Embed Size (px)
DESCRIPTION
EPIC – a Chronic Disease Management Initiative in BC. Barbara Ogle, BSc(Pharm), ACPR, MScPhm, RPh VP Clinical Services, Network Healthcare May 31, 2007. Network Healthcare. Network Healthcare - PowerPoint PPT Presentation
Citation preview
EPIC – a Chronic Disease Management Initiative in
BC
EPIC – a Chronic Disease Management Initiative in
BC
Barbara Ogle, BSc(Pharm), ACPR, MScPhm, RPhVP Clinical Services, Network Healthcare
May 31, 2007
Barbara Ogle, BSc(Pharm), ACPR, MScPhm, RPhVP Clinical Services, Network Healthcare
May 31, 2007
Network Healthcare
Network Healthcare• A health services company that supports the
development & delivery of health care through sophisticated networks of clinical professionals.
Pharmacist Network• A service delivery arm of Network
Healthcare that utilizes pharmacists to deliver care to patients.
Network Healthcare• A health services company that supports the
development & delivery of health care through sophisticated networks of clinical professionals.
Pharmacist Network• A service delivery arm of Network
Healthcare that utilizes pharmacists to deliver care to patients.
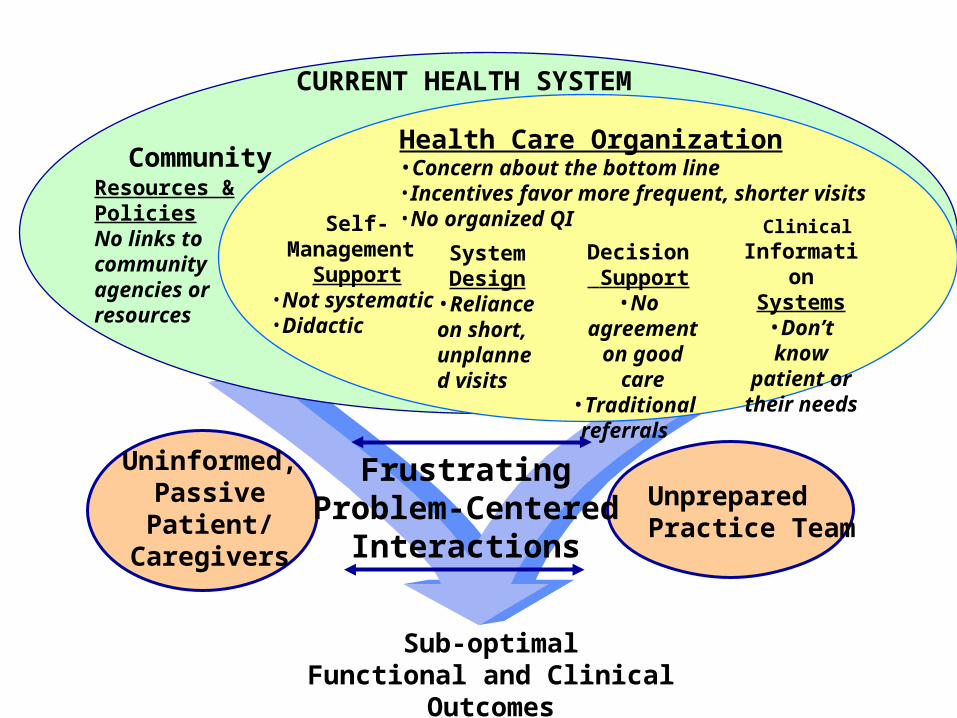
Uninformed,PassivePatient/
Caregivers
FrustratingProblem-Centered
Interactions
UnpreparedPractice Team
SystemDesign
•Reliance on short, unplanned visits
Decision Support
•No agreement on good care
•Traditional referrals
ClinicalInformation
Systems•Don’t know
patient or their needs
Self-Management
Support•Not systematic•Didactic
CURRENT HEALTH SYSTEM
Resources & PoliciesNo links to communityagencies or resources
Community Health Care Organization•Concern about the bottom line•Incentives favor more frequent, shorter visits•No organized QI
Sub-optimalFunctional and Clinical Outcomes
Chronic Disease Management in British Columbia > 50% of BC health care budget goes to
the 10% of people with chronic diseases Ministry of Health’s response
• Adopted the Expanded Chronic Care Model and Patient Self-Management
• Used Primary Health Care Transition Funds for strategic initiatives focused on high-risk, high-cost CDM patients
> 50% of BC health care budget goes to the 10% of people with chronic diseases
Ministry of Health’s response• Adopted the Expanded Chronic Care
Model and Patient Self-Management
• Used Primary Health Care Transition Funds for strategic initiatives focused on high-risk, high-cost CDM patients
Expanded Chronic Care Model

EPIC
Empowering Patients through Integrative Care
Business Need
Expand the primary care team where gaps exist (pharmacist)
Increase system capacity to meet periodic needs of patients for more intense support
Increase access to timely support between appointments and where rural or individual barriers to service exist
Expand the primary care team where gaps exist (pharmacist)
Increase system capacity to meet periodic needs of patients for more intense support
Increase access to timely support between appointments and where rural or individual barriers to service exist
Goal
To develop and evaluate the feasibility of a telehealth model for pharmacists to provide self-management and medication management support to people with diabetes or heart failure in collaboration with primary healthcare teams.
To develop and evaluate the feasibility of a telehealth model for pharmacists to provide self-management and medication management support to people with diabetes or heart failure in collaboration with primary healthcare teams.
Objectives
Increase patient self-efficacy and self-management with medications
Improve attainment of desired drug therapy outcomes
Improve medication safety
Increase patient self-efficacy and self-management with medications
Improve attainment of desired drug therapy outcomes
Improve medication safety
Pharmacist Intervention
Community pharmacist as virtual member of health team
Provide telehealth coaching, information and self-management support for up to 6 weeks
Identify, prevent and/or manage potential and actual drug-related problems
Provide clinical decision support to the family physician and primary healthcare team
Facilitate transition to community resources (e.g., community pharmacist, local groups)
Community pharmacist as virtual member of health team
Provide telehealth coaching, information and self-management support for up to 6 weeks
Identify, prevent and/or manage potential and actual drug-related problems
Provide clinical decision support to the family physician and primary healthcare team
Facilitate transition to community resources (e.g., community pharmacist, local groups)
Project Details
Timeline• Planning 2004• Pilot Testing 2005• Data Collection 2005 – 2006
Team• BC Ministry of Health• BC NurseLine• Pharmacist Network BC• University of Victoria – Centre on Aging• Fraser Health Authority• Northern Health Authority
Timeline• Planning 2004• Pilot Testing 2005• Data Collection 2005 – 2006
Team• BC Ministry of Health• BC NurseLine• Pharmacist Network BC• University of Victoria – Centre on Aging• Fraser Health Authority• Northern Health Authority
Patient Findings (n = 201)
Learned self-management skills Resolved drug-related problems Became more engaged in their own care Improved health status Liked having telehealth in their own
home, interpreters and flexible times Regular follow-up kept patients focused
Learned self-management skills Resolved drug-related problems Became more engaged in their own care Improved health status Liked having telehealth in their own
home, interpreters and flexible times Regular follow-up kept patients focused

Physician Findings (n = 112)
Collaborative interactions observed Electronic lab data accessed for some Telehealth was economical, scalable,
and sustainable Follow-up extended beyond practice
• Focus on patient self-management filled existing care gap
Collaborative interactions observed Electronic lab data accessed for some Telehealth was economical, scalable,
and sustainable Follow-up extended beyond practice
• Focus on patient self-management filled existing care gap
Other Research
Impact of medication therapy discontinuation on mortality after MI• Endpoints: use of aspirin, β blockers and
statins at 1 month; mortality @ 12 months
• >33% had stopped one or more medications
• 12.1% had stopped all three• Poorer 1-year survival than those persisting
88.5% vs 97.7%, p<0.001
• Risk factors include age and education
Impact of medication therapy discontinuation on mortality after MI• Endpoints: use of aspirin, β blockers and
statins at 1 month; mortality @ 12 months
• >33% had stopped one or more medications
• 12.1% had stopped all three• Poorer 1-year survival than those persisting
88.5% vs 97.7%, p<0.001
• Risk factors include age and education
PM Ho et al. Arch Intern Med 2006;166:1842-1847.
Other ResearchOther Research
Drug-related hospitalizations in a tertiary care internal medicine service• n=565 adult patients admitted to hospital
• Drug-related 24.1% (95% CI 20.6-27.8%)– Adverse drug reactions 35.3%
– Improper drug selection 17.6%
– Noncompliance 16.2%
• Majority of cases were preventable• 72.1% (95% CI 63.7-79.4%)
Drug-related hospitalizations in a tertiary care internal medicine service• n=565 adult patients admitted to hospital
• Drug-related 24.1% (95% CI 20.6-27.8%)– Adverse drug reactions 35.3%
– Improper drug selection 17.6%
– Noncompliance 16.2%
• Majority of cases were preventable• 72.1% (95% CI 63.7-79.4%)
Samoy LJ et al. Pharmacotherapy 2006;26:1578-86.
Other Research
Effectiveness of telephone counselling by a pharmacist in reducing mortality in patients receiving polypharmacy• RCT, n=502 non-compliant pts
• 6-8 telephone calls between visits
• Polypharmacy = 5 or more medications
• Endpoint: all-cause mortality in 2 years• ARR 6% (17% control vs 11% intervention)
• RRR 41% (95% CI 0.35-0.97, p=0.039)
• NNT to prevent 1 death = 16
Effectiveness of telephone counselling by a pharmacist in reducing mortality in patients receiving polypharmacy• RCT, n=502 non-compliant pts
• 6-8 telephone calls between visits
• Polypharmacy = 5 or more medications
• Endpoint: all-cause mortality in 2 years• ARR 6% (17% control vs 11% intervention)
• RRR 41% (95% CI 0.35-0.97, p=0.039)
• NNT to prevent 1 death = 16
JYF Wu. BMJ 2006;333:522, doi:10.1136/bmj.38905.447118.2F
Compared to…
Statin therapy• Based on 2003 Canadian guidelines
• NNT to prevent 1 death due to CHD over 5 years for high risk* Canadians is 98
• Canadian statin market = $1.4B
Statin therapy• Based on 2003 Canadian guidelines
• NNT to prevent 1 death due to CHD over 5 years for high risk* Canadians is 98
• Canadian statin market = $1.4B
*10-year risk of CHD ≥ 20%, or history of CVD or diabetes with age > 30 yrs
Going Forward
BC Alberta Service Development
• SAFERx (real world safety & effectiveness)• Seamless Medication Care• Chronic Disease Management (medication
management and self-management support)• Medication Reviews and Assessments• Emergency Preparedness
BC Alberta Service Development
• SAFERx (real world safety & effectiveness)• Seamless Medication Care• Chronic Disease Management (medication
management and self-management support)• Medication Reviews and Assessments• Emergency Preparedness

The ‘Innovation’ Challenge

Contact Information
Barbara Gobis Ogle,
Vice President, Clinical Services
Network Healthcare
604-231-3245