Embed Size (px)
Citation preview

1
Epidemiology of Asthma and COPD in Chicago: Assessing the Presence of Disparities on a City- and Neighborhood-level
Helen Margellos-Anast Senior Epidemiologist
Sinai Urban Health Institute
December 4, 2013

Presenter Disclosures
(1) The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months:
Helen Margellos-Anast
No relationships to disclose

3
Outline
• Introduction
• Methods
• Results
• Discussion
• Limitations
• Conclusions

4
Sinai Urban Health Institute
• SUHI founded in March 2000 – Mission: To serve as a focal point for the evidence based
examination of community health status, the effectiveness of interventions and methods of improving health care delivery
– Particular focus on examining health disparities and contributing factors, and on identifying effective approaches that improve the health of urban communities
• All research and evaluation findings are publically disseminated to inform planning, advocacy, and public policy
www.SUHIChicago.org

Introduction
• Assessing and addressing health disparities is a national priority • Healthy People Goals
• Health disparities in Chicago are prevalent and little progress has been made since 1990 • Margellos H, Silva A, Whitman S. Comparison of Health Status
Indicators in Chicago: Are Black-White disparities worsening? American Journal of Public Health 2004.
• Orsi, JM. Margellos-Anast, H. Whitman, S. Black:White Health Disparities in the United States and Chicago: A 15-Year Progress Analysis. Am J Public Health. 2010 Feb; 100(2): 349-56.
5

Introduction
• Chronic Lower Respiratory Disease (CLRD), which includes both asthma and COPD, is the 3rd leading cause of death in the U.S.
• Significant attention has been devoted to asthma disparities on a national, city and local-level
• Less attention has been devoted to COPD • BRFSS 2011 COPD Module
• An assessment of local-level data that can inform a proper public health response might be viewed as imperative
6

Introduction - Asthma
• 1 in 12 people (8.3%) of people in the U.S. have asthma, which translates to nearly 25 million people
• Disparities are well documented on both a national and local level, with prevalence and associated morbidity being highest among Puerto Rican and non-Hispanic Black people, and in those living in poor, urban environments
• Prevalence in some Chicago communities far exceeds national prevalence
7
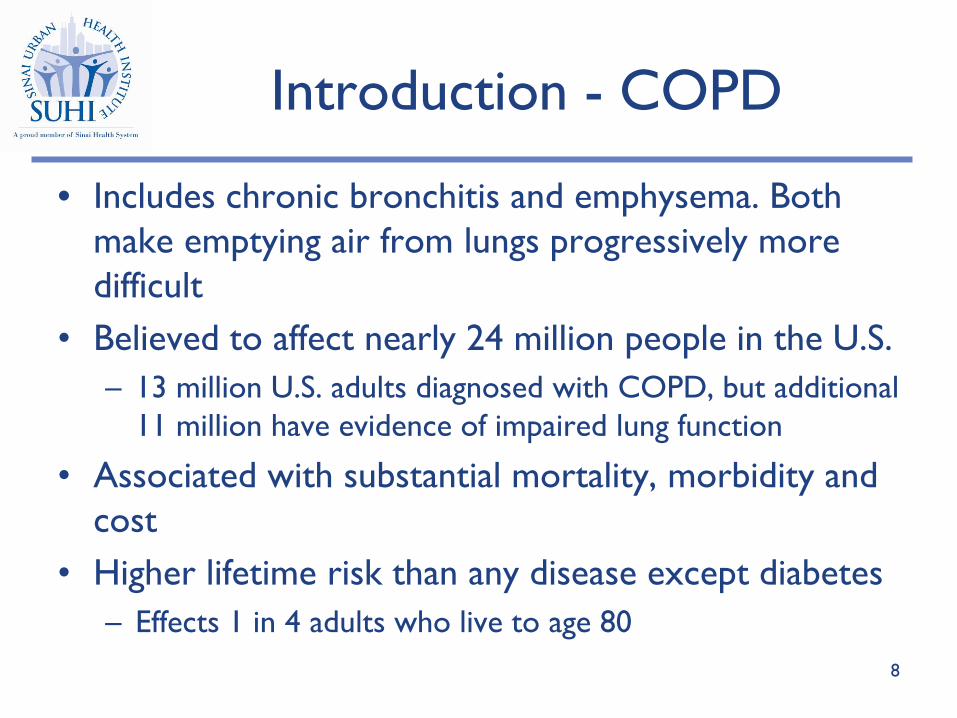
Introduction - COPD
• Includes chronic bronchitis and emphysema. Both make emptying air from lungs progressively more difficult
• Believed to affect nearly 24 million people in the U.S. – 13 million U.S. adults diagnosed with COPD, but additional
11 million have evidence of impaired lung function
• Associated with substantial mortality, morbidity and cost
• Higher lifetime risk than any disease except diabetes – Effects 1 in 4 adults who live to age 80
8

Introduction - COPD
• BRFSS 2011 revealed significant geographic variability suggesting the need for further surveillance to uncover reasons behind clustering
“Continued surveillance for COPD, particularly at state and local levels, is critical to 1) identify communities that likely will benefit most from
awareness and outreach campaigns and 2) evaluate the effectiveness of public health efforts related to the prevention, treatment, and control of the
disease.”1
• Current analysis response to this call for local level data
9
1 Chronic Obstructive Pulmonary Disease Among Adults – United States, 2011. MMWR Nov. 23, 2012; 61(46): 938-943.

10
Introduction
Current Analysis • Assesses the effects of CLRD, and its components COPD
and asthma on Chicago communities by analyzing mortality, hospitalization and Emergency Department (ED) rates on a city and neighborhood-level
• Considers disparities by race/ethnicity, gender, and geography – Current presentation is limited to non-Hispanic Black
(NHB) and non-Hispanic White (NHW)

Methods - 1
• 3-year age-adjusted mortality rates were examined for Chicago and by race/ethnicity and gender for the years 1999-2007
• 3-year age-adjusted inpatient and ED discharge rates were examined for Chicago and by race/ethnicity, gender, and zip code for the years 2008-2010
11

Methods - 2
Data Sources • Deaths were abstracted from vital records
maintained by the Illinois Department of Public Health
• Hospital discharge data were obtained from COMPdata (www.compdatainfo.com), a web-based database maintained by the Illinois Hospital Association and its affiliate, Association Management Resources
12

13
Methods - 3
• Statistical Analysis – Mortality, inpatient and ED data age-adjusted to 2000 US
population – Mortality rates calculated as deaths per 100,000
population – Inpatient and ED rates calculated as discharges per 10,000
populations

14
Methods - 4
• Statistical Analysis (cont.) – Rate Ratios (RRs) were computed and utilized to assess
the presence of disparities – 95% CI around RRs were calculated and utilized in
assessing statistical significance – Relationships between inpatient and ED rates and zip
code-level ecological variables were explored using bivariate correlation analysis
• Maps were generated displaying quartiles of zip code level inpatient and ED rates

Results
Mortality Rates
15
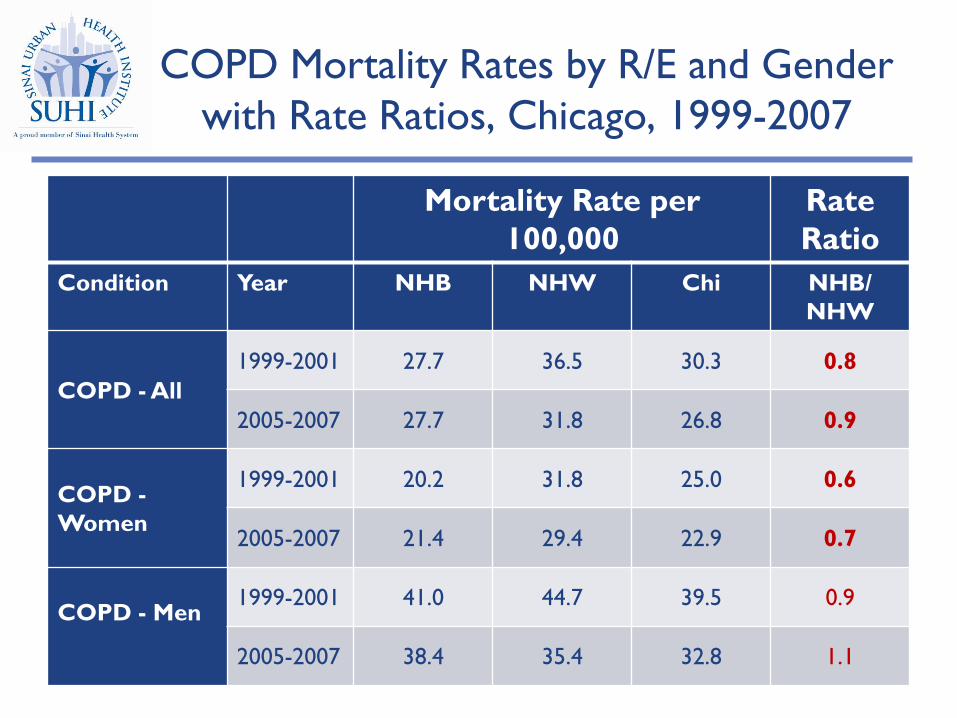
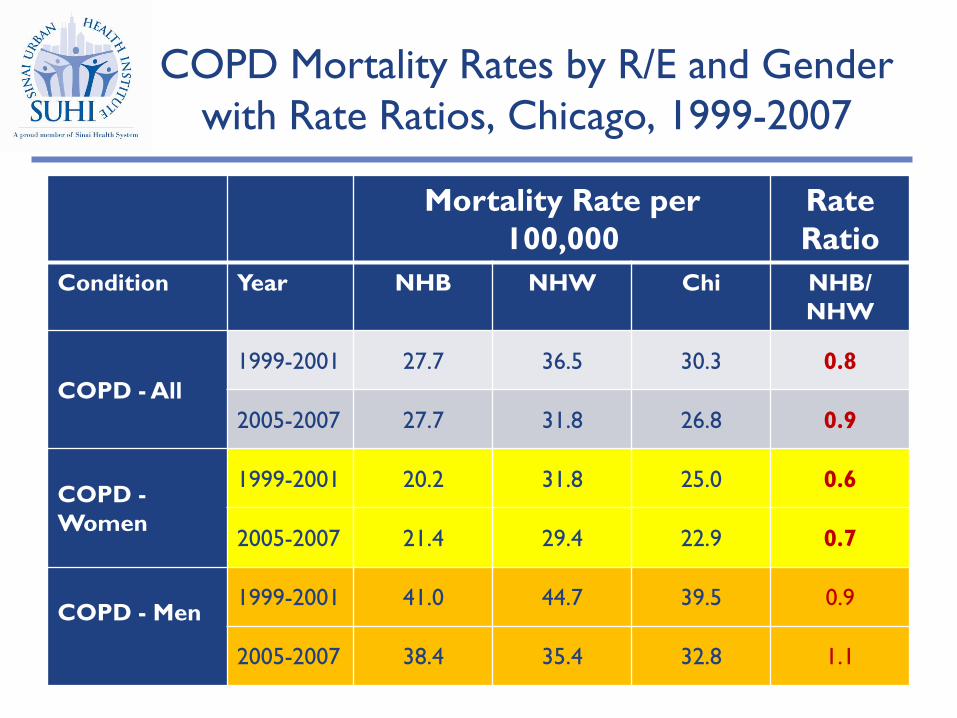
COPD Mortality Rates by R/E and Gender with Rate Ratios, Chicago, 1999-2007
16
Mortality Rate per 100,000
Rate Ratio
Condition Year NHB NHW Chi NHB/ NHW
COPD - All 1999-2001 27.7 36.5 30.3 0.8
2005-2007 27.7 31.8 26.8 0.9
COPD - Women
1999-2001 20.2 31.8 25.0 0.6
2005-2007 21.4 29.4 22.9 0.7
COPD - Men
1999-2001 41.0 44.7 39.5 0.9
2005-2007 38.4 35.4 32.8 1.1

COPD Mortality Rates by R/E and Gender with Rate Ratios, Chicago, 1999-2007
17
Mortality Rate per 100,000
Rate Ratio
Condition Year NHB NHW Chi NHB/ NHW
COPD - All 1999-2001 27.7 36.5 30.3 0.8
2005-2007 27.7 31.8 26.8 0.9
COPD - Women
1999-2001 20.2 31.8 25.0 0.6
2005-2007 21.4 29.4 22.9 0.7
COPD - Men
1999-2001 41.0 44.7 39.5 0.9
2005-2007 38.4 35.4 32.8 1.1
COPD Mortality Rates by R/E and Gender with Rate Ratios, Chicago, 1999-2007
18
Mortality Rate per 100,000
Rate Ratio
Condition Year NHB NHW Chi NHB/ NHW
COPD - All 1999-2001 27.7 36.5 30.3 0.8
2005-2007 27.7 31.8 26.8 0.9
COPD - Women
1999-2001 20.2 31.8 25.0 0.6
2005-2007 21.4 29.4 22.9 0.7
COPD - Men
1999-2001 41.0 44.7 39.5 0.9
2005-2007 38.4 35.4 32.8 1.1

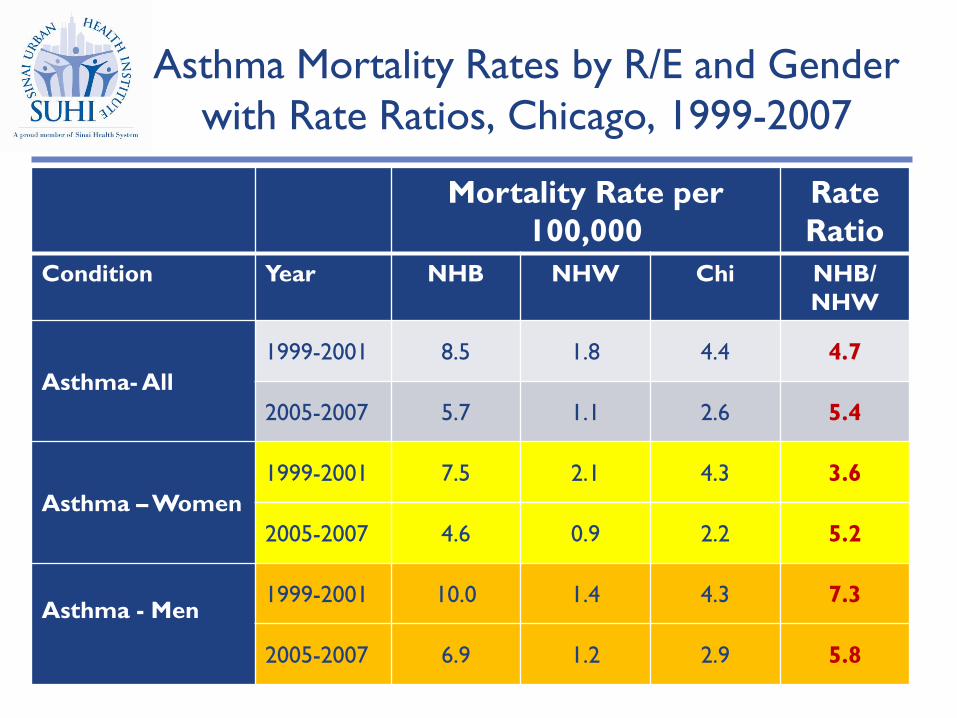
Asthma Mortality Rates by R/E and Gender with Rate Ratios, Chicago, 1999-2007
19
Mortality Rate per 100,000
Rate Ratio
Condition Year NHB NHW Chi NHB/ NHW
Asthma- All 1999-2001 8.5 1.8 4.4 4.7
2005-2007 5.7 1.1 2.6 5.4
Asthma – Women 1999-2001 7.5 2.1 4.3 3.6
2005-2007 4.6 0.9 2.2 5.2
Asthma - Men
1999-2001 10.0 1.4 4.3 7.3
2005-2007 6.9 1.2 2.9 5.8

Asthma Mortality Rates by R/E and Gender with Rate Ratios, Chicago, 1999-2007
20
Mortality Rate per 100,000
Rate Ratio
Condition Year NHB NHW Chi NHB/ NHW
Asthma- All 1999-2001 8.5 1.8 4.4 4.7
2005-2007 5.7 1.1 2.6 5.4
Asthma – Women 1999-2001 7.5 2.1 4.3 3.6
2005-2007 4.6 0.9 2.2 5.2
Asthma - Men
1999-2001 10.0 1.4 4.3 7.3
2005-2007 6.9 1.2 2.9 5.8
Asthma Mortality Rates by R/E and Gender with Rate Ratios, Chicago, 1999-2007
21
Mortality Rate per 100,000
Rate Ratio
Condition Year NHB NHW Chi NHB/ NHW
Asthma- All 1999-2001 8.5 1.8 4.4 4.7
2005-2007 5.7 1.1 2.6 5.4
Asthma – Women 1999-2001 7.5 2.1 4.3 3.6
2005-2007 4.6 0.9 2.2 5.2
Asthma - Men
1999-2001 10.0 1.4 4.3 7.3
2005-2007 6.9 1.2 2.9 5.8

Results
Inpatient and ED Rates
22

COPD Inpatient and ED Rates by R/E and Gender with Rate Ratios,
Chicago, 2008-2010
23
Discharge Rate per 10,000 Rate Ratio
Condition Type NHB NHW Chi NHB/ NHW
COPD - All
Inpatient 24.5 17.3 21.4 1.4
ED 37.3 12.5 22.4 3.0
COPD - Women
Inpatient 22.9 17.0 20.6 1.4
ED 39.5 13.7 24.5 2.9
COPD - Men
Inpatient 27.1 17.5 22.5 1.6
ED 35.1 11.3 20.2 3.1

COPD Inpatient and ED Rates by R/E and Gender with Rate Ratios,
Chicago, 2008-2010
24
Discharge Rate per 10,000 Rate Ratio
Condition Type NHB NHW Chi NHB/ NHW
COPD - All
Inpatient 24.5 17.3 21.4 1.4
ED 37.3 12.5 22.4 3.0
COPD - Women
Inpatient 22.9 17.0 20.6 1.4
ED 39.5 13.7 24.5 2.9
COPD - Men
Inpatient 27.1 17.5 22.5 1.6
ED 35.1 11.3 20.2 3.1

COPD Inpatient and ED Rates by R/E and Gender with Rate Ratios,
Chicago, 2008-2010
25
Discharge Rate per 10,000 Rate Ratio
Condition Type NHB NHW Chi NHB/ NHW
COPD - All
Inpatient 24.5 17.3 21.4 1.4
ED 37.3 12.5 22.4 3.0
COPD - Women
Inpatient 22.9 17.0 20.6 1.4
ED 39.5 13.7 24.5 2.9
COPD - Men
Inpatient 27.1 17.5 22.5 1.6
ED 35.1 11.3 20.2 3.1
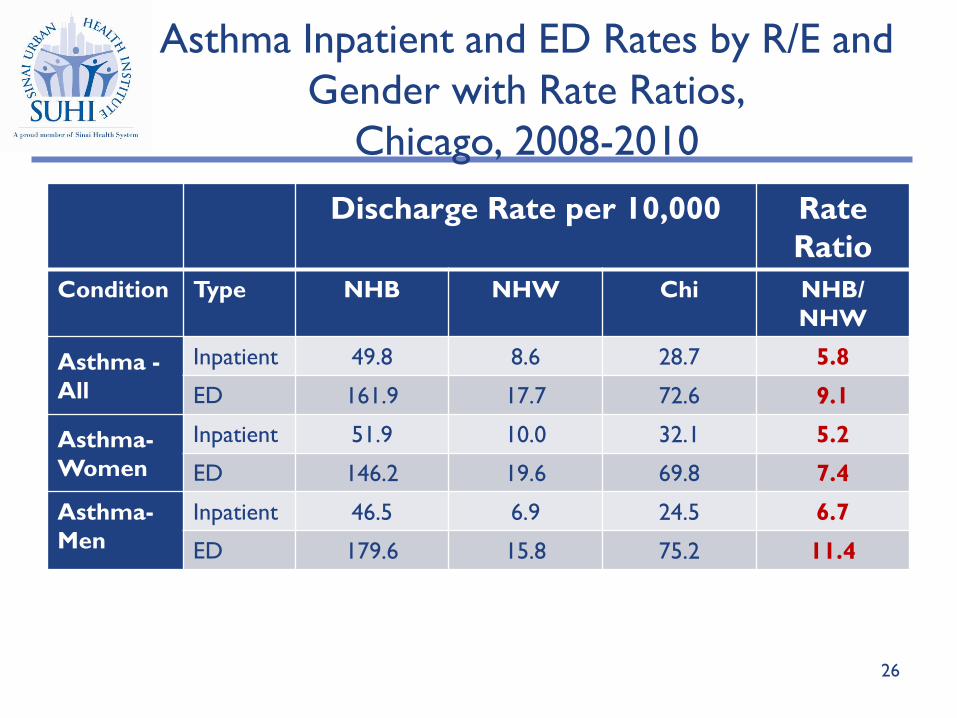
Asthma Inpatient and ED Rates by R/E and Gender with Rate Ratios,
Chicago, 2008-2010
26
Discharge Rate per 10,000 Rate Ratio
Condition Type NHB NHW Chi NHB/ NHW
Asthma - All
Inpatient 49.8 8.6 28.7 5.8
ED 161.9 17.7 72.6 9.1
Asthma- Women
Inpatient 51.9 10.0 32.1 5.2
ED 146.2 19.6 69.8 7.4
Asthma- Men
Inpatient 46.5 6.9 24.5 6.7
ED 179.6 15.8 75.2 11.4

Asthma Inpatient and ED Rates by R/E and Gender with Rate Ratios,
Chicago, 2008-2010
27
Discharge Rate per 10,000 Rate Ratio
Condition Type NHB NHW Chi NHB/ NHW
Asthma - All
Inpatient 49.8 8.6 28.7 5.8
ED 161.9 17.7 72.6 9.1
Asthma- Women
Inpatient 51.9 10.0 32.1 5.2
ED 146.2 19.6 69.8 7.4
Asthma- Men
Inpatient 46.5 6.9 24.5 6.7
ED 179.6 15.8 75.2 11.4

Asthma Inpatient and ED Rates by R/E and Gender with Rate Ratios,
Chicago, 2008-2010
28
Discharge Rate per 10,000 Rate Ratio
Condition Type NHB NHW Chi NHB/ NHW
Asthma - All
Inpatient 49.8 8.6 28.7 5.8
ED 161.9 17.7 72.6 9.1
Asthma- Women
Inpatient 51.9 10.0 32.1 5.2
ED 146.2 19.6 69.8 7.4
Asthma- Men
Inpatient 46.5 6.9 24.5 6.7
ED 179.6 15.8 75.2 11.4

Correlation of Inpatient Rates with R/E Distribution (%) and MHHI of Geographic
Area (zip code), Chicago, 2008-2010
Asthma Rate
COPD Rate
CLRD Rate
NHB (%)
NHW (%)
H (%)
MHHI ($)
Asthma Rate 1.0
COPD Rate 0.9 1.0
CLRD Rate --- --- 1.0
NHB (%) 0.7 0.7 0.7 1.0
NHW (%) -0.9 -0.8 -0.9 -0.8 1.0
Hispanic (%) -0.2 -0.2 -0.2 -0.5 0.1 1.0
MHHI ($) -0.8 -0.7 -0.8 -0.6 0.8 0.0 1.0
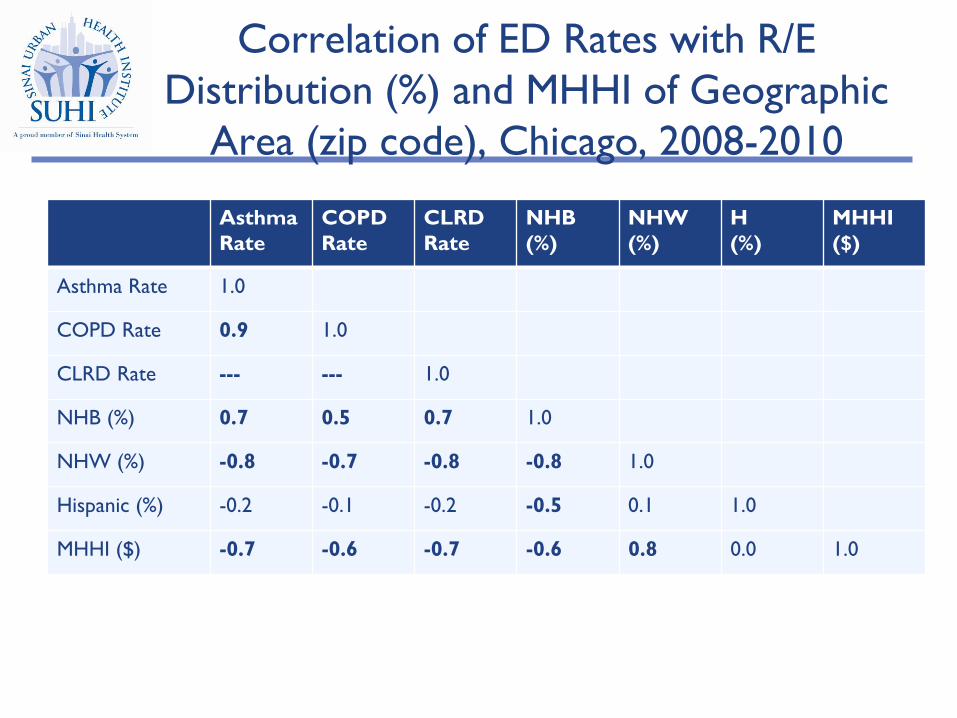
Correlation of ED Rates with R/E Distribution (%) and MHHI of Geographic
Area (zip code), Chicago, 2008-2010
Asthma Rate
COPD Rate
CLRD Rate
NHB (%)
NHW (%)
H (%)
MHHI ($)
Asthma Rate 1.0
COPD Rate 0.9 1.0
CLRD Rate --- --- 1.0
NHB (%) 0.7 0.5 0.7 1.0
NHW (%) -0.8 -0.7 -0.8 -0.8 1.0
Hispanic (%) -0.2 -0.1 -0.2 -0.5 0.1 1.0
MHHI ($) -0.7 -0.6 -0.7 -0.6 0.8 0.0 1.0

Zip Codes vs. Community Areas
• 77 officially recognized Chicago community areas – Comprised of census tracts – Census and mortality data available for community areas
• USPS lists 92 zip codes for Chicago, 52 of which included – Zip code and community area boundaries do not align – COMPdata available at zip code level
• Following correlation and geographic analysis will alternate between the two
31

Predominantly minority communities are concentrated on the west and south sides of Chicago • >75% NHB • >75% Hispanic/ Latino • >75% NHB/
Hispanic/Latino
32

Poorest communities are similarly concentrated on the west and south sides of Chicago • Quartiles of income • Darker colors
represent lower MHHI for community area
33

Communities with highest COPD inpatient rates are located on the west and south sides of Chicago • Quartiles of inpatient
rates • Darker colors
represent higher quartile (i.e., higher rates)
34

Communities with highest COPD ED rates are located on the west and south sides of Chicago • Quartiles of inpatient
rates • Darker colors
represent higher quartile (i.e., higher rates)
35

Communities with highest Asthma inpatient rates are located on the west and south sides of Chicago • Quartiles of inpatient
rates • Darker colors
represent higher quartile (i.e., higher rates)
36
Communities with highest Asthma ED rates are located on the west and south sides of Chicago • Quartiles of inpatient
rates • Darker colors
represent higher quartile (i.e., higher rates)
37

Summary of Key Findings - 1
• An examination of city and neighborhood area mortality and hospitalization data for Chicago reveals significant disparities for COPD and asthma, with NHB people and those living in poorer neighborhoods being the most affected
• The neighborhoods with the highest asthma and COPD inpatient and ED rates are concentrated on the west and south sides of the City, areas that are predominantly NHB and poor
38
Summary of Key Findings - 2
• NHB people have lower COPD mortality rates than NHW people
• Why?
• NHB people are significantly more likely to utilized urgent health services for COPD than are NHW people
• Access to care
39

Summary of Key Findings - 3
• Disparities in mortality and health resource utilization particularly pronounced for asthma
– NHB people were 5.4 times more likely to die of asthma than NHW people, with NHB men experiencing an even greater disparity
– NHB Chicagoans have an asthma ED rate that is 9 times higher that it is for NHW people
40

Summary of Key Findings - 4
• The correlation analysis corroborates the other evidence presented:
– strong, positive and statistically significant correlation between COPD, asthma and CLRD inpatient and ED rates and the proportion of a zip code that is NHB
– strong, negative and statistically significant relationship between COPD, asthma and CLRD inpatient and ED and the proportion of a zip code that is NHW
41

Discussion - Asthma
• Asthma disparities have been well documented on both a national and local level, with studies consistently documenting elevated prevalence and morbidity in PR and NHB people, and in those living below Federal poverty level
• Our findings corroborate prior evidence and reinforce the need for targeted intervention to address asthma
42

Discussion - Asthma
• Asthma mortality disparities have been documented nationally, with NHB people being 3 times as likely to die as NHW people1
• Chicago-level disparities revealed by our analysis much higher – NHB people 5.4 times more likely to die of asthma than
NHW people – Even more dramatic for NHB men
43 1Centers for Disease Control and Prevention. National Center for Health Statistics. National Vital Statistics Reports. Deaths: Final Data for 2006. April 17, 2009. Vol. 57, No. 14.

U.S. vs. Chicago Asthma Mortality Rates per
100,000 by Race and Gender, 2005-2007
• Mortality rates for NHW
Chicagoans similar to what they are nationally, whereas mortality rates for NHB Chicagoans are considerably higher
• NHB people in Chicago may have more poorly controlled asthma than NHB people nationally, leading to mortality disparities
1.1 0.9 0.7 1.2
2.9
4.6
2.6
6.9
0
1
2
3
4
5
6
7
8
U.S. Chicago
NHW Women NHW MenNHB Women NHB Men
44

Discussion - Asthma
• Chicago’s overall inpatient rate is nearly twice as high as that of the U.S. – 28.7 per 10,000 vs. 14.0 per 10,000
• Disparities in Chicago inpatient and ED rates between NHB and NHW people are substantial – NHB people over 9 times more likely to visit an ED – NHB people nearly 6 times more likely to be hospitalized
45

Discussion – COPD
• Data regarding COPD disparities not as prevalent, particularly on a local level – BRFSS 2011 COPD module - a major step in better
monitoring of COPD on a national and state level • 6.0% or 15 million U.S. adults have been diagnosed with COPD,
with highest rates nationally being among the following: – < high school education (9.5%) – Unemployed (7.8%) – Lowest levels of income (9.9% among HHI <$25K)
46

Discussion - COPD
• National data suggests that sex-specific COPD mortality rates from 1999-2008 highest among NHW people
• Our analysis of Chicago data revealed similar mortality advantage for NHB women, but not for NHB men
• Furthermore, whereas NHW Chicago mortality rates lower than they are nationally, NHB Chicago mortality rates are similar or slightly higher
47

U.S. vs. Chicago COPD Mortality Rates per 100,000 by Race and Gender, 2005-2007
• Mortality rates for NHW
Chicagoans lower than they are nationally, whereas mortality rates for NHB Chicagoans are higher than national rates
• Evidence that NHB people in Chicago die more frequently from COPD than do NHB people nationally
39.1
29.4
50.5
35.4
18.9 21.4
37.3 38.4
0
10
20
30
40
50
60
U.S. Chicago
NHW Women NHW MenNHB Women NHB Men
48
Discussion - COPD
• Chicago’s overall COPD inpatient rate (21.4 per 10,000) is nearly identical to rate nationally (21.1 per 10,000)
• NHB Chicagoans have COPD inpatient rate that is 1.4 time higher than it is for NHW people
• NHB Chicagoans have COPD ED rate that is nearly 3 times higher than it is for NHW people
49

Discussion - What Contributes to COPD Disparities?
• History of childhood asthma/ poorly controlled asthma – Asthma and COPD overlap
• Smoking • Air Quality • Access to Care • Early life and prenatal exposures
50

Limitations - 1
• Unable to examine impact of COPD and asthma overlap
• Miscoding – Race/ethnicity – Cause of death
• Use of underlying cause of death only • Use of primary diagnosis only
51

Limitations - 2
• Hospitalization rates refer to number of discharges, not to number of unique patients
• Aspects of this study are ecological, with the well known limitations
52

53
Conclusion • An examination of city and neighborhood level data for
Chicago reveals significant disparities for asthma and COPD, with NHB people and those living in poorer neighborhoods being the most affected
• Examinations of national data can mask the presence of disparities and local-level variation
• Small-level analyses are vital in engaging local communities and in formulating a culturally appropriate response
• Work described will have no merit unless it results in additional efforts to understand the identified disparities and to develop and test solutions towards addressing them

54
Acknowledgements
• SUHI Colleagues: Melissa Gutierrez Kapheim, Jana Hirschtick, Bijou Hunt, Steve Whitman
• Funders: Michael Reese Health Trust, Roe Health Policy Fund
• Rosalind Franklin University of Medicine and Science: Hyeon-Jeong Cho
• Data Sources: Chicago Department of Public Health, Illinois Department of Public Health, Illinois Hospital Association