Embed Size (px)
Citation preview

Epidemiology of Chronic Myeloid Leukemia
Tom Radivoyevitch, PhDAssistant Professor
Epidemiology and BiostatisticsCase Western Reserve University

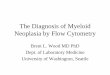
Two CML-ogens: Radiation and Age
𝑦=𝐴𝑒𝑘∗𝑎𝑔𝑒
Not exponential => use additive risk model
Sv = gamma ray dose (Gy) + 10 neutron dose (Gy)
0 20 40 60 80
Age
1
10
102
Ca
ses
pe
r 10
6 P
ers
on
-Ye
ars
U.S. CML Incidence 1973-2009
Males k = 0.047Females k = 0.046
11
1
10 20 30 40 50 60 70
Age
2
2
2 2
3
3
3
3
10
102
103
Ca
ses
pe
r 10
6 P
ers
on
-Ye
ars
Japanese A-Bomb Survivors
D < 0.02 Sv0.02 < D < 1 SvD > 1 Sv

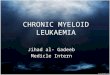
Radiation-induced CML is Multi-scale
Figure by R.K. Sachs.
For a 500 keV incoming photon
J = 6.2e18eVGy = J/kg= 6.2e6eV/pL

Stochastic versus Deterministic
Figure by R.K. Sachs.

Why Study Radiation as the Input?
• Best carcinogen exposure assessment: A-bomb survivors remember exactly where they were, so doses can be reconstructed
• Compared to chemical carcinogen, cannot simply not use it: background, diagnostic, and therapeutic exposures are here to stay
• Physics is understood, so results across x- & γ-rays, neutrons & protons, and α- and β particles at different energies can be unified
Other CML-ogen, aging, also cannot be avoided+exposure is known

Why Study CML as the Output?
• CML is homogeneous: all have BCR-ABL• CML is prevalent: introns large => per-cell
target size for creating bcr-abl is large• leukemias have rapid onset kinetics: white
blood cells go in and out of tissues naturally so they don’t need to learn to metastasize
Chr9 = 136.3 Mb
~140 kb 139.6 Kb DNA Repair 10 (2011) 1131– 1137
~5 kb = introns between e12-e15
Chr 2249.2 Mb
From 1KG browser

PML-RARA intron sizes
~20kbSeer APL/CML 1234/10103= 12%=1/8
40/700=1/18
40%,55% Mediterr J Hematol Infect Dis. 2011;3(1)
~2kb

Dose Response
itkc
iikac
i PetDem iti )( 21 2
)(222
21 ])([ niknikikitniDDD
itkc
iniiikac
i ePetDDDem
ittkcii ettwTbaPN 22)()|(
N is the number of CML target cells in an individual P(ba|T) is the probability of BCR-ABL given a translocation
w(t)=probability density that CML arrives at t given bcr-abl at t=0
2)(
23 tkt
tetktw
30
22
22
t
ctkc
k
edtetR t
Linear R = 0.0075/Gy. LQE posterior R = 0.0022/Gy

CML Target Cell Numbers
• A comparison of age responses for CML and total translocations suggests a CML target cell number of 4x108
• 1012 nucleated marrow cells per adult and one LTC-IC per 105 marrow cells suggests 107 CML target cells
• P(ba|T) = 2TablTbcr/2 may not hold

Kozubek et al. (1999) Chromosoma 108: 426-435
BCR-to-ABL 2D distances

23
Hi-C Data
http://hic.umassmed.edu/heatmap/heatmap.php
133
chr9
chr22
K562 = bcr-abl+ CML cells
Lieberman-Aiden, et al. Science 9 October 2009: 289-293.
23
133
GM06690 = EBV-transformed lymphoblasts
Off by 2 Mb?

Theory of Dual Radiation Action
P(ba|D) = probability of a BCR-ABL translocation per G0/G1 cell given a dose D
tD(r)dr = expected energy at r given an ionization event at the origin
= intra-track component + inter-track component
Sba(r) = the BCR-to-ABL distance probability density
g(r) = probability that two DSBs misrejoin if they are created r units apart
Y = 0.004 DSBs per Mb per Gy; = mass density
TBCR = 5.8 kbp; TABL = 140 kbp
2
02
2 )()(4
)(2)|( DDdrrgrS
r
rtDYTTDbaP bababa
DABLBCR
DrrtrtD24)()(

Total Translocations → g(r) estimate
)/(0
0)( rreprg
6
5
4
3
3
2
0 )16/3()4/9(3)(R
r
R
r
R
rrS
0
)/(2
0
20 0
4
)()(
25.6
)(
4
1dre
r
rSrt
Gp rrd
0
)/(2
0
20 0
4
)()(
25.6
)(
4
1dre
r
rSrt
Gp rrxdx
0
)/(0
20
0)()(4
1drerSGp rr
d
G=25 DSB/Gy
6.25 kev/m3 = 1 Gy
R = 3.7 m r0 = 0.24 m, p0 = 0.12
d in [.01, .025], dx in [.04, .05], d in [.05, .06]

Risk and Target Cell Numbers
Dependence of R and N on the choice of fixed LQE parameters ba/ba and ban/ba
BA/BA BAn/BA R (Gy-1) N
.055/.0107 .8/.0107 .0022 (.0012, .0039)a 6.1x108 (3.3x108, 1.1x109) .055/.022 .8/.022 .0039 (.0020, .0073) 5.2x108 (2.7x108, 9.8x108) .45/3.64 .8/.022 .0094 (.0051, .0176) 7.6x106 (4.1x106, 1.4x107)
aIn parentheses are the 95% CI.
bat
ctkc N
k
edtetR t
30
22
22
ba
RN
Higher risk estimate is more biologically plausible
Linear-to-quadratic transition dose changed from [0.011-0.022]/0.055= [0.2-0.4] Gy to3.64/.45= 8.09 Gy
Linear R = 0.0075/Gy for D < 4Sv is higher here at 0.0094/Gy due to cell killing term

Bcr-Abl to CML Waiting Times
2)(
23 tkt
tetktw
ijkkjiijk PYFDAE
1950 1970 1990
IR-to-CML Latency
Year
Ca
ses
pe
r 10
4 P
ers
on
-Ye
ar-
Sv
0
2
4
6 MalesFemales
M/F=1.42tf-tm=6.3y
M/F=1.6tf-tm=10 yrs
0 20 40 60 80
Age
1
10
102
Ca
ses
pe
r 10
6 P
ers
on
-Ye
ars
U.S. CML Incidence 1973-2009
Males k = 0.047Females k = 0.046

Age at Exposure Dependence
10 20 30 40 50Age at exposure
Ca
ses
pe
r 10
5 P
ers
on
-Ye
ars
0.1
11
0
Males
mostly radiogenic
High DoseMedium DoseLow Dose
10 20 30 40 50Age at exposure
Ca
ses
pe
r 10
5 P
ers
on
-Ye
ars
0.1
11
0
Females
mostly radiogenic
High DoseMedium DoseLow Dose

Nagasaki HSC Reserve Loss?
6 Nagasaki CML vs 53 in Hiroshima Hiroshima PY=1558995 Nagasaki PY= 690084 (i.e. 2.26 lower),
53/2.26 = ~23 cases expected in Nagasaki HSC reserve permanently depleted to 25%?
Human T-cell leukemia virus (HTLV): 22 adult T-cell leukemias (ATLs) in Nagasaki compared to 1 in Hiroshima (2.26 more PY => expect ~50)
11
1
10 20 30 40 50 60 70
Age
2
2
2 2
3
3
3
3
10
102
103
Ca
ses
pe
r 10
6 P
ers
on
-Ye
ars
Japanese A-Bomb Survivors
D < 0.02 Sv0.02 < D < 1 SvD > 1 Sv

Dead-Band Control of HSC levels
• Transplant doses of 10, 100, and 1000 CRU => CRU levels 1-20% or 15-60% normal Blood (1996) 88: 2852-2858
• Broad variation in human HSC levels Stem Cells (1995) 13: 512-516
• Low levels of HSCs in BMT patients Blood (1998) 91: 1959-1965

0 20 40 60 80Age
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
Males
1973-1984 k = 0.0581985-1996 k = 0.0481997-2009 k = 0.038
0 20 40 60 80Age
Females
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
1973-1984 k = 0.0531985-1996 k = 0.0491997-2009 k = 0.038
HSC Reserve Loss Trend?Ave last 7 ratios0.700.49
1995 data yielded k= 0.041 [Radiat Environ Biophys (1999) 38:201–206]. 0.031 in 2006 is consistent with tlcns leading CML by 10 yrs
0.800.54

All Cancer Incidence Conclusion: Cancer therapy is not the cause of the HSC reserve depletion
Other Guesses? Does obesity increase bone marrow fat and thus squeeze out HSC? 1. Mississippi (34.4%) 51. Colorado (19.8%) 0.1*x+1(1-x)=0.5 => .5=.9x => x=.555Prevalence of cause must be greater than 55%Cancer Epidemiol Biomarkers Prev 2009;18:1501-1506 => obesity causes CML
Easier travel=> greater loads on immune system?
0 20 40 60 80
Cumulative Incidence of Cancer
age
prob
abili
ty o
f ca
ncer
10 3
10 2
0.1
0.5
malesfemales
0 20 40 60 80Age
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
Males
1973-1984 k = 0.0581985-1996 k = 0.0481997-2009 k = 0.038
0 20 40 60 80Age
Females
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
1973-1984 k = 0.0531985-1996 k = 0.0491997-2009 k = 0.038

Or is it CMML Misclassification?
CML = ICDO-2 9863 does not include CMML. Maybe all were called CML <1985, 50% in 1985-1995, and 0 after
0 20 40 60 80Age
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
Males
1973-1984 k = 0.0581985-1996 k = 0.0481997-2009 k = 0.038
0 20 40 60 80Age
Females
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
1973-1984 k = 0.0531985-1996 k = 0.0491997-2009 k = 0.038
CML=ICD9 205.1 includes 20% CMML
0 20 40 60 80Age
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
Males
1973-1984 k = 0.0581985-1996 k = 0.0551997-2009 k = 0.053
0 20 40 60 80Age
Females
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
1973-1984 k = 0.0531985-1996 k = 0.0541997-2009 k = 0.05

CMML rises at older ages
ICDO-2 9945 = CMML
0 20 40 60 80Age
0.1
1
10
102
Ca
ses
pe
r 10
6 P
YMales
1985-19961997-2009
0 20 40 60 80Age
Females
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
1985-19961997-2009
Counts of CMML per year. None before 19851984 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 1 40 41 43 50 53 70 61 68 66 65 79 93 65 85 78 82 87 2003 2004 2005 2006 2007 2008 2009 93 127 84 91 104 80 123

AML
More APL or better diagnostics?
0 20 40 60 80Age
10
102
Ca
ses
pe
r 10
6 P
Y
AML Males
1973-19841985-19961997-2009
0 20 40 60 80Age
AML Females
10
102
Ca
ses
pe
r 10
6 P
Y
0 20 40 60 80Age
1
Ca
ses
pe
r 10
6 P
Y
APL Males
1973-19841985-19961997-2009
0 20 40 60 80Age
APL Females
0.1
1
Ca
ses
pe
r 10
6 P
Y

Retinoic Acid and Imatinib
Cures found for cancers that are molecularly homogeneous:simpler cancers are being solved first
0 20 40 60 80 100 1200.
00.
20.
40.
60.
81.
0
APL males
Months
Su
rviv
al
0 20 40 60 80 100 120
0.0
0.2
0.4
0.6
0.8
1.0
APL females
Months
Su
rviv
al
0 50 100 150 200 250 300
0.0
0.2
0.4
0.6
0.8
1.0
CML males
Months
Su
rviv
al
0 50 100 150 200 250 3000.
00.
20.
40.
60.
81.
0
CML females
Months
Su
rviv
al
1973-19811982-19911991-19992000-2009

AML and CLL
More typically progress is slower
0 50 100 150 200 250 300
0.0
0.2
0.4
0.6
0.8
1.0
AML males
Months
Su
rviv
al
0 50 100 150 200 250 300
0.0
0.2
0.4
0.6
0.8
1.0
AML females
Months
Su
rviv
al
0 50 100 150 200 250 300
0.0
0.2
0.4
0.6
0.8
1.0
CLL males
Months
Su
rviv
al
0 50 100 150 200 250 300
0.0
0.2
0.4
0.6
0.8
1.0
CLL females
Months
Su
rviv
al
1973-19811982-19911991-19992000-2009

Acknowledgements
• Department of Epidemiology & Biostatistics • Rainer Sachs (UC Berkeley) • Yogen Saunthararajah (Cleveland Clinic)• Thank you for listening!

SEER Underreporting Possibility
Most conservative claims-based algorithm vs. SEER. B. M. Craig et al. Cancer Epidemiol Biomarkers Prev; 21(3) March 2012

Radiation Doses Rising

AML
Assuming all CML-ogens are also AML-ogens, this implies CML decreases are NOT due to decreases in exposures to bcr-abl forming agents.
No AML trend is consistent with target cells being lineage committed and thus more tightly regulated than HSCs.
0 20 40 60 80Age
10
102
Ca
ses
pe
r 10
6 P
Y
AML Males
1973-19841985-19961997-2009
0 20 40 60 80Age
AML Females
10
102
Ca
ses
pe
r 10
6 P
Y

Others
0 20 40 60 80Age
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
MML Males
1973-19841985-19961997-2008
0 20 40 60 80Age
MML Females
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
0 20 40 60 80Age
0.1
1
10
102
Ca
ses
pe
r 10
6 P
Y
CLL Males
1973-19841985-19961997-2008
0 20 40 60 80Age
CLL Females
1
10
102
Ca
ses
pe
r 10
6 P
Y

All Cancer Incidence
0 20 40 60 80
Age
Cas
es p
er P
erso
n-Y
ear
10 4
10 3
10 2
Males
1973-19841985-19961997-2008
0 20 40 60 80
Age
Cas
es p
er P
erso
n-Y
ear
Females
10 4
10 3
10 2
Incidence of All Cancers

All Cancer Incidence
0 20 40 60 80
Incidence of All Cancers
age
Cas
es p
er P
erso
n-Y
ear
10 4
10 3
10 2
femalesmales
2026202 Males 2157740 Females 438616821 MalePY 454528905 FemPY

Nagasaki HSC Reserve Loss?
Hiroshima
Nagasaki10 20 30 40 50
Age at exposure
Ca
ses
pe
r 10
5 P
ers
on
-Ye
ars
0.1
11
0
mostly radiogenic
High DoseMedium DoseLow Dose
10 20 30 40 50Age at exposure
Ca
ses
pe
r 10
5 P
ers
on
-Ye
ars
0.1
11
0
High DoseMedium DoseLow Dose
6 Nagasaki CML vs 53 in Hiroshima Hiroshima PY=1558995 Nagasaki PY= 690084 (i.e. 2.26 lower),
53/2.26 = ~23 cases expected in Nagasaki HSC reserve permanently depleted to 25%? Human T-cell leukemia virus (HTLV): 22 adult T-cell leukemias (ATLs) in Nagasaki compared to 1 in Hiroshima (2.26 more PY => expect ~40)
iii
i mmO )log(