Embed Size (px)
Citation preview

Epidemiology and Risk Factors of Eating Disorders:A Two-Stage Epidemiologic Study in a Spanish
Population Aged 12–18 Years
Luis Rojo,1,2* Lorenzo Livianos,1,2 Llanos Conesa,3 Angeles Garcıa,4
Alberto Domınguez,5 Gloria Rodrigo,6 Lluis Sanjuan,7 and Marisa Vila2
1 Department of Medicine, University of Valencia, Valencia, Spain2 Eating Disorders Unit, Psychiatric Service, H.U. La Fe, Valencia, Spain
3 Psychiatric Service, Hospital de Sagunto, Valencia, Spain4 Medical Service of Public Health of Exmo, Ayuntamiento de Valencia, Valencia, Spain
5 Consellerıa de Sanidad, Valencia, Spain6 Eating Disorders Unit, Hospital General Universitario, Valencia, Spain
7 Departament d’Infermeria, University of Valencia, Valencia, Spain
Accepted 9 September 2002
Abstract: Objective: The authors studied the prevalence rates of eating disorders (ED) andtheir risk factors in a Spanish population aged 12–18 years. Method: A two-stage epide-miologic study was conducted in the province of Valencia. Educational centers, classrooms,and individuals were selected randomly. The initial sample comprised 544 subjects. DuringStage 1, subjects were screened with the 40-item Eating Attitude Test and a sociodemog-raphic questionnaire that evaluates risk factors. During Stage 2, a semistandardized clinicalinterview was conducted with each participant. A random control group was paired by class,age, and sex. Comorbid psychiatric disorders and partial and subclinical forms weredetected using criteria in the 4th ed. of the Diagnostic and Statistical Manual of MentalDisorders (DSM-IV). Results: Using DSM-IV criteria, the morbidity rate was 2.91%,women comprised 5.17% of the sample, men comprised 0.77% of the sample, and the sexratio was 6.71. Using DSM-IV criteria, including subclinical forms, the morbidity rate was5.56%, women comprised 10.3% of the sample, men comprised 1.07 % of the sample, and thesex ratio was 9.63. Six risk factors were isolated: psychiatric comorbidity, friend on a diet inthe last year, desire to lose weight, desire to be less corpulent, sentimental problems, and dietin the last year. Discussion: This is the first Spanish two-stage epidemiologic study to include acontrol group and to investigate risk factors. # 2003 by Wiley Periodicals, Inc. Int J Eat Disord34: 281–291, 2003.
Key words: epidemiology; eating disorders; risk factors; anorexia nervosa; bulimia nervosa
*Correspondence to: Dr. Luis Rojo, UTCA, Planta 11, Pabellon Maternal, Hospital Universitario La Fe, Avda deCampanar, 21, 46009-Valencia, Spain. E-mail: [email protected]
Grant sponsor: EVES (Escuela Valenciana de Estudios para la Salud), Consellerıa de Sanidad, GeneralitatValenciana; Grant number: 69/1998.
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/eat.10179
# 2003 by Wiley Periodicals, Inc.
INTRODUCTION
Eating disorders (EDs) have increased markedly in Western societies. In the last twodecades, their incidence and prevalence have increased to what some consider to be epi-demic proportions (Hsu, 1996; Livianos & Rojo-Moreno, 2001; Turnbull, Ward, Treasure,Jick, & Derby, 1996).
During the last few years, epidemiologic studies have become more methodologicallyrefined. Because of this, we now have relatively reliable morbidity rates and we have abetter understanding of the risk factors. In addition, we have to include the lesser orpartial forms of ED in epidemiologic studies, given the accumulated evidence that thereare a range of disorders occurring in a vulnerability continuum (Cotrufo, Barretta, &Monteleone, 1997; Dancyger & Garfinkel, 1995; Lewinsohn, Striegel-Moore, & Seeley,2000; Strober, Freeman, Lampert, Diamond, & Kaye, 2000).
Two epidemiologic studies on ED were recently published in Spain (Morande, Celada,& Casas, 1999; Perez-Gaspar et al., 2000). Both presented some methodologic shortcom-ings that warrant a new epidemiologic study. Neither of the two-stage studies includeda control group that scored below the screening instrument’s cutoff point, making itimpossible to make a formal assessment of the instrument. This is the most frequentmethodologic problem encountered in this type of study design (Fairnburn & Beglin,1990). Morande et al. (1999) used the Eating Disorder Inventory (EDI) as the screeninginstrument and admitted that the cutoff point was arbitrary. Furthermore, the populationused in the study consisted of 15-year-old subjects living in one urban area in the localityof Madrid, making it difficult to generalize the results. Social isolation was described asthe risk factor for ED.
The second epidemiologic (Perez-Gaspar et al., 2000) study used a large population of12–21-year-old individuals from the locality of Navarra and was conducted in educationalfacilities, selected after random sampling of localities, teaching centers, and classrooms.This was probably one of the most ambitious epidemiologic studies conducted with aSpanish population, but there were many shortcomings. First, there was no controlgroup. Second, more than 20% of the initially selected subjects dopped out (thisincludes the 13% of women with scores above the cutoff point who refused to takepart in the interviews). Third, the subpopulation of 16–21-year-old individuals was notrepresentative because education was not compulsory and the study did not includeindividuals who discontinued their studies. Fourth, the study did not provide data onrisk factors and it only used strict diagnostic criteria (which include nonspecific forms)as defined in the 4th ed. of the Diagnostic and Statistical Manual of Mental Disorders(DSM-IV; American Psychiatric Association [APA], 1994).
Because of the problems associated with these two studies, we conducted a new two-stage epidemiologic study in the 12–18-year-old segment of a Spanish population froma wide geographic area. Our objective was to investigate the prevalence of ED and theassociated risk factors. This study used separate data analysis of the cases diagnosed withDSM-IV criteria and cases that included subclinical forms (Cotrufo et al., 1997).
METHODS
The data were obtained in an epidemiologic study of the prevalence of ED and theincidence of associated risk factors. The study was conducted during the 1998–1999
282 Rojo et al.
academic year among 12–18-year-old individuals from a territorial demarcation (theprovince of Valencia) comprising 263 townships.
The geographic distribution of the census population included a town of more than100,000 inhabitants, three towns with 50,001–100,000 inhabitants, 63 localities with 5,001–50,000 inhabitants, and 196 townships with less than 5,000 inhabitants.
Census data for the province of Valencia listed a total of 251,187 youths between theages of 12 and 18 years old. There were 235,862 students in public and private educationcenters, comprising 94% of the census population. The remaining 6% or 15,325 youthswere between the ages of 14 and 18 years and had dropped out of the school system.Education was compulsory until the age of 16. The target population was divided intoseven groups by age and sex. Field work took place in two stages.
First Stage
The sample population was screened with the Spanish version of the 40-item EatingAttitude Test (EAT-40; Garner & Garfinkel, 1979; Castro, Toro, Salamero, & Guimera,1991) to detect the at-risk population. We selected the sample through conglomeratesextracted from a probability design proportional to size. A conglomerate sample pro-vides greater precision than a simple sample when conglomerates of low homogeneity(with respect to the variable studied) are obtained. Within each segment, we selecteda simple random sample. The random samples were then united to obtain the total desiredsample. The sampling was done with conglomerates. Because we were dealing with theschool system, we chose the classroom as the sampling unit.
During the first trimester of 1999, we surveyed the total sample population of 544 youths,selected in three stages: a random sampling of townships in each of the demographic-geographic areas; a random sampling of the teaching centers in each selected township;and stratification by the age and sex of each teaching center and random classroomselection. Ten pupils per classroom were interviewed.
In addition to the screening instrument, a sociodemographic poll was administered to thewhole sample in which we tested a range of variables covering the home, dietary practicesin the home and among friends, attitudes regarding weight and physical corpulence,and academic, social, and sentimental problems.
Second Stage
Interviews were conducted with the case group (individuals who scored 30 or higheron the EAT). The control group was selected randomly from the individuals who scoredlower than 30 on the EAT, using individual pairing stratified by age and sex to estimatethe prevalence of ED pathologies.
The interviews were conducted by psychiatrists well experienced in ED. The clinicalinterview was structured so as to yield sufficient information on the positive cases thatcould be used later to classify them using DSM-IV diagnostic criteria (APA, 1994). Thepsychiatrists filled out a questionnaire for each patient that reflected the presence orabsence of all DSM-IV diagnostic criteria for anorexia nervosa (AN) and bulimia nervosa(BN). This enabled us to recognize full syndromes (i.e., those that met all AN [307.1] orBN [307.51] criteria), eating disorder not otherwise specified (EDNOS [307.50]), partialsyndromes (i.e., those that met AN Criteria B and C, but not A or D; or those that met BNCriteria A1, B, D, and E, but not A2 or C), and the subclinical forms (i.e., those that metAN Criteria B and C, but neither A nor D; or those that met BN Criteria A1, B, D, and E,but neither A2 nor C; Cotrufo et al., 1997).
Risk Factors of Eating Disorders 283
Detection of Comorbid Psychiatric Pathologies
As an additional diagnostic measure of psychiatric pathologies, we also administeredthe Schedules for Clinical Assessment in Neuropsychiatry (SCAN; Unidad de Investiga-cion en Psiquiatrıa Social de Cantabria, 1993). The SCAN is a set of instruments designedto analyze, measure, and classify the psychopathology and behaviors associated with theprincipal adult psychiatric disorders. Our study sample was administered the generalmodule, after which the depression and anxiety modules were administered whennecessary. Diagnoses were established using the 10th ed. of the International Classifica-tion of Diseases (ICD-10; World Health Organization, 1992) criteria.
RESULTS
Sixty individuals (‘‘cases’’) scored above the EAT-40 cutoff point. The experimentalmortality rate was 3.6% (a 17-year-old boy and an 18-year-old girl refused to go to theinterview). We conducted 116 interviews, that is, 58 selected cases and 58 control cases,aimed at confirming or rejecting the diagnosis of ED.
Utilizing DSM-IV criteria, the diagnosis of an ED was confirmed in 15 cases: 1 case ofAN, 1 case of BN, and 13 cases of EDNOS. When using wide DSM-IV criteria (includingpartial and subclinical forms), the number of cases increased to 31: 2 full-syndrome cases(AN and BN), 7 partial AN cases, 2 partial BN cases, 17 subclinical AN cases, 2 cases ofcomplete binge eating disorder (BED), and 1 case of subclinical BED.
The morbidity of ED in the 12–18-year-old population in the province of Valencia wasanalyzed using the strict and wide DSM-IV diagnostic criteria.
Strict DSM-IV Diagnostic Criteria
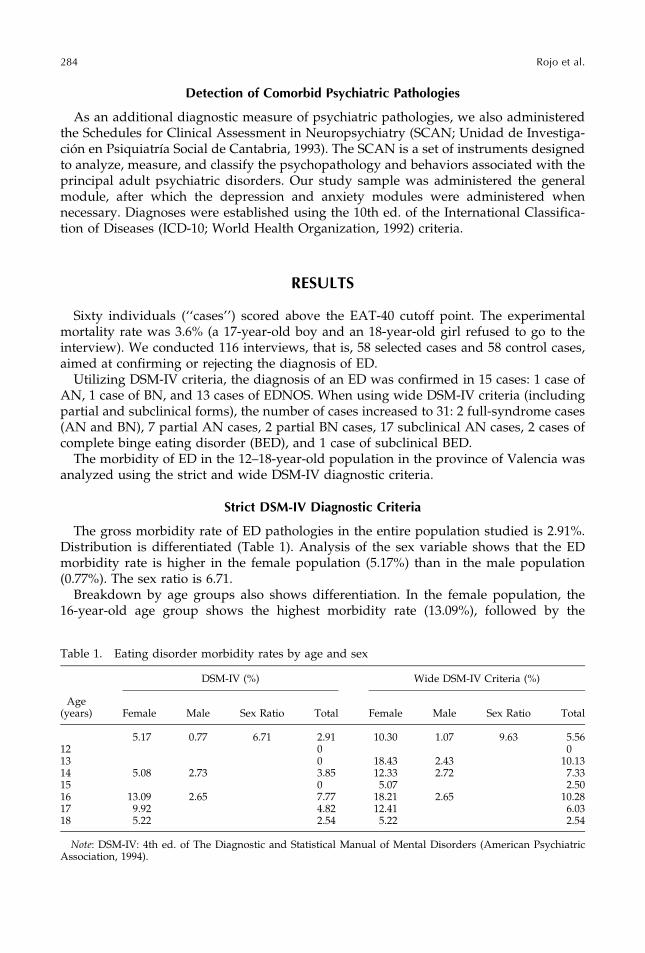
The gross morbidity rate of ED pathologies in the entire population studied is 2.91%.Distribution is differentiated (Table 1). Analysis of the sex variable shows that the EDmorbidity rate is higher in the female population (5.17%) than in the male population(0.77%). The sex ratio is 6.71.
Breakdown by age groups also shows differentiation. In the female population, the16-year-old age group shows the highest morbidity rate (13.09%), followed by the
Table 1. Eating disorder morbidity rates by age and sex
DSM-IV (%) Wide DSM-IV Criteria (%)
Age(years) Female Male Sex Ratio Total Female Male Sex Ratio Total
5.17 0.77 6.71 2.91 10.30 1.07 9.63 5.5612 0 013 0 18.43 2.43 10.1314 5.08 2.73 3.85 12.33 2.72 7.3315 0 5.07 2.5016 13.09 2.65 7.77 18.21 2.65 10.2817 9.92 4.82 12.41 6.0318 5.22 2.54 5.22 2.54
Note: DSM-IV: 4th ed. of The Diagnostic and Statistical Manual of Mental Disorders (American PsychiatricAssociation, 1994).
284 Rojo et al.

17-year-olds (9.92%), the 18-year-olds (5.22), and the 14-year-olds (5.08%). In the male popu-lation, the 14-year-old group has the highest rate (2.73%), followed by the 16-year-oldgroup (2.65%).
Wide DSM-IV Diagnostic Criteria
The gross morbidity rate of the nosologic entity ED in the entire population studies is5.56%, with a differentiated distribution (Table 1). Analysis of the sex variable shows thatthe female population presents a higher rate (10.30%) than the male population (1.07%).The sex ratio is 9.63.
Age-group analysis yields the following distribution. In the female population, thehighest morbidity rate occurs in the 13-year-old age group (18.43%), closely followed bythe 16-year-olds (18.21%), the 14-year-olds (12.33%), and the 17-year-olds (12.41%). Theprevalence is lowest in the 18-year-old (5.22%) and 15-year-old (5.07%) age groups. In themale population, the highest rate occurs in the 14-year-old age group (2.72%), followedby the 16-year-olds (2.65%) and 13-year-olds (2.43%).
Widening the diagnostic criteria almost doubles the prevalence of ED. The ratiobetween prevalence rates with wide/strict criteria is 1.91 for total prevalence, 1.99 forfemale prevalence, and 1.4 for male prevalence. Females account for the lion share of theincrease in the number of cases, as evidenced by the fact that the sex ratio is 6.71 whenusing strict criteria and 9.63 when subclinical forms are included. It is also noteworthythat the new cases emerge in the youngest groups.
Morbidity Distribution by Diagnostic Criteria
Strict DSM-IV CriteriaThe morbidity rate for AN among 12–18-year olds in the province of Valencia is 0.22%.
The prevalence rates among girls and boys are 0.45% and 0%, respectively. The morbidityrate for BN among 12–18-year-olds in the province of Valencia is 0.2%. The prevalencerates among girls and boys are 0.41% and 0%, respectively.
The morbidity rates in the province of Valencia are 2.69% for the entire populationaged 12–18 years old, 4.71 among girls, and 0.77 among boys. The sex ratio is 6.11.Analysis of age group and sex shows that the highest rate occurs among 16-year-oldgirls (13.04%), followed by 17-year-old girls (9.92%), 14-year-old girls (5.08%), and18-year-old girls (2.61%). Among boys, the morbidity rates are 2.72% and 2.61% among14-year-olds and 16-year-olds.
Wide DSM-IV CriteriaThe morbidity rate for partial AN among adolescents aged 12–18 years in the province
of Valencia is 1.34%. The prevalence rates among girls and boys are 2.33% and 0.40%,respectively. The sex ratio is 5.82. Analysis of the combined variables age group and sexshows that among girls, 16-year-olds have the highest rate (7.99%), followed by 17-year-olds (4.94%) and 14-year-olds (2.37%). Among boys, 16-year-olds have a mobidity rateof 2.65%.
The morbidity rate for subclinical AN is 3.09% for the entire population under study.Girls show a 5.22% rate and boys 1.07%. The sex ratio is 4.88. The distribution by agegroup and sex shows that 13-year-old girls have the highest rate (18.43%), followed by14-year-olds (7.92%), 15-year-olds (5.07%) and 16-year-olds (5.11%). Finally, 17-year-oldgirls have a prevalence rate of 2.49%. Boys show very similar rates: 2.77% among 14-year-olds, 2.65% among 16-year-olds, and 2.43% among 13-year-olds.
Risk Factors of Eating Disorders 285
In the province of Valencia, we only detected cases of partial and subclinical BN andfull, partial, and subclinical BED in the female population, with a rate of 1.98%. Break-down by age shows that the prevalence is highest among 17-year-olds (4.98%), followedby 14-year-olds (2.71%), 18-year-olds (2.61%), and 16-year-olds (2.44%).
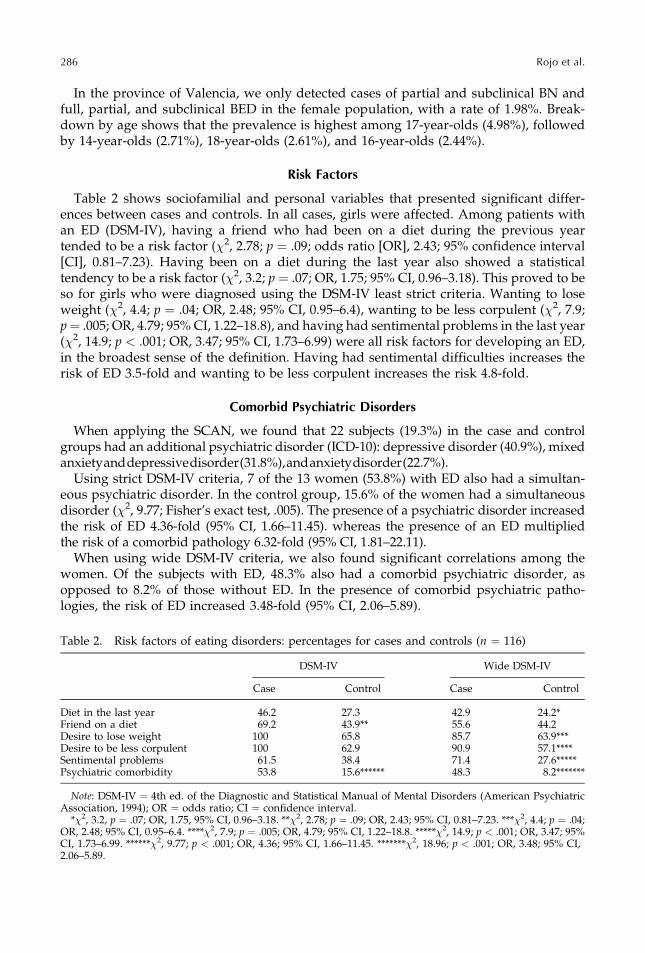
Risk Factors
Table 2 shows sociofamilial and personal variables that presented significant differ-ences between cases and controls. In all cases, girls were affected. Among patients withan ED (DSM-IV), having a friend who had been on a diet during the previous yeartended to be a risk factor (�2, 2.78; p ¼ .09; odds ratio [OR], 2.43; 95% confidence interval[CI], 0.81–7.23). Having been on a diet during the last year also showed a statisticaltendency to be a risk factor (�2, 3.2; p ¼ .07; OR, 1.75; 95% CI, 0.96–3.18). This proved to beso for girls who were diagnosed using the DSM-IV least strict criteria. Wanting to loseweight (�2, 4.4; p ¼ .04; OR, 2.48; 95% CI, 0.95–6.4), wanting to be less corpulent (�2, 7.9;p ¼ .005; OR, 4.79; 95% CI, 1.22–18.8), and having had sentimental problems in the last year(�2, 14.9; p < .001; OR, 3.47; 95% CI, 1.73–6.99) were all risk factors for developing an ED,in the broadest sense of the definition. Having had sentimental difficulties increases therisk of ED 3.5-fold and wanting to be less corpulent increases the risk 4.8-fold.
Comorbid Psychiatric Disorders
When applying the SCAN, we found that 22 subjects (19.3%) in the case and controlgroups had an additional psychiatric disorder (ICD-10): depressive disorder (40.9%), mixedanxietyanddepressivedisorder(31.8%),andanxietydisorder(22.7%).
Using strict DSM-IV criteria, 7 of the 13 women (53.8%) with ED also had a simultan-eous psychiatric disorder. In the control group, 15.6% of the women had a simultaneousdisorder (�2, 9.77; Fisher’s exact test, .005). The presence of a psychiatric disorder increasedthe risk of ED 4.36-fold (95% CI, 1.66–11.45). whereas the presence of an ED multipliedthe risk of a comorbid pathology 6.32-fold (95% CI, 1.81–22.11).
When using wide DSM-IV criteria, we also found significant correlations among thewomen. Of the subjects with ED, 48.3% also had a comorbid psychiatric disorder, asopposed to 8.2% of those without ED. In the presence of comorbid psychiatric patho-logies, the risk of ED increased 3.48-fold (95% CI, 2.06–5.89).
Table 2. Risk factors of eating disorders: percentages for cases and controls (n ¼ 116)
DSM-IV Wide DSM-IV
Case Control Case Control
Diet in the last year 46.2 27.3 42.9 24.2*Friend on a diet 69.2 43.9** 55.6 44.2Desire to lose weight 100 65.8 85.7 63.9***Desire to be less corpulent 100 62.9 90.9 57.1****Sentimental problems 61.5 38.4 71.4 27.6*****Psychiatric comorbidity 53.8 15.6****** 48.3 8.2*******
Note: DSM-IV ¼ 4th ed. of the Diagnostic and Statistical Manual of Mental Disorders (American PsychiatricAssociation, 1994); OR ¼ odds ratio; CI ¼ confidence interval.
*�2, 3.2, p ¼ .07; OR, 1.75, 95% CI, 0.96–3.18. **�2, 2.78; p ¼ .09; OR, 2.43; 95% CI, 0.81–7.23. ***�2, 4.4; p ¼ .04;OR, 2.48; 95% CI, 0.95–6.4. ****�2, 7.9; p ¼ .005; OR, 4.79; 95% CI, 1.22–18.8. *****�2, 14.9; p < .001; OR, 3.47; 95%CI, 1.73–6.99. ******�2, 9.77; p < .001; OR, 4.36; 95% CI, 1.66–11.45. *******�2, 18.96; p < .001; OR, 3.48; 95% CI,2.06–5.89.
286 Rojo et al.
DISCUSSION
The main difficulty associated with epidemiologic studies of ED, especially if riskfactors are also studied, is the low prevalence. If large samples are not used, the resultsshould be generalized with great caution (Patton, Johnson Sabine, Wood, Mann, &Wakeling, 1990). This should be remembered when interpreting our results. In the designof our study, we were careful to avoid the two methodologic problems that Fairburn andBeglin (1990) considered frequent in this type of research: obtaining a representativesample and assessing the screening instrument. We included a control group of indi-viduals who scored below the instrument’s cutoff point, were selected at random, and werepaired with the possible cases by age and sex. We also optimized the clinical identificationof the cases by having the partcipants interviewed by experienced psychiatrists who werefamiliar with the DSM-IV criteria. The diagnostic criteria were assessed in structuredinterviews in which, after a familiarization period and general evaluation of mentalcondition, all criteria were checked one by one to establish their applicability.
We believe that the current study provides some interesting novelties when compared withother studies using Spanish samples (Morande et al., 1999; Perez-Gaspar et al., 2000). First, ithas a control group of subjects scoring below the EAT’s cutoff point. Second, it assessespartial and subclinical ED. Third, it provides an in-depth investigation of risk factors.
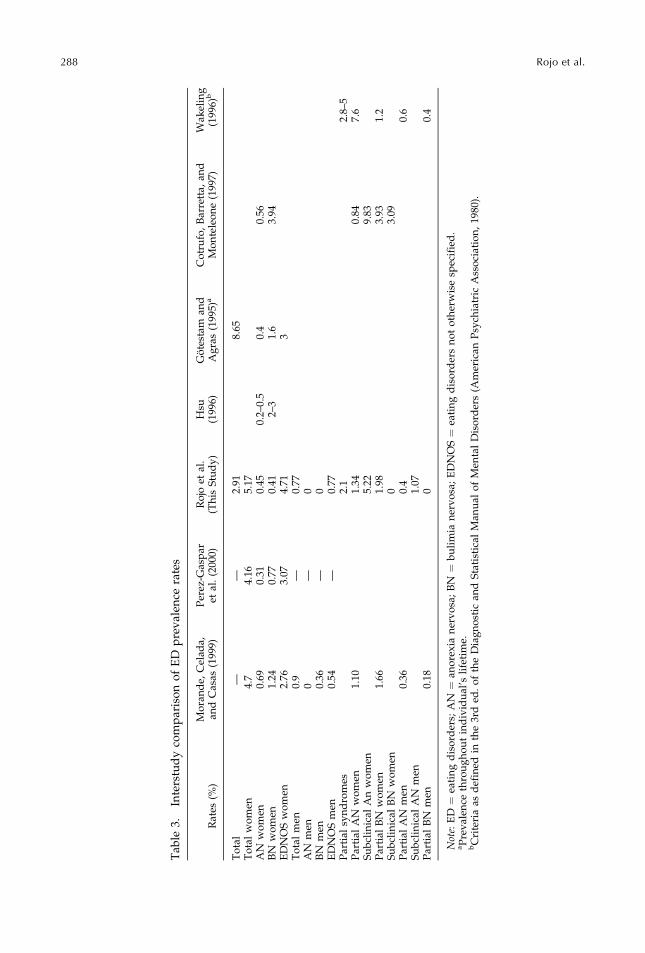
In our study, the total prevalence of ED among women (5.17%) is higher than in theother two studies (Table 3). This increase may have been caused by the inclusion ofEDNOS cases. The inclusion of a control group may also have contributed to the higherrates in our study because false negatives were more likely to be noncomplete forms of ED.
Morande et al. (1999) provided rates of partial forms of AN and BN. Their definition ofpartial AN and BN corresponded with the atypical forms of the ICD-10 (i.e., clinicalforms that are considered light or do not meet the amenorrhea and weight loss criteria ofAN, or in the case of BN, that lack one of the full syndrome’s principal characteristics). Inspite of these differences in definition, their prevalence rates are similar to ours (Table 3).Our BN prevalence rates are lower than those of the other studies and those described inthe literature in general (2–3%). This may in part be due to the age segment (12–18 years).The incidence of BN reaches its peak among individuals 20 years old and older (Turnbullet al., 1996). The maximum age of the sample used by Perez-Gaspar et al. (2000) was 21years, which might explain the higher incidence of BN. However, Morande et al. (1999)used a sample of 15-year-olds. We believe that the differences among the studies may beattributed to several conditions present in the study design characteristics. The sample inthe Morande et al. (1999) study consisted of volunteers, which may have facilitated theincorporation of individuals less likely to hide their symptoms. This is clearly a bias inthe selection of the sample and it may have contributed to the differences we found. Inaddition, the second stage of their study also included individuals who scored above 5 onthe Bulimia subscale of the EDI. This may have caused the higher detection rates of thesedisorders. The combination of these two factors may have favored the higher number offull BN cases in the results. In the Morande et al. study, the partial BN/full BN ratio was1.34, whereas the ratio in our study was 4.05 (i.e., for every full BN case there are fourpartial syndromes). Our result is closer to that of the 3.3 partial BN/full BN ratio found inthe Cotrufo et al. (1997) study.
Compared with other ED prevalence data (Table 3), our AN prevalence rate in women(0.45%) is on the high end of the range (0.2–0.5%) mentioned by Hsu (1996) in his reviewof 6 two-stage epidemiologic studies. Our study’s 4.71% prevalence rate of EDNOS
Risk Factors of Eating Disorders 287
Tab
le3.
Inte
rstu
dy
com
par
iso
no
fE
Dp
rev
alen
cera
tes
Rat
es(%
)M
ora
nd
e,C
elad
a,an
dC
asas
(199
9)P
erez
-Gas
par
etal
.(2
000)
Ro
joet
al.
(Th
isS
tud
y)
Hsu
(199
6)G
ote
stam
and
Ag
ras
(199
5)a
Co
tru
fo,
Bar
rett
a,an
dM
on
tele
on
e(1
997)
Wak
elin
g(1
996)
b
To
tal
——
2.91
8.65
To
tal
wo
men
4.7
4.16
5.17
AN
wo
men
0.69
0.31
0.45
0.2–
0.5
0.4
0.56
BN
wo
men
1.24
0.77
0.41
2–3
1.6
3.94
ED
NO
Sw
om
en2.
763.
074.
713
To
tal
men
0.9
—0.
77A
Nm
en0
—0
BN
men
0.36
—0
ED
NO
Sm
en0.
54—
0.77
Par
tial
syn
dro
mes
2.1
2.8–
5P
arti
alA
Nw
om
en1.
101.
340.
847.
6S
ub
clin
ical
An
wo
men
5.22
9.83
Par
tial
BN
wo
men
1.66
1.98
3.93
1.2
Su
bcl
inic
alB
Nw
om
en0
3.09
Par
tial
AN
men
0.36
0.4
0.6
Su
bcl
inic
alA
Nm
en1.
07P
arti
alB
Nm
en0.
180
0.4
Not
e:E
D¼
eati
ng
dis
ord
ers;
AN
¼an
ore
xia
ner
vo
sa;
BN
¼b
uli
mia
ner
vo
sa;
ED
NO
S¼
eati
ng
dis
ord
ers
no
to
ther
wis
esp
ecif
ied
.aP
rev
alen
ceth
rou
gh
ou
tin
div
idu
al’s
life
tim
e.bC
rite
ria
asd
efin
edin
the
3rd
ed.
of
the
Dia
gn
ost
ican
dS
tati
stic
alM
anu
alo
fM
enta
lD
iso
rder
s(A
mer
ican
Psy
chia
tric
Ass
oci
atio
n,
1980
).
288 Rojo et al.
among women is higher than that the 3% reported by Gotestam and Agras (1995).Wakeling (1996), in a review article, cited an approximate prevalence rate of 4–5% forpartial syndromes among young women. Our prevalence rate is in the same range.
The partial or incomplete forms of ED raise a crucial question in epidemiologic studies:How are cases defined? There is currently a strong debate regarding the criteria used todiagnose ED (Garfinkel et al., 1995, 1996). The basic problem is whether to consider theclinically less serious forms as ED in their own right. Although the issue has not beensettled definitively, the literature offers a wealth of data supporting the inclusion of theless serious forms in the range of ED. They share psychopathology (Dancyger & Garfinkel,1995; Patton & King, 1991), high rates of previous psychiatric treatment (Garfinkel et al.,1995; Lewinsohn et al., 2000), psychosocial characteristics (Kendler et al., 1991), andinheritability (Strober et al., 2000). In addition, they are the most prevalent forms in thegeneral female adolescent population (Wakeling, 1996). Therefore, they must be includedin epidemiologic studies. The problem is that they are not defined homogeneously.For example, Hoek et al. (1995) used the absence of amenorrhea to define an ED.Strober et al. ( 2000) considered the defining element of partial AN to be the absence ofweight loss. Conversely, they defined partial BN using the same criterion as Garfinkel et al.(1995), namely, the frequency of binge eating. Dancyger and Garfinkel (1995) definedpartial AN as the absence of weight loss and amenorrhea. Cotrufo et al.’s proposal(1997) looks very interesting to us because of its pragmatism. They part from the wellknown DSM-IV diagnostic criteria. Its application is easy (see methods). It allows to breakdown the clinical forms of AN, BN, and BED in a major number of clinical categories(full syndrome, partial, and subclinical forms) depending on their clinical gravity.
The diverse definitions in use make it very difficult to compare studies that providerates of partial syndromes. Table 3 presents the differences among studies. Our findingswould be comparable to those of Cotrufo et al. (1997). Prevalence rates show importantdifferences that reflect the differences in sample origin, sample age, and screeningmethod. Our prevalence rate of 5.22% for subclinical AN among women is similar to the5% prevalence rate of partial AN reported by Dancyger and Garfinkel (1995), althoughtheir definition of partial AN corresponded with our definition of subclinical AN.
Risk Factors
Our study identified six risk factors for ED. If out study had been limited to fullsyndromes and EDNOS, only the variables friend on a diet in the last year and psychia-tric comorbidity would have shown a significant tendency to be a risk factor. Its presencemultiplies the ED risk by 2.43 and 4.36-fold, respectively (Table 2).
Two of the remaining factors (desire to be less corpulent and desire to lose weight)could be considered part of the clinical criteria. However, we believe this should notbe so. In our overall sample of 272 women, 60.2% wanted to lose weight and 56% wantedto be less corpulent. Among men, we found discordant figures: 82.7% wanted to be morecorpulent and only 26% wanted to lose weight. These numbers demonstrate how wide-spread this phenomenon is among women. Table 2 shows the breakdown of thesevariables in the case and control groups. Although these variables are still present inthe case group and can be considered as symptoms, it must be remembered that the sameapplies to being on a diet, in spite of this being one of the most widely recognized riskfactors (King, 1989; Patton et al., 1990; Patton, Selzer, Coffey, Carlin, & Wolfe, 1999). Thisis why we consider desire to lose weight (which shows a statistical tendency to be a riskfactor) and desire to be less corpulent to be ED risk factors, in the widest diagnostic sense.
Risk Factors of Eating Disorders 289
Having been on a diet in the last year also showed a clear tendency to be an ED riskfactor in our study. It seems that diet is the variable, or at least an important variable, thatmediates the vulnerability effect of the factors related to body dissatisfaction. In thegeneral population we studied, 47% of women had been on a diet in the last year,compared with 20% for males. In the case group, 43% had been on a diet, compared with24% in the control group. Although the proportion is similar, the intensity of a diet isa key element for increased ED risk. Patton et al. (1999) found that an intense diet increasedthe ED risk 18-fold among adolescents, whereas a moderate diet increased the risk 5-fold.In addition, there is a strong relationship between body dissatisfaction and having beenon a diet in the last year. For example, when using DSM-IV diagnostic criteria, 100% ofindividuals who had been on a diet in the last year wanted to lose weight and to be lesscorpulent. When applying less strict criteria, this was still the case in 75% and 80% of thecases, respectively.
Another risk factor was the existence of sentimental problems in the last year. Itspresence increases the ED risk 3.5-fold (�2, 14.9; p < .001; OR, 3.47; 95% CI, 1.73–6.99).
An unexpected result is that, in spite of the high sex ratio, sex is not a risk factor. Thisresult can be explained by the size of the sample. However, Patton et al. (1999) believedthat sex is a secondary risk factor. Having been on a diet and psychiatric morbidity,which are more prevalent among females, would be the real variables predicting ED.
The inclusion of partial syndromes makes it possible to better recognize ED riskfactors. One of the major handicaps in studying risk factors is the low prevalence ofthese disorders. The inclusion of partial syndromes, which are highly similar to fullsyndromes in many variables, allows larger case samples to be used. This, in turn,improves the generalizability of the results. Dancyger and Garfinkel (1995) maintainedthat because of the dimensional nature of ED, there is a vulnerability continuum based onthe number of risk factors and not exclusively on the degree of diet.
Psychiatric comorbidity is a risk factor, both when using strict (the risk is increased4.36-fold) and wider diagnostic criteria (the risk is increased 3.48-fold). The psychiatricpathologies were almost exclusively depressive and/or anxiety disorders. Several otherstudies reached similar conclusions. Patton et al. (1999) conducted a prospective studyof first-time ED prediction factors. Their population comprised 2,032 adolescents aged14–15 years old who were selected randomly in secondary education centers in Victoria,Australia. They found that the presence of another psychiatric diagnosis is a risk factorfor the development of ED, independent of diet. When the factor having been on a dietwas taken into account, patients with another psychiatric diagnosis were six times morelikely to develop an ED for the first time. Similarly to our results, Kendler et al. (1991)found that was significant comorbidity between AN and BN, affective disorders (majordepression and dysthymia), anxiety disorders (separation anxiety disorder; no phobias orpanic disorder), and substance abuse (alcohol and other toxic substances).
Garfinkel et al. (1995) studied BN cases of community origin. They did not find anydifferences between the full and partial forms when associated with major depressivedisorder (the risk increased threefold) and anxiety disorder (the risk increased twofoldfor phobic anxiety disorder and social phobia). Only in full BN was there an increasedrisk of generalized anxiety disorder, agoraphobia, and panic disorder.
Finally, Lewinsohn et al. (2000) showed that psychiatric comorbidity does not occuramong adults exclusively (as our study also shows) nor is it a consequence of thechronicity of an ED.
Our study shows how many 12–18-year-olds in this Spanish sample are susceptibleto develop an ED and, by extension, how many individuals may require specific
290 Rojo et al.

support services. This information may serve as a valuable reference for health careplanning.
The authors thank Marıa Jose Abad, Emilia Chavez, and Marıa Jose Hernandez for their help.
REFERENCES
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.).Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.).Washington, DC: Author.
Castro, J., Toro, J., Salamero, M., & Guimera, E. (1991). The Eating Attitudes Test: Validation of the Spanishversion. Psychological Assessment, 7, 175–190.
Cotrufo, P., Barretta, V., & Monteleone, P. (1997). An epidemiological study on eating disorders in two highschools in Naples. European Psychiatry, 12, 342–344.
Dancyger, I.F., & Garfinkel, P.E. (1995). The relationship of partial syndrome eating disorders to anorexianervosa and bulimia nervosa. Psychological Medicine, 25, 1019–1025.
Fairnburn, C.G., & Beglin, S.J. (1990). Studies of the epidemiology of bulimia nervosa [Review]. AmericanJournal of Psychiatry, 147, 401–408.
Garfinkel, P.E., Lin, E., Goering, P., Spegg, C., Goldbloom, D., Kennedy, S., Kaplan, A.S., & Woodside, D.B.(1995). Bulimia nervosa in a Canadian community sample: Prevalence and comparison of subgroups.American Journal of Psychiatry, 152, 1052–1058.
Garfinkel, P.E., Lin, E., Goering, P., Spegg, C., Goldbloom, D., Kennedy, S., Kaplan, A.S., & Woodside, D.B.(1996). Should amenorrhoea be necessary for the diagnosis of anorexia nervosa? Evidence from a Canadiancommunity sample. British Journal of Psychiatry, 168, 500–506.
Garner, D.M., & Garfinkel, P.E. (1979). The Eating Attitude Test. Psychological Medicine, 9, 273–279.Gotestam, K.G., & Agras, W.S. (1995). General population-based study of eating disorders in Norway. Interna-
tional Journal of Eating Disorders, 18, 119–126.Hoek, H.W., Bartelds, A.I., Bosveld, J.J., van der Graaf, Y., Limpens, V.E., Maiwald, M., & Spaaij, C.J. (1995).
Impact of urbanization on detection rates of eating disorders. American Journal of Psychiatry, 152, 1272–1278.Hsu, L. (1996). Epidemiology of the eating disorders. The Psychiatric Clinics of North America, 19, 681–700.Kendler, K.S., MacLean, C., Neale, M., Kessler, R., Heath, A., & Eaves, L. (1991). The genetic epidemiology of
bulimia nervosa. American Journal of Psychiatry, 148, 1627–1637.King, M.B. (1989). Eating disorders in a general practice population. Prevalence, characteristics and follow-up at
12 to 18 months. Psychological Medicine, 14, 1–34.Lewinsohn, P.M., Striegel-Moore, R.H., & Seeley, J.R. (2000). Epidemiology and natural course of eating
disorders in young women from adolescence to young adulthood. Journal of the American Academy ofChild and Adolescent Psychiatry, 39, 1284–1292.
Livianos, L., & Rojo-Moreno, L. (2001). ¿Son realmente mas frecuentes los Trastornos de la Conducta Alimen-taria? [Is there a real increase of Eating Disorders?] Segundo Congreso Virtual de Psiquiatrıa. Interpsiquis2001. Disponible en: www.interpsiquis.com
Morande, G., Celada, J., & Casas, J.J. (1999). Prevalence of eating disorders in a Spanish school-age population.Journal of Adolescent Health, 24, 212–219.
Patton, G.C., Johnson Sabine, E., Wood, K., Mann, A.H., & Wakeling, A. (1990). Abnormal eating attitudes inLondon schoolgirls—a prospective epidemiological study: Outcome at twelve month follow-up. Psycho-logical Medicine, 20, 383–394.
Patton, G.C., & King, M.B. (1991). Epidemiological study of eating disorders: Time for a change of emphasis[Editorial]. Psychological Medicine, 21, 287–291.
Patton, C.G., Selzer, R., Coffey, C., Carlin, J.B., & Wolfe, R. (1999). Onset adolescent eating disorders: Populationbased cohort study over 3 years. British Medical Journal, 318, 765–768.
Perez-Gaspar, M., Gual, P., de Irala-Estevez, J., Martinez-Gonzalez, M.A., Lahortiga, F., & Cervera, S. (2000).Prevalencia de trastornos de la conducta alimentaria en las adolescentes navarras. [Prevalence of EatingDisorders among young women in Navarra, Spain] Medicina Clinica (Barcelona), 114, 481–486.
Strober, M., Freeman, R., Lampert, C., Diamond, J., & Kaye, W. (2000). Controlled family study of anorexianervosa and bulimia nervosa: Evidence of shared liability and transmission of partial syndromes. AmericanJournal of Psychiatry, 157, 393–401.
Turnbull, S., Ward, A., Treasure, J., Jick, H., & Derby, L. (1996). The demand for eating disorder care. Anepidemiological study using the general practice research database. British Journal of Psychiatry, 169, 705–712.
Unidad de Investigacion en Psiquiatrıa Social de Cantabria. (1993). Cuestionarios para la Evaluacion Clınica enNeuropsiquiatrıa. [Schedules for Clinical Assessment in Neuropsychiatry, SCAN] Madrid: Meditor.
Wakeling, A. (1996). Epidemiology of anorexia nervosa. Psychiatry Research, 62, 3–9.
Risk Factors of Eating Disorders 291





























