Embed Size (px)
Citation preview
Epicondylitis:Why Bother?
Graham Chuter
SpR Teaching, Freeman Road Hospital March 2007
Overview
• Definition
• Demographics
• Presentation
• Differential Dx
• Management
• Results
• Summary
Names
• Epicondylitis
• Tendonitis
• Tendinosis
• Epicondylalgia
• Epitrochleitis
What is ‘Epicondylitis’?
• Pathological change in the musculo-tendinous origin at the epicondyle
• Acute (rare)• Inflammatory cells
• Chronic• No inflammatory cells• Degenerative
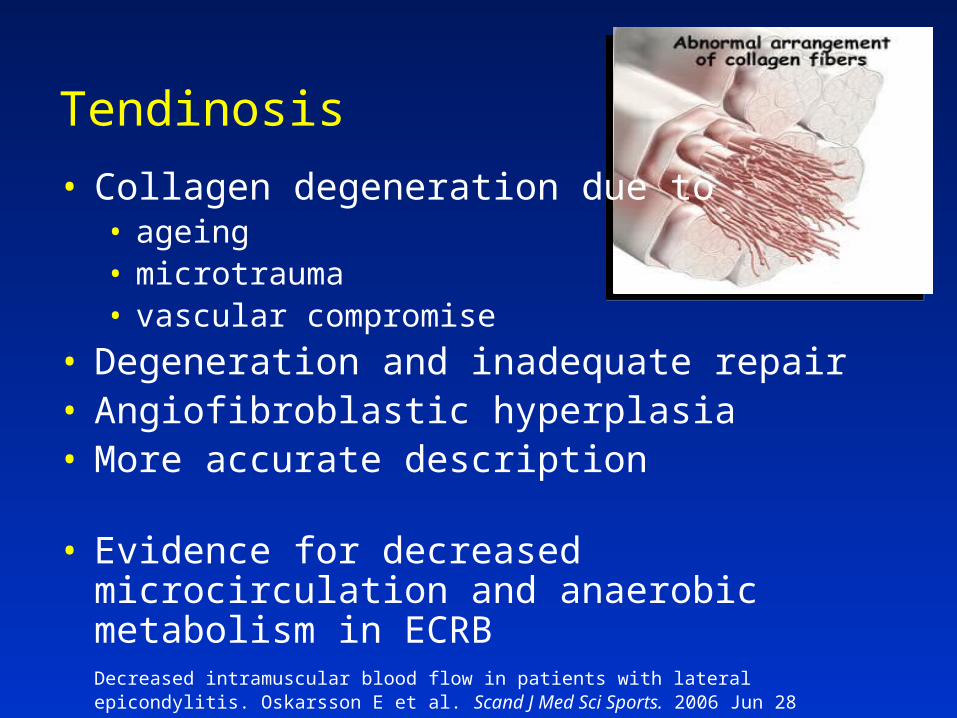
• Collagen degeneration due to• ageing• microtrauma• vascular compromise
• Degeneration and inadequate repair• Angiofibroblastic hyperplasia• More accurate description
• Evidence for decreased microcirculation and anaerobic metabolism in ECRBDecreased intramuscular blood flow in patients with lateral epicondylitis. Oskarsson E et al. Scand J Med Sci Sports. 2006 Jun 28
Tendinosis

Definitions
• Medial“Golfer’s elbow”“Pitcher’s elbow”
• Lateral“Tennis elbow”
Medial epicondylitis (“Golfer’s”)• Overuse syndrome of flexor/pronator mass• Throwing athletes (pitchers)• May be microtear between pronator teres and FCR• Often assoc with ulnar neuritis
Medial epicondylitis (“Golfer’s”)• Overuse syndrome of flexor/pronator mass• Throwing athletes (pitchers)• May be microtear between pronator teres and FCR• Often assoc with ulnar neuritis
Lateral epicondylitis (“Tennis”)• Repetitive pro/supination with elbow extended• Primarily involves ECRB
Demographics
• 4 – 7 per 1000 per year
• Affects 1 – 3% of the population
• Peak at 35 – 54 years
• 4♂:1♀• Medial : lateral → 1:3
• Most common elbow complaint
Demographics
• 15% of workers in ‘at-risk industries’
• Millions of lost workdays per year
• Duration: 6 months to 2 years
• Self-limiting; 90% resolve within 1 year
• Recurrence is common
Risk factors
• Smoking (OR=3.4)• Obesity
• Repetitive movements
• Forceful activities
Prevalence and determinants of lateral and medial epicondylitis: a population study. Shiri R et al. Am J Epid Dec 2006, 164(11):1065
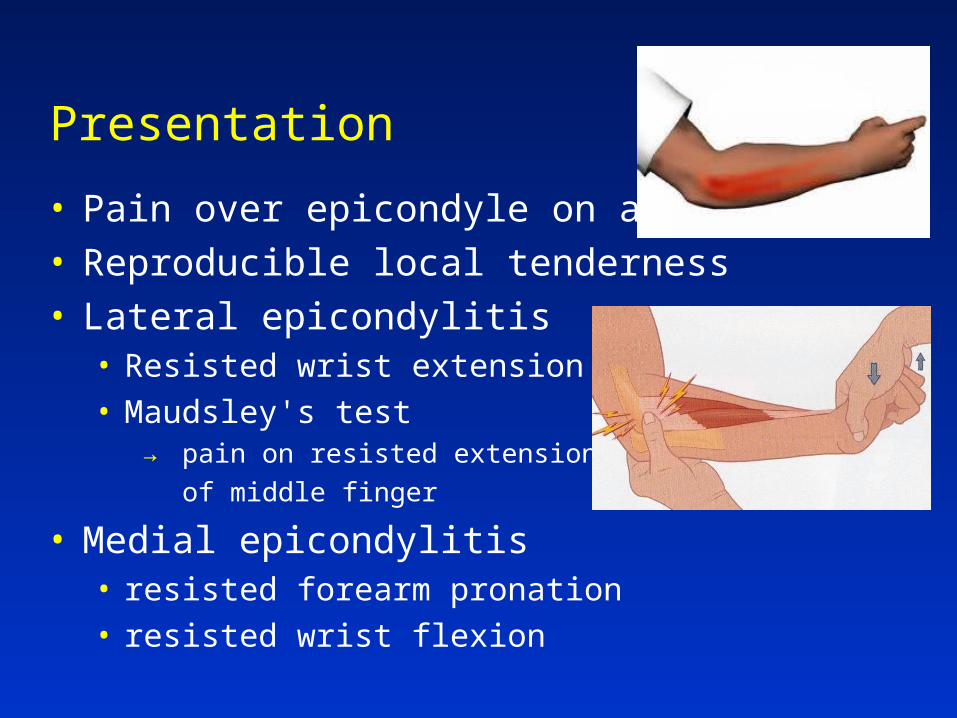
Presentation
• Pain over epicondyle on activity• Reproducible local tenderness• Lateral epicondylitis
• Resisted wrist extension• Maudsley's test
→ pain on resisted extension
of middle finger
• Medial epicondylitis• resisted forearm pronation• resisted wrist flexion
Differential diagnosis of ‘Tennis Elbow’
• C6/7 radiculopathy
• Radial tunnel syndrome
• Posterior interosseous nerve syndrome
• Distal biceps tendon degeneration
• Radiocapitellar arthritis
• Capsular infolding
• Posterolateral instabilityManagement of nerve compression lesions of the upper extremity. Spinner M et al. Management of peripheral nerve problems 2nd ed. 1998 Philadelphia, pp.501-33
(10%)
Management
• Non-operative • successful in 95%
• Operative• only after failed non-operative Rx• usually successful
Non-operative options
• Analgesia• Acupuncture • Blood injection• Bracing• Botulinum toxin• Casting• Change of job• Endurance training • Extracorporeal shockwave Rx• Heat• Ice• Iontophoresis• Low-level laser therapy• Manipulation
• Massage• Oedema control• Phonophoresis• Physio• Polarized polychromatic non-
coherent light • Pulsed electromagnetic field Rx• Rest• Splinting• Steroid injection • Taping• TENS• Topical NSAID gel• Ultrasound
Steroid injection
• Good short-term relief for 6 weeks
• Poorer outcome in the longer term than• watch and wait• physio• placebo
Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. Bisset L et al. BMJ 2006 Nov 4;333(7575):939-44
Steroid injection therapy is the best conservative treatment for lateral epicondylitis: a prospective randomised controlled trial. Tonks J et al. Int J Clin Pract 2007 Feb;61(2):240-6
Physiotherapy
• At 6 weeks:• better than ‘watch and wait’• worse than steroid injection
• Long-term:• better than steroid injection• same as ‘watch and wait’
Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. Bisset L et al. BMJ 2006 Nov 4;333(7575):939-44
Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. Smidt N. Lancet 2002;359: 657-62
Brace / elbow clasp
• Between 12 and 24 weeks:• Pain reduction• Improved functionality• Improved pain-free grip strength
• No better at 12 months
Dynamic extensor brace for lateral epicondylitis. Faes M et al. Clin Orthop Rel Res 2006;442:149-57
Predictors of poor outcome• Dominant hand (OR=3.4)• Manual labour (OR=2.3)• High physical strain at work (OR=3.6)• High level of baseline pain (OR=2.3)• Lower social class
Prognostic factors in lateral epicondylitis: a randomised trial with one-year follow-up in 266 new cases treated with minimal occupational intervention or the usual approach in general practice. Haarh J, Andersen J. Rheumatology. Oct 2003, 42(10):1216
• 83% improved at 1yr, regardless of occupational input
• Intervention did not reduce visits
Predictors of poor outcome
• Workers’ compensation does not appear to affect outcome
But: more workers changed jobs if symptoms persisted
Outcome of surgery for lateral epicondylitis (tennis elbow): effect of worker's compensation. Balk ML et al. Am J Orthop. 2005 Mar;34(3):122-6
Operative options
• Open release
• Arthroscopic release
• Percutaneous release
• Suture anchor repair
• Microtenotomy
• Anconeus transposition
• Radiofrequency probe
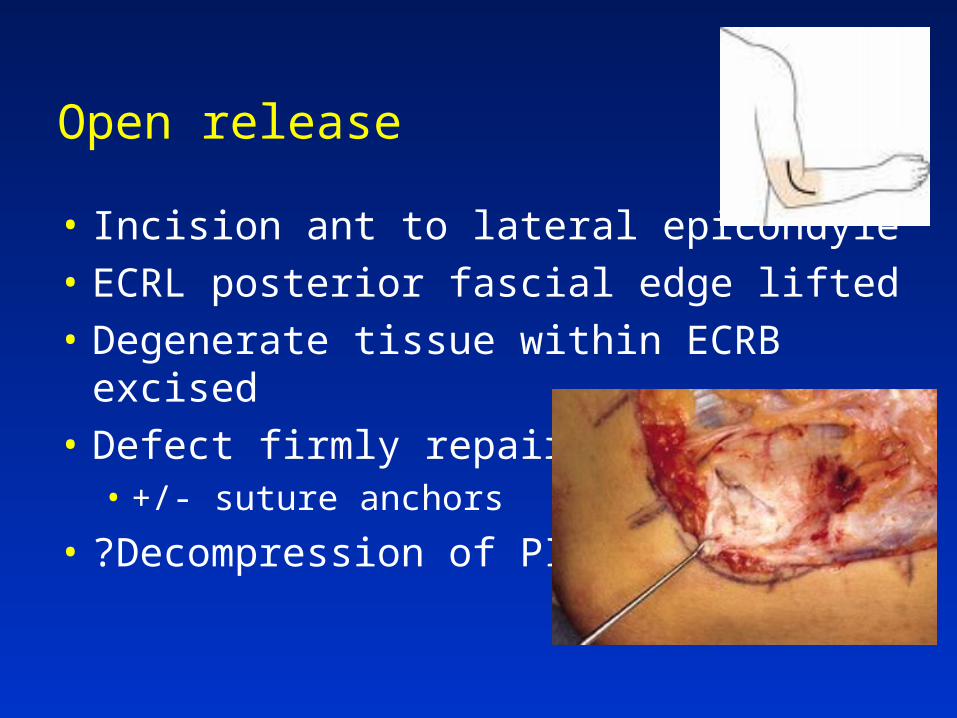
Open release
• Incision ant to lateral epicondyle
• ECRL posterior fascial edge lifted
• Degenerate tissue within ECRB excised
• Defect firmly repaired• +/- suture anchors
• ?Decompression of PIN
Open release
• Excellent / good 75 – 91% • Poor / failed 2 – 11%• 80 – 95% return to normal activity in 4/12
Lateral extensor release for tennis elbow. A prospective long-term follow-up study. Verhaar J et al. JBJS(Am) 1993;75(7):1034-43
The surgical treatment of chronic lateral humeral epicondylitis by common extensor release. Goldberg E et al. Clin Orthop 1998;Aug(233):208-12
Outcome of release of the lateral extensor muscle origin for epicondylitis. Svernlov B et al. Scand J Plast Recon Surg Hand 2006;40(3):161-5
Percutaneous release
• As good as open or arthroscopic• May have earlier return to work
Long-term follow-up of open and endoscopic Hohmann procedures for lateral epicondylitis. Rubenhaler F et al. Arthroscopy 2005;21(6):684-90
Surgical treatment of tennis elbow: percutaneous release of the common extensor origin. Kaleli T et al. Acta Orthop Belg 2004;70(2):131-3
Tendinosis of the extensor carpi radialis brevis: an evaluation of three methods of operative treatment. Szabo SJ et al. J Shoulder Elbow Surg 2006;15(6):721-7
Arthroscopy
• 70% satisfactory to excellent• 473 cases
• 4 deep infection• 33 prolonged drainage• 12 transient nerve palsies
Arthroscopic tennis elbow release. Kalainov D et al. Techniques in Hand and Upper Extremity Surgery. 2007;11(1):2-7
• Arthroscopy leaves residual tendinopathy• Gross and histological• Results in poorer outcomes
Lateral Epicondylitis: In Vivo Assessment of Arthroscopic Debridement and Correlation With Patient Outcomes. Cummins CA. Am J Sports Med Sep 2006, 34(9):1486
Summary
• Why bother?• Poor high level evidence• 95% settle without surgery
• Short-term: steroids +/- physio
• Long-term: ‘watch and wait’ as good as any
• Surgery only after failed non-operative Rx• high success rate• consider other diagnoses

Thank you