Embed Size (px)
Citation preview

POSTGRAD. MED. J. (1966), 42, 623.
THE EPIDEMIOLOGY AND CLINICAL FEATURESOF ASBESTOSIS AND RELATED DISEASES
P. C. ELMES, B.M., M.D., M.R.C.P.
Reader in Therapeutics and Pharmacology,
Institute of Clinical Science, The Queen's University of Belfast, Belfast 12.
DURING the last 100 years many materials have beenused by industry for a while and then found to haveunexpected harmful effects. Usually the risk ceaseswhen safety measures are adopted but sometimesthese measures are found to be inadequate and newones must be introduced. This has happenedrecently after the re-investigation of flax byssinosis(Carey, Elwood, McAulay, Merrett and Pemberton,1965).But with asbestos the situation is not so simple.
Following the report in 1930 (Merewether and Price)on the dangers of exposure to asbestos dust safetymeasures were adopted in factories and certainworkers kept under medical surveillance. Sincethen a series of other risks have been recognisedwhich indicate that the measures were eitherinadequate or did not cover a sufficiently widevariety of asbestos workers. Both cancer of thelung and mesothelioma are now recognised asresulting from levels of exposure to asbestos whichstill occur in spite of these measures.The summary of present knowledge about the
epidemiology of asbestosis and related diseaseswhich follows is necessarily brief and emphasisesthose points at which our knowledge is as yetincomplete.
The Nature and Uses of AsbestosThe word asbestos is used to cover a group of
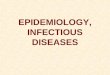
fibrous silicate minerals whose chief value is thatthey have a high melting point and are non-in-flammable. Therefore asbestos is used as strength-ening or insulation where high temperatures occur.But because it is relatively cheap and strong (thefibres are comparable in tensile strength to steel),and is resistant to many chemicals and to abrasion,asbestos has many other uses. These other usesaccount for the increased consumption of asbestosin an industrial city since 1940 (Fig. 1) (Elmes andWade, 1965). Asbestos cement is used to protect
the steel framework of modem buildings againstfire, to form pipes and ducts for water, air andchemicals and to form corrugated roofing. Asbestosis incorporated in brake pads and linings and inheavy duty flooring. Soft asbestos boarding andtiles are used to give heat and sound insulation toceilings and asbestos is sprayed on to the insides ofair conditioning ducts, roofs and pipes to preventcondensation. Asbestos is spun and woven to makefire protective clothing, oven cloths, wicks for oilstoves etc. It is even used in the filters of certaintypes of gas mask.Three types, chrysotile, crocidolite and amosite
make up the bulk of the asbestos used. Of theothers such as tremolite and actinolite onlyanthophyllite is of particular medical interest.Chrysotile is mined in the greatest quantity and ismineralogically separate from the others being apyroxene while the others are amphiboles (Table 1).They were all formed early in geological historyprobably about 2,000 million years ago. They wereproduced when the original rocks were subjected tohot water under pressure. As the rock formationcooled these compound silicates crystallised out infibrous form. The type of deposit and length offibres depended on the condition of the parentrock. Most chrysotile asbestos was formed incracks between shattered fragments of serpentine,a relatively hard rock. But the amphibole asbestoseswere deposited in the interstices of sedimentaryrocks such as banded ironstones. Harrington(1962) has demonstrated the presence of oils andwaxes which suggest that organic matter must havebeen present when the fibres formed. These may bethe cause of the fibrogenic and carcinogenic activityof asbestos.
Modes of ExposureMiningAsbestos is obtained from both open cast and
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

624 POSTGRADUATE MEDICAL JOURNAL October 1966
SHIPBUILDING and ASBESTOS IMPORTS.
Netgmt r Belfast. 1906-1960.Tor""g. -Tons.140.000 As6estos. 400
1900 10 20 30 40 50 60 70 1000
Boiler60.000 Cmoition - oo
20.000 / 00
1900 10 20 30 40 50 60 70Courtesy Belfast Harbour Commissioners.
FIG. 1-The dramatic increase in tonnage of asbestosimported to Belfast since 1940. (See Elmes &Wade, 1965).
TABLE 1
KINDS OF ASBESTOS IN COMMERCIAL USE
Percentage ofName Formula and Geological Name world production*
Chrysotile Mg3 (Si2 05) (OH) 4 93Chrysotile
Crocidolite Na2 Fe3+ + Fe2+++ (Si8 022) (OH,F)2 3.5"Blue" Riebeckite
Amosite (Mg, Fe+ +)7 (Si8 022) (OH)2 2.4Cummingtonite
Anthophyllite (Mg, Fe++ )7 (Si8 022) (OH, F)2 l.1*Anthophyllite
(always mixed with Gedrite)
*Estimated Total Production (1962) 3.2 million tons
**Including actinolite and tremolite
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

ELMES: Epidemiology of Asbestosis
deep mines. Drilling and explosives are used whenthe host rock is hard and mechanical excavationwhen it is softer. The crude ore is milled to removethe host rock and the fibrous asbestos is partiallyteazed out before it is packed into bags. Wherelabour is cheap some of the separation of rockfrom fibre is done by hand (cobbing) by womenoften accompanied by their babies. Until recentlylarge amounts of asbestos fibre escaped into the airfrom the mines and mills so that not only theminers and millers but the whole population of themining towns and the surrounding countryside havebeen exposed.
It was customary to transport asbestos from themines to the factories in jute bags. This exposureof a whole series of transport workers could beeliminated by using sealed impervious bags.Work in asbestos factories
It was here that the danger of exposure toasbestos dust was first recognised and investigated.The asbestos is teazed out again so that the fibresare separated and particles of rock etc., removed.The next process depends upon whether the fibreis to be woven into a textile or mixed with somebinding material for the fabrication of boards,pipes etc. The textile procedures are similar tothose used in the wool and cotton industries,carding being the dustiest. In the fabrication ofboard and cement products there was a considerablehazard when the product was cut and trimmed ormachined.No special effort was made to suppress dust in
these factories and the dust was everywhere inthem. Although all workers, even the clerks in theoffices, were exposed, some jobs were worse thanothers. Where forced ventilation was used thedusty air was often discharged unfiltered producinghigh levels of air pollution close to the factories.The protection of workers at certain scheduled
processes from asbestos dust became compulsoryunder the Government regulations which followedthe publication of the Merewether report(Merewether and Price, 1930). The workers alsocame under compulsory medical supervision andthere was an incentive for the relatives to ask for anautopsy when a death occurred. Cleaning up thevery dusty processes and filtering the effluent of theexhaust ventilation systems also reduced thegeneral air pollution of the factory and itsenvironment.
Although measurements of the dust concentrationswere started at this time they are technically difficult.They may not detect the smallest fibres, and thesemay be as harmful and be disseminated morewidely than the larger fibres.Use of asbestos goodsThe products of the asbestos factories are not
usually supplied direct to the public but are used inthe manufacture of factories, houses, power units,ships, cars, domestic stoves etc., by a variety ofskilled tradesmen with their helpers. These mensometimes use powdered material which they mixand apply on the spot or they use prefabricatedblocks, quilts etc., which require cutting, sawing orshaping to make them fit. The materials areusually rough-finished when they leave the factoryand release some dust when handled by storemenand transport workers. Insulation workers havebeen using asbestos goods in this way for a longtime. More recently building workers, interiordecorators and many others have started to usethem. Others (electricians, plumbers, fitters, paint-ers etc.) may work in the same confined space asinsulators and become exposed to the same dust ormay create dust cutting or drilling asbestos materialin the course of their own work.Most asbestos materials are coated with paint
or sandwiched between other materials so that theydo not present a continuing risk until the buildingor installation is demolished. But asbestos roofingand brake linings must cause some general atmos-pheric pollution and certain uses such as the liningof air condition ducts with soft asbestos and the useof unsealed ceiling tiles cause continuous pollutionof the air of office and factory buildings wherepeople work all day.A simple industrial history will not necessarily
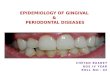
reveal exposure to asbestos when this has occurred.A careful description of the type of work and thematerials encountered at work will often help butthere remains the uppredictable exposures whichwill only be revealed by chance. A woman of 53(Fig. 2) was recently investigated following aspontaneous pneumothorax. She had been increas-ingly breathless and been under observation by theChest Clinic because of pulmonary fibrosis forseveral years. The findings were compatible withasbestosis but the patient denied occupationalexposure. A few days later she told the housephysician that she had helped her husband buildtwo asbestos bungalows in 1947 - 8. She had heldthe sheets while her husband sawed them up andthey lived in one of the bungalows for about twoyears before painting over the asbestos sheetslining the walls and ceilings. The husband was adeck-hand on a long-haul merchantman and alsohad no 'occupational' exposure to asbestos. X-raystaken when he was next in port revealed a similarextensive fibrosis although he was still able to work.Similar unexpected sources of exposure can berevealed by retrospective investigation of patientsdying of asbestosis or its complications. Newhouseand Thompson (1965) describe the wife whobrushed the asbestos dust off her husband's clotheswhen he came home in the evenings.
625October 1966
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

626 POSTGRADUATE MEDICAL JOURNAL October 1966
FIG. 2-Woman aged 53 who helped her husband buildtwo asbestos bungalows 18 years before. Herhusband shows similar changes. Diffuse fibrosiswith linear markings in the lower zones. Pleuralthickening with loss of clear demarcation ofdiaphragms. The scarring or 'large opacities' inthe middle and upper zones may representinactive tuberculosis.
The Diseases Related to Asbestos ExposureAsbestosisMany descriptions of asbestosis appeared in the
literature between 1924 and 1933. Descriptionssuch as those of Seiler (1928), Cooke (1927), Oliver(1927) and Wood (1928) refer to fibrosis resultingfrom a level of dust exposure far in excess of thoseexperienced now. There have been two changessince, the disease now comes on more slowly andthere has been a virtual disappearance of con-comitant tuberculosis. In Wyers' series (Wyers',1949) collected at an east London factory between
1931 and 1949 no less than 31 % had active tuber-culosis at necropsy compared with only 4 healedlesions found in 71 necropsies carried out between1957 and 1964 on cases from the same source(Table 2) (Smither, 1965).
This difference in exposure and absence ofcomplicating tuberculosis results in a more insidiousonset of symptoms which may start 20 or 30 yearsafter first exposure to asbestos and may evendevelop years after the exposure has ceased.
SymptomsThe first symptoms are breathlessness on exertion
and productive cough. The breathlessness isrelatively severe compared with the accompanyingcough and spit and is not associated with upperrespiratory infections or adverse weather conditions.But when 50 asbestos workers were carefullymatched with controls recently both severe coughand more than minimal sputum production weresignificantly more frequent.
Pain in the chest is emphasised in the earlyliterature, but our patients more often complain ofa 'tightness' than a pain. This is unrelated to effortand comes and goes unpredictably. Sometimes itmay be described as a pain by the younger and moreapprehensive asbestos worker who may show nodefinite evidence of asbestosis. Severe gnawingpain suggests the development of some complication.
Clubbing and warts: As in other conditions ofinsidious on,et associated with clubbing of thefingers only the occasional patient is aware of it.Clubbing does not seem to occur in the absence ofsignificant chest disese and is not invariably presentwhen the chest disease is severe. Warts are commonin people who handle asbestos and are liable to havecuts or abrasions of their hands. 42 per cent of agroup of 100 insulators had these at the time ofexamination and a further 26 had had them in the
TABLE 2
POST MORTEM FINDINGS IN ASBESTOS FACTORY WORKERS
(AFTER SMITHER 1965)
1931 - 49 1957 - 64
Number of cases 115 71Age at death 40.8 56Tuberculosis 36 4*Carcinoma of lung 17 26Primary pleural malignancy 1 2Primary peritoneal malignancy 0 13Other abdominal malignancy | 7 77
*lesions inactive
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

October 1966 ELMES: Epidemiology of Asbestosis 627
......... .:
.~~~~........:... .
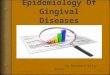
. *.. :. ::: :.*~~~~~~~~~~~~~~~~~~~~~~~~~~~~ .. ... .... ..FIG. 3-Pipe coverer (insulation worker) for 16 years;
died at 65 years of carcinoma of the stomach.No metastasis found in the lung at postmortem.Diffuse fibrosis with linear markings in themiddle and lower lobes. Loss of clear outlineof both diaphragms. The scarring in the rightupper zone was not tuberculous.
past. They start as a lump in the skin which becomeshyperkeratotic and a central white area appears. Ifthis centre is picked out with a pin the lesion willdisappear but otherwise it will persist for months oryears.
Physical signsThe main features of the more severe case are
cyanosis, restricted chest movement, kyphosis, finerales heard over the lung bases and clubbing of thefingers. In a group of 21 insulation workers (Table3) with definite asbestosis who were still at work,six were cyanosed, 7 showed clubbing of the fingersand 13 had basal rales. The signs became morefrequent and marked as the disease progresses and
: .:... .:....siZ
..... :.::.:::.:: :........ ... .... ...... .... ........
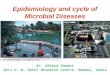
FIG. 4-Pipe coverer (insulation worker) for 26 years;died at the age of 71 years of cor pulmonale.In addition to the diffuse fibrosis there isextensive calcification of pleural plaques moremarked on the left than the right. There is somegeneralised pleural thickening and a loss ofclear demarcation of both diaphragms andpericardium.
when definite signs of right heart failure appear themen are unable to work and are unlikely to survivethe next acute respiratory illness. The rales andclubbing together present a pattern which it is easyto distinguish from chronic bronchitis. The raleshave a characteristic fine "dry" character which ispersistent in spite of deep breathing or coughing.They are often mistaken for a rub and are sodescribed in the earlier literature. These signs areof no value in distinguishing asbestosis from otherforms of chronic interstitial fibrosis with clubbingof the fingers. But with restriction of chest move-ment, kyphosis (loss of height) and cyanosis theyare useful in the detection and assessment ofasbestosis in workers on whom serial examinations
TABLE 3
SYMPTOMS AND SIGNS IN EARLY ASBESTOSIS IN 21 WORKING MENWITH DEFINITE RADIOLOGICAL CHANGES
Cough (other than 'in mornings only') 14Spit ('During the day' as well as 'in mornings') 10Breathlessness (M.R.C. grade 2 or more) 4Clubbing of the fingers.. .. .. .. .. .. .. .. .. .. .. .. .. .. 7Warts .. .. .. .. .. .. .. .. .. .. .. 16Cyanosis'rre .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. 6Basal 'dry' rales ...... . . . . . . . . . . . . . . 13
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

628 POSTGRADUATE MEDICAL JOURNAL October 1966
are carried out. For instance in this survey ofinsulation workers it was found that the 21 men withdefinite pulmonary fibrosis averaged 1 inchesshorter (making allowance for age) than those withno evidence of pulmonary fibrosis.
X-ray changesThe changes which result from exposure to
asbestos can occur with other forms of chronicdiffuse fibrosis involving the pleura. Localisedareas of damage resulting from tuberculosisor intercurrent infections give rise to an irregularscarring in the upper or midzone (Figs. 2 and 3).Linear markings in the periphery appear first in thelower zones. They run out into the pleura and withincreasing change join to produce a honeycomb orcystic appearance at the base. There is loss of theclear-cut margin between lung and pleura over thediaphragm and pericardium. By the time thisappearance has developed at the bases, linearmarkings are usually apparent over the whole lungand there are usually some localised scars ("lungopacities" as defined by the I.L.O. classification of1958). The early changes do not reproduce well butall the films (Figs. 2 - 6) show easily recognisablelinear shadowing with loss of the clear-cut line ofthe pleura.An adaption of the I.L.O. classification of X-ray
changes in pneumoconiosis to make it applicable toasbestosis is at present under discussion (U.I.C.C.Report, 1965). This will enable the findings ofdifferent groups to be compared.
Pleural thickening, as opposed to the loss ofclear demarcation between lung and pleura, cantake two forms. The first is a diffuse thickeningwith ill-defined margins which is most marked overthe lower lobes and is related in severity to theparenchymal change. The second is the formationof plaques which are circumscribed areas of hyalinefibrous tissue in the parietal pleura. On the dia-
phragm or pericardium they are rounded, but onthe chest wall they are guttate and lie along the lineof the ribs usually from the mid-axillary lineforward. They are not easy to see on X-ray untilthey begin to calcify. When calcified plaques havea characteristic appearance with clear cut marginsand a bilateral distribution (as in Fig. 4) they areprobably diagnostic of asbestos exposure. Theymay appear before the parenchymal changes andhave been used by Kiviluoto (1965) to plot theenvironmental area of asbestos exposure in Finland.In the Belfast series of dead asbestos workersthere were 13 with plaques out of the 87 for whomchest X-rays were available. In a survey of 100living pipe coverers of varying ages in the same areasix showed plaques and the only one under 40 yearsof age had been exposed in childhood.
Plaques are very common in and around theanthophyllite mining areas in Finland and inworkers in Eastern Germany using anthophylliteand other fibres. In South Africa they are seenboth in the blue asbestos and in the amosite miningareas (Sluis-Cremer, 1965). The incidence in thechrysotile mining areas of Quebec varies from mineto mine (Cartier, 1965). Although mesotheliomashave developed in patients with calcified plaquesthey are not necessarily associated. Mesotheliomasare unknown both in Finland, and in the amositeareas of South Africa where plaques are quitecommon (Table 4).
Laboratory testsNo test, short of lung biopsy, is diagnostic of
asbestosis, but some tests results support thediagnosis:-Sputum: The sputum is mucoid unless there is
complicating bronchial infection. There are nospecific cytological changes but malignant cells maybe found before there is other evidence of carcinoma.The sputum may contain both asbestos bodies and
TABLE 4
GEOGRAPHICAL RELATIONSHIP BETWEEN PLAQUES AND MESOTHELIOMAS
l ~~~~~~~~~~~FrequencyofArea Fibre Plaques Mesotheliomas
Finland Anthophyllite Common NoneE. Germany Anthophyllite and Common 6 since 1957
other fibresS. Africa Crocidolite Common CommonS. Africa Amosite Common NoneQuebec mines and l Chrysotile fSometimes rare Rarerelated textile mills 1 Sometimes common J
Insulation Workers:New York Mixed Common CommonBelfast Mixed Common Common
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

ELMES: Epidemiology of Asbestosis
fibres. These are not easy to see on direct examina-tion. If the sputum is first treated with "Eusol" orantiformin and the sediment examined by phasecontrast or with the substage condenser loweredasbestos bodies show up clearly (Gloyne, 1932).Polarised light may be needed to recognise theasbestos fibres. The presence of fibres only in-dicates current exposure and asbestos bodiesindicate exposure in the recent or distant past.Neither can be considered proof either that thepatient has asbestosis in the absence of definiteX-ray changes or that the pulmonary fibrosis seenon X-ray is due to exposure to asbestos.
Respiratory function tests: When applied togroups of asbestos workers compared with compar-able controls there are clear-cut differences. Theseresult from:
(i) Low total lung volume.(ii) Low vital capacity without evidence of
airways obstruction.(iii) Low pulmonary compliance.(iv) Low diffusing capacity (transfer factor).Williams and Hugh-Jones (1960) reported abnor-
malities in diffusing capacity for carbon dioxidebefore X-ray changes in factory workers. But inBelfast insulation workers the carbon monoxidediffusion test is less sensitive than X-rays in detectionof early evidence of asbestosis.There is a large range of normal for all these
tests and each may be made abnormal by a varietyof diseases. Therefore the tests are of little value inthe detection of early asbestosis in the individualcase unless serial readings over previous years areavailable (Bader, Bader, Tierstein and Selikoff,1965; Hunt, 1965). The extent of the diffusiondefect is the best estimate of disability.
The Complications of AsbestosisThe pattern of morbidity and mortality amongst
asbestos workers has changed as the conditions ofwork have improved. Just as children are no longerput into the sacks to stamp down the fibrousamosite in the mills in the South African mines(Schepers, 1965) so the machinery for cuttingasbestos board in the modern factory is automated,enclosed and subjected to exhaust ventilation.
In some factories where crippling pulmonaryfibrosis used to occur in less than 10 years, there arenow men who have worked continuously since 1933without any detectable evidence of pulmonaryfibro is. Heavily exposed workers were unable towork in the factories for long enough for the latecomplications of asbestos exposure to appear whilethey were still at work. But those who left the workafter a short period of exposure lived to developcarcinoma of the lung and mesothelioma of the
pleura. These cases have only recently been broughtto light by studies in which the fate of workers wholeft factories before 1933 are being traced (Newhouse,1966).The second factor which delayed the recognition
of the malignant complications was the longinterval between first exposure and the developmentof malignancy. The asbestos industry had startedon a small scale at the end of the last century andcontinued to employ small numbers of men andwomen until the first World War. A large popu-lation did not reach the length of exposure or agefor cancer until 1940 - 50.
Since 1931 all workers in the scheduled occupa-tions in Great Britain have been registered and keptunder medical supervision. Their deaths arereported to the coroner and a postmortem isusually carried out so from that time the cause ofdeath amongst workers who were already incertain jobs in the asbestos industry is fairly accurate-ly known. It was not until the figures for 1947 werepublished (H.M.S.O. 1949) that an undue incidence(13 %) of death due to cancer of the lung wasnoticed. Amongst the men there were no cases ofcancer of the lung under the age of 45 but abovethat age they amounted to 22 out of 76 with a peakincidence in the 55 - 64 age group. Detailed studieson one asbestos textile factory has confirmed thehigh incidence of cancer of the lung (Knox, Doll andHill, 1965) but indicate that only workers exposedto the heavy dust concentrations before 1933 wereat risk. Although workers taken on after that datein that factory appear to run no greater risk ofdeveloping cancer of the lung than other sections ofthe population, the national figures still show arising incidence. Nearly 50% of deaths in workerswith certified asbestosis in the 1961 - 3 period weredue to intrathoracic tumours (Buchanan, 1965).
Studies from another asbestos factory (Smither,1965) reveal a similar change in pattern (see Table2). Tuberculosis has been replaced by primarycarcinoma of the lung and by mesothelial tumoursof the pleura and peritoneum. In Dresden the causesof death for asbestos workers have been recordedseparately since 1952 (Jacob and Anspach, 1965).There were no cases of intrathoracic tumoursamong 18 deaths in the first year but in the nexttwo five-year periods the incidence was 19% and29% of 47 and 85 deaths respectively. One-fifth ofthese intrathoracic tumours were mesotheliomas ofthe pleura. The duration of exposure for thesecases varied between two and 42 years (average14.2 years) and the average latent period for allintrathoracic tumours was 30.7 years and formesothelioma was 31.8 years.The epidemiology and pathogenesis of these two
tumours, cancer of the lung and mesothelioma, is
October 1966 629
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

630 POSTGRADUATE MEDICAL JOURNAL October 1966
still under investigation in relation to asbestosexposure.
Cancer of the lungThis appears to occur in workers exposed to any
type of asbestos fibre but statistics are very frag-mentary. It has been observed in all mining areas,but little accurate information is available tocompare with the general population allowing forfactors such as smoking and atmospheric pollution.Finland is a country with a high rate for cancer ofthe lung anyway and in all countries the rapidlyrising incidence which has been attributed tocigarette smoking makes all such statistics difficultto interpret.The factory populations (Knox, Doll and Hill,
1965; Smither, 1965; Jacob and Anspach, 1965)already mentioned show an incidence of pulmonaryor pleural neoplasms of the order of 30% amongstmen exposed to dusty conditions which are notsufficiently severe to cause death due to pulmonaryfibrosis and respiratory failure in more than 20%.This risk of cancer of the lung amongst workersexposed to factory conditions before any effort atdust suppression has been estimated as 15 times thatexpected.The conditions under which insulators work have
only changed gradually over the years. Part of thischange has been due to the introduction of pre-fabricated materials which are easier and lessdusty to handle. More recently materials which donot contain asbestos have been used. Althoughmasks have been supplied for certain very dustyjobs such as limpet spraying no deliberate efforthas been made to reduce the dustiness of this typeof work.
In Belfast all insulators over 50 years of age and30 years of exposure so far examined show definiteevidence of pulmonary damage whereas only about30% of men between the ages of 30-40 or with10 - 19 years of exposure show such evidence.This suggests a degree of exposure less than thatwhich existed in some of the factories before 1933,but more than that described by Knox and others(1965) following that date. 107 deaths in insulatorsin Belfast since 1940 have been investigated so far.The causes of death are given in Table 5. There isa moderately high incidence of non-malignantrespiratory deaths but it is not far in excess of thatexpected as in the first half of the period tuberculosiswas still relatively common. It has not been easyto differentiate between deaths due to cancer of thelung and those due to pleural mesothelioma whereno autopsy material has been preserved. They havebeen classified together and are about five times theexpected.
There has been no definite change in pattern ofdeaths amongst insulation workers over the years(see Fig. 6) apart from the disappearance ofpulmonary tuberculosis. The age of death, pro-portion of cases with pulmonary fibrosis andproportion with cancer have all remained the samesuggesting a constant level of exposure at leastuntil 10- 15 years ago.Hammond, Selikoff and Churg (1965) have found
an incidence of intrathoracic tumours in insulationworkers seven times the expected and also a highrate of gastrointestinal neoplasms. The peakmortality due to lung cancer for men in all reportedseries of asbestos workers is between 55 and 60years of age and the only clinical difference betweenthese and other lung cancers is a higher proportion
TABLE 5
CAUSE OF DEATH IN INSULATION WORKERSBELFAST 1940- 65
TOTAL: 107 MEAN AGE: 55.3 ± 11.25 YEARS
Cause Observed Expected*
MALIGNANTIntrathoracic neoplasms 28 5.3Abdominal neoplasms 15 9.0Other neoplasms 4 6.7
NON-MALIGNANT :-Pulmonary disease 31 25.6Cardiac and circulatory 21 37.1Other causes 5 21.3Unknown 3
*This is a rough estimate based on the Registrar General's distribution of deaths in the age group 45 - 64 inthe year 1951 (H.M.S.O. 1953).
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

October 1966 ELMES: Epidemiology of Asbestosis 631
Distr i bution of Deaths by Year of Death.1940 1945 1950 1955 1960-44. -49. -54. -59. -64 .
40 s
nonMal inant
30~~~ ~ ~ ~~ 1 1 Z~~~~~~~~~~~abestos.30"' ~~~~~~~~~~~~~~~~~~~PuImon)ory
*~~~~ ~~~~~~~~~~~~~~~~~~~~i[brosis% | I ~~~~~~~~~~~~~~~~~~~~~contri butory.
U 20in . Malignant.
o00
0 d0
Mea)n Age. 507 54.8 53.4 57*1 57.1Mean Exposure 16 25 22*Z 272 264
(Years)
FIG. 5-The increasing number of deaths relating to successive five year periods may be due toincreasingly efficient case finding rather than a change in the death rate among insulation workers.
TABLE 6
MESOTHELIOMAS AND EXPOSURE TO ASBESTOSEXAMPLES OF RETROSPECTIVE STUDIES
Exposure
Source Total EnvironmentalDirect Casual or None
Domestic
LONDON Cases 76 31 0 9 36Newhouse & Thompson Controls 76 8 0 1 67
(1965)BELFAST Cases 42 8 24 0 10Elmes & Wade (1965) Controls 42 2 7 0 3
LIVERPOOL Cases 17 7 6 0 4Owen (1965) Controls 0
SOUTH AFRICAWagner, Sleggs & Cases 33 14 5 13 1Marchand (1960) Controls 0
TOTAL Cases 168 60 35 22 5136% 21% 13% 30%
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

632 POSTGRADUATE MEDICAL JOURNAL October 1966
... .............
... .. ...... .. _,
i.:..... :^.......... ...........8;S ,...-:,,::........... .. ... .j :S t''.*.'....'.'.'..,...' .'..:.'::''
.........~ ~ ... ...:~~~~~~~~~~.,",...'''',-................:
~~~~~~~~~~~~~~.'-,:::.'.''. ........ .....:i:- ..-.'' ..... ',... '.
..::.:...". ..:... :...:.'. - .-
.. -.,'..... ..........:.,:..- .. :.:::.... . : ..: '
~~~~~~~~~~~~~~~~~~~~~~~.:.,::... .:.'. ...... .:. ':'E...'
.: .. .. , ... : - .:- ! ,S .............................,.:~~~~~~~~~.. .. ..
~~~~~~~~:..':....:..;.............'.:
.''
.~~~~~~~~~....'....m::.........'.:
... ......,-',...'.:: '.z ',-
* .: .: . .. -: .. ... :.'.'-z.,_ l,''.~~~~~~~~~~~. ...
.~~~''.'.;....[...
*;,. ... '..
..... .. ... .... ...
~ ~~~ ~ ~~~~~~~......
* ~~~~~~~~~~~~~~~~~. .... .... .::.''
.... ..... .::::..::.:..,.:
..: .. .:.'.
.....
FIG. 6-Pipe coverer (insulation worker) for 26 years;died of a primary carcinoma of the lung aged 66years. Linear marking and small opacities inthe middle and lower zones. Loss of cleardemarcation of the diaphragm and pericardium.The peripheral tumour in the left upper lobe isindistinguishable radiologically from amesothelioma.
of lower lobe tumours (Jacob and Anspach, 1965).The symptoms, signs and X-ray changes of,
cancer of the lung are too well known to requiredescription here. Fig. 6 shows the chest film of aninsulation worker with both asbestosis and aprimary cancer of the lung. In all the cases ofproven primary carcinoma of the lung in the Belfastseries there was histological evidence of asbestosis,but this was not always obvious on X-ray.
MesotheliomaEpidemiology: This tumour has been the subject of
considerable research and comment since McCaughey(1958) described a series of cases in Belfast andWagner and others (1960) related an even largerseries to environmental exposure to blue asbestos.The histological evidence relating mesothelioma tothe inhalation or ingestion of asbestos is veryimpressive. When a history of exposure to asbestosis looked for in cases of mesothelioma it can usuallybe found (Table 6). But in only a third of cases isthis exposure of the sort of intensity that might
~.'-.. .." .. .".....; ''
~~~~~~~~-. j.. ...... '..- .' .. .. :.fcSf.'ci
....._<-............m~~~~~~~~lS..'.......,':....''"6tf~~~~~~~~~~~~~~~~:',.. ::: .., ... ........... _^,',~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ . . '.G . . . . . . . . .... ' :". S.:.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. ......... . .- 'r . . . .,-~~~~~~~~~~~~~~~~~~~~~ .f" .. ." .. .. .. .. .. .. ",~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ .':.' . : .+ . . . . . .-
.:~~ ~~~ ~ ~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.: :: .,::.-,'t,~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.' . . . ... .,.~ ~ ~ ~~ ~ ~~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.:,* ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. .... .. . .
*: ~ ~~~~~~~~~~~~~~~~ .: .. .-... ... .~ ~..
FIG. 7-Pipe coverer (insulation worker) for nearly 30years; died at 44 years of a mesothelioma of theleft pleura. The tumour is visible above thelevel of the left basal effusion. There is a partialcollapse of the right lower lobe. Pulmonaryfibrosis, though present, is not sufficient to showin the reproduction.
cause asbestosis or carcinoma of the lung. Inanother third of the cases there is an apparentlytrivial exposure at work or in the home environment.The environmental exposure ranged from playingon the slag heaps outside an asbestos mine up tothe age of seven years in a woman who died of amesothelioma at the age of 35 (Wagner, Sleggs andMarchand, 1960) to the woman who developed amesothelioma at 63 years and who used to washout her daughter's overalls when the latter workedin an asbestos factory (Newhouse and Thompson,1965). Casual exposure at work ranged fromoccasionally having to remove the remains oflagging from machinery which was being dismantledfor servicing, to the repairing of hessian bags someof which had been used for asbestos (Owen, 1965).The relatively large group (30%) with no history
of exposure can be accounted for in three ways:1. Occupational exposure which the patient had
forgotten or in which he was unaware of thenature of the materials handled.
2. Environmental or domestic exposure of whichthe patient was unaware.
3. No exposure at all.In (1) and (2) one would expect to find asbestos
bodies or fibres in the lungs. In a retrospectivestudy of 20 patients dying with asbestos bodies in
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

ELMES: Epidemiology of Asbestosis
the lungs the source of exposure was only found in14 (Elmes and Wade, 1965). This deficit couldaccount for all the mesotheliomas for whom nohistory of exposure is obtained. Nevertheless thereremains the possibility from epidemiological studiesthat a small proportion of mesotheliomas occur inpatients who have never been exposed to asbestos.
Because of the trivial exposures recorded in athird of the cases and the increasing and manifolduse to which asbestos has been put we can expect anincreasing number of mesotheliomas at least overthe next 40 years. (In the London series the intervalbetween first exposure and death varied between 29years for factory exposure and 48 years for environ-mental exposure. For the Belfast group as a wholethe interval was 43 years± 13).Numerous cases of mesothelioma have been
identified amongst people who have lived or workedin blue asbestos mining areas in South Africa(Table 4) and cases have been reported from thearea around the crocidolite mines in WesternAustralia. No cases have been reported fromaround the amosite mines in South Africa or theanthophyllite mines in Finland and only two casesfrom the Quebec chrysotiie mining area. Muchfactory work entails exposure to mixed dusts butso far the evidence from the factories indicatesthat frequency of mesotheliomas may vary with theextent to which blue asbestos is used. In insulationworkers it is usually impossible to identify theextent to which individual workers have beenexposed to individual types of asbestos. Theincidence of mesothelioma amongst these workersand amongst other workers exposed to the samematerials is relatively high.
Clinical features of mesothelioma: This tumouroccurs in either sex and people exposed duringchildhood may develop it earlier than those exposedduring adult life. The age of onset varies from 31years to 83 years and the mode for most series liesbetween 55 and 65 years. Other evidence of asbestosexposure (clubbing of the fingers, asbestos warts,pulmonary fibrosis and basal rales) is often absent.
Pleural casesMode of onset: This usually starts with gradually
increasing pain or breathlessness, taking severalweeks before the patient seeks medical advice.Because of this insidious onset the condition maybe found accidentally. One patient recently wasadmitted to hospital with a fall, another withsevere influenza and yet another was submitted toroutine chest X-rays as part of an occupationalsurvey. Only on direct questioning was the historyof pain or breathlessness elicited. The onset ofboth symptoms is sometimes so gradual that thepatient is unable to say which symptom startedfirst. The pain is described as a heavy feeling and
confined to the affected side of the chest at firstand then radiates to the shoulder and epigastrium.
It becomes more severe, a "dull toothache"little influenced by respiration on movement unlessthere is a secondary frozen shoulder.
In a few cases breathlessness comes on in amatter of hours or 2 - 3 days, and in these casesthere is usually a large pleural effusion which issometimes bloody. But even in these cases there isseldom much evidence on examination of a shift ofthe mediastinum to the opposite side. As thetumour extends around the lung there is restrictionof movement on that side with a shrinking down ofthe whole of that side of the chest and a pullingover the heart and mediastinum to the affected side.Tumour may become palpable in the supraclavicularfossa and between the ribs but seldom growsthrough the chest wall unless it is along the trackof a thoracentesis needle, through a thoracotomywound, at the site of a fractured rib or through anarea of chest wall damaged by deep X-ray therapy.X-ray appearances (see Fig. 7) are indistinguish-
able in most cases from a simple pleural effusionwith or without some degree of pulmonary fibrosis.The actual tumour may not be visible until the fluidis aspirated when it usually shows up as a lumpyarea in the pleura which also shows some degree ofthickening all round the lung. Rib destructionappears late and local lymph node enlargement israrely apparent on X-ray.
Diagnosis: This can often be made on clinicalgrounds after the exclusion of other causes ofpersistent pleural effusion in the middle-aged orelderly and the failure to find a distant primarymalignancy. It is difficult to verify the diagnosis.The fluid, when clear, is often unusually viscous,but frequently contains fresh or altered blood.Cytological examination of the fluid may revealcells strongly suggestive of mesothelioma but thediagnosis should not be based on this alone(Klempman, 1962; Naylor, 1963). The presence ofhyaluronic acid (Harrington, Wagner and Smith,1963) is also strongly suggestive but may occurwith other malignant lesions of the pleura. Thepresence of blood interferes with this test.
Especially in the absence of free fluid the diagnosiscan only be verified by biopsy, but there is avariation in the histological appearance in differentparts of a single tumour. There are often extensiveareas of fibrous tissue which are indistinguishablefrom chronic inflammatory disease. Thereforeneedle biopsy, and even limited surgical biopsy,may fail to provide the pathologist with sufficientmaterial to make the correct diagnosis. An openthoracotomy must be performed and pieces oftissue from different areas taken. To avoid tumourgrowing through the thoracotomy wound Thompson
October 1966 633
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
(1965) advocates the instillation of nitrogen mustardinto the pleural cavity at the end of procedure.
Treatment: Neither radical surgery nor radio-therapy can improve the prognosis and both mayencourage direct extension of the tumour throughthe chest wall. Palliative treatment should berestricted to removal of the pleural fluid to relievebreathlessness and instillation of nitrogen mustardinto the space if the accummulation of fluid israpid. Pain due to infiltration of the chest wall andvertebrae does not usually respond to radiation orsystemic cytotoxic drugs; it is usually too extensivefor treatment by regional nerve root section.
Course and prognosis: Patients seldom survivemore than a year from the time the diagnosis isestablished. The survival from onset of symptomsor from the earliest X-ray changes may be consider-ably longer but four years is probably the maximum.Apart from increasing pain and breathlessness thepatients usually remain in good health until invasionof the mediastinal tissue interferes with nutritionand they lose weight. Death is usually due torestriction of ventilation but intercurrent chestinfection may complicate the terminal illness.
Peritoneal casesThe onset is even more insidious than in the
pleural cases. The symptoms may mimic any formof abdominal neoplasm, presenting as upper orlower gastrointestinal tract obstruction with orwithout pain. Sometimes painless ascites is thepresenting feature. The diagnosis can usually onlybe established by laparotomy and adequate biopsybut occasionally cytology of the fluid may besufficient. Weight loss occurs earlier than in thepleural lesion but the interval between diagnosisand death is the same. No treatment is of any valueexcept that the rapid re-accumulation of asciticfluid can be checked by local nitrogen mustardtherapy.
Summary and ConclusionsPulmonary fibrosis due to exposure to asbestos
dust in factory workers has become uncommon andwhen it occurs is less severe than it was before theintroduction of dust suppression measures in1932 - 33. However there remain occupationswhich were not covered by the Merewether reportwhich can cause sufficiently severe fibrosis to leadto death before the retiring age. Insulation workersare a group in which this is likely to occur but thespreading use of asbestos in the building industrymay be leading to similar levels of exposure amongoccupational groups where this hazard has notexisted before.An increase in the number of such cases can only
be prevented by constant vigilance on the part of
the medical profession in identifying this as a causeof diffuse pulmonary fibrosis in individual cases andbringing them to the notice of the factory inspector-ate. One of the difficulties here is the lack of clinicalfeatures to distinguish asbestosis from other formsof diffuse fibrosis. When the source of exposure isnot obvious open biopsy of the lung may be necessaryto establish the cause and initiate investigation forsources of exposure.
Carcinoma of the lung resulting from exposureto asbestos appears to be common in patients whoseexposure to the dust was insufficiently long orintense to cause crippling fibrosis. There is evidencethat the risk may have been eliminated by theapplication of thorough dust suppression underfactory conditions. But there may be many otherworkers handling asbestos who are still at risk ashas been shown for insulation workers. The nature,age of onset and course of cancer of the lungsecondary to asbestos exposure does not appear todiffer greatly from cases arising in the generalpopulation.
A rapidly increasing number of cases of mesothe-lioma of the pleura and peritoneum have beenrecognised in the last 10 years. It is an invariablyfatal tumour for which there is no satisfactorypa'liative treatment. There is an associationbetween exposure to asbestos and the developmentof this tumour. The degree of exposure in manycases is slight and indicates that many people mayby now have had sufficient exposure either in thecourse of their work, hobbies or in the home. Asthere is no evidence of another factor operating inthe initiation of this tumour it seems likely thatincreasing numbers of cases will arise in the next30 years. Prevention of further cases beyond thatdate depends on the restriction of use and greaterprecautions in the handling of all types of asbestosfibre now. It is possible that the elimination ofone type of fibre (crocidolite) from commercial usemight reduce the incidence of the tumour veryconsiderably.
In writing this article I have drawn on informationwhich has become available as a result of research workdone in the Department of Therapeutics and Pharma-cology by Professor 0. L. Wade, Dr. Jean H. M.Langlands and Dr. W. F. M. Wallace as well as myselfsome of which has not yet been published. This workis part of a collaborative study of the problem of asbestosexposure organised by Dr. J. C. Gilson, Director of theM.R.C. Pneumoconiosis Research Unit at Cardiff. TheBiological Effects of Asbestos were discussed at anInternational Symposium held in New York under theauspices of the New York Academy of Sciences inOctober 1964. For convenience I have quoted referencesto the proceedings of this Symposium although much ofthe work has also been published elsewhere.
634 October 1966
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from

October 1966 ELMES: Epidemiology of Asbestosis 635
REFERENCESBADER, M. E., BADER, R. A., TIERSTEIN, A. S., andSELIKOFF, I. J. (1965): Pulmonary Function in Asbestosis.
Several Tests in a Long Term Prospective Study, Ann.N. Y. Acad. Sci., 132, 391.
BUCHANAN, W. D. (1965): Asbestosis and PrimaryIntrathoracic Neoplasms, Ann. N. Y. Acad. Sci., 132,507.
CAREY, G. C. R., ELWOOD, P. C., MCCAULAY, I. R.,MERRETT, J. D., and PEMBERTON, J. (1965): Byssinosis in
Flax Workers in Northern Ireland. Belfast: H.M.S.O.CARTIER, P. (1955): Some Clinical Observations of
Asbestosis in Mine and Mill Workers, A.M.A. Arch.Indust. Health, 11, 204.
CARTIER, P. (1965): Discussion on Pleural Plaques, Ann.N. Y. Acad. Sci., 132, 387.
COOKE, W. E. (1927): Pulmonary Asbestosis, Brit. med.J., ii, 1024.
ELMES, P. C., and WADE, 0. L. (1965): Relationshipbetween Exposure to Asbestos and Pleural Malignancyin Belfast, Ann. N. Y. Acad. Sci., 132, 549.
GLOYNE, S. R. (1932): The Asbestosis Body, Lancet, i,1351.
HAMMOND, E. C., SELIKOFF, 1. J., and CHURG, J. (1965):Neoplasia among Insulation Workers in the UnitedStates with Special Reference to IntraabdominalNeoplasia, Ann. N. Y. Acad. Sci., 132, 519.
HARRINGTON, J. S. (1962): Natural Occurrence of OilsContaining 3-4-benzpyrene and Related Substances inAsbestos, Nature (Lond.), 193, 43.
HARRINGTON, J. S., WAGNER, J. C., and SMITH, M.(1963): The Detection of Hyaluronic Acid in PleuralFluids of Cases with Diffuse Pleural Mesotheliomas,Brit. J. exp. Path., 44, 81.
HUNT, R. (1965): Routine Lung Function Studies on830 Employees in an Asbestos Processing Plant, Ann.N. Y. Acad. Sci., 132, 406.
H.M.S.O. (1949): Annual Report of the Chief Inspectorof Factories for the Year 1947, p. 79. London:H.M.S.O.
H.M.S.O. (1953): Thirtieth Annual Report of theRegistrar General for the Year 1951. Belfast:H.M.S.O.
JACOB, G., and ANSPACH, M. (1965): Pulmonary Neo-plasia among Dresden Asbestos Workers, Ann. N. Y.Acad. Sci., 132, 536.
KIvILUOTO, R. (1965): Pleural Plaques and Asbestos:Further Observation on Endemic and other Non-occupational Asbestosis, Ann. N.Y. Acad. Sci., 132,235.
KLEMPMAN, S. (1962): The Exfoliative Cytology ofDiffuse Pleural Mesothelioma, Cancer, 15, 691.
KNOX, J. F., DOLL, R. S., and HILL, I. D. (1965): CohortAnalysis of Changes in Incidence of BronchialCarcinoma in a Textile Factory, Ann. N. Y. Acad. Sci.,132, 526.
MCCAUGHEY, W. T. E. (1958): Primary Tumours of thePleura, J. Path. Bact., 76, 517.
MEREWETHER, E. R. A., PRICE, C. W. (1930): Effects ofAsbestos Dust on Lungs and Dust Suppression.London: H.M.S.O.
NAYLOR, B. (1963): The Exfoliative Cytology of DiffuseMalignant Mesothelioma, J. Path. Bact., 86, 293.
NEWHOUSE, M. L., and THOMPSON, H. (1965): Mesotheli-oma of the Pleura and Peritoneum following Exposureto Asbestos in the London Area, Brit. J. industr. Med.,22, 261.
NEWHOUSE, M. L. (1966): Personal Communication.OLIVER, SIR T. (1927): Clinical Aspects of Pulmonary
Asbestosis, Brit. med. J., ii, 1026.OWEN, W. G. (1965): Mesothelial Tumours and Ex-
posure to Asbestos Dust, Ann. N. Y. Acad. Sci., 132,674.
SEILER, H. E. (1928): A Case of Pneumoconiosis: theResult of Inhalation of Asbestos Dust, Brit. med. J.,ii, 982.
SCHEPERS, A. W. H. (1965): Discussion on 'HumanExposure to Asbestos: Community Studies,' Ann.N.Y. Acad. Sci., 132, 246.
SLUIS-CREMER, G. K. (1965): Asbestosis in South Africa- Certain Geographical and Environmental Con-'siderations, Ann. N. Y. Acad. Sci., 132, 215.
SMITHER, W. J. (1965): Secular Changes in Asbestosis inan Asbestos Factory, Ann. N.Y. Acad. Sci., 132, 166.
THOMPSON, V. C. (1965): Clinical Aspects of DiffuseMesothelial Tumours, Proc. Thor. Soc., Thorax, 20,286.
U.I.C.C. INTERNATIONAL UNION AGAINST CANCER (1965):Report and Recommendations of the Working Groupon Asbestos and Cancer, Ann. N. Y. Acad. Sci., 132,706.
WAGNER, J. C., SLEGGS, C. A., and MARCHAND, P.(1960): Diffuse Mesothelioma and Asbestos Exposurein the North West Cape Province, Brit. J. industr.Med., 17, 260.
WILLIAMS, R., and HUGH-JONES, P. (1960): LungFunction Changes in Asbestosis, Thorax, 15, 109.
WOOD, W. B. (1928): Pulmonary Asbestosis, Tubercle(Edinb)., 10, 353.
WYERS, H. (1949): Asbestosis, Postgrad. med. J., 25, 631.
by copyright. on M
arch 21, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.492.623 on 1 O
ctober 1966. Dow
nloaded from