Embed Size (px)
Citation preview

International Review of Psychiatry, October 2009; 21(5): 465–471
Enhancing Pathways Into Care (EPIC): Community development workingwith the Pakistani community to improve patient pathways within a crisisresolution and home treatment service
RASHNA HACKETT1, JO NICHOLSON2, SIMON MULLINS1, TONY FARRINGTON1,
SHARON WARD1, GARETH PRITCHARD1, ELIZABETH MILLER1, &
NAYLA MAHMOOD1
1Sheffield Health and Social Care NHS Foundation Trust, Sheffield, UK and 2Sheffield Teaching Hospital NHS Foundation
Trust, Sheffield, UK
AbstractBlack and Minority Ethnic (BME) communities receive different pathways into mental health care with BME service usersoften presenting in crisis. This is associated with both an over representation of such groups in psychiatric wards and peopleavoiding mainstream services altogether. The Sheffield Crisis Resolution Home Treatment (CRHT) created the EnhancingPathways Into Care (EPIC) project, which initially focused on engagement with the Pakistani community (the largest BMEgroup in Sheffield). The project aimed to empower the Pakistani community to seek mental health support earlier withintheir own community, build up trust in mainstream services and enhance the clinical pathways within services to providemore culturally appropriate care. CRHT joined with the local Pakistani Muslim Centre (PMC) to work in partnership. ThePMC had existing links with the Pakistani community and provided a range of social, respite and occupational opportunities.The partnership created an innovative new role: the Pakistani link worker. The EPIC partnership strengthened the PMC’sinfluence and raised awareness of mental health issues in the community. Through integration of the link worker within theeveryday practice of clinicians, pathways of care showed evidence of positive change including more referrals to the PMCfrom psychiatric services. The EPIC project piloted a model of partnership working that is effective and transferable.
Introduction
The city of Sheffield has developed from its largely
industrial roots to cover an extensive economic base.
The city enjoyed world-wide recognition during
the nineteenth century for its production of steel.
International competition resulted in the decline
of the local industry in the 1970s–1980s. The
population of Sheffield is estimated at 513,234
people. The ethnic composition of Sheffield’s pop-
ulation is 91.2% white, 5.1% Asian, 1.8% black and
1.6% mixed. Sheffield also has large Polish, Somali,
Slovak, Yemeni and Albanian populations.
According to the 2001 Census (Sheffield City
council, 2001), Pakistanis form the largest black
and minority ethnic (BME) group in Sheffield with a
population of 15,844 people (3.1%). Sheffield has for
three decades had twice the national representation
of Pakistanis (White & Scott, 2006).
Evidence suggests that the majority of the black
and minority ethnic population live in the major
cities and particularly inner cities. Pakistanis and
Bangladeshis are most likely to live in the most
deprived wards (Dorsett, 1998). The related social
disadvantage has implications for health and illness.
In terms of health in Sheffield, the Pakistani,
Bangladeshi and mixed ethnic groups have a high
incidence of long-term limiting illness and for the
Pakistani population this is despite having very
low numbers of older people. According to a 2006
report by the Sheffield Director of Public Health,
increased diversity of the population of Sheffield has
resulted in services struggling to respond adequately.
The position in mental health services mirrors this
finding.
Sheffield enhancing pathways into care
The available national evidence suggests that by
the time many BME communities access secondary
mental health services it is usually in crisis. This in
turn creates a profound impact on their families, and
individuals can experience great difficulty in reinte-
grating back into their communities with any sense of
dignity. The poor early detection of mental health
Correspondence: Rashna Hackett, Email: [email protected]; Simon Mullins, Email: [email protected]; J. Nicholson. E-mail: J.nicholson@
sth.nhs.uk
ISSN 0954–0261 print/ISSN 1369–1627 online � 2009 Institute of Psychiatry
DOI: 10.1080/09540260903163366
Int R
ev P
sych
iatr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
7/14
For
pers
onal
use
onl
y.

problems in primary care compounds the problem of
pathways of care for BME communities seeking
mental health services. Further, data gathered from
the audit department of Sheffield Health and Social
Care NHS foundation trust (SHSC) suggests that
BME representation within the acute psychiatric
wards is disproportionately high.
It is within this context that our project is set; the
CRHT Service has been in a unique position to
contribute to the improvements in pathways of care
for our Pakistani population. The Sheffield CRHT
leadership took on the challenge of improving health
inequalities and created the EPIC project. The
project mission was to empower the Pakistani
community to seek mental health support earlier
within their own community and build up trust to
use the mainstream services. CRHT joined with a
community organisation called the PMC to work in
partnership. The PMC is located in the heart of the
Pakistani community in Sheffield and provides a
range of social, respite and occupational opportu-
nities. The partnership created an innovative new
role, the Pakistani link worker, influenced by the
Department of Health (2006) guide to ‘Community
Development Workers’. This role was to build
bridges with the Pakistani community and integrate
with the everyday practice of the acute care staff to
influence their pathways of acute care. The EPIC
partnership achieved much broader influences and
these only emerged as the relationships flourished.
The evidence of change (both quantitative and
qualitative) is presented below.
Crisis resolution and home treatment
(CRHT)
One of the Government’s key targets for mental
health services was the establishment of 335 crisis
resolution and home treatment teams by Dec 2004.
These teams act as the gatekeepers to acute psychi-
atric services and aim to provide home treatment
for people in crisis, as far as possible, as well as
supporting early discharge for those admitted into
inpatient beds (Department of Health, 2001). In
addition, the Sheffield CRHT was seeking to make
the service more responsive and accountable to the
local population and prioritise social inclusion with
scope to involve voluntary and non-statutory agen-
cies in a coordinated system of mental health care.
The team was also keen to ensure equitable
care pathways were sought, i.e. varied routes to the
recovery process.
Translating policy into practice
The EPIC project design was influenced by govern-
ment policy. The Delivering Race Equality (DRE)
action plan (Department of Health, 2005) was
launched after an enquiry into the death of an
African Caribbean man in a forensic unit. Systemic
review of the evidence base for working with BME
communities led to a three building block framework
for services to seek local solutions to the problem of
inequalities in care.
Delivering Race Equality
1. Better Information more intelligently used
2. Community engagement
3. More appropriate and responsive service
Utilising this framework enabled the project team
to have a robust strategy for developing a cohesive
approach to project management, including identifi-
cation of areas for capacity building but also resource
constraints.
Engaging the Pakistani community in a process that
would yield partnership work was the first step to this
project. The CRHT leadership team sought to utilise
the community development model to enhance
services for Pakistani communities. The strength of
the community development approach recognises the
belief that people know best about their own needs
and requirements, and that they have knowledge,
abilities and experiences which should be utilised.
However, the responsibility for policy development
and practice cannot be the individual responsibility of
the Pakistani communities; it requires a multi-agency
approach with effective partnership arrangements.
This involves building on the strength and creativity of
the community in a manner which does not exploit or
oppress them.
A partnership was created by the CRHT with
a local non-statutory provider called the Pakistani
Muslim Centre (PMC).
Strategic and clinical intervention
The EPIC project has two strands of delivery;
strategic and clinical. The strategic intervention
focused upon the DRE building blocks and within
this framework sought to address:
. Better information more intelligently used – utilise
audit department within SHSC, reciprocal skills
transfer between PMC and SHSC for data collec-
tion, management and interpretation, planning
and provision of reciprocal training initiatives
. Community engagement – introducing forums and
consultations that involved executive board mem-
bers/directors from SHSC and PMC as well as
project team members, full representation of PMC
to national EPIC forums, PMC facilitating SHSC
and the project team to meet the ‘community’
through formal and informal events, commitment
466 R. Hackett et al.
Int R
ev P
sych
iatr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
7/14
For
pers
onal
use
onl
y.

to social inclusion agenda expressly stated and
articulated in project aims
. More appropriate and responsive services – the
conceptualisation of an improved/enhanced care
pathway for Pakistani people was achieved through
the two foundations of better information and
community engagement.
Overall, the strategic delivery aimed to build
capacity across both organisations and communities.
The clinical strand aimed to better understand and
improve the pathway and experience of Pakistani
patients in receipt of Home Treatment and/or
admitted to the Acute Psychiatric Inpatient Services.
Strategic outcomes
A major outcome was developing a well described
model of community involvement, participation and
collaboration that could be transparently utilised as
a basis for other DRE-related initiatives. However,
the model is not restricted to issues of diversity
in terms of race and culture but is applicable to
development work with any community organisation
that aims to improve health outcomes.
Another major outcome was the recruitment of
a dedicated community development worker, whose
job specification was to improve patient pathways
for Pakistani service users. This post was funded
by SHSC, specifically following on from the early
involvement of SHSC executive board members and
the SHSC equalities lead. Significantly, this post,
whilst funded through the statutory board, handed
management and ownership to the host community
of the PMC. This continued as a mutually beneficial
and reciprocal arrangement with clinical supervision,
mentoring and guidance provided through CRHT
and inpatient staff.
Other outcomes, that should not be underplayed,
included attendance by PMC members to national
EPIC events and hosting of a national EPIC event
within PMC and with open attendance by commu-
nity members. This significantly reflects the degree
of partnership and the genuine embracing of
collaborative working. The attendance and involve-
ment of community at the national EPIC event
within PMC meant a transparent and explicit
statement from SHSC acknowledging problems
for community access, and demonstration of a pre-
paredness to seek mutually acceptable and flexible
approaches to improve relationships.
Clinical outcomes
In terms of the clinical strand, the EPIC project
built upon service strengths within the Sheffield
CRHT. From service inception, the Sheffield
Crisis Resolution and Home Treatment service had
a comprehensive audit strategy that had a core
purpose of facilitating examination of issues of
diversity and equity. There was also a small, but
significant, number of staff who expressed an interest
and wish to improve the ‘reception’ and experience
of people from black and minority ethnic groups.
The EPIC project utilised these internal resources,
successfully developing, expanding but also focusing
the clinical interests and strategic repertoire of the
existing staff. A core project team internal to the
CRHT service was therefore built, whose members
could ‘champion’ the project within the service and
whose composition reflected the multi-disciplinary
ethos of CRHT.
Audit design
The focus of the EPIC audit was to provide data
about patterns of access and standards of care within
CRHT across a two-year period (presenting data
from 2005 and comparing this to 2006). These two-
year periods could be roughly conceptualised as
representing periods prior to EPIC (year period
2005) and active project development (year period
2006). Whilst there had been problems and delays
in achieving full implementation in 2006, this
year period still represented an impactful stage of
preparation where engagement of stakeholders,
refinement and development of project purpose
were all actively occurring both within and outside
CRHT.
The pathway of focus for this audit is diagram-
matically represented in Figure 1.
Measures
The Sheffield CRHT has a clinical database that
included information on patterns of access, clinical
Pakistani patient referred to CRHT in crisis
Home treatment Early discharge
PMC link worker/
CRHT
Inpatient ward
Social/respite and
occupational needs
PMC link worker/CRHT
Social/respite and
occupational needs
PMC link worker
Pakistani Muslim Centre
Figure 1. Sheffield EPIC – Clinical intervention pathways.
Enhancing Pathways Into Care 467
Int R
ev P
sych
iatr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
7/14
For
pers
onal
use
onl
y.
pathways within CRHT, clinical outcomes, inpatient
activity and demographic data. The existing database
enabled the working team to easily examine patterns
of access and changes across the two time-periods,
although some data components were not available
across both year periods.
Specific to the EPIC project, a ‘Standards of Care
Checklist’ was developed that enabled retrospective
interrogation of case notes and could be used to
compare received care standards across different
ethnic groups. The checklist provided a detailed
examination of the core administrative and clinical
care components delivered to patients and families.
The checklist was completed based upon the
written notes and, therefore, was as much an audit
of documentation standards as of quality of care
provided.
The Pakistani link worker also provided a quali-
tative account of their project work and processes.
Results
Demographics
As CRHT is effectively a community service, but
one that provides a crisis response and an alterna-
tive to hospital admission, it was important to
understand whether CRHT had differential rates of
access as compared with inpatient services and to
the population statistics for the Sheffield area. The
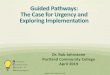
results are summarised in Figure 2 which shows the
local situation mirrored the national picture of
disproportionate use of inpatient care for BME
groups (Healthcare Commission, 2005). In 2005,
the proportion of BME groups on psychiatric wards
in Sheffield was double what you would expect if it
simply reflected the general population in the
community (21.5% cf. 10.9%). However, the fact
that Pakistanis only represented 3.9% of the total
Sheffield inpatient population in 2005 (cf. 3.1% of
the general Sheffield population in 2001) indicates
that over representation on inpatient wards is more
of an issue for other BME groups. It is heartening
to find at face value that the CRHT had a very
similar percentage distribution to the acute inpatient
services for BME groups, as access to community-
based services can be a problem for BME groups.
The CRHT and inpatient data was interrogated
in more detail, which showed there was a marginal,
increase in referral rate of British Asian/Asian
Pakistanis to the CRHT service between 2005 and
2006. There were no significant changes in propor-
tional distribution of inpatient admission rate
between 2005 and 2006 across the ethnic
groups reported. It is probably to be expected that
the EPIC project would not significantly impact on
some pathways of care within a year. However,
Table 1 shows the changes that occurred reflecting,
on face value an overall positive trend towards
pathways that EPIC aimed to enhance. For example,
proportionately more Pakistanis were referred to the
CRHT (31 more Pakistani patients in total) which
may indicate greater confidence in use of the service.
Despite these ‘green shoots of recovery’, statistically
significant changes in pathways such as avoiding
Table 1. Comparing clinical pathways for Pakistanis before EPIC
(2005) and during the first year of the project (2006). Pathways
relate to those represented in Figure 1.
2005 2006
Pakistanis referred to CRHT
in crisis
80(2.6%) 111(3.2%)
Pakistanis receiving Home
Treatment
19(3.8%) 17 (3.4%)
Pakistanis admitted to hospital 33(4%) 32(3.8%)
Referred to PMC from Home
Treatment
1 7
Referred to PMC from
Inpatient ward
0 9
Numbers in brackets are the proportion that Pakistanis representof the whole clinical population.
89.1 84.878.5 83.0
10.9 15.221.5 17.0
3.1 2.7 3.9 2.9 3.60
102030405060708090
100
2001 Census SheffieldPsychiatricInpatient
Admissions2005–2006
CAHT TotalEpisodes
2005–2006
CAHT HomeTreatment
2005–2006
All black and minority ethnicWhite British British asian/Asian Pakistani
Health carecommission 2005
SnapshotPsychiatric
Inpatient survey
83.0
17.0
Figure 2. Summary demographic data for Sheffield, Sheffield CRHT and inpatient services by BME group.
468 R. Hackett et al.
Int R
ev P
sych
iatr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
7/14
For
pers
onal
use
onl
y.

admission to hospital and improved access to Home
Treatment could not be shown.
Standards of Care Checklist
The Standards of Care Checklist was used to compare
different groups for the 2005 period. Three sample
groups from the home treatment population were
identified for comparison of checklist standards;
White UK, British Asian/Asian Pakistani, Black/
Black British Caribbean. This enabled comparison
of potential differences of White UK compared to
BMEs, but also Pakistani service users as compared
to other BME groups. For the White UK group
a random sample of patient identification numbers
was drawn from the database. For the two BME
groups the sample represents every case-note file that
could be found for the CRHT BME service user
population. For both BME groups some files were
not accessible at the time of the audit. For the 2006
period the checklist was used to interrogate notes
for Pakistani home treatment patients only, enabling
comparison in standards between the two year-
periods.
The analysis of the Standards of Care Checklist
revealed huge discrepancies in the standard of
note keeping from individual case to individual
case – but no discernable trends by group were
observed and the amount of variability case by case
meant the audit tool served best to illustrate
problems in quality of note keeping across the
board rather than the tool having utility for the task
in hand – i.e. to discern potential differences in qual-
ity in processes and procedures of care for specific
groups.
As the project was subject to a developmental
process of refinement (i.e. increasing clarity regard-
ing the focus and specificity of intervention) that was
not mirrored by changes in the audit tools, the audit
tool was found to have limited utility for the
emerging purpose of the EPIC project.
Patient pathway
The pathway data from CRHT and inpatient services
shows that whilst there are minimal fluctuations in
access rates to both services, the early discharge flow,
and the flow to the PMC improved (see Table 1) is
significantly improved. Whilst the numbers are small,
the dramatic difference to quality of life and function
that can be afforded by community support and
access cannot be underestimated. Reduction in
isolation, increase in opportunity and access can all
make a critical difference to the individual pathway to
recovery. Further, there were marked improvements
in 2006 in access for CRHT Pakistani service users
to statutory day services and alternative non-
statutory services (usually when refusing attendance
at the PMC, in contrast to clinical practice prior to
the EPIC project, Pakistani patients were offered a
mainstream alternative). Therefore, the EPIC project
had served to highlight and put the social and
occupational and needs of this vulnerable group
high onto the agenda of staff working within the
CRHT service, facilitating referral onwards to com-
munity-based support services.
Qualitative report from link worker
The PMC link worker provides regular contact
to both the CRHT and the acute psychiatric inpa-
tient wards. In both settings the worker, where
appropriate and practically achievable, would attend
multidisciplinary team meetings. This enabled recip-
rocal learning:
. The link worker learnt about the roles of staff and
the structures, processes and methods of clinical
decision making
. A developing relationship enabled increased
understanding and trust over time, a mutual
exploration of role, value and contribution
. The link worker provided information and acts as
a resource for staff to explore issues of culture,
increasing capacity through knowledge sharing to
make inpatient staff more aware and sensitive of
cultural needs, to apply this learning to enhance
the care of new patients who may enter the wards
at later times
. It assisted in the identification of unmet need
with patients, carers and other family members,
advocating and signposting to both mainstream
and culturally appropriate support services
. It provided a link to the PMC as a culturally
appropriate community resource
. It provided knowledge of the capacity of inpatient
wards as compared to CRHT
The link worker identified the particular concerns
of families and carers and their fears about treatment
on inpatient wards, in particular where the patient is
a female member of the family. The link worker
observed that members of the family would often stay
with the patient 24 hours a day, despite reassurances
about safety. She commented that ‘the cultural
aspect is so strong that girls are not left by themselves
in any case, mothers will stay with them despite
hassle and inconvenience to them by doing this’. In
these cases the link worker would advocate for early
discharge to home treatment.
Enhancing Pathways Into Care 469
Int R
ev P
sych
iatr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
7/14
For
pers
onal
use
onl
y.
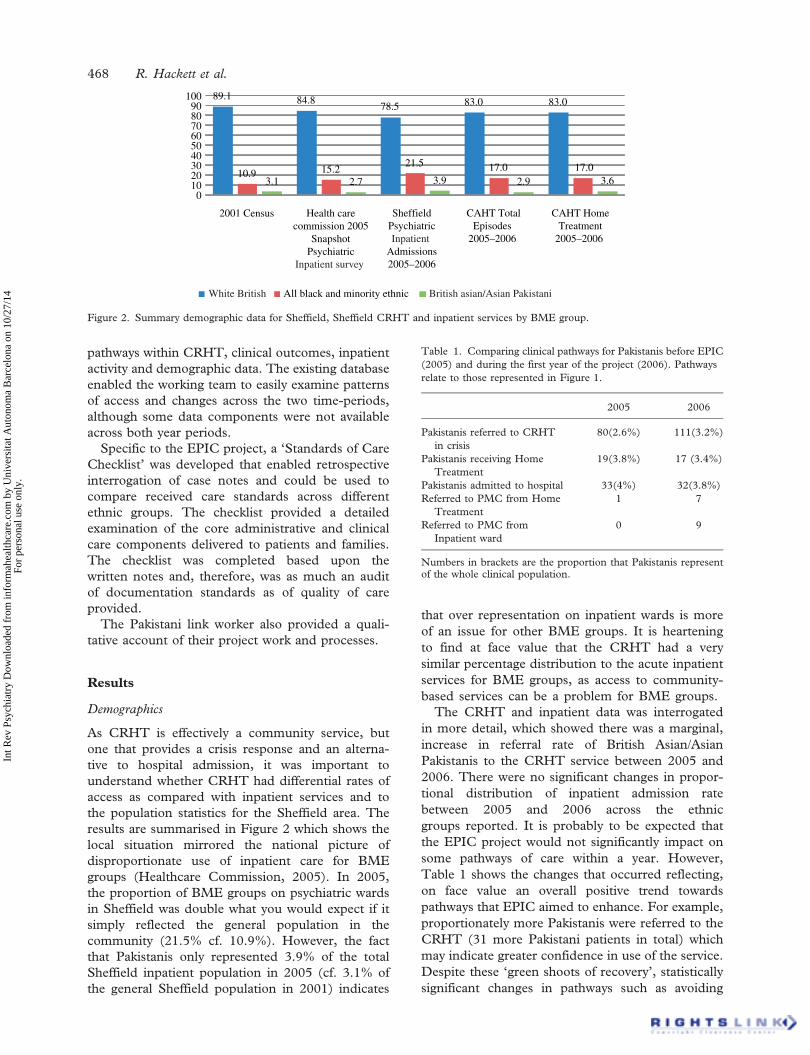
Impact for inpatient services
A further measure of outcome for EPIC was impact
on inpatient admission and length of stay for the
Pakistani group. There were minimal fluctuations
in numbers and proportional percentages admitted
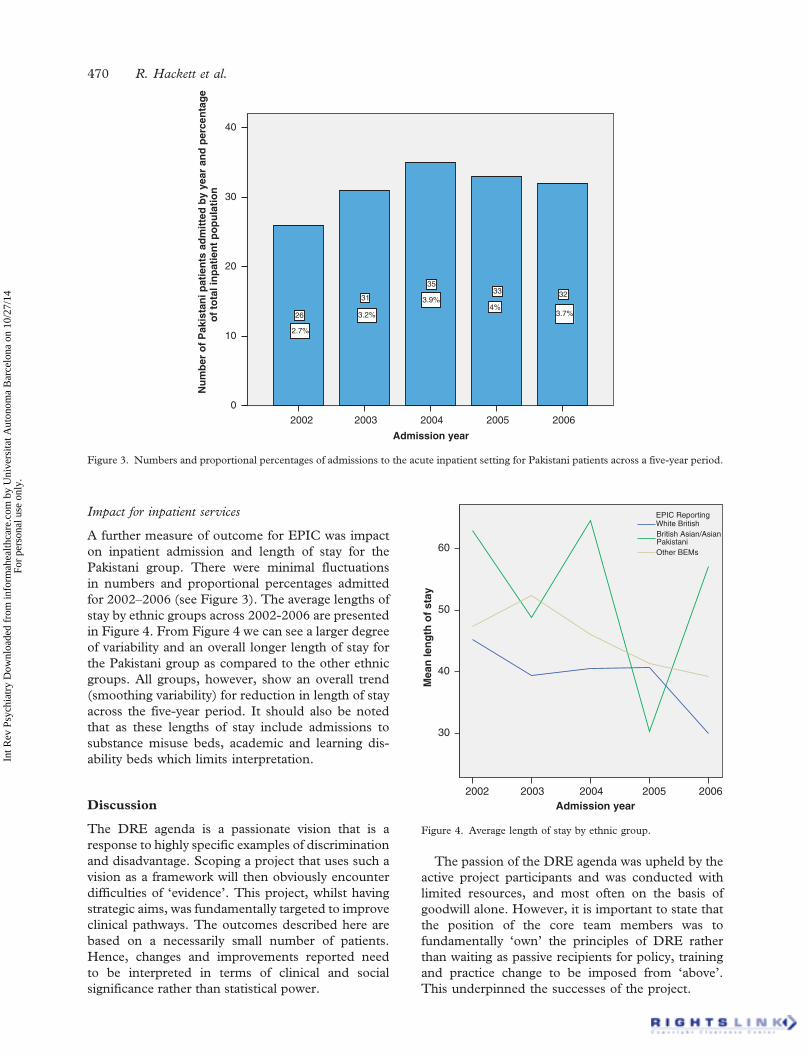
for 2002–2006 (see Figure 3). The average lengths of
stay by ethnic groups across 2002-2006 are presented
in Figure 4. From Figure 4 we can see a larger degree
of variability and an overall longer length of stay for
the Pakistani group as compared to the other ethnic
groups. All groups, however, show an overall trend
(smoothing variability) for reduction in length of stay
across the five-year period. It should also be noted
that as these lengths of stay include admissions to
substance misuse beds, academic and learning dis-
ability beds which limits interpretation.
Discussion
The DRE agenda is a passionate vision that is a
response to highly specific examples of discrimination
and disadvantage. Scoping a project that uses such a
vision as a framework will then obviously encounter
difficulties of ‘evidence’. This project, whilst having
strategic aims, was fundamentally targeted to improve
clinical pathways. The outcomes described here are
based on a necessarily small number of patients.
Hence, changes and improvements reported need
to be interpreted in terms of clinical and social
significance rather than statistical power.
The passion of the DRE agenda was upheld by the
active project participants and was conducted with
limited resources, and most often on the basis of
goodwill alone. However, it is important to state that
the position of the core team members was to
fundamentally ‘own’ the principles of DRE rather
than waiting as passive recipients for policy, training
and practice change to be imposed from ‘above’.
This underpinned the successes of the project.
20062005200420032002
Admission year
40
30
20
10
0
Nu
mb
er o
f P
akis
tan
i pat
ien
ts a
dm
itte
d b
y ye
ar a
nd
per
cen
tag
eo
f to
tal i
np
atie
nt
po
pu
lati
on
323335
31
26
2.7%
3.2%
3.9%4%
3.7%
Figure 3. Numbers and proportional percentages of admissions to the acute inpatient setting for Pakistani patients across a five-year period.
20062005200420032002Admission year
60
50
40
30
Mea
n le
ng
th o
f st
ay
Other BEMs
British Asian/AsianPakistani
White BritishEPIC Reporting
Figure 4. Average length of stay by ethnic group.
470 R. Hackett et al.
Int R
ev P
sych
iatr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
7/14
For
pers
onal
use
onl
y.

This does not imply that the process was an easy or
a smooth one. Negotiation for consensus of personal
and professional meaning in relation to project aims,
objectives and procedures often delayed progress
and interrupted process. The issue of resourcing
was also a highly significant factor to delay, arrest
and interruption of the work in hand. The issue of
resourcing remains as the community development
post initiated was not funded through recurring
funds and hence there are issues of continuity.
The project team also hold broad professional
interests and have to some extent dispersed to
follow other (often related but separate) strands of
diverse work.
Lord Darzi (Darzi, 2008) has published a review
that sets out a vision to provide mental health
services for all. ‘Partnership Working’ and improving
pathways are key elements for achieving positive
change. This project was necessarily limited because
of focus on crisis and acute working; similar work is
urgently needed for early detection and improved
early access to primary care assessments and inter-
vention. This has implications for primary care trust
planning and development, with need for specific
focus on BME mental health needs and particularly
at a time of transformation in terms of world-class
commissioning and integration of health and social
care.
Declaration of interest: The authors report no
conflict of interest.
References
Bhui, K., Stansfield, S., Hull, S., Priebe, S., Mole, F. & Feder, G.
(2003). Ethnic variations in pathways to and use of specialist
mental health services in the UK. British Journal of Psychiatry,
182, 105–116.
Darzi, A. (2008). High Quality Care For All: NHS Next Stage
Review Final Report. London: Department of Health. Available
at www.dh.gov.uk/en/Publicationsandstatistics/Publications/
PublicationsPolicyAndGuidance/DH_085825
Department of Health (2001). Mental Health Policy Implementation
Guide. London: Department of Health. Available at
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/
PublicationsPolicyAndGuidance/DH_4009350
Department of Health (2005). Delivering Race Equality in Mental
Health Care, an Action Plan for Reform Inside and Outside
Services; and the Government’s Response to the Independent Inquiry
into the Death of David Bennett. London: Department of Health.
Available at http://www.dh.gov.uk/en/Publicationsandstatistics/
Publications/PublicationsPolicyAndGuidance/DH_4100773
Department of Health (2006). Community Development Workers for
Black and Minority Ethnic Communities: Final Handbook
Department of Health. London: Department of Health.
Available at http://www.dh.gov.uk/en/Publicationsandstatistics/
Publications/PublicationsPolicyAndGuidance/DH_062802
Dorsett, R. (1998). Ethnic Minorities in the Inner City. Bristol: The
Policy Press / Joseph Rowntree Foundation.
Healthcare Commission (2005). Count Me In. London: Healthcare
Commission. Available at http://www.cqc.org.uk/guidancefor
professionals/healthcare/allhealthcarestaff/countmeincensus.cfm
Sheffield City Council (2001). Census. Sheffield: Sheffield City
Council. Available at http://www.sheffield.gov.uk/your-city-council/
sheffield-facts-figures/population-information/2001-census
White, P., & Scott, S (2006) Migration and Diversity in Sheffield:
Past, Present and Future. Sheffield: Department of Geography,
University of Sheffield. Available at http://www.sheffield.gov.uk/
EasySite/lib/serveDocument.asp?doc=92399&pgid=106674)
Enhancing Pathways Into Care 471
Int R
ev P
sych
iatr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
7/14
For
pers
onal
use
onl
y.