Embed Size (px)
Citation preview

Stephen Moore
Yvonne Whitfield
September 19, 2012
Enteric Outbreak Investigations

www.oahpp.ca
Outline
• PHO Role in Outbreak Investigations
• Descriptive Epidemiology of Enteric Disease in Ontario
• Looking Forward
2

www.oahpp.ca
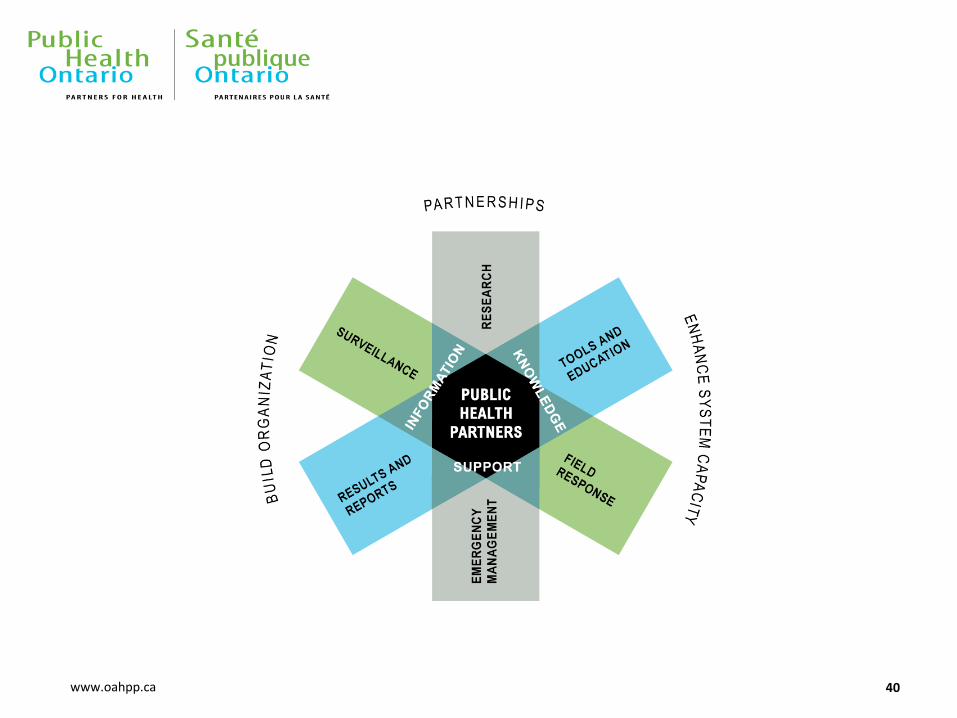
Public Health Architecture
3

www.oahpp.ca
Who: Enteric Outbreaks at PHO
• Communicable Disease Prevention & Control (Jason Garay)
• Surveillance Services Unit • Anne Winter, Tina Badiani,
Brenda Lee, Ellen Chan, Ryan Walton
• Enteric Zoonotic & Vector Borne Diseases Unit • Stephen Moore, Jackson Chung,
Christina Lee, Dr Dean Middleton, Yvonne Whitfield
• PHO Laboratories • Dr Vanessa Allen, Dr Tony
Mazzuli, Dr Anna Majury, Anne Maki, Erik Kristjanson, Peter Boleszczuk, Analyn Peralta, Suzanne Lombardi
4
• Environmental & Occupational Health (Dr Ray Copes)
• Akbar Ali, Naghmeh Parto, Alison Samuel
• Emergency Preparedness (Dr Brian Schwartz)
• Incident Response • Lisa Fortuna, Dr Mark Nelder,
Amrita Maharaj
• Communicable and Infectious Diseases (Dr Natasha Crowcroft)
• Dr Colin Lee, Dr Liane MacDonald

www.oahpp.ca
What We Do: Provincial Outbreaks
• S. Heidelberg, By Month, Ontario, Jan. 2008 – Mar. 2012*
5 * As of Mar. 9, 2012

www.oahpp.ca
6

www.oahpp.ca
How We Detect Provincial Outbreaks
• Laboratory Line List Review
• National Enteric Surveillance Program (NESP) algorithms
• Early Aberration Reporting System (EARS) flags
• Notifications from partners
• Informal communications with partners
7

www.oahpp.ca
Outbreak Communications & Coordination
• Daily Situation Report & Morning Rounds
• Public Health Alerts
• Enhanced Surveillance Directive
• Important Health Notices
• Outbreak Central
• Outbreak reports
• Ontario Outbreak Investigation Coordination Committee
8
Notifications of suspect and confirmed Botulism cases in Ontario
Communications Issued

www.oahpp.ca
• Loyalty Card Data
• Trace back and trace forward
• Environmental sampling
• Case Control Study
9
Microbiology Epidemiology Food Safety Investigation
Weight of Evidence
Health Risk Assessment
Action
Hypothesis Generation
• Standardized questionnaires
• Food Frequency tables & comparisons to reference values
• Field Epidemiologist (Centralized Interviewing)
• Laboratory sub-typing
Outbreak Investigation
Hypothesis Testing

www.oahpp.ca
Who Takes Public Health Action
• Health Units
• MOHLTC
• Canadian Food Inspection Agency • Product Tracing Investigations
• Environmental Testing
• Collates evidence for submission to Health Canada for a Health Risk Assessment
• Voluntary Recalls (company initiated or CFIA requested)
• Mandatory Recalls by Ministerial order (rare)
10
Trigger
Recall
Implementation
Recall Effectiveness
Verification
Corrective Action/
Follow-up
Health Risk
Assessment
Food Safety
Investigation
Recall
Decision-
making

www.oahpp.ca
Health Canada
• http://www.hc-sc.gc.ca/fn-an/alt_formats/pdf/pubs/securit/2011-food-illness-outbreak-eclosion-malad-ailments-eng.pdf
11
• Epidemiology, Microbiology, Product Tracing
• Comments on Intact vs Non-Intact samples
• Content & Format of a Health Risk Assessment (HRA)
• Information needed for a HRA
• Health Risk Definitions

www.oahpp.ca
Public Health Agency of Canada
• Leadership and coordination in national outbreaks
• In provincial outbreaks • Can do jurisdictional scans to identify similar clusters in other provinces
or countries
• Can supply field epidemiologists if required
• Develops common platforms to aid outbreak investigation (CNPHI, CIOSC, etc)
• Reviews strength of outbreak epidemiological evidence to give opinion to Health Canada during the health risk assessment process
12

www.oahpp.ca
Ontario Ministry of Agriculture Food & Rural Affairs (OMAFRA) • Meat Inspection Program, Dairy Food Safety Program, Foods of Plant Origin
• Monitor compliance with standards, licensing, inspection, audit, advisory, education
• Detention, seizure, disposal but not recall authority
• Licensed meat and dairy facilities can have licenses suspended or revoked
• Areas like minimally processed foods and niche milk products not well covered by existing legislation
13
Ministry of Natural Resources (MNR)
Our Provincial Colleagues
• Interim food fish safety program
• Seizure of product possible but no recall authority and no ability to close operations
Ministry of Health and Long Term Care (MOHLTC) • Policy and programs
• Provincial Outbreak Leadership
• Public Health Action

www.oahpp.ca
PHO Functions in Enteric Outbreaks
• Incident Response • Communications with partners • Briefing of CMOH and other Senior
Management
• Enteric, Zoonotic, and Vector Borne Diseases Unit • Outbreak detection through lab
surveillance and external notifications • Investigation of clusters • Technical advice on case related
aspects of investigations • Information gathering, hypothesis
generation, planning • Public Health Alerts
• Surveillance Services Unit • iPHIS based outbreak detection • Formal data analysis (food frequency
tables, etc) • Questionnaire design • Enhanced Surveillance Directives
14
• Environmental and Occupational Health Department • Product tracing investigations • Scientific and technical advice related
to environmental aspects of investigations
• Communicable and Infectious Diseases Department • Medical consultative advice as required
• PHO Laboratories • Testing & Subtyping of clinical
specimens • Testing & Subtyping of environmental
isolates • Facilitating and arranging testing and
subtyping at federal labs where assays are not available provincially
• Medical Microbiologists interpretation of laboratory results
• Guidance on sample collection and submission

www.oahpp.ca
Guidance Documents
• 2004:
• Canada Foodborne Illness Outbreak Response Protocol to Guide a Multi-Jurisdictional Response
• 2006:
• Ontario Foodborne Health Hazard and Illness Outbreak Investigations Memorandum of Understanding (MOU)
• 2010:
• Canada’s Foodborne Illness Response Protocol (FIORP)
• The Ontario Multi-Agency Foodborne Outbreak/Food Recall Working Group organizes a Subgroup to develop Ontario’s Foodborne Illness Outbreak Response Protocol (ON-FIORP)
• Other Guidance Documents • Food Premises Plant Investigation
• Traceback Traceforward
• Effectiveness Checks for Food Recalls
• CFIA Verification Procedures
15
www.oahpp.ca
The Value of Your Work in Provincial Outbreaks
• Thorough case exposure ascertainment generates strong hypotheses
• Timely entry of cases assists with early outbreak detection
• Notification of situations of interest can help determine if subtyping would be useful
• Environmental specimen collection and handling can make or break an HRA
• Specific product details are critical for recall action to occur
• Your input in outbreak debriefs improves future investigations
16

www.oahpp.ca
A DESCRIPTIVE STUDY OF REPORTABLE GASTROINTESTINAL ILLNESSES (GI) IN ONTARIO, CANADA, FROM 2007 TO 2009
17
Linda Vrbova, Karen Johnson, Yvonne Whitfield, Dr. Dean Middleton, PHO Surveillance and Epidemiology Team

www.oahpp.ca
Study Purpose
• Conduct analysis of the Integrated Public Health Information System (iPHIS)data for reportable Gastrointestinal Illness (GI) for the period of January 2007 –December 2009
• Examine the incidence of each disease, demographics, outcomes, seasonality, likely sources of infection and exposure settings
18

www.oahpp.ca
Flow diagram of reported GI illnesses 2007 to 2009
Not Successfully Followed Up:
Lost to Follow Up (3,588)
Untraceable (171)
Pending (1,612)
No Exposure Information (4,464)
Exclusions by Exposure Information:
Multiple exposures (460)
Unclear/Unclassifiable Exposures
(559)
Reported confirmed GI cases for 14
reportable diseases (n=29,897)
Cases not followed
up or excluded based
on unclassifiable
exposure information
Cases with exposure information
(n=19,043, 63.7% of all cases)
Sporadic endemic GI cases
(n=13,341, 44.6% of all cases)
Travel and Outbreak Exclusions:
Relevant travel history outside of
Ontario (5,248; 17.6% of all cases)
Non-index case in an outbreak (454)
Cases excluded due to
travel or for being part
of an outbreak
Cases successfully followed up
(n=20,062, 67.1% of all cases)
19
Data source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2012/04/01]

www.oahpp.ca
Results: Incidence by Illness
Reportable gastrointestinal illnesses in Ontario by year, 2007 to 2009.
Data source: Ontario Ministry of Health and Long-Term Care, integrated Public Health
Information System (iPHIS) database, extracted by Public Health Ontario [2012/04/01]
Reportable Disease
2007 2008 2009 Total
N1 Incidence /100,0002
N1 Incidence /100,0002
N1 Incidence /100,0002
N3 Mean annual
incidence /100,0004
Amebiasis 814 6.4 761 5.9 559 4.3 2,134 5.5
Campy 3,883 30.3 3,789 29.3 3,244 24.8 10,916 28.1
Giardiasis 1,612 12.6 1,610 12.4 1,504 11.5 4,726 12.2
Salmonellosis 2,819 22.0 2,385 18.4 2,310 17.7 7,514 19.4
VTEC 317 2.5 278 2.1 165 1.3 760 2.0
Total Overall 10,746 84.0 10,125 78.3 9,026 69.1 29,897 77.1

www.oahpp.ca
Reportable gastrointestinal illnesses in Ontario by travel, outbreak, hospitalization, and mortality
Top Travel-related GI
• Paratyphoid Fever
• Typhoid Fever
• Cyclosporiasis
• Hepatitis A
High Hospitalization Rates
• Botulism
• Listeriosis
• Typhoid Fever
• VTEC /Paratyphoid Fever
21

www.oahpp.ca
Results: Reported Exposure Source, Ontario, 2007-2009
Reportable Disease
Primary Source (%)*
n Animal Food Person Water Other
Amebiasis 120 1.7% 8.3% 82.5% 5.8% 1.7%
Campylobacteriosis 1,272 26.9% 63.1% 6.0% 2.8% 1.3%
Giardiasis 344 14.2% 5.5% 36.0% 40.7% 3.5%
Hepatitis A 54 0.0% 7.4% 87.0% 0.0% 5.6%
Listeriosis 12 8.3% 75.0% 8.3% 8.3% 0.0%
Paratyphoid Fever 2 0.0% 50.0% 50.0% 0.0% 0.0%
Salmonellosis 1,148 15.2% 73.1% 9.9% 1.3% 0.4%
Shigellosis 90 0.0% 16.7% 80.0% 0.0% 3.3%
Typhoid Fever 2 0.0% 0.0% 50.0% 0.0% 50.0%
VTEC-illness 158 18.4% 49.4% 19.6% 10.8% 1.9%
Yersiniosis 84 15.5% 81.0% 1.2% 0.0% 2.4%
Total 3,466 19.8% 54.2% 16.9% 7.6% 1.5%
22 Data source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2012/04/01]

www.oahpp.ca
Results: Sporadic domestic reportable GI Ontario, 2007-2009
Reportable Disease
Primary Setting (%)†
n Food Premises Private Home Other
Amebiasis 15 33.3% 26.7% 40.0%
Campylobacteriosis 796 31.2% 47.5% 21.3%
Cryptosporidiosis 92 2.2% 16.3% 81.5%
Cyclosporiasis 10 70.0% 20.0% 10.0%
Giardiasis 164 3.7% 33.5% 62.8%
Hepatitis A 16 25.0% 50.0% 25.0%
Listeriosis 9 22.2% 44.4% 33.3%
Salmonellosis 754 37.7% 48.4% 14.0%
Shigellosis 28 46.4% 50.0% 3.6%
VTEC-illness 106 28.3% 43.4% 28.3%
Yersiniosis 65 15.4% 66.2% 18.5%
Total 2,058 29.7% 45.5% 24.8%
23 Data source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2012/04/01]

www.oahpp.ca
Incidence of Reportable Disease by Age, Ontario, 2007-2009
24
Data source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2012/04/01]
www.oahpp.ca
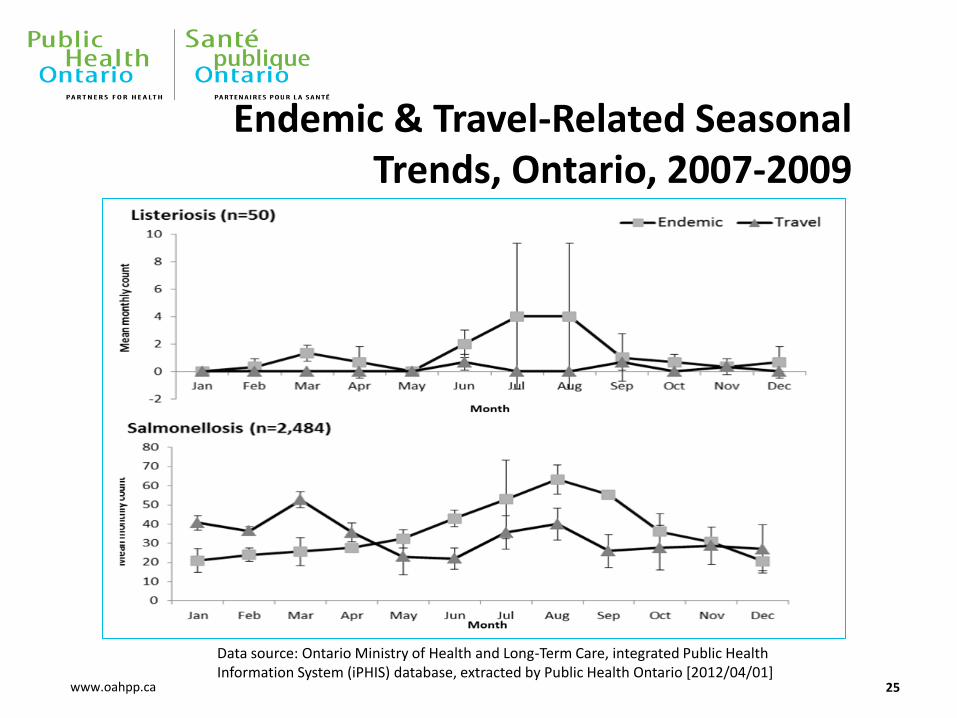
Endemic & Travel-Related Seasonal Trends, Ontario, 2007-2009
25
Data source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2012/04/01]

www.oahpp.ca
Endemic and Travel Related Illness, Ontario, 2007-2009
26
Data source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2012/04/01]

www.oahpp.ca
Discussion
• Approximately 9000 to 10,700 cases of GI are reported annually
• A slight decrease in the overall numbers was detected when compared to data from 1997 to 2003
• Disease with highest incidence is campylobacter followed by salmonellosis
• Salmonella outbreaks accounted for 42% of outbreaks reported
• 27 per cent of GI cases were acquired outside of the province, with marked variation by pathogen
• Food was identified as the primary source (54%) of GI reported for all pathogens combined
27

www.oahpp.ca
Discussion
• Contact with animals accounted for 19.8 % of all GI
• The private home was the most common (45.5%) primary exposure setting reported for all sporadic endemic cases for nine of 14 diseases
• Exposure to food premises accounted for 29.7% of GI illness cases during the study period
• The following diseases followed a seasonal distribution of cases: campylobacteriosis, cryptosporidiosis, giardiasis, salmonellosis and E. coli infections
28

www.oahpp.ca
Study Limitations
• iPHIS is a passive, dynamic surveillance system
• 34.8 per cent of cases were not successfully followed up by public health due lost to follow-up, case refusing to be interviewed etc.
• Disease follow-up is often prioritized by risk of transmission and/or severity of the disease. Not all diseases are “treated equally”
• Follow-up of reportable diseases varies by health unit
• Exposure and risk setting data are based on the recall of the cases and on the assessment of the public health investigators
• A large proportion of exposures are not reported because of difficulties in identifying the source of infection and/or missing data
29

www.oahpp.ca
Conclusions
• Reportable GI continues to be a burden in Ontario
• Food, animal contact and contact with ill persons are the most commonly reported sources of illness
• Food premises and private homes are the most commonly reported risk setting
• International travel is an important risk factor for most GI, with travel-related cases presenting distinct seasonal patterns from endemic cases.
• These findings underscore the ongoing need for public education on safe handling of food and animals as well as proper hand hygiene practices.
30

www.oahpp.ca
LOOKING FORWARD
31

www.oahpp.ca
32

www.oahpp.ca
Centralized Interviewing
• Numerous interviewers do not allow for: • Effective hypothesis generation through informal information gathered
from cases by a single interviewer
• Timely follow-up/testing of hypotheses
• Numerous interviewers introduce: • Variation in interviewing style
• Variation in questionnaires used
• Variation in data recording on questionnaires
• History in Ontario: • December 2000 Salmonella Enteritidis PT30 associated with almonds
• Numerous Federal Field Epidemiologists
• August 2010: Minnesota model
• Today: Increasingly widely applied model across US
33

www.oahpp.ca
Enteric Exposure Data
• Web Based Data Capture • Real-time access to questionnaire data
• Centralized database
• Entry from multiple sites
• Entry from multiple users simultaneously
• No/limited need for data entry at PHO
• Self-administered questionnaires?
• Advantages of Fluid Surveys • Data stored on Canadian servers
• Wide variety of question types (branching, skip patterns)
• User-friendly interface (no/limited training requirements)
• Small company open to collaboration/opportunities to develop tools
34

www.oahpp.ca
Improving Efficiency
Clusters Detected
Clusters Investigated
Outbreaks Investigated
Outbreaks Successfully Investigated
35
• Review Lab Line List • Monitor iPHIS based EARS Flags • Monitor Lab based NESP Flags
• Review iPHIS Exposure Data • Request Exposure Data from HUs • Call Health Units to discuss cases • Preliminary Conference Call
• Public Health Alert • OOICC or OICC • Enhanced Surveillance Directive • Field Epi (Single Interviewer) • Data Entry • Hypothesis Generation & Testing
• Effective infection control measure • Food Recall

www.oahpp.ca
Days Post Exposure = Recall Bias
What Can We See?
Under Reporting
Cluster
Case Interviewed
Case Reported to Public Health
Lab Confirmed Case
Sample Obtained
Case Seeks Care
Case Experiences Symptoms/Illness Onset
Person Consumes Exposure of Interest
36
• Telehealth (600 per Wk)
• Over the Counter Pharmaceutical Purchases
• Google Search Terms/Social Media
• Emergency Room/Physician Visits
• Lab Line List (Crystal Reports/NESP)
• Loyalty Cards 0
?
• iPHIS (About 9,000 enteric cases/year)
• Exposure Data Received at PHO

www.oahpp.ca
Exposure Based Aberration Detection
37

www.oahpp.ca
Optimizing Questionnaire Design
3 days before illness (interviewer, record date: d____ / m____ / y______; ( M T W Th F Sat Sun )
(Interviewer note: please probe regarding where foods were eaten and how prepared, e.g. prepared and eaten at home, eaten at a restaurant, take-out, ready-to-eat meal, frozen dinner, etc) Breakfast Lunch Dinner Snacks
38

www.oahpp.ca
The Shotgun
• 12 of 18 pages • Font Size 8
39
Onions
If yes, please specify type(s) below:
Y P N DK
White Y P N DK Yellow Y P N DK Green (scallions) Y P N DK Red Y P N DK Shallots Y P N DK Leeks Y P N DK Other onions
If yes, specify:_______
www.oahpp.ca 40