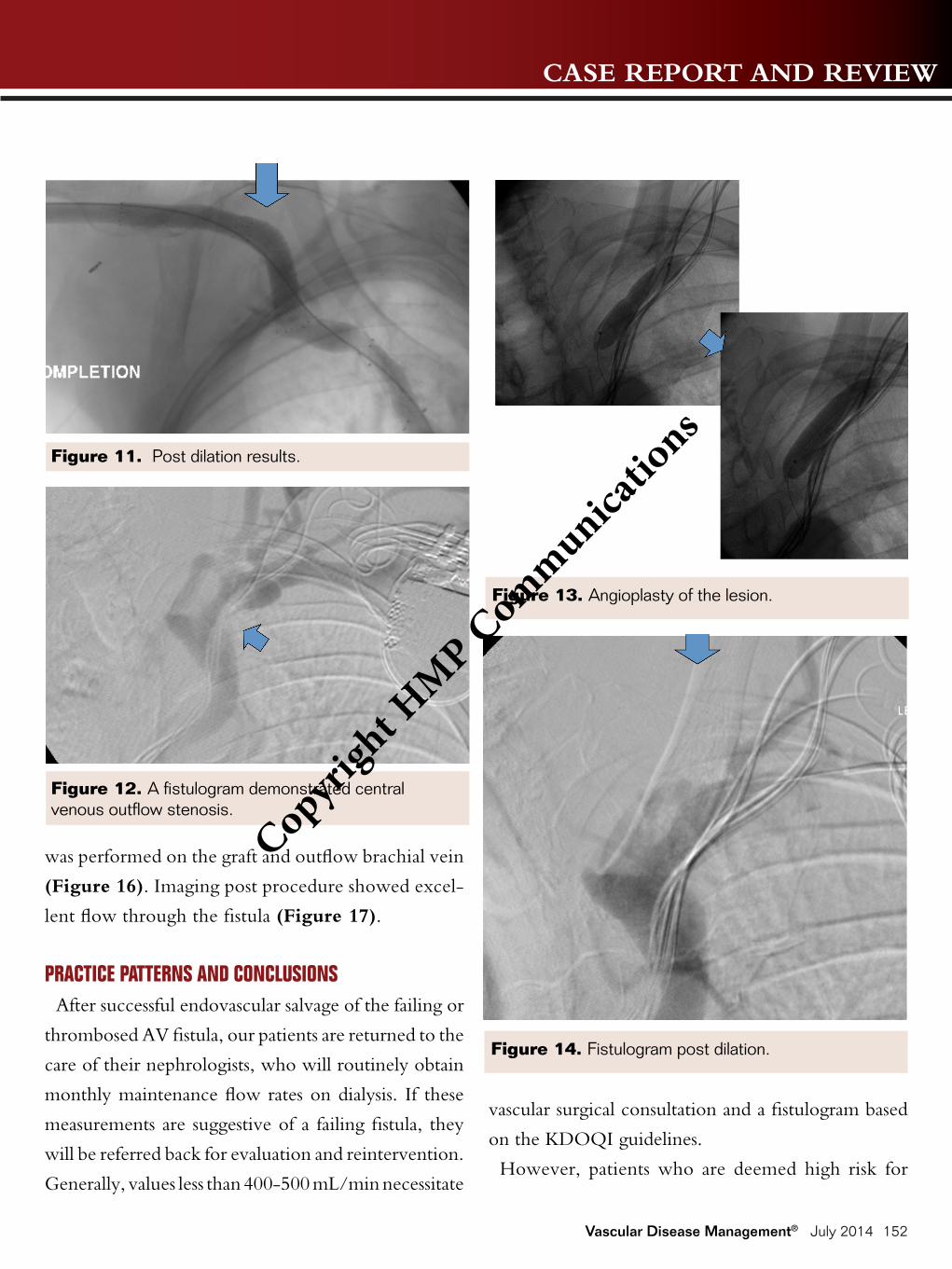
balloon (Figure 10). Post dilation imaging revealed
excellent results (Figure 11).
Case 4
A 73-year-old male with stage 4 chronic kidney dis-
ease had previously received a brachiobasilic AVF. On
follow-up, he was noted to have a persistent massively
Figure 6. Ultrasound showed the cephalic vein measured 5.6 mm to 7.2 mm throughout the forearm and upper arm with no evidence of residual stenosis present in the fistula.
Figure 7. Fistulogram and mechanical thrombectomy of the occluded cephalic vein.
Copyri
ght H
MP Com
munica
tions
CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 151
swollen left arm. An initial fistulogram demonstrated
central venous outflow stenosis (Figure 12). Angio-
plasty was performed on the lesion (Figure 13) and
a post dilation fistulogram demonstrated resolution in
the outlet obstruction stenosis (Figure 14).
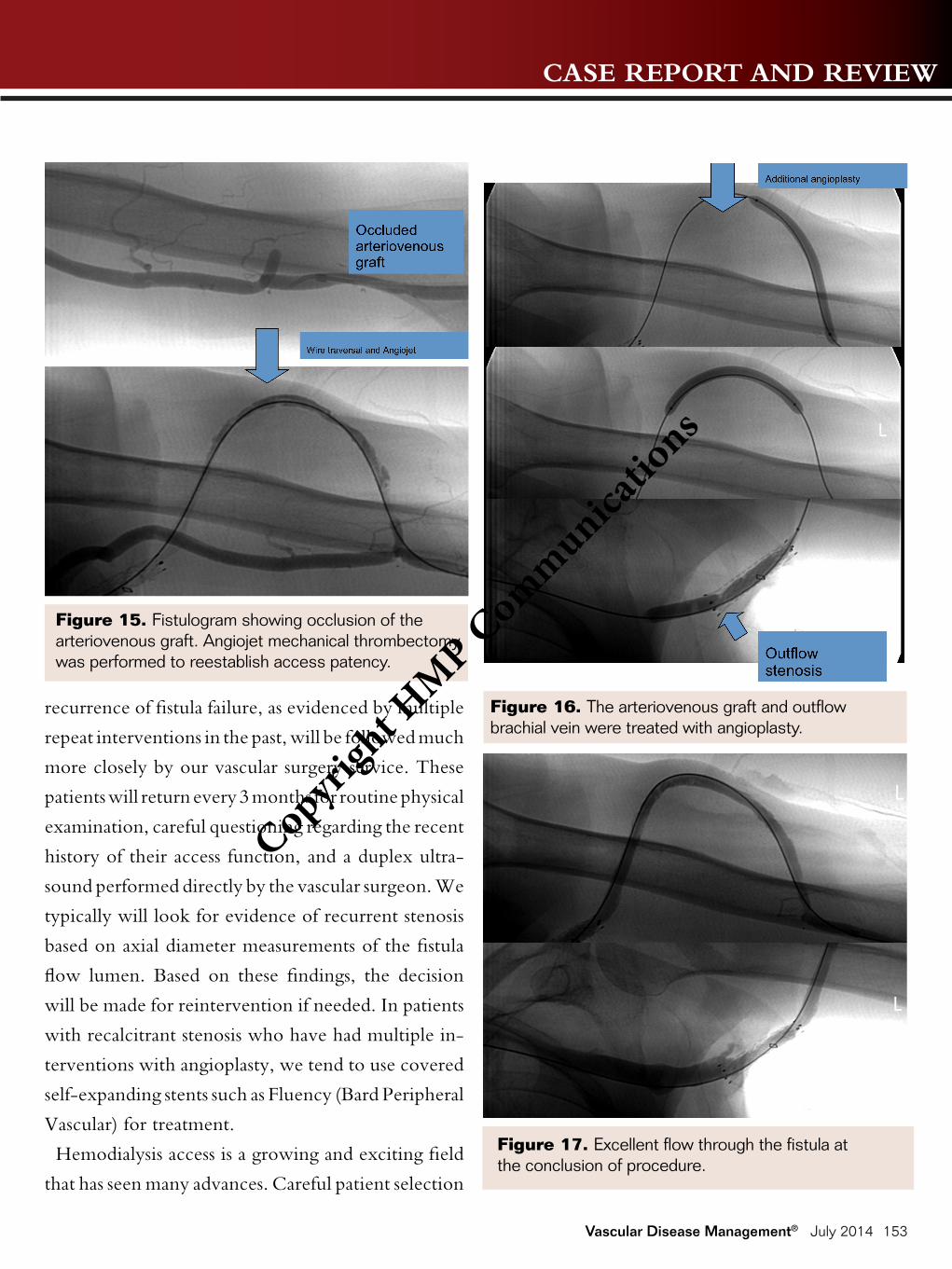
Case 5
An 85-year-old male with ESRD had a brachiobasi-
lic straight AVG previously placed. Prior intervention
necessitated placement of a covered stent for outflow
stenosis. He presented to the office with occlusion of
his AVG access. Initial fistulogram confirmed occlu-
sion of the AVG (Figure 15). A Glidewire was used
to traverse the occluded graft and outflow vein after
access was gained via a direct brachial artery punc-
ture. Angiojet mechanical thrombectomy was then
performed to reestablish access patency. Angioplasty
Figure 8. Angioplasty performed with a 6 mm compliant balloon.
Figure 9. Angioplasty of a persistent stenotic segment resulted in resolution of stenosis and complete restoration of flow.
Figure 10. Fistulogram demonstrated severe central venous stenosis. Angioplasty was performed with an 8 mm noncompliant balloon.
Copyri
ght H
MP Com
munica
tions
CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 152
was performed on the graft and outflow brachial vein
(Figure 16). Imaging post procedure showed excel-
lent flow through the fistula (Figure 17).
PRACTICE PATTERNS AND CONCLUSIONSAfter successful endovascular salvage of the failing or
thrombosed AV fistula, our patients are returned to the
care of their nephrologists, who will routinely obtain
monthly maintenance flow rates on dialysis. If these
measurements are suggestive of a failing fistula, they
will be referred back for evaluation and reintervention.
Generally, values less than 400-500 mL/min necessitate
vascular surgical consultation and a fistulogram based
on the KDOQI guidelines.
However, patients who are deemed high risk for
Figure 11. Post dilation results.
Figure 12. A fistulogram demonstrated central venous outflow stenosis.
Figure 13. Angioplasty of the lesion.
Figure 14. Fistulogram post dilation.
Copyri
ght H
MP Com
munica
tions
CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 153
recurrence of fistula failure, as evidenced by multiple
repeat interventions in the past, will be followed much
more closely by our vascular surgery service. These
patients will return every 3 months for routine physical
examination, careful questioning regarding the recent
history of their access function, and a duplex ultra-
sound performed directly by the vascular surgeon. We
typically will look for evidence of recurrent stenosis
based on axial diameter measurements of the fistula
flow lumen. Based on these findings, the decision
will be made for reintervention if needed. In patients
with recalcitrant stenosis who have had multiple in-
terventions with angioplasty, we tend to use covered
self-expanding stents such as Fluency (Bard Peripheral
Vascular) for treatment.
Hemodialysis access is a growing and exciting field
that has seen many advances. Careful patient selection
Figure 15. Fistulogram showing occlusion of the arteriovenous graft. Angiojet mechanical thrombectomy was performed to reestablish access patency.
Figure 16. The arteriovenous graft and outflow brachial vein were treated with angioplasty.
Figure 17. Excellent flow through the fistula at the conclusion of procedure.
Copyri
ght H
MP Com
munica
tions

CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 154
is necessary for placement of permanent dialysis access
with preference of fistula over graft. After completion
of the procedure, is it essential to continue to regularly
monitor the maturation of the access site. Multiple
techniques may be used to accelerate maturation of
an AVF. After successful cannulation of the fistula or
graft, it is essential to be aware of potential stenosis
from intimal hyperplasia over time that may cause
dysfunctional flow. Multiple endovascular meth-
ods, including thrombectomy, angioplasty, and stent
placement, may be used to salvage a failing access. n
Editor’s Note: Disclosure: The authors have completed
and returned the ICMJE Form for Disclosure of Potential
Conflicts of Interest. The authors report no conflicts of interest
regarding the content herein.
Manuscript received March 4, 2014; provisional acceptance
given April 2, 2014; final version accepted April 28, 2014.
Address for correspondence: Yury Bak, DO, Deborah Heart
and Lung Center, 200 Trenton Rd., Browns Mills, NJ
08015, United States. Email: [email protected]
REFERENCES 1. Brescia MJ, Cimino JE, Appel K, Hurwich BJ. Chron-
ic hemodialysis using veni-puncture and a surgi-cally created arteriovenous fistula. N Engl J Med. 1966;275(20):1089-1092.
2. Macsata RA, Sidawy AN. Hemodialysis access: general considerations. In: JL Cronenwett and KW Johnston, eds. Rutherford’s Vascular Surgery. 7th ed. Maryland Heights, Mo: Saunders Elsevier; 2010:1104-1113.
3. Vassalotti JA, Jennings WC, Beathard JA, et al. Fistula first breakthrough initiative: targeting catheter last in fistula first. Sem Dialysis. 2012. http://fistulafirst.org/LinkClick.aspx?fileticket=GN8QYytKHFo%3d&tabid=39
4. Lin PH, Bush RL, Nguyen L, Guerrero MA, Chen C, Lumsden AB. Anastomotic strategies to improve hemo-dialysis access patency- a review. Vasc Endovascular Surg. 2005;39(2):135-142.
5. Tortolani EC, Tan AH, Butchart S. Percutaneous translu-minal angioplasty. An ineffective approach to the failing vascular access. Arch Surg. 1984;119(2):221-223.
6. Collier PE, Saracco GM, Young JC, Fragola JA, Con-tractor FM, Diamond DL. Nonoperative salvage of subcutaneous hemodialysis fistulae. Am J Nephrol. 1985;5(5):333-337.
7. Berger MF, Aruny JE, Skibo LK. Recurrent thrombosis of PTFE dialysis fistulas after recent surgical thrombec-tomy: salvage by means of thrombolysis and angioplasty. J Vasc Interv Radiol. 1994;5(5)725-730.
8. Tan TL, May KK, Robless PA, Ho P. Outcomes of endo-vascular intervention for salvage of failing hemodialysis access. Ann Vasc Dis. 2011;4(2):87-92.
9. Raynaud A, Novelli L, Bourquelot P, Stolba J, Beys-sen B, Franco G. Low-flow maturation failure of distal accesses: treatment by angioplasty of forearm arteries. J Vasc Surg. 2009;49(4):995-999.
10. Hood DB, Yellin AE, Richman MF, Weaver FA, Katz MD. Hemodialysis graft salvage with endoluminal stents. Am Surg. 1994;60(10):733-777.
11. Davila Santini L, Etkin Y, Nadelson AJ, Safa T. Stent-grafts improve secondary patency of failing hemodialy-sis grafts. J Vasc Access. 2012;13(1):65-70.
12. Beathard GA, Settle SM, Shields MW. Salvage of the nonfunctioning arteriovenous fistula. Am J Kidney Dis. 1999;33(5):910-916.
13. Beathard GA, Arnold P, Jackson J, Litchfield T; Phy-sician Operators Forum of RMS Lifeline. Aggres-sive treatment of early fistula failure. Kidney Int. 2003;64(4):1487-1494.
14. Tordoir JH, Rooyens P, Dammers R, van der Sande FM, de Haan M, Yo TI. Prospective evaluation of failure modes in autologous radiocephalic wrist access for he-modialysis. Nephrol Dial Transplant. 2003;18(2):378-83.
15. Back MR, Maynard M, Winkler A, Bandyk DF. Ex-pected flow parameters within hemodialysis access and selection for remedial intervention of nonmaturing conduits. Vasc Endovascular Surg. 2008;42(2):150-158.
16. Scaffaro LA, Bettio JA, Cavazzola SA, et al. Main-tenance of hemodialysis AVF by an interventional strategy: clinical and duplex US surveillance fol-
Copyri
ght H
MP Com
munica
tions
CASE REPORT AND REVIEW
Vascular Disease Management® July 2014 155
lowed by transluminal angioplasty. J Ultrasound Med. 2009;28(9):1159-1165.
17. Falk A. Maintenance and salvage of arteriovenous fistu-las. J Vasc Interv Radiol. 2006;17(5):807-813.
18. Miller GA, Hwang W, Preddie D, et al. Percutaneous salvage of thrombosed immature arteriovenous fistulas. Semin Dial. 2011; 24(1):107-114.
19. De Marco Garcia LP, Davila-Santini LR, Feng Q,
Calderin J, Krishnasastry KV, Panetta TF. Primary bal-loon angioplasty plus balloon angioplasty maturation to upgrade small-caliber veins for AVFs. J Vasc Surg. 2010;52(1):139-144.
20. Gorin DR, Perrino L, Potter DM, Ali TZ. Ultrasound-guided angioplasty of autogenous arteriovenous fistulas in the office setting. J Vasc Surg. 2012;55(6):1701-1705.
Copyri
ght H
MP Com
munica
tions