Embed Size (px)
Citation preview

Endovascular treatment for aorto-enteric
fistula and aorto-caval communication
Athanasios D. Giannoukas, MD, MSc, PhD, FEBVS
Professor of Vascular Surgery
University of Thessaly Medical School
Chairman, Department of Vascular Surgery
University Hospital of Larissa, Greece
Aorto-enteric fistula
• Abnormal communication between aortic and bowel
lumen necessitating immediate intervention
• Primary (incidence 0.02 – 0.07%)or secondary (more
often: <1%)
• GI bleeding alone or in combination with sepsis
Aorto-enteric fistula
Conventional surgical repair
• Primary: Aortic ligation and extra-anatomic bypass
• Secondary: extra-anatomic by-pass, graft excision
and aortic ligation or
graft excision and in-situ aortic reconstruction
• High morbidity and mortality rates (>40%)
O’Mara CS et al. Am J Surg 1981;142:203
Bianchi P et al. Surg Today 2007;37:1053
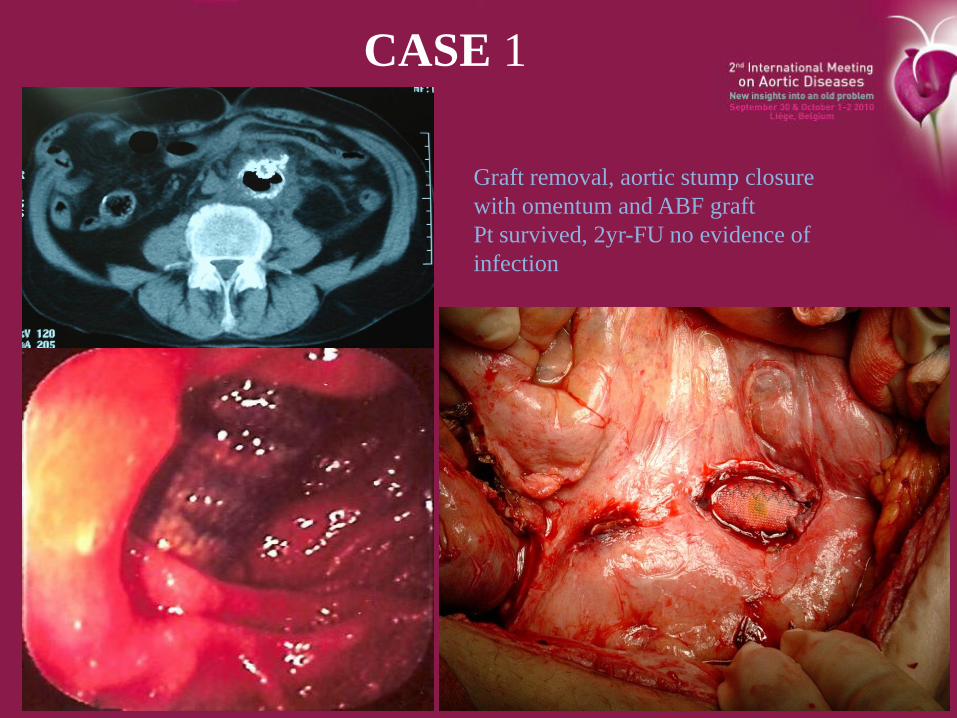
CASE 1
Graft removal, aortic stump closure
with omentum and ABF graft
Pt survived, 2yr-FU no evidence of
infection
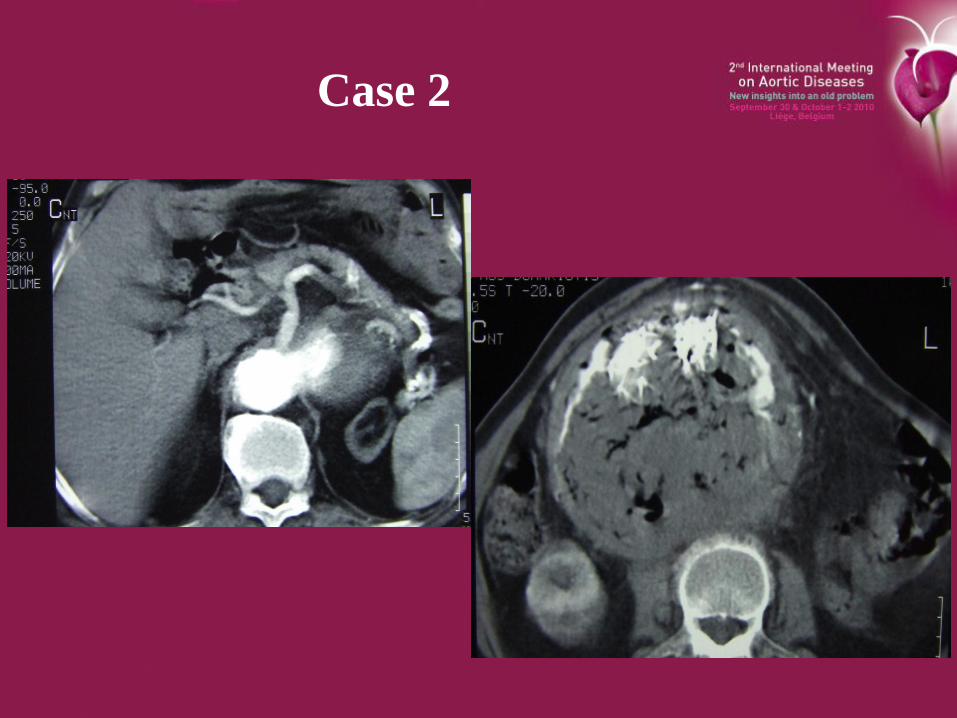
Case 2
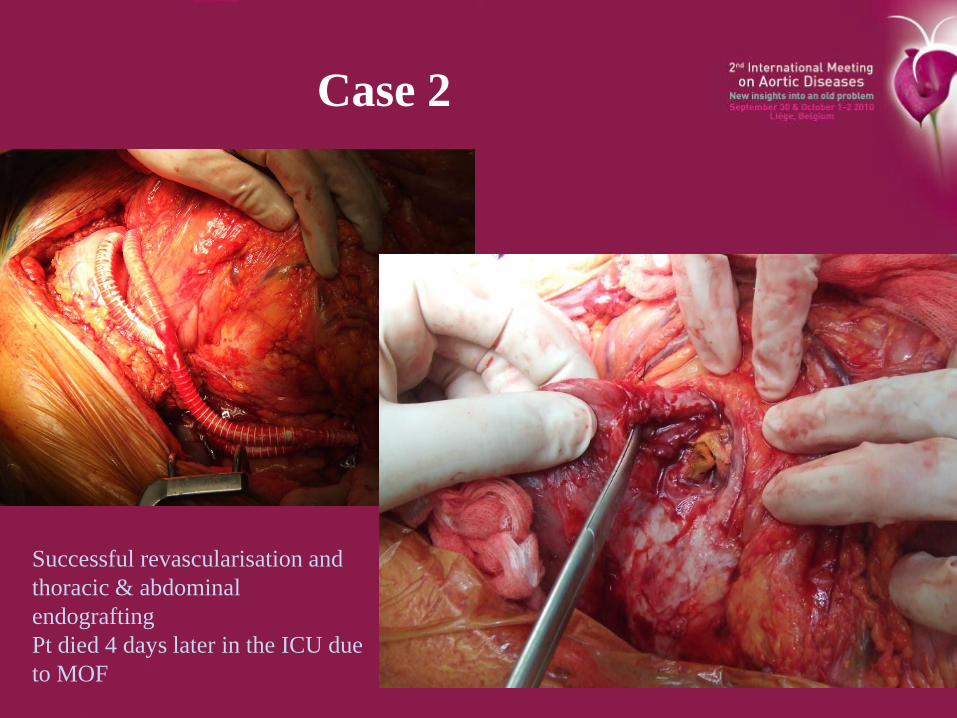
Case 2
Successful revascularisation and
thoracic & abdominal
endografting
Pt died 4 days later in the ICU due
to MOF
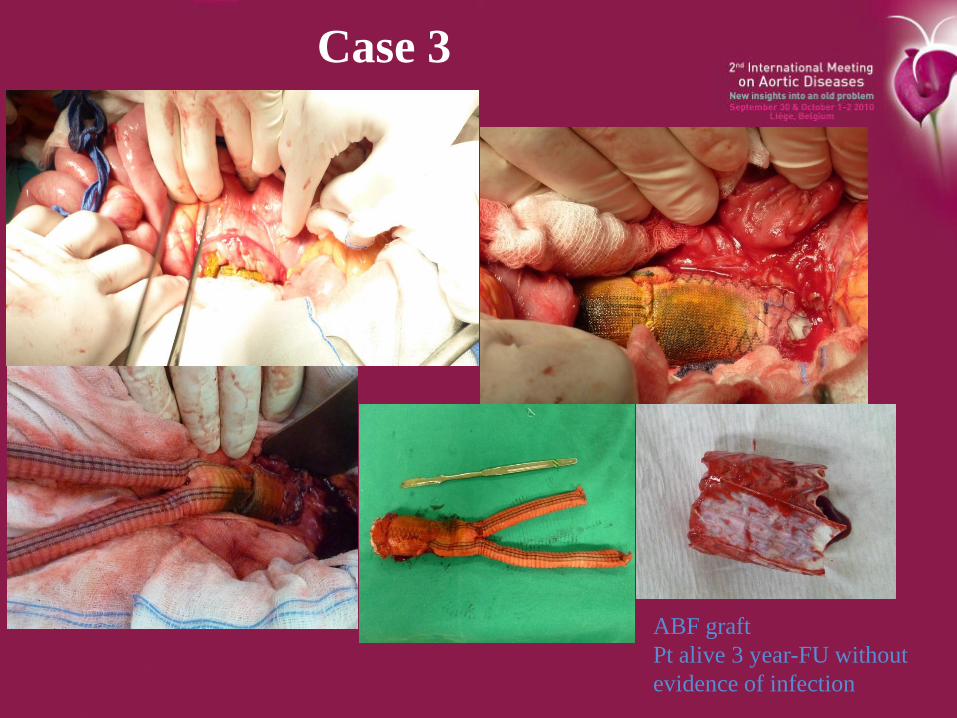
Case 3
ABF graft
Pt alive 3 year-FU without
evidence of infection
Aorto-enteric fistulawhy endovascular treatment?
• Patients with AEFs have limited overall survival.
• Endovascular therapy is an alternative to open repair
associated with decreased perioperative morbidity
and mortality and a shorter in-hospital stay, and
allows for acceptable survival given the presence of
coexisting medical co-morbidities.
• Furthermore, endovascular repair provides a
therapeutic option to control bleeding and allows for
continued intervention in a stabilized setting.
Baril DT et al. J Vasc Surg 2006;44:250
Endovascular repair of
Aorto-enteric fistula
• Systematic review of English literature up to April
2008
• Endovascular repair of primary or secondary A-E
fistulae
• 33 reports with 41 pts
Antoniou GA, Koutsias S, Antoniou SA, Georgiakakis A, Lazarides M,
Giannoukas AD. J Vasc Surg 2009;49:782-9
Endovascular repair of
Aorto-enteric fistula
• Persistent/recurrent/new infection or haemorrhage
developed in 44% after a mean f-up of 13 mths
• Secondary as compared to primary AEF had an
almost three-fold increased risk
• Evidence of co-existing sepsis was factor of
unfavourable outcome (p< .05)
• Persistent/recurrent/new infection after treatment was
associated with worse 30-day and overall outcome
(p< .05)
Antoniou GA, Koutsias S, Antoniou SA, Georgiakakis A, Lazarides M,
Giannoukas AD. J Vasc Surg 2009;49:782-9
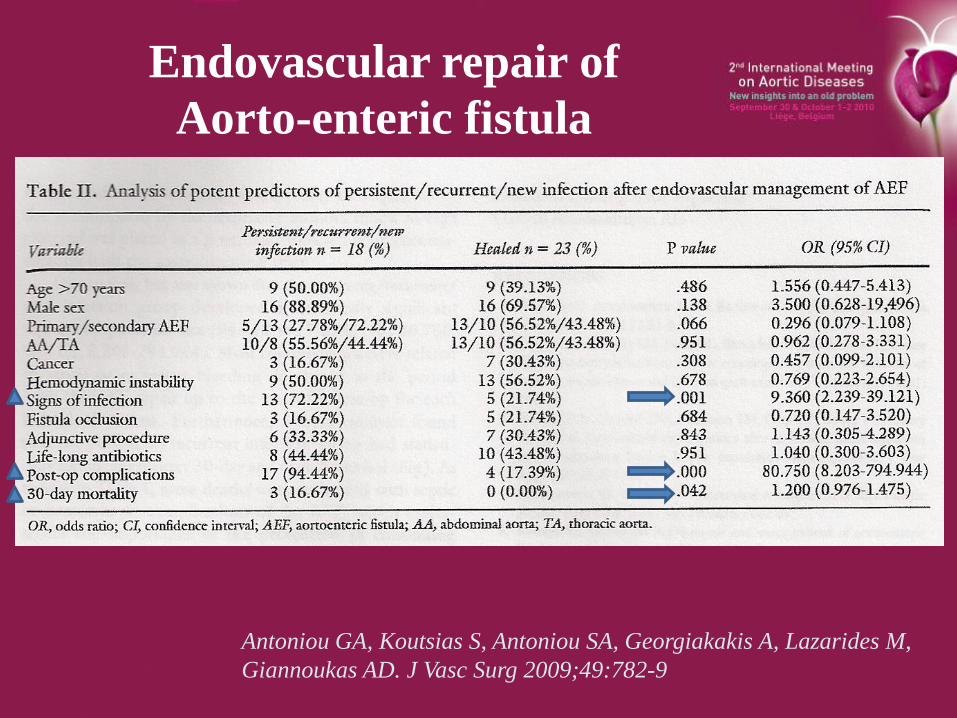
Endovascular repair of
Aorto-enteric fistula
Antoniou GA, Koutsias S, Antoniou SA, Georgiakakis A, Lazarides M,
Giannoukas AD. J Vasc Surg 2009;49:782-9
Aorto-enteric fistulaEVAR vs surgical repair
• Report on 25 pts during 12 year period
• Preoperative sepsis in 76% (19)
• EVAR: 8 pts – OR: 17 pts
• In-hospital mortality better in EVAR (0% VS 35%)
• Recurrence-free, sepsis-free & overall long-term
survival similar in both groups
• 2-year overall survival in pts with pre-op sepsis was
worse (24% vs 50%)
Kakkos SK, Antoniadis PN, Clonaris C, Papazoglou KO, Giannoukas AD, Matsagas MI, Kotsis T,
Dervisis K, Gerasimidis T, Tsolakis IA, Liapis CD.
Presented at ESVS 2010 Annual meeting in Amsterdam
Aorto-enteric fistulaIn-situ surgical repair with homografts
• 57 patients treated with cryopreserved arterial homografts for
the in situ reconstruction of abdominal aortic infections.
• Thirty-day mortality was 9% (5 of 57 patients).
• Median follow-up was 36 months (range, 4-118 months);
• 3-year survival was 81%, and freedom from reoperation was
89%.
• Five patients (9%) required reoperation, in one patient each
for postoperative bleeding, acute cholecystitis, homograft
occlusion, homograft-duodenum fistula, and aneurysmal
degeneration.
• No recurrence of infection was reported.
Bisdas T et al. J Vasc Surg 2010;52:323

EVAR: bridge therapy or complete treatment?
Do we need RCT?
Aorto-enteric fistulaEVAR vs surgical repair
Aorto-caval communication
• Rare clinical condition
• Abnormal communication between the aorta or the
iliac arteries and the inferior vena cava or the iliac
veins
• Primary (80%) – Secondary (iatrogenic or traumatic)
Historical aspects
• 1st description by Syme in 1831
Syme J. Edinb Med Surg J 1831;36:104-6
• 1st surgical repair by Cooley
Cooley DA. Ann Surg 1955;142:623
Open surgical repair
• Associated with high morbidity and mortality
• Problems
arterialisation of venous structures
perivascular inflammation blood loss
risk of pulmonary embolism
cardiac decompensation because of hyperdynamic state
Adjuncts to open surgery
• Percutaneous balloon occlusion of the IVC to
facilitate open surgery and minimise blood loss
Laureys M et al. J Vasc Interv Radiol 2002;13:211-3
Espinel CF et al. J Vasc Surg 2006;43:834-5
Endovascular repair
• Systematic review
• English literature from 1/1990 – 1/2009
• 21 articles reporting on 22 pts plus 1 pt in our own
report Total 23 pts
Antoniou GA, Koutsias S, Karathanos Ch, Sfyroeras G, Vretzakis G,
Giannoukas AD. J Endovasc Ther 2009;16:514-23
Endovascular repair
• Primary 65%
• Secondary 35%22% (5 pts ) after AAA open repair (2) or EVAR (3)
9% (2) previous open abdo trauma
4% iatrogenic trauma in lumbar disc surgery
Condition initially misdiagnosed in 22% (5 cases)
Endovascular repair
• Technical success 96%
Failure in 1 case with primary aorto-left renal vein fistula
• No 30-day mortality
• Mean ICU stay 2 days (0-9)
• Mean post-intervention in –hospital stay 9 days (2-24)
• 1 death to unrelated reasons in mean f-up 9 mths (7-24)
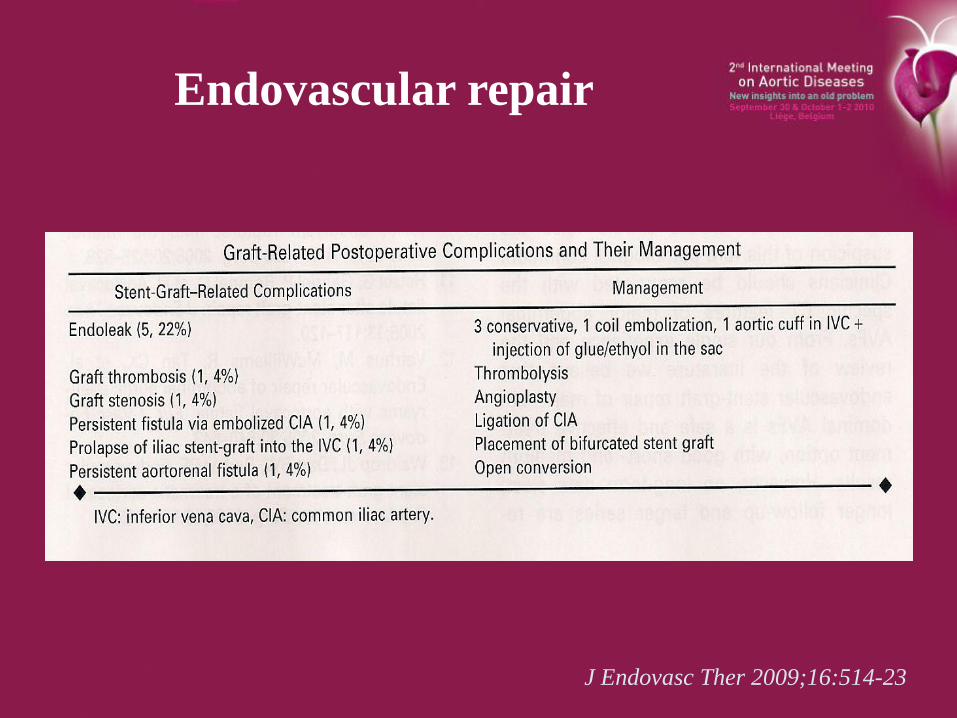
Endovascular repair
J Endovasc Ther 2009;16:514-23
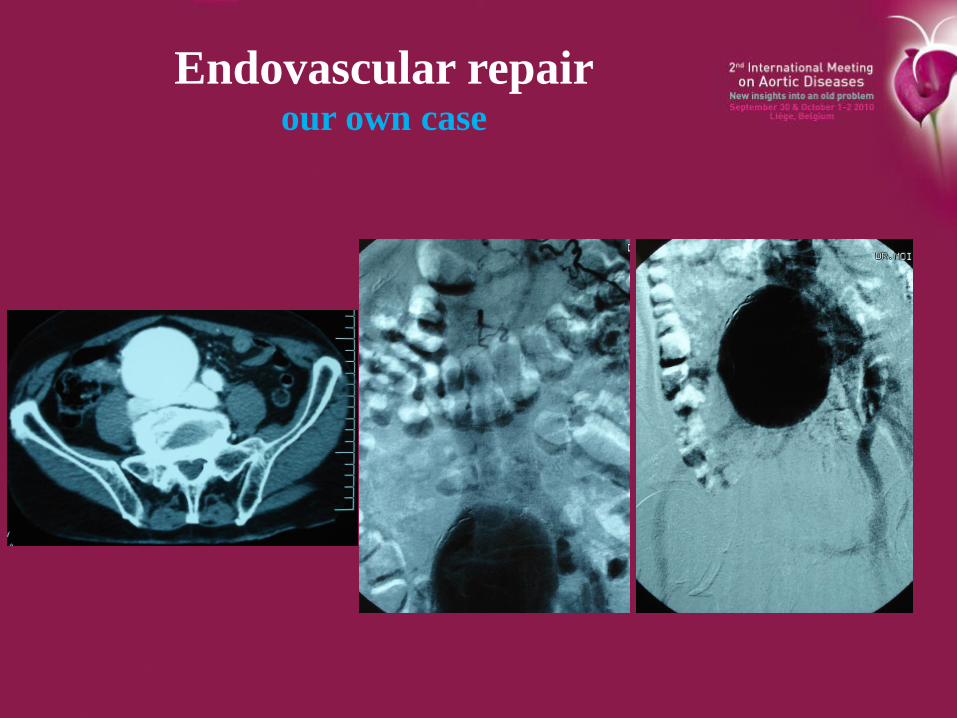
Endovascular repairour own case
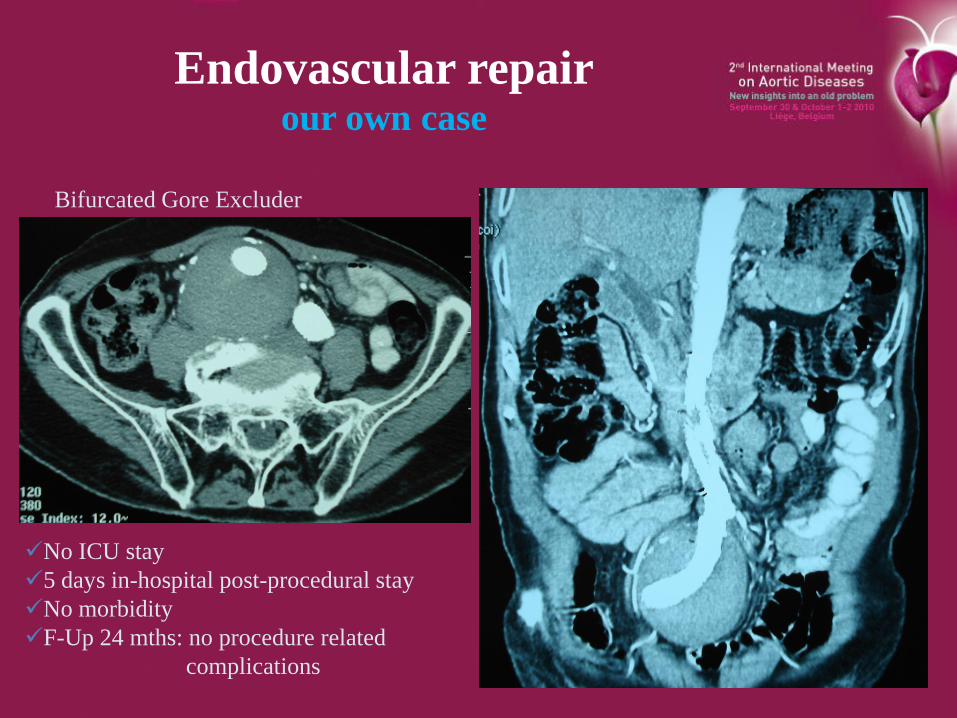
Endovascular repairour own case
Bifurcated Gore Excluder
No ICU stay
5 days in-hospital post-procedural stay
No morbidity
F-Up 24 mths: no procedure related
complications

Thanks for the attention