Embed Size (px)
Citation preview

Epidemiology of Hypertension
Stanley S. Franklin, MD, FACP, FACC
Clinical Professor of MedicineUniversity of California at IrvineAssociate Medical DirectorUCI Heart Disease Prevention ProgramIrvine, California

Agenda: epidemiology of hypertension
1 BP measurement
2 Defining hypertension
3 Why an important public health problem
4 Global risk assessment
5 Intervention trials and meta-analyses
6 Management strategies
7 Barriers to treatment
8 Prevention strategies
1 BP measurement
2 Defining hypertension
3 Why an important public health problem
4 Global risk assessment
5 Intervention trials and meta-analyses
6 Management strategies
7 Barriers to treatment
8 Prevention strategies

1. How to measure blood pressure?

Nokolai Korotkoff, 1905
Ascultatory method of
blood pressure measurement

Noninvasive Blood Pressure Measurement
Noninvasive Blood Pressure Measurement
Methodologies
- Auscultatory (K sound) - Mercury
- Aneroid
- Oscillometric
Locations Situations
- Upper arm - Clinic
- Wrist - Home
- Finger - Ambulatory
Methodologies
- Auscultatory (K sound) - Mercury
- Aneroid
- Oscillometric
Locations Situations
- Upper arm - Clinic
- Wrist - Home
- Finger - Ambulatory

2. Defining Hypertension:
(a) By the numbers?≥95 DBP160/95140/90130/85 >120/80
“A number at which the benefits of intervention exceed those of
inaction”

2098 Franklin #7
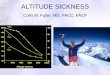
CV Mortality Risk Doubles withEach 20/10 mm Hg BP Increment*
*Individuals aged 40-70 years, starting at BP 115/75 mm Hg.CV, cardiovascular; SBP, systolic blood pressure; DBP, diastolic blood pressureLewington S, et al. Lancet. 2002; 60:1903-1913. JNC 7. JAMA. 2003;289:2560-2572.
CVmortality
risk
SBP/DBP (mm Hg)
0
1
2
3
4
5
6
7
8
115/75 135/85 155/95 175/105

2098 Franklin #8
JNC Reclassification of BP Based on Risk
Source for JNC VI: Arch Intern Med. 1997;157:2413-2446.Adapted with permission from Chobanian AV et al. Hypertension. 2003;42:1206-1252.
JNC VIJNC VISBP
(mm Hg)SBP
(mm Hg)DBP
(mm Hg)DBP
(mm Hg)SBP
(mm Hg)SBP
(mm Hg)DBP
(mm Hg)DBP
(mm Hg)
Optimal Normal80 <120<120 and 80and
Normal
Hi-normalPrehypertension
120-129
130-139120-139
80-84
or 85-89
and80-89or
Stage 1
Hypertension
Stage 1140-159 140-15990-99or 90-99or
Stage 2
Stage 3Stage 2
160-179
≥ 180≥ 160
100-109or
≥ 110or≥ 100or
CategoryCategory CategoryCategory
JNC 7JNC 7

BP CategoryBP Category PrevalencePrevalence
NormalNormal 38%38%
PrehypertensionPrehypertension 31%31%
HypertensionHypertension 31%31%
Prevalence of Blood Pressure Prevalence of Blood Pressure Categories in US Adults ≥20 Years of Categories in US Adults ≥20 Years of
Age Age (NHANES 1999-2000)(NHANES 1999-2000)
Prevalence of Blood Pressure Prevalence of Blood Pressure Categories in US Adults ≥20 Years of Categories in US Adults ≥20 Years of
Age Age (NHANES 1999-2000)(NHANES 1999-2000)
Greenland, Croft, Mensah (CDC). Arch Intern Med. 2004;164:2113fGreenland, Croft, Mensah (CDC). Arch Intern Med. 2004;164:2113f

Prehypertension …Prehypertension …Prehypertension …Prehypertension …
• Is Is notnot a disease, a disease,
• Is Is notnot “hypertension”, “hypertension”,
• Is Is notnot an indication for drug treatment of HTN, an indication for drug treatment of HTN,
• Does Does notnot have a BP goal, have a BP goal,
• DoesDoes predict a higher risk for developing CV predict a higher risk for developing CV
events,events,
• DoesDoes predict a higher risk for developing HTN, predict a higher risk for developing HTN,
• Should be an incentive to improve lifestyle Should be an incentive to improve lifestyle
practices for prevention of HTN and CVD.practices for prevention of HTN and CVD.
• Is Is notnot a disease, a disease,
• Is Is notnot “hypertension”, “hypertension”,
• Is Is notnot an indication for drug treatment of HTN, an indication for drug treatment of HTN,
• Does Does notnot have a BP goal, have a BP goal,
• DoesDoes predict a higher risk for developing CV predict a higher risk for developing CV
events,events,
• DoesDoes predict a higher risk for developing HTN, predict a higher risk for developing HTN,
• Should be an incentive to improve lifestyle Should be an incentive to improve lifestyle
practices for prevention of HTN and CVD.practices for prevention of HTN and CVD.

Defining Hypertension:
(b) By hemodynamic mechanism?
Increased peripheral vascular resistance
versus
Increased large artery stiffness

The Arterial Pulse Wave
75
125
Pre
ssu
re (
mm
Hg
)
Systolic Systolic pressurepressure
Diastolic Diastolic pressurepressure
Mean Mean pressurepressure
Diastolic decay Diastolic decay curvecurve
Dicrotic notchDicrotic notch(aortic valve (aortic valve
closes)closes)
Time
Pulse Pulse pressurpressuree
= 1/3 SBP + 2/3 DBP

Hemodynamic Components of BP
MAP - STEADY COMPONENT (due to CO and SVR)
• PP – PULSATILE COMPONENT (due to LV ejection
and elastic artery stiffness)
• SBP – rises with increased resistance and stiffness
• DBP – rises with increased resistance and decreases
with increased stiffness
Elzinga G, Westerhof N. Circ Res 1973;32:178-186. Yano, et al. Basic Res Cardiol 1997;92:115-122.
Berne RM, Levy MN. Cardiovascular Physiology 1992:135-151.

Overview of Arterial Blood Pressure Hemodynamics
1. Steady component MAP = CO x PVR ↑Resistance small art. MAP = 1/3(SBP) + 2/3(DBP)
Predominantly diastolic “Essential HTN”--young
-- ↑VC or ↓VD responses -- ↑wall-to-lumen diameter -- Rarefaction (Art./Cap.)
2. Pulsatile component PP = SBP – DBP ↑Stiffness large arteries ↑CO and ↑SV Isolated systolic HTN Pathologic aging
-- Disarray of elastin protein-- Abn. extracellular matrix-- ↑Collagen/Calcium depos.

Defining Hypertension:
(c) By subtype?
IDH, SDH, ISH

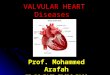
<40 40-49 50-59 60-69 70-79 80+Age (y)
17% 16% 16% 20% 20% 11%
Distribution of Hypertension Subtype in the Untreated Distribution of Hypertension Subtype in the Untreated Hypertensive Population by Age Hypertensive Population by Age (NHANES III)(NHANES III)
ISH (SBP 140 mm Hg and DBP <90 mm Hg) SDH (SBP 140 mm Hg and DBP 90 mm Hg)IDH (SBP <140 mm Hg and DBP 90 mm Hg)
0
20
40
60
80
100
Numbers at top of bars represent the overall percentage distribution of untreated hypertension by age. Franklin et al. Hypertension. 2001;37: 869-874.
Frequency of hypertension
subtypes in all untreated
hypertensives (%)
} Diastolic Hypertension

An Analysis of NHANES III Blood Pressure DataSummary: Hypertensives fall into one of two categories:
1. A smaller (26%), younger (age 50 years), predominantly male (63%) with diastolic hypertension out of proportion to systolic hypertension (primarily IDH and SDH)
2. A larger (74%), older (age 50 years), predominantly female (58%) with systolic hypertension out of proportion to diastolic hypertension (primarily ISH).
Summary: Hypertensives fall into one of two categories:
1. A smaller (26%), younger (age 50 years), predominantly male (63%) with diastolic hypertension out of proportion to systolic hypertension (primarily IDH and SDH)
2. A larger (74%), older (age 50 years), predominantly female (58%) with systolic hypertension out of proportion to diastolic hypertension (primarily ISH).
Franklin et al. Hypertension 2001;37: 869-874

2098 Franklin #18
3. Why is hypertension considered a major Public health problem in the United States?
Firstly, hypertension is very common In the adult population

50
65
0
20
40
60
80
100
1988-1994 1999-2000
National Health and Nutrition Survey (NHANES)
Increased Prevalence of Hypertension in the Increased Prevalence of Hypertension in the United States from 1988-1994 (NHANES III) to United States from 1988-1994 (NHANES III) to
1999-2000 NHANES1999-2000 NHANES
Increased Prevalence of Hypertension in the Increased Prevalence of Hypertension in the United States from 1988-1994 (NHANES III) to United States from 1988-1994 (NHANES III) to
1999-2000 NHANES1999-2000 NHANES
Fields, et al. Hypertension. 2004;44:398f
Po
pu
lati
on
Wit
h
Hyp
erte
nsi
on
(m
illi
on
s)
30% increase, p<.00130% increase, p<.001
Nearly 1 in 3 Adults (31%) in the US Has Hypertension

2098 Franklin #20
Trends in Prevalence of Hypertension in the US Population, by Race/Ethnicity,1988-2000
0
5
10
15
20
25
30
35
Pre
vale
nce
(%)
Non-Hispanic White Non-Hispanic Black Mexican American
1988-1991
1991-1994
1999-2000
*p<0.01, **p<0.001,compared to Non-Hispanic Whites within given time period; no significant trends across time periods within gender; analyses are age-adjusted to 2000 US population. Data from Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988-2000. JAMA 2003; 290: 199-206.
** ****
* *

Chobanian A. N Engl J Med 2009;361:878-887
Hypertension Paradox: Changes in the Prevalence and Control of Hypertension in the United States (1988-2004)
Rate of control:27% to 35%Rate of control:27% to 35%

Colors of Salt
• White• Black• Red• Yellow• Green• Brown• Clear
• Table salt• Soy sauce• Catsup• Mustard• Pickles• Soups & gravies• Saline

The connection between salt, obesity, hypertension and CVD mortality• During the past 25 years salt intake has
increased by 1/3 to 150-170 mmol/day (3.5 to 4.0 g sodium/day).
• This has contributed to the growing obesity epidemic and increased prevalence of hypertension by causing increased intake of high-calorie soft drinks containing corn sugar
• Recent studies suggests that a decrease of 50 mmol/day below the current level (a reduction of 1/3) would decrease BP by 4.0/2.5 mm Hg in hypertensives and reduce CVD mortality in the US by more than 100,000/yr.
• During the past 25 years salt intake has increased by 1/3 to 150-170 mmol/day (3.5 to 4.0 g sodium/day).
• This has contributed to the growing obesity epidemic and increased prevalence of hypertension by causing increased intake of high-calorie soft drinks containing corn sugar
• Recent studies suggests that a decrease of 50 mmol/day below the current level (a reduction of 1/3) would decrease BP by 4.0/2.5 mm Hg in hypertensives and reduce CVD mortality in the US by more than 100,000/yr.

Secondly, hypertension is
associated with considerable
cardiovascular risk.
3. Why is hypertension considered a major Public health problem in the United States?

2098 Franklin #25
Global Mortality 2000: Impact of Hypertension and Other Health Risk Factors
Ezzati et al. Ezzati et al. Lancet.Lancet. 2002;360:1347-1360. 2002;360:1347-1360.Attributable Mortality Attributable Mortality
(In thousands; total 55,861,000)(In thousands; total 55,861,000)
High mortality, developing regionHigh mortality, developing region
Lower mortality, developing regionLower mortality, developing region
Developed regionDeveloped region
00 8000800070007000600060005000500040004000300030002000200010001000
High blood pressureHigh blood pressure
TobaccoTobacco
High cholesterolHigh cholesterol
Unsafe sexUnsafe sex
High BMIHigh BMI
Physical inactivityPhysical inactivity
AlcoholAlcohol
Indoor smoke from solid fuelsIndoor smoke from solid fuels
Iron deficiencyIron deficiency
UnderweightUnderweight

Is it a true risk factor or a risk marker?
A true risk factor is suspected of being causative of the disease process.
A risk marker is associated with the disease process without being in the
causal pathway.

TIA = transient ischemic attack; LVH = left ventricular hypertrophy; CHD = coronary heart disease; HF = heart failure.Cushman WC. J Clin Hypertens. 2003;5(Suppl):14-22.
Retinopathy Renal failurePeripheral vascular
disease
Complications of Hypertension:
LVH, CHD, HF
TIA, stroke
Hypertension Hypertension is a risk factoris a risk factor

2098 Franklin #28
:“Diabesity”

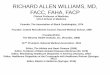
Association of Systolic BP andCV Death in Type 2 Diabetes
0
25
50
75
100
125
150
175
200
225
250
<120 120–139 140–159 160–179 180–199 200
Without diabetes
With diabetes
CV
mort
alit
y r
ate
/10,0
00 p
ers
on-y
Systolic BP (mm Hg)Stamler et al. Diabetes Care. 1993;16:434.

Progression of Diabetes
DeathIGTIGT
•Genetic susceptibility
•Environmental factors– Nutrition– Obesity
– Inactivity
– Insulin resistance– HDL-C
– Triglycerides– Atherosclerosis– Hypertension
Hyperglycemia RetinopathyNephropathyNeuropathy
BlindnessESRD/Dialysis/Transplantation
CHDStroke
AmputationBrown. Diabetes Obes Metab.
2000;2:S11.
Ongoing Ongoing hyperglycemiahyperglycemia
Diagnosis ofDiagnosis ofdiabetesdiabetes
Appearance of Appearance of complicationscomplications
DisabilityDisability

Stages of Chronic Kidney Disease
Stage Description GFR
mL/min/1.73 m2
1 Kidney damage with normal or increased GFR
≥ 90
2 Kidney damage with mild decreased GFR
60-89
3 Moderate decreased GFR 30-59
4 Severe decreased GFR 15-29
5 Kidney failure < 15 (or dialysis)

Proteinuria Is an Independent Risk Factor for Mortality in Type 2 Diabetes
1.0
0.9
0.8
0.7
0.6
0.50 1 2 3 4 5 6
Years
Surv
ival
(all-
cause
mort
alit
y)
Normoalbuminuria(n=191)
Microalbuminuria(n=86)
Macroalbuminuria(n=51)
P<0.01, normo- vs micro- and macroalbuminuria.P<0.05, micro- vs macroalbuminuria.
Gall et al. Diabetes. 1995;44:1303.

Diabetes:The Most Common Cause of ESRD
United States Renal Data System. Annual data report. 2000.
Primary Diagnosis for Patients Who Start Dialysis
Diabetes50.1%
Hypertension27%
Glomerulonephritis
13%
Other
10% No. of patientsProjection95% CI
1984 1988 1992 1996 2000 2004 20080
100
200
300
400
500
600
700
r2=99.8%243,524
281,355520,240
No
. o
f d
ialy
sis
pat
ien
ts
(th
ou
san
ds)

ESRD in the USA
↓ Mortality from MI & stroke over past 30 years
↑ Life expectancy contributed to ↑ ESRD
Currently in USA > 300,000 patients on dialysis
The cost exceeds $ 50,000 per patient per year
Twenty one billion $ projected cost in 2002
First year mortality ~ 20%
~ 50% of deaths are cardiac (USRDS)

Life Expectancy for Selected U.S. Populations
0
5
10
15
20
25
30
35
Age 49 Age 59
U.S.Prostate cancerColon cancerESRDLung cancer
USRDS 1993 Annual Data Report
USRDS 1993 Annual Data Report
Expe
cted
rem
aini
ng y
ears

Thirdly, there is considerablereduction in cardiovascular riskwith effective lowering of blood
pressure with therapy.
3. Why is hypertension considered a major Public health problem in the United States?

35%-40%
20%-25%
>50%
Average reduction in events
(%)
–60
–50
–40
–30
–20
–10
0Stroke
Myocardialinfarction Heart failure
Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet. 2000;355:1955-1964.
Long-Term Antihypertensive Therapy Significantly Reduces CV Events

Fourthly, there is insufficientawareness, treatment andcontrol of hypertension.
3. Why is hypertension considered a major Public health problem in the United States?

0
10
20
30
40
50
60
70
80
Hypertension Awareness, Treatment, and Control: US 1976 to 2000*
NHANES III NHANES III (Phase 2) (Phase 2) 1991-19941991-1994
NHANES III NHANES III (Phase 1) (Phase 1) 1988-19911988-1991
51%51%
73%73% 68%68%
31%31%
55%55% 54%54%
10%10%
29%29% 27%27%
% A
du
lts
% A
du
lts
NHANES II NHANES II 1976-19801976-1980
NHANES NHANES 1999-20001999-2000
70%70%
59%59%
34%34%
Healthy People Healthy People
2000/2010 2000/2010
Control Control
Target = 50%Target = 50%
ControlControl
AwarenessAwareness
TreatedTreated
Chobanian et al. Chobanian et al. JAMAJAMA. 2003;289:2560-2572.. 2003;289:2560-2572.

4. Global Risk Assessment

Risk Factor Clustering With HypertensionRisk Factor Clustering With Hypertension
Risk factor clustering with hypertension, ages 18–74 years. Framingham offspring.
Kannel WB. Am J Hypertens. 2000.
0 1 2 3
5
0
10
15
20
25
30MenWomen
17%19%
26% 27% 25% 24%22%
20%
8%12%
≥4
RiskFactors
(%)
Number of Risk Factors

BP is a risk marker for “The Metabolic Syndrome”
*Diagnosis is established when ≥3 of these risk factors are present.
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
NCEP-ATP III Definition: ≥3 of the Following*NCEP-ATP III Definition: ≥3 of the Following*• Men: >102 cm (>40 in)
• Women: >88 cm (>35 in)
Fasting glucose
• ≥130/≥85 mmHg (risk marker)
Blood pressure
HDL-C
• ≥150 mg/dLTriglycerides
Abdominal obesity (waist circumference)
• Men: <40 mg/dL
• Women: <50 mg/dL
• ≥100 mg/dL

Other CVD Risk Factors: JNC 7
Physical inactivity Cigarette smoking Age (older than 55 for men, 65 for women) Family history of premature CVD
(men under age 55 or women under age 65)
*Components of the metabolic syndrome in blue Chobanian et al. Chobanian et al. JAMAJAMA. 2003;289:2560-. 2003;289:2560-25722572

700
600
500
400
300
200
100
8 Y
ea
r P
rob
ab
ility
Pe
r 1
,00
0
Systolic BP:Cholesterol:Glucose Intol.:Cigaretes:ECG-LVH:
105 >>> 185185
000
105 >>> 185335
000
105 >>> 185335+00
105 >>> 185335++0
105 >>> 185335+++
Kannel, 1983
Framingham Heart Study (1983)Framingham Heart Study (1983) CV Risk ProfileCV Risk Profile
703
459
326
210
46

Expert Panel on Detection, Evaluation, and Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Treatment of High Blood Cholesterol in Adults. JAMAJAMA. 2001;285:2486-2497.. 2001;285:2486-2497.
Age, yAge, y PointsPoints
20-3420-34 -9-935-3935-39 -4-440-4440-44 0045-4945-49 3350-5450-54 6655-5955-59 8860-6460-64 101065-6965-69 111170-7470-74 121275-7975-79 1313
11
22
55
TotalTotal AgeAge AgeAge AgeAge AgeAge AgeAgeCholesterolCholesterol 20-3920-39 40-4940-49 50-5950-59 60-6960-69 70-7970-79
<160<160 00 00 00 00 00160-199160-199 44 33 22 11 00200-239200-239 77 55 11 33 00240-279240-279 99 66 44 22 11
280280 1111 88 55 33 11
AgeAge AgeAge AgeAge AgeAge AgeAge20-3920-39 40-4940-49 50-5950-59 60-6960-69 70-7970-79
HDL mg/dLHDL mg/dL PointsPoints
6060 -1-150-5950-59 0040-4940-49 11
<40<40 22
Systolic BPSystolic BP IfIf IfIfmm Hgmm Hg UntreatedUntreated TreatedTreated
<120<120 00 00120-129120-129 00 11130-139130-139 11 22140-159140-159 11 22160160 22 33
Point TotalPoint Total 10-Year Risk, %10-Year Risk, %
<0<0 <1<100 1111 1122 1133 1144 1155 2266 2277 3388 4499 55
1010 661111 881212 10101313 12121414 16161515 20201616 2525
1717 3030
66
ATP-III: Framingham Point ScoresEstimate of 10-Year Risk for Men
NonsmokerNonsmoker 00 00 00 00 00SmokerSmoker 88 55 33 11 11
44
33

2098 Franklin #46

5. Intervention Trials

Trial duration is <10 years; treatment benefits should be considered in the very long term (decades).
Drop-in effect (subjects under placebo are given active drug) and drop-out effect (drop-outs in the active treatment group.
Subjects included in the trials are generally healthier than those treated in the clinical practice (selection of low-risk subjects).
Secondary end-points & subgroup analyses difficult to interperet.
Trials & meta-analyses:What we do not know (...and maybe will never
know)

2098 Franklin #49
•“Hypertension may be an important compensatory mechanism which should not be tampered with, even were it certain that we could control it.”
•“Hypertension may be an important compensatory mechanism which should not be tampered with, even were it certain that we could control it.”Paul Dudley White, 1931 Textbook of Cardiology.

2098 Franklin #50Messerli, F. H. Messerli, F. H. N Engl J MedN Engl J Med 1995 1995

Hypertension Intervention Trials: 1959-1970
Trial Severity of Hypertension
CV events/yr. In CTRL Group
CV events/yr: CTRL vs Ther. Group
Harrington, et al (1959)
Malignant Hypertension
90% Mortality 90% vs 50% (Mortality / Yr)
VA Coop. Study (1967)
Severe (DBP 115 mmHg) 187/121
29% 10:1 (1.5 Yr.)
VA Coop. Study (1970)
Moderate (DBP 105-114 mmHg) 165/105
5.5% 3.5:1 (4.5 Yr.)

TOMHSTOMHSVA MONORxVA MONORx
CONVINCECONVINCEALLHAT ALLHAT ANBP2ANBP2
LIFELIFE
HAPPHYHAPPHYMAPHYMAPHY
INSIGHTINSIGHTNORDILNORDIL
CAPPPCAPPPSTOP-2STOP-2
VALUEVALUEASCOTASCOT
ACCOMPLISHACCOMPLISH
Clinical Trials in Hypertension
HR Black, 2003.HR Black, 2003.
1960s1960s 1970s1970s 1980s1980s 1990-19951990-1995 1996-19991996-1999 20002000 2001-20032001-2003 2004-20082004-2008
Should we treat Should we treat diastolic HBP?diastolic HBP?
What is the What is the best way to best way to treat HBP?treat HBP?
Should we treat Should we treat DBP in older DBP in older
persons?persons?
What is theWhat is the goal of goal of
treatment?treatment?
Should we Should we treat ISH in treat ISH in
older older persons?persons?
Can we Can we prevent prevent
hypertension?hypertension?
VA VA Cooperative Cooperative
StudiesStudiesMRC-1MRC-1
ANHBP-1ANHBP-1
EWPHEEWPHE
MRC-2MRC-2
STOP-1STOP-1
SCOPESCOPEHDFPHDFP HOTHOT
UKPDSUKPDS
Syst-EurSyst-EurSyst-ChinaSyst-China
SHEPSHEP TROPHYTROPHY

SHEP Trial:Design
• N: 4736; 43% male
• Age: >60
• BP: SBP 160-219 and DBP <90
• Design: Placebo control, double blind
• Active Rx: Chlorthalidone (atenolol as step 2)
• SBP difference: 12 mm Hg
• Duration: 4.5 years
JAMA 1991;265:3255

2098 Franklin #54
SHEP Trial:Cardiovascular Disease Endpoints
JAMA 1991;265:3255

HR 95% CI P value
All stroke - 34% 0.46 - 0.95 0.025
Total mortality - 28% 0.59 - 0.88 0.001
Fatal stroke - 45% 0.33 - 0.93 0.021
Cardiovascular mortality - 27% 0.55-0.97 0.029
Heart failure - 72% 0.17-0.48 <0.001
Cardiovascular events - 37% 0.51-0.71 <0.001
HYVETResults All Outcomes
Per Protocol
Beckett N. N Engl J Med. 2008;358: epub. March 31, 2008.

6. Management of Hypertension

Seventh Report of the Joint National Committee onPrevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) EXPRESS
Seventh Report of the Joint National Committee onPrevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) EXPRESS
National Heart, Lung, andBlood Institute
National High Blood PressureEducation Program

JNC 7: Appropriate BP Targets• For both CVD and kidney disease, systolic BP is far
more important than diastolic BP
• Systolic BP should be <140 mm Hg in all patients, and ideally between 120-130 mm Hg in patients with complications (diabetes, heart failure, kidney disease)
• Only a small fraction of hypertensives are achieving appropriate BP control
• Multiple antihypertensive agents are needed for most patients
• Those with SBP 120–139 mmHg or DBP 80–89 mmHg should be considered pre-hypertensive who require health-promoting lifestyle modifications to prevent CVD.
• For both CVD and kidney disease, systolic BP is far more important than diastolic BP
• Systolic BP should be <140 mm Hg in all patients, and ideally between 120-130 mm Hg in patients with complications (diabetes, heart failure, kidney disease)
• Only a small fraction of hypertensives are achieving appropriate BP control
• Multiple antihypertensive agents are needed for most patients
• Those with SBP 120–139 mmHg or DBP 80–89 mmHg should be considered pre-hypertensive who require health-promoting lifestyle modifications to prevent CVD.

JNC 7: Considerations for olderpersons with hypertension
This population has the lowest rates of BP control and the greatest absolute benefit with effective therapy.
Lower initial drug doses may be indicated to avoid symptoms; standard doses and multiple drugs will be needed to reach BP targets.
More than two-thirds of people over 65 have HTN, i.e. ISH (Isolated systolic hypertension).

JNC 7: Considerations for special populations with hypertension
• Treatment generally similar for all demographic groups
• Socioeconomic factors and lifestyle important barriers to BP control
• Prevalence, severity of hypertension increased in blacks
• Treatment generally similar for all demographic groups
• Socioeconomic factors and lifestyle important barriers to BP control
• Prevalence, severity of hypertension increased in blacks
JNC 7. JAMA. 2003;289:2560-2672.

Intervention
Exercise
Weight reduction
Alcohol intake reduction
Sodium intake reduction
DASH diet
Intervention
Exercise
Weight reduction
Alcohol intake reduction
Sodium intake reduction
DASH diet
Lifestyle Interventions for Prevention or Treatment of Hypertension
Blood Pressure Effect
5-10 mm Hg (>30 min >3x/wk)
1-2 mm Hg/Kg
1 mm Hg/drink/d
1-3 mm Hg/40 mmol/d
3-10 mm Hg
Blood Pressure Effect
5-10 mm Hg (>30 min >3x/wk)
1-2 mm Hg/Kg
1 mm Hg/drink/d
1-3 mm Hg/40 mmol/d
3-10 mm Hg Adapted from Cushman et al. Endocrine Practice 1997;3:106 & Sacks, et al. NEJM 2001;334:3

2098 Franklin #62

Lifestyle Treatment Measures
Nonpharmacologic treatments are used for:
Lowering blood pressure
Reducing need for antihypertensive agents
Minimizing associated risk factors
Primary prevention of hypertension

19721972 19731973 19761976 19801980 19841984 19881988 19931993 19971997 20032003
Development of Hypertension Guidelines: the JNCs and Drug Therapy
NHBPEPNHBPEPSTARTSSTARTS
EarliestEarliestGuidelinesGuidelines
28 drugs28 drugsDBP DBP 105105DiureticsDiuretics
JNC IJNC I
43 drugs43 drugs
diuretics,diuretics,-blockers-blockers
AddedAdded
JNC IIIJNC III
JNC IIJNC II
34 drugs34 drugsDiureticsDiuretics
JNC IVJNC IV
50 drugs50 drugsACEI, CAsACEI, CAs
addedadded
JNC VIJNC VI
84 drugs84 drugs7 options7 options
Low-doseLow-dose
JNCs I-7.JNCs I-7.
68 drugs68 drugsDiuretics/Diuretics/-blockers-blockers
JNC VJNC V JNC 7JNC 7
> 125 drugs> 125 drugsDiureticsDiuretics

2098 Franklin #65
0.5 1.0 2.0
BP-Lowering Treatment TrialistsComparisons of Different Active Treatments
Relative Risk RR (95% CI)RR (95% CI)BP DifferenceBP Difference
(mm Hg)(mm Hg)
FavorsFavorsFirst ListedFirst Listed
FavorsFavorsSecond ListedSecond Listed
Major CV eventsMajor CV events
CV mortalityCV mortality
Total mortalityTotal mortality
1.02 (0.98, 1.07)1.02 (0.98, 1.07)2/02/0 ACEI vs D/BBACEI vs D/BB
1.03 (0.95, 1.11)1.03 (0.95, 1.11)2/02/0 ACEI vs D/BBACEI vs D/BB
1.00 (0.95, 1.05)1.00 (0.95, 1.05)2/02/0 ACEI vs D/BBACEI vs D/BB
1.04 (0.99, 1.08)1.04 (0.99, 1.08)1/01/0 CA vs D/BBCA vs D/BB
1.05 (0.97, 1.13)1.05 (0.97, 1.13)1/01/0 CA vs D/BBCA vs D/BB
0.99 (0.95, 1.04)0.99 (0.95, 1.04)1/01/0 CA vs D/BBCA vs D/BB
0.97 (0.95, 1.03)0.97 (0.95, 1.03)1/11/1 ACEI vs CAACEI vs CA
1.03 (0.94, 1.13)1.03 (0.94, 1.13)1/11/1 ACEI vs CAACEI vs CA
1.04 (0.98, 1.10)1.04 (0.98, 1.10)1/11/1 ACEI vs CAACEI vs CA
Blood Pressure Lowering Treatment Trialists’ Collaboration. Blood Pressure Lowering Treatment Trialists’ Collaboration. LancetLancet. 2003;362:1527-1535.. 2003;362:1527-1535.

Not at Goal Blood Pressure (<140/90 mm Hg) (<130/80 mm Hg for those with diabetes or chronic kidney disease)
Not at Goal Blood Pressure (<140/90 mm Hg) (<130/80 mm Hg for those with diabetes or chronic kidney disease)
Initial Drug ChoicesInitial Drug Choices
Drug(s) for the compelling indications
Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB)
as needed
Drug(s) for the compelling indications
Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB)
as needed
With Compelling Indications
With Compelling Indications
Lifestyle ModificationsLifestyle Modifications
Not at Goal Blood Pressure
Not at Goal Blood Pressure
Optimize dosages or add additional drugs until goal blood pressure is achieved
Consider consultation with hypertension specialist
Optimize dosages or add additional drugs until goal blood pressure is achieved
Consider consultation with hypertension specialist
Stage 2 Hypertension (SBP >160 or DBP >100 mm Hg)
2-drug combination for most (usually thiazide-type diuretic and
ACEI, or ARB, or BB, or CCB)
Stage 2 Hypertension (SBP >160 or DBP >100 mm Hg)
2-drug combination for most (usually thiazide-type diuretic and
ACEI, or ARB, or BB, or CCB)
Stage 1 Hypertension(SBP 140-159 or DBP 90-99 mm
Hg) Thiazide-type diuretics for most
May consider ACEI, ARB, BB, CCB,
or combination
Stage 1 Hypertension(SBP 140-159 or DBP 90-99 mm
Hg) Thiazide-type diuretics for most
May consider ACEI, ARB, BB, CCB,
or combination
Without Compelling Indications
Without Compelling Indications
JNC 7 Algorithm for Treatment of Hypertension
Chobanian et al. Chobanian et al. JAMAJAMA. 2003;289:2560-2572.. 2003;289:2560-2572.

Number of Medications to Achieve Goal BP in 5 Trials of DM &/or Renal Disease
3.8
3.3
3.6
2.8
2.7
0 1 2 3 4
AASK (<92 mm Hg MAP)
HOT (<80 mm Hg DBP)
MDRD (<92 mm Hg MAP)
ABCD (< 75 mm Hg DBP)
UKPDS (<150/85 mm Hg)
Number of BP Meds
Bakris. Bakris. J Clin HypertensJ Clin Hypertens 1999;1:141-7 1999;1:141-7

7. Barriers to Treatment

Barriers to Controlling Hypertension
HealthcareSystem
Patients Providers

2098 Franklin #70
The Initial Confrontation of the HTN Problem
• Upon making a diagnosis of HTN, tell patient the BP reading and what it should be (provide a written copy).
• Prepare patient for the probable necessity for polypharmacy to control BP with a minimum of side effects
• Advise Home BP measurement (135/85 mmHg is considered to be hypertensive).
• Upon making a diagnosis of HTN, tell patient the BP reading and what it should be (provide a written copy).
• Prepare patient for the probable necessity for polypharmacy to control BP with a minimum of side effects
• Advise Home BP measurement (135/85 mmHg is considered to be hypertensive).
Table 28. JNC 7 Report. Hypertension. 2003;42(6):1240.

Self-Measurement of BP
Provides information useful for:
1. assessing response to antihypertensive Rx
2. improving adherence with therapy
3. evaluating white-coat HTN
Home BP is more strongly related to target organ damage and has better prognostic accuracy than office BP.

8. Prevention Strategy:
General Population StrategyVersus
Targeted Intensive Strategy

Strategies for Prevention of High Blood Pressure
General Population Strategy
Attempt to shift (downwards) the distribution of BP in entire population
Targeted Intensive Strategy
More intensive efforts to reduce BP in individuals/groups at highest risk of hypertension
High normal BP
Family history of hypertension
High risk groups
Environmental exposures that increase probability of hypertension
High weight High salt intake Alcohol consumption Physical inactivity
17% reduction in prevalence of hypertension
14% reduction in average annual incidence of stroke
6% reduction in average annual incidence of CHD
Estimated Effect of 2 mm Hg Reduction inAverage Diastolic BP in General Population
Cook N R et al., Arch Intern Med 1996
35-64 year old White Residents of United States
FollowingIntervention
BeforeIntervention
Whelton, PK, He J, Appel LA et al., JAMA 2002;288:1882-1888

• Epidemiology Summary:
– Increasing prevalence; world wide problem
– Blood pressure as a moving target
– ↑ PVR in the young, ↑ stiffness in the elderly
– Predominantly isolated systolic hypertension
– Consider special populations at increased risk
– Hypertension as a part of absolute global CV risk
– Population vs. high risk approaches for prevention
• Epidemiology Summary:
– Increasing prevalence; world wide problem
– Blood pressure as a moving target
– ↑ PVR in the young, ↑ stiffness in the elderly
– Predominantly isolated systolic hypertension
– Consider special populations at increased risk
– Hypertension as a part of absolute global CV risk
– Population vs. high risk approaches for prevention