Embed Size (px)
Citation preview

I
From the Institute for Community Medicine, Department SHIP/ Clinical-Epidemiological
Research
Director: Prof. Dr. Henry Völzke
Of the Faculty of Medicine, University Medicine Greifswald
Epidemiology of Iodine Deficiency Disorders in Pakistan and North-
East Germany
Inaugural – Dissertation
to
Attainment of Academic Grades
in
Doctor of Natural Sciences in Medicine
(Dr.rer.med)
from
Faculty of Medicine
of
University Medicine Greifswald
2017
Presented by: Rehman Mehmood Khattak
born on: 07 January 1979
in: Karak, Pakistan

II
Dean: Prof. Dr. Max P. Baur
1. Expert: Prof. Dr. Henry Völzke
2. Expert: Prof. Dr. D. Rothenbacher
3. Expert: Prof. Dr. Thomas Remer
City, Room: , Greifswald
Day of Defence: 26 March, 2018

III
Table of Contents
1. Introduction ......................................................................................................................... 1
1.1. Iodine Deficiency Disorders ............................................................................................. 1
1.2. IDD in Pakistan ................................................................................................................ 1
1.3. IDD in North-East Germany ............................................................................................ 2
2. Methodology ......................................................................................................................... 3
2.1. Study Design and Subjects. .............................................................................................. 3
2.1.1. Pregnant Women Study Population ........................................................................... 3
2.1.2. SHIP Study Population ............................................................................................. 3
2.2. Exclusion Criteria ............................................................................................................ 3
2.3. Assessments in Pregnant Women Population ................................................................... 4
2.4. Assessments in the SHIP Population ................................................................................ 4
2.5. Thyroid Ultrasound .......................................................................................................... 5
2.6. Statistical Analysis ........................................................................................................... 6
3. Results .................................................................................................................................. 6
3.1. Iodine Nutrition in Pregnant Women and Regional Influence in Pakistan ......................... 6
3.2. Monitoring the Prevalence of Thryoid Disorders in North-East Germany ......................... 8
4. Discussion ........................................................................................................................... 10
4.1. Iodine Nutrition in Pregnant Women and Regional Influence ......................................... 10
4.2. Monitoring the Prevalence of Thryoid Disorders in North-East Germany ....................... 11
4.3. The Common Lessons .................................................................................................... 12
4.4. Strengths and Limitations ............................................................................................... 14
5. Conclusion .......................................................................................................................... 14
6. Literature Cited ................................................................................................................. 15

IV
7. Scientific work .................................................................................................................... 20
7.1. Regional Influence on Iodine Nutritional Status of Pakistani Pregnant Women .............. 20
7.2. Monitoring the Prevalence of Thyroid Disorders in the Adult Population of Northeast
Germany ................................................................................................................................... 46
7.3. Factor Affecting Sustainable Iodine Deficiency Elimination in Pakistan: A Global
Perspective ............................................................................................................................... 58
8. Appendix ............................................................................................................................ 68
A. Statutory Declaration ..................................................................................................... 68
B. Own Contributions ......................................................................................................... 69
C. Curriculum Vitae ........................................................................................................... 70
D. Scientific Output ............................................................................................................ 71
E. Acknowledgements .............................................................................................................. 74

v
List of Tables
Table 1. Association of Demographic Characteristics with Iodized Salt Intake, Goiter
Prevalence and UIC <150 µg/L…………………………………………………………........7
Table 2. Change in Thyroid Characteristics between SHIP-0 (1997 - 2001) and SHIP-Trend-
0 (2008 - 2012) ......................................................................................................................9
Figure 1. Adjusted Association of Urban-rural Distribution to Various Parameters of Iodine
Deficiency .............................................................................................................................7


1
1. Introduction
1.1. Iodine Deficiency Disorders
Iodine deficiency disorders (IDD) result from insufficient iodine intake, and may lead to many
adverse effects on growth, development and thyroid diseases in humans (1). The nature of IDD is
variable depending on the region, iodine supplementation, stage of life and physiological
prospects (2).
Goiter presents the classic sequel of chronic iodine deficiency (3). When the iodine intake
decreases, the secretion of the thyroid-stimulating hormone (TSH) is enhanced for the reason to
increase the uptake of available iodine. TSH concentrations in turn stimulate hypertrophy and
hyperplasia of the thyroid, resulting in goiter. Initially goiters are characterized by diffuse,
homogeneous enlargements, but over time nodules and (subclinical) hyperthyroidism often
develop in adults.
Fetal damage is considered as the most serious adverse effect of iodine deficiency (3).
Insufficient iodine supply to the fetus impairs brain development (3). Severe iodine deficiency
during pregnancy may also result in stillbirths, abortions, and congenital abnormalities (4,5).
1.2. IDD in Pakistan
Pakistan is a country with history of iodine deficiency (6). McCarrison firstly identified the
region as severely iodine deficient in 1908 (7). Since then almost all the studies reported a high
goiter prevalence and iodine deficiency particularly in the Khyber Pakhtunkhwa (KPK) province
of Pakistan (6). Pakistan formally adopted the universal salt iodization programme in 1994.
These efforts resulted in a decline of iodine deficiency up to 50% (8). However, the estimated
improvement in IDD eradication is not uniform and may be over-estimated (6). The major
reasons for this are lack of proper planning, political will, and monitoring as well as myths
regarding iodized salt and socioeconomics (6).
Apart from others− Pakistani society is exposed to rural/urban disparity (9) and gender
discrimination (10). When on one hand urban populations enjoy more livelihood facilitation (9),
on the hand females are exposed to direct neglect in the society in terms of exposure, equality

2
and socioeconomic opportunities (10). Women in pregnancy are considered as the most affected
group for iodine deficiency because more iodine is needed during pregnancy (11). In Pakistan
there is less awareness and intake of iodized salt in the general population, as well as no
systematic adaptation of iodine supplementation to pregnant women (6). Hence females are more
exposed to the iodine deficiency issues in Pakistan, while the regional influence work
simultaneously.
1.3. IDD in North-East Germany
Before reunification both parts of Germany were iodine deficient. In the Eastern part, however,
due to mandatory iodine prophylaxis adaptation in 1983, the iodine status of the population
improved from moderate to mild iodine deficiency. After the reunification of Germany in 1989
“voluntary principle” was adopted leading again to a decrease in iodine intake (5). After
improving the legislation of the voluntary iodine fortification programme in 1993, the urinary
iodine excretion levels were elevated and goiter prevalence decreased (12,13). The North-East
German population demonstrated major consequences of long-term iodine deficiency in adults; a
high prevalence of goiter, thyroid nodules and hyperthyroidism in general population, as
extracted from the results of first Study of Health in Pomerania cohort (SHIP-0) conducted
between 1997 to 2001 (14).
A stable IDD prevention would result in a decrease of IDD without increase in the prevalence of
hypothyroidism and autoimmune thyroid disorders (15). The continuously improved iodine
status in North-East German population was reflected by the five-year follow-up examinations of
SHIP; showing a reduction of goiter, thyroid nodules and hyperthyroidism. Likewise, a decrease
in the incidence of positive autoantibodies to thyroperoxidase (anti-TPO Abs) was observed (16).
Germany and Pakistan present different socioeconomics, cultural values and adaptations to the
IDD eradication but have resemblance in history of iodine deficiency. In the recent years
Germany has improved in IDD eradication more than Pakistan. The purpose of this research was
to study the regional influence on iodine nutritional status of pregnant women in Pakistan and to
monitor the effectiveness of the iodine fortification programme in the North-East German
population.

3
2. Methodology
Our results are based on cross-sectional data obtained from pregnant women in the KPK
province of Pakistan and from the general population of a population based study SHIP− in the
North-East of Germany
2.1. Study Design and Subjects.
2.1.1. Pregnant Women Study Population
Pregnant women data was obtained from randomly selected (public and private) prenatal clinics
in five districts of the KPK province of Pakistan. Women visited there for their routine checkup
between March and September 2012. Data were obtained from almost 250 pregnant women from
each district reaching to a total of 1260 in all five districts.
2.1.2. SHIP Study Population
The SHIP project consists of two population-based cohorts, for which only individuals with
German citizenship and main residency in the study area were recruited. (17) In the first SHIP
cohort; SHIP-0, individuals aged 20-79 years were selected from population registries by a two-
stage cluster sampling method. The net sample (without migrated or deceased persons)
comprised 6265 eligible subjects, of which 4308 (response 68.8%) participated between 1997
and 2001. A separate stratified random sample of 8826 adults aged 20-79 years was drawn for
SHIP-Trend, of which 4420 subjects participated between 2008 and 2012 (response 50.1%) in
SHIP-Trend-0.
All participants gave written informed consent before data collection for pregnant women and
SHIP data. The SHIP study conformed to the ethical guidelines of the Declaration of Helsinki as
reflected in a priori approval by the local ethics committee of the University of Greifswald, while
for the pregnant women study an institutional approval from the academic research committee of
Kohat University of Science and Technology (KUST), Kohat, Pakistan was obtained.
2.2. Exclusion Criteria
Pregnant women with self-reported chronic medical disorders were not included in the study.
The study population available for the final analysis consisted of 1246 pregnant women.

4
For the analysis of monitoring trend of thyroid diseases in SHIP, 36 individuals were excluded
from analysis in SHIP-0 and 13 in SHIP-Trend-0 because of missing data regarding diagnosed
thyroid disorders.
2.3. Assessments in Pregnant Women Population
All the pregnant women were asked to complete a short interview questionnaire containing the
information related to sources and reasons for intake and non-intake of iodized salt. The
questionnaire also comprised questions related to knowledge of iodized salt nutrition.
Information on the number of previous pregnancies and/or abortions (fetal loss due to various
reasons, not including voluntary termination of pregnancy) was also obtained.
The gestational age of the pregnant women was determined from the first day of the last regular
menstrual period with gestational ages of ≤14.9, 28.9, and ≥29 weeks comprising the first,
second, and third trimesters of pregnancy, respectively.
For goiter assessment in pregnant women the WHO/UNICEF/IGN recommended palpation
method was used (18). UIC was measured using a modification of the Sandell-Kolthoff reaction
with spectrophotometric detection. The inter-assay coefficient of variation (CV) was calculated
to be 5.6%. Evaluation of group iodine status was based on median UIC categories defined by
the WHO/IGN (19). These are: recommended – median 150-249 μg/L; mild iodine deficiency –
median <150 μg/L.
2.4. Assessments in the SHIP Population
For the analysis of monitoring trends of thyroid diseases in SHIP, diagnosed thyroid disorders
were assessed by computer-assisted personal interviews. All participants were asked to bring
their medications taken seven days prior to the time of examination. Medication data were
obtained online using the IDOM program (online drug-database leaded medication assessment)
and classified according to the Anatomical-Therapeutic-Chemical (ATC) classification system
(17).
In SHIP population goiter assessment was based on thyroid volume determined with
ultrasonography. Goiter was defined as a thyroid volume exceeding 18 mL in women and 25 mL
in men (20). Urinary iodine concentrations were measured from spot urine samples by a

5
photometric procedure (Photometer ECOM 6122, Eppendorf, Hamburg, Germany) with Sandell
and Kolthoff reaction. The inter-assay coefficient of variation (CV) was calculated to be 5.6%.
Urinary creatinine concentrations were determined with the Jaffé method (SHIP-0: Hitachi 717,
Roche Diagnostics, Germany; SHIP-Trend-0: Dimension Vista, Siemens Healthcare Diagnostics,
Eschborn, Germany). Evaluation of group iodine status was based on median UIC categories
defined by the WHO/IGN (18). The iodine/creatinine ratio was calculated by dividing urinary
iodine by urinary creatinine concentrations.
Serum TSH, fT3, fT4 levels in SHIP study were measured by an immunochemiluminescent
procedure (SHIP-0: LIA-mat, Byk Sangtec Diagnostica GmbH, Frankfurt, Germany; SHIP-
Trend-0: Dimension Vista, Siemens, Eschborn, Germany). The functional sensitivity of the TSH
assay was 0.03 mIU/L (21) for SHIP-0 and 0.005 mIU/L for SHIP-Trend-0 (22). For SHIP-0
coefficients of variation for TSH were 5.0% at 0.3 mIU/L, 3.7% at 16.1 mIU/l, while for SHIP-
Trend-0 these were 2.04% or 2.20% for TSH. A method comparison between the two TSH
laboratory methods showed only negligible differences (23). High and low serum TSH levels
were based on the reference range established from data for SHIP-0 (0.25 mIU/L - 2.12 mIU/L)
and SHIP-TREND-0 (0.49 mIU/L - 3.29 mIU/L) respectively (21,22).
Anti-TPO Abs were measured by an enzyme immunoassay in the whole SHIP study
(VARELISA, Elias Medizintechnik GmbH, Freiburg, Germany). The functional sensitivity of
this assay was 1 IU/ml, and the coefficient of variation over the whole study period was 12%.
The anti-TPO Abs status was defined as follows: normal < 60 IU/ml in men and < 100 IU/ml in
women; increased > 60 IU/ml in men and > 100 IU/ml in women; positive: > 200 IU/ml in both
sexes (24).
2.5. Thyroid Ultrasound
Thyroid ultrasonography was performed in SHIP-0 using an ultrasound VST-Gateway with a 5
MHz linear array transducer (Diasonics, Santa Clara, CA, USA). In SHIP-Trend-0
ultrasonography was performed with a portable device using a 13-MHz linear array transducer
(Vivid-I, General Electrics, Frankfurt, Germany). In both studies intra- and inter-observer
reliabilities were assessed before the start of the study and semi-annually during the study. For
thyroid volume all inter-observer and inter-device variabilities showed mean differences (±2 SD)

6
of < 5% (<25%) (25). Thyroid volume was calculated as length x width x depth x 0.479 (ml) for
each lobe (26). The normal thyroid echo pattern was classified as homogeneous. A homogeneous
echo pattern with reduced echogenicity was defined as hypoechogenic. Nodular changes
exceeding 10 mm in diameter were defined as thyroid nodules.
2.6. Statistical Analysis
Multivariable logistic regression analysis adjusting for age was used to regress the outcome
measures (knowledge about IDD, iodized salt intake, UIC <150mIU/L and goiter prevalence) on
regional influences (as exposure) in each specific district. These results are presented as odd
ratios and their 95% confidence interval.
For the analysis in SHIP, all analyses were standardized by base-weights to account for different
sampling probabilities. In SHIP-Trend-0, additionally, inverse probability weights for study
participation were calculated, which were multiplied with the base-weights. Differences in
median levels between SHIP-0 and SHIP-Trend-0 were tested by median regression models;
prevalence differences between SHIP-0 and SHIP-Trend-0 were tested by Poisson regression
models.
A p-value of <0.05 was considered statistically significant. All analyses were carried out with
Stata 13.1 and 11.2 (Stata Corporation, College Station, TX, USA).
3. Results
3.1. Iodine Nutrition in Pregnant Women and Regional Influence in Pakistan
The majority of pregnant women (88.0%) had no knowledge about IDD (Table 1). A very high
(79%) percentage of pregnant women were not taking iodized salt, out of which 36.6% reported
that iodized salt would negatively affect reproduction and for 17.0%, it was too expensive.
Iodized salt intake in pregnant women was high in the big cities (Peshawar, Nowshehra) and in
the urban areas (27.0%) (Table 1).

7
Table 1. Association of Demographic Characteristics with Iodized Salt Intake, Goiter
Prevalence and UIC <150 µg/L
Characteristic
N=
1246
Iodized salt intake
(n=262; 21.0%)
Goiter prevalence
(n=318; 25.5%)
UIC <150 µg/L
(n=731; 58.7%)
n n (%) P value n (%) P value n (%) P value
District
Lakki
Marwat 244
45 18.4 0.64
44 18.0 0.656
57 23.4 0.096
Karak 252 9 3.6 <0.001 111 44.1 <0.000 208 82.5 <0.001
Kohat 249 27 10.8 <0.001 54 21.7 0.565 165 66.3 <0.001
Nowshehra 251 68 27.1 <0.001 60 23.9 0.244 226 90.0 <0.001
Peshawar 250 113 45.2 Ref 49 19.6 Ref 75 30.0 Ref
Residence
Rural 783 137 17.5 <0.001
209 26.7 0.218
467 59.6 0.364
Urban 463 125 27.0 109 23.5 264 57.0
Knowledge
about IDD
No 1093 147 13.5 <0.001
290 26.5 0.030
659 60.3 0.002
Yes 153 115 75.2 28 18.3 72 47.1
P-value calculated from logistic regression, adjusted for age, (Ref = reference category)
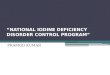
Figure 1. Adjusted Association of Urban-rural Distribution to Various Parameters of Iodine
Deficiency

8
In 41.3% of the pregnant women, we observed a UIC of >150mIU/L. The median UIC level for
the pregnant women was 131µg/L. The total goiter prevalence in pregnant women was 25.5%.
The prevalence of UIC <150mIU/L in pregnant women did not differ between rural and urban
areas (Table 1). The results based on logistic regression analysis shows that the prevalence on
knowledge about IDD, iodized salt intake, UIC <150mIU/L, and goiter did not differ in pregnant
women between urban and rural areas (Figure 1). In district Lakki Marwat except, the pregnant
women from urban residence had higher odds of having knowledge on IDD and iodized salt
intake than their rural counterparts.
3.2. Monitoring the Prevalence of Thryoid Disorders in North-East Germany
The prevalence of diagnosed thyroid disorders increased from 7.6% [CI 6.9-8.5] in SHIP-0 to
18.9% [CI 17.6-20.1] in SHIP-Trend-0 (Table 2). Likewise, the prevalence of thyroid medication
intake increased from 6.2% [CI 5.5-7.0] to 11.1% [CI 10.1-12.2]. The median urinary iodine
excretion levels decreased significantly, which was more pronounced in females than in males
(Table 2). The median iodine-to-creatinine ratio declined in all sex- and age-groups with stronger
decrease in females than in males. The prevalence of median urinary iodine excretion levels
<100µg/L increased between SHIP-0 and SHIP-Trend-0 (Table 2). Median serum TSH levels
increased significantly between SHIP-0 and SHIP-Trend-0, resulting in a right shift of the serum
TSH level distribution (Table2). The prevalence of high serum TSH levels remained almost
stable between SHIP-0 and SHIP-Trend-0. Likewise, the prevalence of low TSH remained
almost stable between SHIP-0 and SHIP-Trend-0. The prevalence of increased anti-TPO Abs
and positive anti-TPO Abs decreased from SHIP-0 to SHIP-Trend-0 in the whole study
population (Table 2). The prevalence of hypoechogenic thyroid pattern decreased from SHIP-0
to SHIP-Trend-0 (Table 2). The median thyroid volume remained similar between SHIP-0 and
SHIP-Trend-0 in the whole study population (Table 2). Goiter prevalence decreased
significantly; more pronounced in males than in females, while the prevalence of thyroid nodules
increased between SHIP-0 and SHIP-Trend-0.

9
Table 2. Change in Thyroid Characteristics between SHIP-0 (1997 - 2001) and SHIP-Trend-0 (2008 - 2012)
All Males Females
SHIP-0 SHIP-Trend-0 p* SHIP-0 SHIP-Trend-0 p* SHIP-0 SHIP-Trend-0 p*
Iodine; µg/l 123.0 (122.5; 123.5) 112.0 (111.5; 112.5) <0.001 134.0 (133.2; 134.8) 126.0 (125.5; 126.5) <0.001 108.0 (107.2; 108.8) 91.9 (91.4; 92.4) <0.001
Iodine to creatinine ratio;
µg/g 130.1 (129.8; 130.4) 113.7 (113.3; 114.0) <0.001 116.2 (115.7; 116.8) 105.8 (105.4; 106.2) <0.001 152.2 (151.4; 153.0) 128.0 (127.2; 128.8) <0.001
Iodine < 100 µg/L; % 37.7 (36.0; 39.5) 43.9 (42.0; 45.7) <0.001 30.5 (28.2; 32.9) 36.2 (33.9; 38.6) 0.001 45.6 (43.0; 48.3) 53.8 (51.0; 56.6) <0.001
Thyroid volume, ml 18.41 (18.36; 18.46) 18.27 (18.24; 18.30) <0.001 21.79 (21.71; 21.87) 20.39 (20.35; 20.44) <0.001 15.31 (15.26; 15.36) 15.43 (15.40; 15.47) <0.001
Goiter; % 35.1 (33.5; 36.7) 29.4 (27.8; 31.0) <0.001 36.5 (34.2; 38.8) 26.6 (24.7; 28.7) <0.001 33.7 (31.5; 36.0) 32.9 (30.4; 35.6) 0.676
Thyroid nodules; % 18.5 (17.3; 19.8) 30.5 (29.0; 32.1) <0.001 14.8 (13.2; 16.7) 24.4 (22.5; 26.4) <0.001 22.5 (20.7; 24.3) 38.4 (35.9; 41.0) <0.001
Hypoechogenic thyroid
pattern; % 5.4 (4.8; 6.2) 3.7 (3.1; 4.4) 0.001 1.8 (1.3; 2.4) 2.6 (1.9; 3.4) 0.113 9.5 (8.1; 11.0) 5.2 (4.1; 6.5) <0.001
Increased anti-TPO
antibodies; % 6.7 (5.8; 7.6) 5.2 (4.5; 6.0) 0.013 3.7 (2.9; 4.8) 3.7 (2.9; 4.7) 0.994 9.9 (8.5; 11.5) 7.1 (5.9; 8.6) 0.007
Positive anti-TPO
antibodies; % 3.9 (3.2; 4.6) 2.9 (2.4; 3.5) 0.022 1.3 (0.9; 1.9) 1.4 (1.0; 2.1) 0.677 6.7 (5.6; 8.1) 4.7 (3.7; 6.0) 0.017
TSH; mIU/L 0.69 (0.68; 0.70) 1.19 (1.18; 1.20) <0.001 0.68 (0.67; 0.69) 1.16 (1.15; 1.17) <0.001 0.71 (0.70; 0.72) 1.24 (1.23; 1.25) <0.001
Increased TSH; % 2.6 (2.1; 3.2) 2.9 (2.4; 3.6) 0.452 1.6 (1.1; 2.4) 2.4 (1.7; 3.3) 0.122 3.7 (2.9; 4.8) 3.6 (2.7; 4.8) 0.960
Decreased TSH; % 6.6 (5.8; 7.5) 6.4 (5.6; 7.3) 0.737 6.7 (5.6; 8.1) 6.4 (5.4; 7.6) 0.684 6.5 (5.4; 7.7) 6.4(5.2; 7.8) 0.940
Dichotomous data is presented as percentage and 95% confidence interval; continuous data as median and 95% confidence; all analyses are weighted by sampling weights; *p-values for differences between the studies are taken from Poisson (dichotomous data) and median regression models (continuous data)

10
4. Discussion
4.1. Iodine Nutrition in Pregnant Women and Regional Influence
The assessment of USI programme success in a population is based on the indicators of iodine
deficiency, which includes awareness in the public, iodized salt intake rate, urinary iodine
excretion levels and goiter prevalence (18) apart from more advanced parameters. The awareness
campaign on IDD and iodized salt consumption in Pakistan was poorly managed in the past
decade. It faced challenges at two fronts. First the effects of historical advertisement mistake (27)
leading to misconception about iodized salt, still exist. Second, there was a lack of locally
adoptive scientific interventions in campaigning (28). This can be clearly seen in our results
where only 13% pregnant women were aware about the IDD and iodized salt. In line with
previous studies (29,30) from Pakistan, the frequency of using iodized salt is far lower than the
international recommendations (18). Regarding UIC, in concordance with the results of a
previous study for our study region (31), the median UIC of 131 µg/L indicating a mild iodine
deficiency in pregnant women. The prevalence of goiter is in consonance with previous studies
conducted in the same region in school aged children (32,33).
In spite of huge differences in the urban and rural disparity index in Pakistan (KPK in particular)
(9), the odds for having greater knowledge about IDD, iodized salt intake, prevalence of UIC
<150mIU/L and goiter prevalence did not differ among urban and rural pregnant women.
Although due to ease availability and preference of selling in the urban areas in the big towns,
iodized salt intake in consonance with national nutrition survey 2011 (31) was higher.
Consequently goiter prevalence was lower in the urban than in the rural areas, although we could
not observe a significant difference in UIC among pregnant women from rural and urban origin.
The high goiter prevalence in district Karak is a result of low intake of iodized salt, geography
and previous history. The higher odds of rural pregnant women than the urban; to have
knowledge on IDD and having higher iodized salt intake in Lakki Marwat district may be related
to higher rural health standards and differences in rural/urban health care providers in
comparison to other districts (34). The lower goiter prevalence in this district may be because of
an already high intake of iodized salt, with the possibility of higher natural soil iodine in the

11
drinking waters and to the higher iodine contents in the sedimentary rock formation of district
Lakki Marwat (35,36).
4.2. Monitoring the Prevalence of Thyroid Disorders in North-East Germany
A general decline in IDD was observed during the last decade in the North-East German
population, in spite that an increase was observed in the self-reported diagnosed thyroid
disorders and treatments by thyroid medication. The increase in self-reported diagnosed thyroid
disorders and treatments by thyroid medication may be due to following factors apart from
increased awareness. First, due to therapeutic misjudgment prescription of thyroxine for non-
thyroid indications may not be ruled out, as observed in the Framingham (37) and DanThyr
studies (38). Second, it may be because of the wrong use of TSH reference intervals obtained
from the data in SHIP-0. Additionally, the different devices used in ultrasound for examination
of thyroid nodules in the two cohorts render non-comparable results. So, the probable increase in
prescription rate of thyroxine for the treatment of thyroid nodules in SHIP-Trend-0 may also not
be ruled out entirely.
In line with a general decline reported across Germany (39), a slight decline was observed in the
median iodine excretion levels between SHIP-0 and SHIP-Trend-0, but importantly without
detrimental effects. Median iodine excretion levels were lower in females (particularly in
younger women) than in males in both studies. A greater than normal intake of water will
increase the urine volume, leading to lower urinary creatinine and lower iodine concentrations,
but usually will not reduce the amount of creatinine excreted daily (40). Thus, the
iodine/creatinine ratio adjusts for differences in fluid intake and may provide a better estimate of
the true iodine intake in young females. On the other hand, there was a marginal but significant
increase in median thyroid volume in women, while goiter prevalence remained nearly
unchanged. In contrast thyroid volume and goiter prevalence decreased in men. This sex-
specific difference may be explained by a suboptimal iodine status in women compared to men.
When improving iodine supply there is always a risk to overcompensate, which may result in a
higher prevalence of hypothyroidism and thyroid antibodies. However, it depends on the pattern
of supplementation. A sudden, strong or periodic increase in iodine intake may provoke the
formation of thyroid antibodies and hypothyroidism, while a consistently optimal iodine intake,

12
like in our study (14,16) and in a Chinese study (15) does not. The former effect was observed in
studies from Denmark and Slovenia (41,42). Rather, we observed a decrease in the prevalence of
elevated and positive anti-TPO Abs between SHIP-0 and SHIP-Trend-0, which along with
equilibrium in prevalence of hypo- and hyperthyroidism argue for an optimal iodine supply in
our study region over the past two decades. It is evident that the current and history of iodine
supply to a region determines the distribution of TSH values of the population (24). Going
through transition in iodine supply from deficiency to sufficiency− accordingly TSH distribution
may shift from left to right if the iodine supply is persistent (21,22). We assume that the change
in TSH distribution we observed is mainly related to the improved iodine supply. A similar
association has been previously reported for the Danish population (43).
4.3. The Common Lessons
The IDD prevention programme of Germany comparatively presents a good example for
Pakistan to adopt, in order to reduce the long-term effects of iodine deficiency in the general
population. The IDD prevention programme in Germany has improved in many aspects in almost
the same time period since Pakistan adopted the USI programme (6,14). Germany has adopted a
nationwide uniform legislation for the IDD prevention (13). The IDD prevention programme is
regularly monitored by the nationwide studies in children, adolescent and adults [Studie zur
Gesundheit von Kindern und Jugendlichen in Deutschland (KIGGS) (13) and Studie zur
Gesundheit Erwachsener in Deutschland (DEGS) (12) and regional studies such as SHIP
(14,16,44). Furthermore, there is central advisory body Arbeitskreis Jodmangel, which provides
support through intensive educational work and with the help of service material for
professionals and end users in improving iodine supply and further to raise awareness of thyroid
health (45). However, Germany is lacking in studies on iodine deficiency effects on pregnant
women and neonates. Also options to control the effectiveness of IDD prevention is hampered
by limited or even not at all possible access to valid information on incident thyroid diseases,
treatments and costs in the national health-care system.
On Pakistani side, in spite of implementation problems, lots of effort on the iodized salt
production and supply have been made (46). There is a strong network present for the IDD
control at the national, provincial and district level (46). However, due to lack of proper
planning, political will, and monitoring as well as myths regarding iodized salt and

13
socioeconomics, the benefit to the end user is still impending (6). The “IDD control bill 2009” is
still awaiting approval from the national parliament, while provinces have differential adaptation
of pre-existing laws (6). The monitoring of IDD control programme is poorly managed. There is
no existence of national or regional monitoring studies and monitoring mechanism are affected
by insufficient resources; over-reliance on spot-test results; insufficient consideration of quality
assurance systems; and poorly established study protocols, laboratory resources, and expertise
(6,46). In spite of quantitative and qualitative differences in IDD prevention programme both
countries have a lot of space to work on many fronts regarding iodine deficiency elimination.
This may be in the form of utilizing expertise from Germany to assess prevalence and incidence
of common risk factors, subclinical disorders and clinical diseases related to thyroid dysfunction
and to investigate associations and interactions among them and with other disorders. From
Pakistan; due to lacking previous studies, qualitative data may be produced to look for the course
of iodine deficiency related disorders in general and targeted populations. Quality of data
collection may be optimized and standardized according to the German standards.
From future perspective both the countries need registry data for thyroid related outcomes,
regarding health care patterns, decision making, and delivery, as well as the subsequent
association of these factors with patient outcomes. There is dire need for cost effective analysis
of IDD prevention programme to adopt systematic approach for balancing resource implications
(cost) against results (effectiveness) of alternatives and is preferable to other approaches such as
gut feelings, or educated guesses. The results of cost effective analysis will provide decision
makers with information on costs, effectiveness, and the relationship between the two (i.e., the
value attained). A central advisory board with updated knowledge funded from public sources
may be established to give recommendation to the governmental authorities, general public for a
sustained programme for the elimination of IDD. Coordinated information campaigns organized
by central agencies are very important to bring awareness in public about the health benefits of
iodized salt, and health implications of iodine deficiency. The most important aspect may be to
develop a political will by enhancing the awareness among the politicians who may directly
influence the policy making infrastructure. A sustained programme is needed for the elimination
of IDD, as IDD is not a condition like smallpox, for which when once virus is removed would
not emerge again. Unless effective dietary supplementation programs are sustained, the people of
these regions will continue to suffer iodine deficiency disorders.

14
4.4. Strengths and Limitations
For the first time the iodine nutritional status with its regional effects was reported from
socioeconomically deprived districts with the largest study population of pregnant women in
Pakistan. Strengths of the SHIP data are the population based design, and that both SHIP studies
were conducted in nearly the same study regions ten years apart. In both SHIP studies
examinations were executed in the same laboratory with a common approach to high
standardization of measurements.
Our data from Pakistan was limited by not providing the personal educational level, occupation,
socioeconomic status and receiving or not receiving health and prenatal care. Further we had not
assessed iodine in salt due to resource limitations. In the SHIP studies different thyroid ultrasound
devices were used, which particularly led to a higher detection rate of thyroid nodules in SHIP-TREND-0
than in SHIP-0. In SHIP-Trend-0, we had no data on fT3 and fT4, making it impossible to distinct overt
and subclinical forms of thyroid dysfunction. Additionally, results may be affected by selection bias as
the participation reduced to 50.1%, in SHIP-Trend-0 as compared to 68.8% in the baseline cohort.
Though inverse probability weights were calculated for SHIP-Trend-0 study participation and used
multiplicatively to the base-weights to reduce selection bias. We present our results on the basis of
cross sectional data− of which we cannot draw causal inference.
5. Conclusion
In pregnant women in Pakistan due to insufficient awareness campaigns and low literacy ratio in
rural areas urinary iodine excretion levels indicate a stable iodine supply, which is still not
sufficient. Our results show that rural/urban disparity is affecting the IDD prevention program in
rural districts, but not in general. The SHIP data indicate that the improved iodine supply over
the past two decades in Germany is paralleled by a reduction in prevalence of IDDs, while no
increase was observed in markers of autoimmune thyroid disorders arguing for an optimal iodine
supply of the general adult population in Northeast Germany. The increase in prevalence of
diagnosed thyroid disorders and the intake of thyroid medication might be because of
inappropriate therapeutical decisions which should be made with caution, based on regional TSH
reference ranges, its prognostic value, and compliance with treatment.

15
6. Literature Cited
1. Delange F, B H. The iodine deficiency disorders. In: DeGroot LE, Hannemann G, eds
The thyroid and its diseases.http://www.thyroidmanager.org/Chapter20/20-frame.htm.
Accessed 17-10-2017, 2017.
2. Zimmermann MB, Jooste PL, Pandav CS. Iodine-deficiency disorders. The Lancet.
2008;372(9645):1251-1262.
3. De Escobar GM, Obregón MJ, Del Rey FE. Role of thyroid hormone during early brain
development. European Journal of Endocrinology. 2004;151(Suppl 3):U25-U37.
4. Pharoah P, Buttfield I, Hetzel B. Neurological damage to the fetus resulting from severe
iodine deficiency during pregnancy. The Lancet. 1971;297(7694):308-310.
5. Dillon J, Milliez J. Reproductive failure in women living in iodine deficient areas of West
Africa. BJOG: An International Journal of Obstetrics & Gynaecology. 2000;107(5):631-
636.
6. Khattak RM, Khattak MNK, Ittermann T, Völzke H. Factors affecting sustainable iodine
deficiency elimination in Pakistan: A global perspective. Journal of Epidemiology. 2017.
7. McCarrison R. Observations on endemic cretinism in the Chitral and Gigit valleys. The
Lancet. 1908;172(4444):1275-1280.
8. ICCIDD. Striking progress against IDD in Pakistan; 50% decrease in iodine deficiency
in children over the past decade. 2013.
9. Rahman A, Hayat Y, Habib Z, Iqbal J. Rural-Urban Disparities in Khyber Pakhtunkhwa
Pakistan. Sarhad J Agric. 2011;27:477-483.
10. Delavande A, Zafar B. Gender discrimination and social identity: experimental evidence
from urban Pakistan. 2013.
11. Glinoer D. The regulation of thyroid function during normal pregnancy: importance of
the iodine nutrition status. Best Practice & Research Clinical Endocrinology &
Metabolism. 2004;18(2):133-152.
12. Meng W, Scriba P. Jodversorgung in Deutschland Probleme und erforderliche
Massnahmen: Update 2002. DEUTSCHES ARZTEBLATT-KOLN-. 2002;99(39):2048-
2048.

16
13. Thamm M, Ellert U, Thierfelder W, Liesenkotter KP, H V. [Iodine intake in Germany.
Results of iodine monitoring in the German Health Interview and Examination Survey for
Children and Adolescents (KiGGS)]. Bundesgesundheitsblatt Gesundheitsforschung
Gesundheitsschutz. 2007;50(5-6):744-749.
14. Völzke H, Lüdemann J, Robinson DM, Spieker KW, Schwahn C, Kramer A, John U,
Meng W. The prevalence of undiagnosed thyroid disorders in a previously iodine-
deficient area. Thyroid. 2003;13(8):803-810.
15. Teng W, Shan Z, Teng X, Guan H, Li Y, Teng D, Jin Y, Yu X, Fan C, Chong W. Effect
of iodine intake on thyroid diseases in China. New England Journal of Medicine.
2006;354(26):2783-2793.
16. Völzke H, Ittermann T, Albers M, Friedrich N, Nauck M, Below H, Kramer A. Five-year
change in morphological and functional alterations of the thyroid gland: the Study of
Health in Pomerania. Thyroid. 2012;22(7):737-746.
17. John U, Hensel E, Lüdemann J, Piek M, Sauer S, Adam C, Born G, Alte D, Greiser E,
Haertel U. Study of Health In Pomerania (SHIP): a health examination survey in an east
German region: objectives and design. Sozial-und Präventivmedizin. 2001;46(3):186-194.
18. WHO, ICCIDD, UNICEF. Assessment of iodine deficiency disorders and monitoring
their elimination: a guide for programme managers. Geneva: WHO;2007.
19. WHO/ICCIDD/UNICEF. Assessment of iodine deficiency disorders and monitoring their
elimination: a guide for programme managers. Geneva. Genava: World Health
Organization;2007.
20. Gutekunst R BW, Hehrmann H, Olbricht W, Pfannenstiel P. Ultrasonic diagnosis of the
thyroid gland. DMW. 1988;113:1109-1112.
21. Völzke H, Alte D, Kohlmann T, Lüdemann J, Nauck M, John U, Meng W. Reference
intervals of serum thyroid function tests in a previously iodine-deficient area. Thyroid.
2005;15(3):279-285.
22. Ittermann T, Khattak RM, Nauck M, Cordova CM, Völzke H. Shift of the TSH reference
range with improved iodine supply in Northeast Germany. European journal of
endocrinology. 2015;172(3):261-267.

17
23. Ittermann T, Khattak RM, Nauck M, Cordova CMM, Völzke H. Shift of the TSH
reference range with improved iodine supply in Northeast Germany. European Journal of
Endocrinology. 2015;172(3):261-267.
24. Völzke H, Ludemann J, Robinson DM, Spieker KW, Schwahn C, Kramer A, John U,
Meng W. The prevalence of undiagnosed thyroid disorders in a previously iodine-
deficient area. Thyroid. 2003;13(8):803-810.
25. Völzke H, Werner A, Wallaschofski H, Friedrich N, Robinson DM, Kindler S, Kraft M,
John U, W H. Occupational exposure to ionizing radiation is associated with autoimmune
thyroid disease. J Clin Endocrinol Metab. 2005;90:4587-4592.
26. Brunn J BU, Ruf G, Bos I, Kunze WP, PC S. Volumetric analysis of thyroid lobes by
real-time ultrasound. DMW. 1981;106:409-414.
27. Leiby R. Salt rumors add to health crisis in Pakistan:
https://www.washingtonpost.com/world/asia_pacific/salt-rumors-add-to-health-crisis-in-
pakistan/2012/12/30/bb5f5e48-4619-11e2-8c8f-fbebf7ccab4e_story.html. The
Washington Post. 31 December 2012, 2012.
28. Lowe N, Westaway E, Munir A, Tahir S, Dykes F, Lhussier M, McKeown M,
Zimmerman M, Andersson M, Stinca S. Increasing Awareness and Use of Iodised Salt in
a Marginalised Community Setting in North-West Pakistan. Nutrients. 2015;7(11):9672-
9682.
29. Elahi S, Rizvi NB, Nagra SA. Iodine deficiency in pregnant women of Lahore. J Pak
Med Assoc. 2009;59(11):741-743.
30. Saeed M, Yaqub M, Roohi M, Ashraf M. Prophylactic use of iodized salt in pregnancy.
Professional. 2000;7(1):66-69.
31. National Nutrition Survey (NNS). Aga Khan University, Pakistan Medical Research
Council (PMRC) and the Nutrition Wing, Ministry of Health, Pakistan;2011.
32. Jahangir M, Khattak R, Shahab M, Tauseef I, Khattak M. Prevalence of goiter and iodine
nutritional status in School-age Children of District Karak, Khyber Pakhtunkhwa,
Pakistan. Acta Endocrinologica (1841-0987). 2015;11(3).
33. Subhan F, Jahangir M, Saira S, Khattak RM, Shahab M, Haq M, Khattak MNK.
Prevalence of goiter and iodine status among 6-12 years school age children in district
Kohat, Pakistan. South East Asia Journal of Public Health. 2015;4(2):42-46.

18
34. Khyber Pakhtunkhwa: Health Sector Situation Analysis. Peshawar: Government of
Khyber Pakhtunkhwa;2010.
35. Johnson CC. The geochemistry of iodine and its application to environmental strategies
for reducing the risk from iodine deficiency disorders (IDD). UK: British Geological
Survey;2003. DfID KAR Project R7411.
36. Hemphill WR, Kidwai AH. Stratigraphy of the Bannu and Dera Ismail Khan areas,
Pakistan. USA: United States Department of the Interior: Geological Survey 1973. 2330-
7102.
37. Sawin CT, Geller A, Hershman JM, Castelli W, Bacharach P. The aging thyroid: the use
of thyroid hormone in older persons. Jama. 1989;261(18):2653-2655.
38. Cerqueira C, Knudsen N, Ovesen L, Laurberg P, Perrild H, Rasmussen LB, Jørgensen T.
Doubling in the use of thyroid hormone replacement therapy in Denmark: association to
iodization of salt? European journal of epidemiology. 2011;26(8):629-635.
39. Johner SA, Thamm M, Schmitz R, Remer T. Examination of iodine status in the German
population: an example for methodological pitfalls of the current approach of iodine
status assessment. European journal of nutrition. 2015:1-8.
40. Andersen SL, Møller M, Laurberg P. Iodine concentrations in milk and in urine during
breastfeeding are differently affected by maternal fluid intake. Thyroid. 2014;24(4).
41. Pedersen IB, Knudsen N, Carlé A, Vejbjerg P, Jørgensen T, Perrild H, Ovesen L,
Rasmussen LB, Laurberg P. A cautious iodization programme bringing iodine intake to a
low recommended level is associated with an increase in the prevalence of thyroid
autoantibodies in the population. Clinical endocrinology. 2011;75(1):120-126.
42. Zaletel K, Gaberšček S, Pirnat E, Krhin B, Hojker S. Ten-year follow-up of thyroid
epidemiology in Slovenia after increase in salt iodization. Croatian medical journal.
2011;52(5):615-621.
43. Laurberg P, Pedersen KM, Hreidarsson A, Sigfusson N, Iversen E, Knudsen PR. Iodine
intake and the pattern of thyroid disorders: a comparative epidemiological study of
thyroid abnormalities in the elderly in Iceland and in Jutland, Denmark. The Journal of
Clinical Endocrinology & Metabolism. 1998;83(3):765-769.

19
44. Khattak RM, Ittermann T, Nauck M, Below H, Völzke H. Monitoring the prevalence of
thyroid disorders in the adult population of Northeast Germany. Population health
metrics. 2016;14(1):39.
45. Arbeitskreis Jodmangel e.V. (AKJ): http://jodmangel.de/. 2017. Accessed 23.11.2017,
2017.
46. Masuood AK, Janjua TA. Achieving Universal Salt Iodisation (USI) in Pakistan:
Challenges, Experiences and the Way Forward. IDS Bulletin. 2013;44(3):57-65.

20
7. Scientific work
Article in Final Editor Review of “Thyroid”
7.1. Regional Influence on Iodine Nutritional Status of Pakistani Pregnant Women
Rehman Mehmood Khattak1, 6, Zuhra Saifullah2, Ghulam Khadija3, Amina Fayyaz3, Salma
Zaman4, Mahwish Gul4, Muhammad Nasir Khan Khattak5, 7, Birgit Schauer1, Henry Völzke1,
Till Ittermann1,
1Institute for Community Medicine, University Medicine Greifswald, Germany,
2Department of Zoology, University of Peshawar, Pakistan,
3Department of Zoology, Kohat University of Science and Technology (KUST), Kohat, Pakistan,
4Department of Animal Sciences, Quaid-i-Azam University Islamabad, Pakistan,
5Department of Zoology, University of Hazara, Mansehra, Pakistan,
6Department of Zoology, Islamia College Peshawar (CU), Pakistan,
7Department of Applied Biology, University of Sharjah, Sharjah, United Arab Emirates
Short running title: Iodine Nutritional Status in Pregnancy in Pakistan
Keywords: Iodine Deficiency Disorder, Pregnancy, Goiter Prevalence, Iodized Salt, Pakistan

21
Regional Influence on Iodine Nutritional Status of Pakistani Pregnant Women
Rehman Mehmood Khattak1, 6, Zuhra Saifullah2, Ghulam Khadija3, Amina Fayyaz3, Salma
Zaman4, Mahwish Gul4, Muhammad Nasir Khan Khattak5, 7, Birgit Schauer1, Henry Völzke1,
Till Ittermann1
1Institute for Community Medicine, University Medicine Greifswald, Germany, 2Department of
Zoology, University of Peshawar, 3Department of Zoology, Kohat University of Science and
Technology (KUST), Kohat, Pakistan, 4Department of Animal Sciences, Quaid-i-Azam
University Islamabad, 5Department of Zoology, University of Hazara, Mansehra, Pakistan,
6Department of Zoology, Islamia College Peshawar (CU), Pakistan, 7 Department of Applied
Biology, University of Sharjah, Sharjah, United Arab Emirates .
Short running title: Iodine Nutritional Status in Pregnancy in Pakistan
Keywords: Iodine Deficiency Disorder, Pregnancy, Goiter Prevalence, Iodized Salt, Pakistan

22
Abstract
Background
Keeping the rural-urban disparities in Pakistan in mind, this study aimed at assessing the regional
influence on nutritional iodine status of pregnant women, the most vulnerable group for iodine
deficiency.
Methods
Data were collected from 1246 pregnant women in all trimesters of pregnancy who visited pre-
natal clinics for routine checkups in five districts of the Khyber Pakhtunkhwa province.
Information on iodized salt intake and knowledge on iodine deficiency disorders (IDD) were
obtained through an interview questionnaire. Goiter and urinary iodine excretion levels were
assessed by the palpation method and the Sandell-Kolthoff reaction, respectively. Logistic
regression analysis was used for quantifying an association of residence (rural/urban), trimester
of pregnancy and previous abortion on the outcomes; knowledge about IDD, iodized salt intake,
presence of goiter and urinary iodine concentration (UIC) <150 μg/L.
Results
Overall, 87.7% of pregnant women had no knowledge about IDD, while only 21.0% were taking
iodized salt. Goiter prevalence in pregnant women was 25.5% and an UIC >150 μg/L was
observed in 41.3%. There were no significant differences between pregnant women from rural
and urban settings in regions with a solid socioeconomic status with respect to knowledge on
IDD, iodized salt intake, iodine deficiency and prevalence of goiter. Urban/rural differences were
observed only in socioeconomically deprived districts. Only in the district Lakki Marwat,
pregnant women from urban regions had higher odds of having knowledge on IDD and iodized
salt intake than those from rural regions. Trimesters of pregnancy and previous abortions of
pregnant women had no significant effect on the outcome measures.
Conclusions
UIC levels indicate a stable (in comparison to the national nutrition survey from 2011) but
mildly deficient iodine supply, while goiter prevalence and lack of iodized salt intake remain

23
high, especially in rural areas. Rural/urban disparities were observed only in socioeconomically
deprived districts, which limit the effectiveness of the IDD prevention program in rural areas in
Pakistan. The results suggest that the implementation of mandatory salt iodization needs to be
improved and the program’s effectiveness monitored to protect pregnant women from the
adverse health effects of sub-optimal nutritional iodine status.

24
Introduction
Pakistan is a country with endemic iodine deficiency resulting in high goiter prevalence (1, 2). A
program for the control of iodine deficiency disorders (IDD) has been adopted since 1994.
Although the iodization of salt is mandatory in the country according to the partially
implemented, drafted “IDD control bill 2009” (3), but its implementation is not regulated and
there is no regular monitoring of the program’s effectiveness (1). For these reasons, 20-50% of
all school-aged children suffer from goiter in certain areas (4-6). The Khyber Pakhtunkhwa
(KPK) province located in the Northwest is the most endemic IDD region in Pakistan, where the
prevalence of goiter is not consistent with the reported household usage of iodized salt (1).
Iodine deficiency in women of reproductive age is a big issue in Pakistan. The results of
the national nutrition survey in 2011 revealed that 48% of all 1460 women of reproductive age
(15-49 years) had less than the recommended urinary iodine concentration (UIC) of 100 µg/L,
while in the KPK province this prevalence was even lower (23.9%) (7). The median UIC of
women of reproductive age was 104 μg/L, whereas the median reported from KPK was 148.6
μg/L. In a recent study in pregnant women (n=202) (4) from the Charsadda district located in the
Peshawar valley the overall goiter prevalence was 20.7%, while median UIC was only 89.5
µg/L, which is far below the WHO recommended level of 150 µg/L (8). It is a common issue of
IDD surveys in Pakistan, that remote and rural districts are not covered resulting in biased
estimates about the progress in the correction of IDD (1). Our study includes data from two
districts located in the Peshawar valley (Peshawar and Nowshehra) (9) and three other districts
(Kohat, Karak and Lakki Marwat) not being part of the Peshawar valley. These five districts
represent a good cross section in terms of urbanization, topography, socioeconomics and
potential environmental threats to natural soil iodine including floods, drought, intense rainfall,
earthquake and cyclones (7, 9-12). The previous study performed in Charsadda did not focus on
regional effects on the nutritional iodine status of pregnant women. In the previous study the
study population (202) was very small, while in our study 1246 pregnant women were included.
In comparison to the previous study, we enrolled more parameters to improve the understanding
of potential causes underlying iodine deficiency.
During pregnancy, iodine supplementation is very important because more iodine is
required due to an increased renal clearance of iodide in early gestation, which persists until birth

25
of the child (13, 14). It is recommended that iodine intake should be optimized before or early in
pregnancy to prevent fetal damage. An optimal iodine intake is not only needed for maintaining
maternal euthyroidism, but is also needed for fetal thyroid hormone production and brain
development (8, 13). The WHO, the Iodine Global Network (IGN), and UNICEF, agreed on a
recommended daily allowance of 250 µg/day for pregnant women compared to 150 µg/day for
non-pregnant women (8). A median UIC of 150-249 µg/L is recommended by WHO as an
indicator of adequate iodine intake in pregnant women. In countries or regions where 90% of
households are using iodized salt and the median UIC in school-age children is around 100 µg/L,
WHO recommends iodine supplementation in pregnancy and infancy (8).
The Pakistani society is exposed to disparities between genders, regions, societal,
socioeconomic, and educational factors, which can affect health outcomes. Apart from
differences in living standards, these disparities also trigger migration from rural to urban areas
(15). A recent survey reported significantly higher disparities between rural and urban areas for
both genders, education, livelihood, health services, and sanitation in KPK (16). The observed
sex disparity highlights social and economic dominancy of men in families located in rural
regions, whereas individuals from urban regions had better education and education facilitation
related to infrastructure and quality (particularly at grade 10 and above). Furthermore, the quality
of infrastructure, housing, health services, drinking water supply, transportation, communication
and sanitation were also better in urban areas compared to rural regions.
The purpose of this study was to evaluate the nutritional iodine status of pregnant women
and associated factors with particular emphasis on differences between rural and urban residents
who live in a province with endemic iodine deficiency.
Materials and Methods
Study Area
This study was conducted in five districts of the KPK province in northwestern Pakistan (Figure
1). A choropleth map of the study region was created using ArcGIS for Desktop 10.3.1.

26
Study Design and Subjects
This cross-sectional study was conducted in randomly selected (public and private) prenatal
clinics in the selected districts. If private clinics declined to participate, the data collection was
restricted to public clinics only. The details of the data collection with name of the clinic, its
official status and number of participants is given in supplementary table 1. The details of the
public health care delivery units were obtained from the office of district health officers. In KPK,
maternal care is provided by three tiers of the public health delivery system: the primary health
care units (basic health units, rural health centers), the secondary care hospitals [district and
tehsil (administrative sub-division of the district) headquarter hospitals], and the tertiary
care/teaching hospitals and mother and child care centers (11).
Data were collected from pregnant women, who visited prenatal clinics for their routine
checkup between March and September 2012. From every district, data were collected from a
subtotal of almost 250 pregnant women reaching to a total of 1260 including participants from
all five districts. Pregnant women with self-reported chronic medical disorders such as
hypertension, diabetes mellitus, tumors, renal diseases, with regular use of any medication and
with history of blood borne diseases were not included in the study. The proportion of pregnant
women who declined to participate was not recorded. After exclusion of 14 individuals with
insufficient amount of urine for UIC analysis, the final study population consisted of 1246
pregnant women.
The gestational age was determined by the gynecologists in antenatal clinics based on the
last menstrual period. Gestational age was calculated from the first day of the last menstrual
period with gestational ages of ≤14.9, 14.9 to 28.9, and ≥29 weeks comprising the first, second,
and third trimesters of pregnancy, respectively. Information on the number of previous
pregnancies and/or abortions (fetal loss due to various reasons, not including voluntary
termination of pregnancy) was obtained. A written informed consent was obtained from each
participant before data collection. An institutional academic research committee approval of
Kohat University of Science and Technology (KUST), Kohat, Pakistan was obtained for this
study.

27
Iodized Salt Intake and Knowledge
All participants were asked to complete a short interview questionnaire containing questions
related to iodized salt intake. The questionnaire comprised questions related to knowledge on
iodized salt consumption and on health implications associated with inadequate intake of iodized
salt. It further included questions regarding knowledge about IDDs, sources for the input of
knowledge about IDD including media, doctors, or schools. In Pakistan the universal salt
iodization (USI) program has been affected by lack, uniformity of awareness and misconceptions
about IDDs and iodized salt (1). Thus, knowledge about IDD and iodized salt affects the
utilization of iodized salt, UIC levels, and goiter prevalence. Questions related to nutritional
practices focused on intake of iodized salt, identification of sources of iodized salt, and reasons
for or against utilization of iodized salt.
Urinary Iodine Concentration
The participants were asked to give a urine sample in the vicinity of the antenatal care unit. A
total of 1246 urine samples (≈ 2 ml) were collected in tight screw-capped plastic bottles. Each
bottle was labeled with a sample number, name of the district, name of the antenatal care unit,
and time and date of urine collection. The urine samples were kept in a cool dry box and
transported to the Institute of Radiotherapy and Nuclear Medicine (IRNUM), Peshawar, where
the samples were chilled at 4ºC until urinary iodine analysis. UIC was measured using a
modification of the Sandell-Kolthoff reaction with spectrophotometric detection. The inter-assay
coefficient of variation (CV) was calculated to be 5.6%. Evaluation of iodine status was based on
median UIC categories defined by the WHO/IGN (8). These are: recommended – median 150-
249 μg/L; mild iodine deficiency – median <150 μg/L.
Goiter Assessment
For goiter assessment the WHO/UNICEF/IGN recommended palpation method was used. All the
pregnant women were examined for the presence of palpable goiter as follows. No palpable and
visible goiter was graded as 0. Palpable but no visible goiter was graded as I, and palpable and
visible goiter as Grade II. Palpation examination was carried out by trained examiners in all the
districts, who were trained in the central laboratory of Kohat University of Science and

28
Technology (KUST), Kohat, Pakistan. The severity of the goiter prevalence in the whole study
area and the concerned district was outlined based on the recommended WHO/IGN criteria (8).
Statistical Analysis
Categorical data are presented as absolute numbers and percentages, while continuous data are
presented as absolute numbers and mean or median. Analyses were carried out to identify
differences in iodine deficiency between the urban/rural distribution, trimesters, and previous
abortions among pregnant women of each district. Multivariable logistic regression analysis
adjusting for age was used to regress the outcome measures (knowledge about IDD, iodized salt
intake, UIC <150 µg/L and goiter prevalence) on regional influences (as exposure) in each
specific district. These results are presented as odd ratios and their 95% confidence intervals. A
p-value of <0.05 was considered statistically significant. All analyses were carried out with Stata
11.2 (Stata Corporation, College Station, TX, USA)
Results
The description and location of the studied districts (7, 10-12, 17) is given in Table 1 and Figure
1. The mean age of pregnant women was 27.1 years (age range: 15-50 years) (Table 2). The
baseline characteristics and numbers of studied pregnant women in all the districts are
summarized in tables 2 and 3.
Knowledge about IDD
The majority of pregnant women (88.0%) had no knowledge about IDD (Table 3). Interestingly,
13.5% of pregnant women were utilizing iodized salt despite of the fact that they had no
knowledge about IDD. The major sources of awareness about IDD for the pregnant women were
printed or electronic media (37.3%), schools (19.0%), and doctors (16.3%) (Supplementary table
2). While explaining the reason for taking iodized salt, 50.8% pregnant women reported that they
were taking it for better health, while 20.6% were taking iodized salt because of its better taste
and 13.7% because of family preferences (Supplementary table 3). When asked about the
definition of better health, 46.6% of pregnant women replied that it inhibits goiter development

29
and 12.0% reported it prevents IDD in general. However, 24.8% of the pregnant women taking
iodized salt for better health could not define better health. Among the 79% of the pregnant
women not taking iodized salt, most of them (44.5%) could not state any reasons for not taking
iodized salt, while 36.6% reported that it negatively affects reproduction, and for 17.0% iodized
salt was too expensive (Supplementary table 3).
The results based on logistic regression analysis show that; except for Lakki Marwat
district, the odds of having knowledge about IDD did not differ between rural and urban
pregnant women (Figure 2). In Lakki Marwat district, the pregnant women from urban residence
had higher odds of having knowledge on IDD than their rural counterparts.
Iodized Salt Intake
Around 79.0% pregnant women were not taking iodized salt (Table 3). Iodized salt intake in
pregnant women was higher in the big cities (Peshawar, Nowshehra) than in the smaller ones.
The highest intake was reported from Peshawar district (45.2%) and the lowest intake of iodized
salt was observed in Karak district (3.6%). In comparison to Peshawar iodized salt intake was
significantly lower in pregnant women in all other districts.
Frequencies of iodized salt intake were not significantly different between the first and
the other trimesters of pregnancy (Table 3). Similarly, iodized salt intake of pregnant women did
not differ significantly if they had a history of a previous abortion.
Iodized salt intake was higher in urban than in rural pregnant women, but this difference
was except for the Lakki Marwat district not statistically significant (Figure 2).
Urinary Iodine Concentration
In 41.3% of the pregnant women, we observed a UIC of >150 µg/L (Table 3). The median UIC
level for the pregnant women was 131 µg/L. The prevalence of UIC <150 µg /L was
significantly higher among pregnant women in the Nowshehra, Karak and Kohat districts in
comparison to Peshawar. The prevalence of UIC <150 µg/L in pregnant women did not differ in
rural and urban areas (Table 3). Similarly, the odds of having UIC <150 µg/L was not different
between rural and urban areas in all the districts (Figure 2). However, in Nowshehra district it
barely missed statistical significance. Knowledge about IDD was a contributory factor in

30
overcoming iodine deficiency. Pregnant women who had knowledge about IDD had a
significantly lower prevalence of UIC <150 µg/L (Table 3). The frequency of UIC <150 µg/L
was not significantly different among the pregnant women in all the three trimesters of
pregnancy. Previous abortion of pregnant women was not a determining factor for iodine
deficiency.
Goiter Prevalence
The goiter prevalence in pregnant women was 25.5%. Goiter prevalence was lowest in the Lakki
Marwat and Peshawar district (Table 3). A goiter prevalence of 44.1% was measured in the
Karak district, which was significantly higher than in Peshawar district (19.6%). There was no
significant difference in goiter prevalence of rural compared to urban pregnant women (Table 3).
Consistent with these findings, the odds of having a goiter were not different between women
from urban and rural areas (Figure 2).
Discussion
The present study was conducted to evaluate the rural/urban differences in nutritional iodine
status among pregnant women in the KPK province of Pakistan. Overall, there was mild iodine
deficiency among pregnant women. In a country with a history of iodine deficiency, urban
residence and awareness about IDD were associated with iodine sufficiency among pregnant
women.
Effective public health mass media campaigns are dependent on the literacy ratio of the
community, the medium of marketing and the quality of the message (18). In Pakistan, the
awareness campaign on IDD and iodized salt consumption has been poorly managed in the past
decade. This is evident from the results presented here that show a low level (12%) of awareness
about IDD or iodized salt utilization of pregnant women (13.5%) without knowledge about IDD.
This may partially be explained by a dissemination of information between the governmental
authorities and the general population for the historical advertisement mistake− in which iodine
intake advertisement was immediately followed by a fertility control advertisement on national
television− in a culturally conservative and religiously intact society. It resulted in misconception

31
of “iodized salt negatively affecting fertility”, which is still frequently believed in Pakistan (20).
Additionally, this may also be explained by the lack of locally adoptive scientific or social
interventions in campaigning (20, 21), involving local community through the Jirga system or
through the clerics. Jirga is an informal gathering of men that has a key governing and decision-
making role in the Pushtun community of KPK. A recent study conducted in a culturally and
socioeconomically similar population like ours showed a lower prevalence of goiter and higher
prevalence of iodized salt intake after intervention against IDD (20). Similarly, polio eradication
campaign, facing similar misconceptions like iodized salt, is progressing towards a probable end
in Pakistan (among the three countries around the world to have existence of polio virus), after
involving the local clerics for convincing the general public through direct speeches and fatwas
(22, 23).
Despite of limited access to electricity, particularly in rural areas of Pakistan, the
strongest medium promoting awareness about IDD are printed or electronic media. Our results
highlight the importance of media in awareness campaigns, which is consistent with other studies
(24, 25). However, we did not collect information about− when for the first time the pregnant
women started knowing about iodized salt or IDD. So, it is not certain whether knowing about
IDD represents the current or their previous knowledge from a decade ago, given the schooling
age as the second highest source of knowledge for all pregnant women. This is in line with the
phases of governmental efforts regarding awareness about iodized salt and IDD (1).
Urbanized settings are more suitable for awareness campaigns due to comparatively
higher chances of high-quality education and social integration. There are huge differences in
urban and rural disparity indices in Pakistan (KPK in particular) (16). Regarding iodine, iodized
salt and IDD the previous studies have reported a higher knowledge in urban than in the rural
populations (26-28). In contrast, we observed no difference in odds, between urban and rural
pregnant women for having greater knowledge about IDD. We suppose that due to focus of the
government on polio eradication during the last decade, the vigorous campaigning (including
awareness in population) for the IDD control program was slow. Further, because of missing
iodine supplementation in women during pregnancy, pregnant women in rural and urban areas
have similar knowledge about iodized salt or IDD. The Lakki Marwat district, in which rural
pregnant women had higher odds of having knowledge about IDD, was an exception. This may

32
be related to differences in rural/urban health care providers in comparison to other districts (11).
Thus, the literacy ratio and poverty index alone could not explain these differences.
Iodized salt intake is indispensable in populations less relying on foods rich in iodine (8).
The rapid physiological changes during pregnancy and the higher iodide requirements in
pregnant women define them as a special target group for iodine supplementation (13). Our
results show that a high frequency (79%) of pregnant Pakistani women were not taking iodized
salt (29). A low intake of iodized salt was reported in previous studies from the urban
metropolitan city of Lahore (34%) in 2009 (30) and a study from Faisalabad (6%) in 2000 (31)
from Punjab province. Likewise, the national nutrition survey in 2011 reported an intake of
iodized salt in only 40% of all women of reproductive age (7). Apart from the myth associated to
the iodized salt, the price of iodized salt is three times higher in comparison to the non-iodized
salt. Moreover, the price for iodized salt has been doubled during the last decade. These factors
contribute to a general less frequent use of iodized salt (1). In addition, disparities in salt intake
prevalence across Pakistani studies may be explained by regional differences and changes over
time (1). As demonstrated in our study, the prevalence of iodized salt intake is significantly
different even between districts of one province. This finding clearly demonstrates the need for a
consistent iodine fortification program throughout Pakistan. Overall, our and all previous studies
indicate that the prevalence of pregnant women taking iodized salt is far lower than international
recommendations (8).
Iodized salt intake was higher in the big cities like Peshawar and Nowshehra than in the
smaller ones (Karak and Kohat). Iodized salt intake was also higher in the pregnant women of
urban areas compared to rural areas. These results are consistent with data from the national
nutrition survey in 2011 (7). This may be due to preference of selling the iodized salt, because of
their organized packing in the urban areas of the big towns, apart from awareness. This is
highlighted by no significant differences in the pregnant women’s odds of iodized salt intake
from urban and rural residence. A recent study in the rural suburb of district Peshawar revealed
that− against the household iodized salt consumption of only 2.6% with awareness in general
public only 3%− 67.9% of the shopkeepers in the area regularly stocked iodized salt before
intervention (20). These results clearly show that iodized salt use is affected by its availability in
urban population, apart from other reasons. However, this is not a generalized rule, particularly

33
in the smaller towns. Increased urbanization may also increase the prevalence of iodized salt
intake. A good example can be elaborated from the district Karak in our results, where there was
extremely low intake of iodized salt among pregnant women in the whole district. However, due
to the urbanization effect reinforced by the higher literacy ratio of urban women− resulted in
marginal odds to have knowledge about IDD− the prevalence for iodized salt intake was high in
the urban settings, although around 93% of the population in this district lives under rural
conditions. District Lakki Marwat was the only exception where there was a reversed trend;
possibly because of higher rural health standards and significant advantage of the rural pregnant
women to have knowledge about IDD than in other districts may have contributed to the high
iodized salt intake in rural pregnant women.
UIC is a well-accepted sensitive marker and at population level a useful measure to
assess changes in the iodine status. The median UIC was lower (131 µg/L) than recommended
by the WHO, indicating a mild iodine deficiency. This finding is in concordance with those
reported in the national nutrition survey-2011; 149 µg/L for women of reproductive age in the
whole KPK province (7). However, UIC in our study is higher than in a study conducted in
school aged children of the same study region in 2015-16 (5, 6). Frequency of having UIC <150
µg/L were significantly higher among pregnant women in the districts Nowshehra, Karak and
Kohat in comparison to Peshawar. This is explained by their iodized salt intake and goiter
prevalence in line with previous history of iodine deficiency (1). We could not observe a
significant difference in UIC among pregnant women from rural and urban origin except a
marginally significant result in district Nowshehra. This finding is in in contrast to the results of
national nutrition survey-2011, where prevalence of normal and median UIC was higher in rural
areas than in urban.
In accordance with other studies in regions with low daily dietary iodine intake UIC
levels remained nearly stable or increased with trimesters of pregnancy (14, 32, 33). The increase
in iodine loss can be accounted for renal iodine loss during pregnancy, reflecting not only daily
dietary iodine intake but also initial thyroid iodine content depletion in the absence of increased
dietary iodine intake (14). There is an established association between the iodine deficiency and
reproductive failures including abortions (34, 35). The risk of reproductive failure is twice as
high in iodine deficient women than in woman with normal iodine level (34). This influence of

34
iodine deficiency is also demonstrated by the reduction in reproductive failures when iodine is
administered to women before pregnancy (36, 37). However, according to our results, previous
abortion could not motivate the pregnant women to overcome iodine deficiency, which is
possibly due to lack of awareness, resources or access. Hence the loss of iodine in the course of
successive pregnancies, iodine loss in trimesters of pregnancies (14) may further aggravate the
iodine deficiency related reproductive complications.
Pregnancy-induced goitrogenesis is evident from the association of biochemical features
of thyroidal stimulation with volumetric changes in the gland at least in conditions with a low
iodine intake (32) and this increase is observed accordingly during the trimesters of pregnancy
(13). There is no previous study reporting goiter prevalence in pregnant women in our study
region, but our results are in consonance with the previous studies conducted in the same regions
in school aged children (4-6). It is also known that goiter formation during pregnancy can be
prevented by increasing the iodine supply during pregnancy (33), compensating the increased
renal loss of iodine contributed to thyroid enlargement. Our study region had been passing
through a transition phase from being historically iodine deficient towards betterment. Naturally,
in the transition phase we may still expect goiter prevalence in our population. Additionally, the
environmental factors affecting natural soil iodine may also be contributing at population level
(1). It has been reported that thyroid volume in pregnant women increases significantly
compared to the non-pregnant women and accordingly during the trimesters of pregnancy (13),
but our results show a non-significant decrease and then increase in goiter prevalence in second
and third trimester of pregnancy respectively (Table 3). However, it may be argued that, due to
low sensitivity of goiter determination through palpation rather than ultrasound and further due
to interobserver variabilities, the precise estimate of goiter prevalence may have been
confounded by these factors. Goiter prevalence was lower in the urban than in the rural areas.
Reciprocated by the lower intake of iodized salt, geography and previous history (38), goiter
prevalence was almost twice higher in the Karak district than in the other districts. The factors
for the lowest goiter prevalence from district Lakki Marwat may be an already higher intake of
iodized salt, with the possibility of higher natural soil iodine in the drinking waters and to the
higher iodine contents in the sedimentary rock formation of district Lakki Marwat (12, 39). This
may be the reason that there are no previous reports of goiter prevalence and iodine deficiency
for any group from this region in history.

35
The strength of our study is that it is the first study from socioeconomically deprived
districts with the largest study population of pregnant women in Pakistan ever been studied. Our
study is limited by not presenting the personal educational level but we have interpreted results
based on the literacy ratio of the district concerned. Similarly we had not collected data about the
occupation, socioeconomic status and further about pregnant women receiving or not receiving
health and prenatal care. Additionally selection bias may have occurred as this study targeted
pregnant woman attending prenatal clinics. The data reporting from pre-natal clinics was self-
limiting by the fact that only 50% (11), women receive care from any level of prenatal care in
KPK province of Pakistan. Hence, results from this study cannot be generalized to the entire
population of the study region. A bias in the results may have been introduced because data from
private clinics was not available from all the districts due to non-response and cultural factors.
However, the results provide a very useful reference for woman attending prenatal clinics for this
province given the large sample size. Further, we had not assessed iodine in salt due to resource
limitations. Goiter prevalence may be confounded by interobserver variability and low sensitivity
of goiter determination by palpation rather than the ultrasound.
Conclusion
Urinary iodine excretion levels indicate a stable iodine supply, but still not sufficient based on
the goiter prevalence and iodized salt intake rate. This may be due to insufficient awareness
campaigns and low literacy ratio in rural areas. Our results show that rural/urban disparity is
affecting the IDD prevention program in rural districts, but not in general, and there is urgent
need for a uniform approach throughout Pakistan towards the elimination of iodine deficiency.

36
Acknowledgments
This project has received funding from the European Union’s Horizon 2020 research and
innovation program under grant agreement No. 634453. We also received partial support for the
analyses from the German Research Foundation under the project number DFG-VO955/10-2.
We acknowledge the contribution of all the persons; hospital administration, physicians,
provincial and district level health department administration and Department of Zoology; Kohat
University of Science and Technology (KUST), Kohat, Pakistan for their support in data
collection.
Author Disclosure Statement
No competing financial interest exist
Address for correspondence:
Rehman Mehmood Khattak
Institute for Community Medicine,
University Medicine Greifswald,
Walther Rathenau Str. 48, 17475 Greifswald, Germany
Phone: +49 - 3834 - 866683
FAX: +49 - 3834 – 867541
e-mail: [email protected]

37
References
1. Khattak RM, Muhammad Nasir Khan Khattak, Till Ittermann, Völzke H 2016 Factors
affecting sustainable iodine deficiency elimination in Pakistan: a global perspective. J
Epidemiol 27:249-257.
2. McCarrison R 1908 Observations on Endemic Cretinism in the Chitral and Gigit Valleys.
The Lancet 2:1275-1280.
3. 2015 Review of National Legislation for Universal Salt Iodization: South and East Asia
and the Pacific United Nations Children’s Fund (UNICEF) East Asia and Regional Office
(EAPRO) Bangkok, Thailand.
4. Saira S, Khattak RM, Rehman AU, Khan AA, Khattak MNK 2014 Prevalence of goiter
and iodine status in 6-12 years school children and pregnant women of district
Charsadda, Pakistan. Acta Endocrinologica (Buc) 10:65-75.
5. Subhan F, Jahangir M, Saira S, Khattak RM, Shahab M, Haq M, Khattak MNK 2013
Prevalence of goiter and iodine status among 6-12 years school age children in district
Kohat, Pakistan. South East Asia Journal of Public Health 4:42-46.
6. Jahangir M, Khattak R, Shahab M, Tauseef I, Khattak M 2015 Prevalence of goiter and
iodine nutritional status in school age children of district Karak, Khyber Pakhtunkhwa,
Pakistan. Acta Endocrinologica (BUC) 11:337-342.
7. 2011 National Nutrition Survey (NNS). Aga Khan University, Pakistan Medical Research
Council (PMRC) and the Nutrition Wing, Ministry of Health, Pakistan.
8. WHO/ICCIDD/UNICEF 2007 Assessment of iodine deficiency disorders and monitoring
their elimination: a guide for programme managers. Geneva. World Health Organization,
Genava.
9. 1998 Provincial Census Report NWFP. Population Census Organization. Statistics
Division, Government of Pakistan Islamabad.
10. 6th Population and Housing Census. Khyber Pakhtunkhwa. Pakistan Bureau of Statistics,
Government of Pakistan: District at a Glance http://pbscensus.gov.pk/content/khyber-
pakhtunkhwa (Last accessed on 27.11, 2015).
11. 2010 Khyber Pakhtunkhwa: Health Sector Situation Analysis. Government of Khyber
Pakhtunkhwa, Peshawar.

38
12. Johnson CC 2003 The geochemistry of iodine and its application to environmental
strategies for reducing the risk from iodine deficiency disorders (IDD) Commissioned
Report. British Geological Survey, Natural Environment Research Council, UK, 54 pp.
13. Glinoer D 2004 The regulation of thyroid function during normal pregnancy: importance
of the iodine nutrition status. Best Practice & Research Clinical Endocrinology &
Metabolism 18:133-152.
14. Smyth P, Hetherton A, Smith D, Radcliff M, O’herlihy C 1997 Maternal iodine status
and thyroid volume during pregnancy: correlation with neonatal iodine intake. The
Journal of Clinical Endocrinology & Metabolism 82:2840-2843.
15. Lall SV, Selod H, Shalizi Z 2006 Rural-urban migration in developing countries: A
survey of theoretical predictions and empirical findings. Development Research Group of
the World Bank, Washington.
16. Rahman A, Hayat Y, Habib Z, Iqbal J 2011 Rural-Urban Disparities in Khyber
Pakhtunkhwa Pakistan. Sarhad J Agric 27:477-483.
17. Salma S, Rehman S, Shah MA 2012 Rainfall trends in different climate zones of
Pakistan. Pakistan Journal of Meteorology (Pakistan) 9:37-47.
18. Randolph W, Viswanath K 2004 Lessons learned from public health mass media
campaigns: Marketing health in a crowded media world. Annu Rev Public Health
25:419-437.
19. Leiby R 2012 Salt rumors add to health crisis in Pakistan:
https://www.washingtonpost.com/world/asia_pacific/salt-rumors-add-to-health-crisis-in-
pakistan/2012/12/30/bb5f5e48-4619-11e2-8c8f-fbebf7ccab4e_story.html The
Washington Post, Washington USA.
20. Lowe N, Westaway E, Munir A, Tahir S, Dykes F, Lhussier M, McKeown M,
Zimmerman M, Andersson M, Stinca S 2015 Increasing Awareness and Use of Iodised
Salt in a Marginalised Community Setting in North-West Pakistan. Nutrients 7:9672-
9682.
21. Anonymous 2004 Neuromarketing: beyong branding. Lancet Neurol 3:71.
22. Mahmood SU, Ahmed SA, Shoaib M, Khan T, Majeed M 2017 Polio Eradication in
Pakistan: Call for Alliance. The Ochsner Journal 17:13-14.

39
23. 2010 Polio drops declared ‘halal’ The Express Tribune Pakistan:
https://tribune.com.pk/story/81400/polio-drops-declared-halal/. The Express Tribune
Islamabad: Accessed 13.11.2017.
24. Charlton KE, Gemming L, Yeatman H, Ma G 2010 Suboptimal iodine status of
Australian pregnant women reflects poor knowledge and practices related to iodine
nutrition. Nutrition 26:963-968.
25. Cavill N, Bauman A 2004 Changing the way people think about health-enhancing
physical activity: do mass media campaigns have a role? Journal of sports sciences
22:771-790.
26. Mohapatra SS, Bulliyya G, Kerketta AS, Geddam JJ, Acharya AS 2001 Elimination of
iodine deficiency disorders by 2000 and its bearing on the people in a district of Orissa,
India: a knowledge–attitude–practices study. Asia Pacific journal of clinical nutrition
10:58-62.
27. Aruna R, Sarojani J, Devendrappa S, Lata P 2014 Impact of education intervention on
prevention of iodine deficiency disorder in Dharwad Taluk, Karnataka. International
Journal of Farm Sciences 3:156-163.
28. Guajardo A 2015 Knowledge of dietary iodine and iodine concentration in household
iodized salt in rural and urban Jalisco, Mexico [Honors Theses]: College of Saint
Benedict, Saint John's University.
29. Bath SC, Steer CD, Golding J, Emmett P, Rayman MP Effect of inadequate iodine status
in UK pregnant women on cognitive outcomes in their children: results from the Avon
Longitudinal Study of Parents and Children (ALSPAC). The Lancet 382:331-337.
30. Elahi S, Rizvi NB, Nagra SA 2009 Iodine deficiency in pregnant women of Lahore.
Journal of Pakistan Medical Association 59:741-743.
31. Saeed M, Yaqub M, Roohi M, Ashraf M 2000 Prophylactic use of iodized salt in
pregnancy. Professional 7:66-69.
32. Glinoer D, NAYER PD, Bourdoux P, Lemone M, Robyn C, STEIRTEGHEM AV,
Kinthaert J, Lejeune B 1990 Regulation of Maternal Thyroid during Pregnancy. The
Journal of Clinical Endocrinology & Metabolism 71:276-287.

40
33. Liesenkötter KP, Göpel W, Bogner U, Stach B, Grüters A 1996 Earliest prevention of
endemic goiter by iodine supplementation during pregnancy. European Journal of
Endocrinology 134:443-448.
34. Dillon J, Milliez J 2000 Reproductive failure in women living in iodine deficient areas of
West Africa. BJOG: An International Journal of Obstetrics & Gynaecology 107:631-636.
35. Glinoer D 2007 The importance of iodine nutrition during pregnancy. Public health
nutrition 10:1542-1546.
36. Pharoah POD, Buttfield IH, Hetzel BS 1971 Neurological damage to the fetus resulting
from severe iodine deficiency during pregnancy. The Lancet 1:308-310.
37. Thilly C, Delange F, Stanbury J 1980 Epidemiologic surveys in endemic goiter and
endemic cretinism. John Wiley, New York.
38. Khattak MNK, Haq M, Khan A, Cheema A 2006 Prevalence of endemic goiter and
urinary iodine contents in the population of Lawaghar and Chontra areas of district Karak
(North Western Frontier Province), Pakistan. Pakistan Journal of Scientific Research
58:1-4.
39. Hemphill WR, Kidwai AH 1973 Stratigraphy of the Bannu and Dera Ismail Khan areas,
Pakistan Geological Investigations in Pakistan, Geological Survey Professional Paper
716-B. United States Department of the Interior: Geological Survey USA, 10-11.

41
Table 1. Characteristics of the Study Area with Potential Threats to Natural Soil Iodine
Characteristics Lakki Marwat Karak Kohat Nowshehra Peshawar
Total Urbanized area
(%) 9.7 6.5 27.0 26.0 49.0
Estimated population
(in million) 0.065 0.058 0.076 0.124 0.283
Literacy ratio
(total/female) (%) 54/29 58/36 47/28 50/35 56/36
Literacy ratio female
(Urban/rural) (%) 49/26 62/34 49/23 41/32 45/26
Topography Desert with
mountainous
outskirts
High mountain
ranges with barren
plain areas
High mountain
ranges with fertile
plain areas
Plain riverine with
mountainous
outskirts
Plain, fertile,
riverine area
Potential
environmental threats
Cyclones, drought Floods, drought,
intense rainfall,
earthquake
Intense rainfall,
earthquake
Floods, intense
rainfall
Floods, intense
rainfall, earthquakes
(7, 9-11) Population data is based on the 1998 census

42
Table 2. Selected Baseline Characteristics of Pregnant Women in Five Districts
Characteristic Lakki
Marwat Karak Kohat Nowshehra Peshawar
Age (years) 26.3 ± 5.5 28.2 ± 4.9 28.5 ± 4.3 25.5 ± 5.9 27.0 ± 6.2
Age range
(years) 15-45 17-40 17-39 15-45 16-50
BMI (Kg/m2) 26.5 ± 6.3 25.2 ± 3.6 21.3 ± 3.9 26.7 ± 5.6 26.8 ± 6.0
Locality
Rural n (%) 173 (22.1) 195 (24.9) 192 (24.5) 123 (15.7) 100 (12.8)
Urban n (%) 71 (15.3) 57 (12.3) 57 (12.3) 128 (27.7) 150 (32.4)
Trimester of
pregnancy
First n (%) 42 (17.3) 39 (16.1) 76 (31.3) 56 (23.1) 30 (12.1)
Second n (%) 94 (24.7) 53 (13.9) 99 (26.1) 73 (19.2) 61 (16.1)
Third n (%) 108 (17.3) 160 (25.7) 74 (11.9) 122 (19.6) 159 (25.5)
Previous abortion
No n (%) 210 (21.7) 181 (18.7) 194 (20.1) 194 (20.1) 187 (19.4)
Yes n (%) 34 (12.1) 71 (25.4) 55 (19.6) 57 (20.4) 63 (22.5)
Number of
abortions
0 n (%) 210 (21.7) 181 (18.7) 194 (20.1) 194 (20.1) 187 (19.4)
1 n (%) 19 ( 12.1) 39 (24.8) 27 (17.2) 31 (19.8) 41 (26.1)
2 n (%) 9 (11.8) 20 (26.3) 19 (25.0) 14 (18.4) 14 (18.4)
3 n (%) 5 (20.0) 7 (28.0) 5 (20.0) 7 (28.0) 1 (04.0)
4 n (%) 0 (0.00) 4 (40.0) 2 (20.0) 2 (20.0) 2 (20.0)
5 n (%) 1 (10.0) 0 (0.00) 2 (20.0) 2 (20.0) 5 (50.0)
6 n (%) 0 (0.00) 0 (0.00) 0 (0.00) 1 (100.0) 0 (0.00)
10 n (%) 0 (0.00) 1 (100.0) 0 (0.00) 0 (0.00) 0 (0.00)
Data presented as absolute numbers (percentages) or mean ± standard deviation

43
Table 3. Association of Iodized Salt Intake, Goiter Prevalence and Recommended Baseline UIC with Different Demographic
Characteristics
Characteristic
Survey sample
(n=1246)
Iodized salt intake
(n=262; 21.0%)
Goiter prevalence
(n=318; 25.5%)
UIC <150 µg/L
(n=731; 58.7%)
n % n (%) P value n (%) P value n (%) P value
District
Lakki Marwat 244 19.6 45 18.4 <0.001 44 18.0 0.656 57 23.4 0.096
Karak 252 20.2 9 3.6 <0.001 111 44.1 <0.000 208 82.5 <0.001
Kohat 249 20.0 27 10.8 <0.001 54 21.7 0.565 165 66.3 <0.001
Nowshehra 251 20.1 68 27.1 <0.001 60 23.9 0.244 226 90.0 <0.001
Peshawar 250 20.1 113 45.2 Ref 49 19.6 Ref 75 30.0 Ref
Residence
Rural 783 62.8 137 17.5 <0.001
209 26.7 0.218
467 59.6 0.364
Urban 463 37.2 125 27.0 109 23.5 264 57.0
Knowledge
about IDD
No 1093 87.7 147 13.5 <0.001
290 26.5 0.030
659 60.3 0.002
Yes 153 12.3 115 75.2 28 18.3 72 47.1
Trimester of
pregnancy
First 245 19.7 46 18.9 Ref 62 25.5 Ref 150 61.7 Ref
Second 379 30.4 81 21.3 0.471 85 22.4 0.367 226 59.5 0.575
Third 622 44.0 135 21.7 0.373 171 27.5 0.564 355 57.0 0.203
Previous
abortion
No 966 77.5 200 20.7 0.603
236 24.4 0.101
563 58.3 0.607
Yes 280 22.5 62 22.1 82 29.3 168 60.0
P-value calculated from logistic regression, adjusted for age, (Ref = reference category); The percentages presented are row
percentages

44

45

46
7.2. Monitoring the Prevalence of Thyroid Disorders in the Adult Population of Northeast
Germany
Rehman Mehmood Khattak*1, 4, Till Ittermann*1, Matthias Nauck2, Harald Below3, Henry Völzke1
* equally contributed as first authors
1Institute for Community Medicine,
2Institute of Clinical Chemistry and Laboratory Medicine,
3Institute of Hygiene and Environmental Medicine,
Ernst Moritz Arndt University Greifswald, Germany,
4Department of Zoology, Islamia College Peshawar (CU), Pakistan
Short running title: Monitoring of Thyroid Disorders
Keywords: Thyroid Disorders, Epidemiology, Monitoring, Prevalence Trend

47

48

49

50

51

52

53

54

55

56

57

58
7.3. Factor Affecting Sustainable Iodine Deficiency Elimination in Pakistan: A Global
Perspective
Rehman Mehmood Khattak1, 3, Muhammad Nasir Khan Khattak2, 4, Till Ittermann1, Henry
Völzke1
1Institute for Community Medicine, University Medicine Greifswald, Germany,
2Department of Zoology, University of Hazara, Mansehra, Pakistan,
3Department of Zoology, Islamia College Peshawar (CU), Pakistan,
4Department of Applied Biology, University of Sharjah, Sharjah, United Arab Emirates
Short running title: Iodine Nutritional Status in Pregnancy in Pakistan
Keywords: Iodine Deficiency Disorder, Goiter Prevalence, Iodine Nutritional Status Salt,
Iodization, Pakistan

59

60

61

62

63

64

65

66

67

68
8. Appendix
A. Statutory Declaration
Hiermit erkläre ich, dass ich die vorliegende Dissertation selbstständig verfasst und keine
anderen als die angegebenen Hilfsmittel verwendet habe.
Die Dissertation ist bisher keiner anderen Fakultät vorgelegt worden
Ich erkläre, dass ich kein Promotionsverfahren erfolglos beendet habe und dass eine
Anerkennung eines bereits erworbenen Doktorgrades nicht vorliegt
Greifswald, Date: Rehman Mehmood Khattak

69
B. Own Contributions
Explanation of Individual Shares in Joint Work
Data for this research was derived from pregnant women in the Khyber Pakhtunkhwa (KPK)
Province of Pakistan and from the SHIP database of the Community Medicine research Network.
The author was involved in the data collection from pregnant women in KPK, Pakistan,
The author performed the literature search, conceptual design of data analysis, explored the
theoretical framework, performed the statistical analysis and drafted all the research articles and
the thesis to their final version.
Rehman Mehmood Khattak Prof. Dr. Henry Völzke
The above information is confirmed:
Prof. Dr. Henry Völzke
Greifswald, Date:

70
C. Curriculum Vitae
Personal Data
Name Rehman Mehmood Khattak
Date of Birth 07 January 1979
City of Birth Karak, Pakistan
Address
Permanent Village Askari Alikhel, Tehsil and District Karak,
Khyber Pakhtunkhwa, Pakistan
Temporary Makarenko Street 51-B, 17491, Greifswald,
Germany
Marital status Married
Education
2005-2007 MPhil. Reproductive Physiology; Department of
Zoology, Bahauddin Zakariya University, Multan,
Punjab, Pakistan
2001-2003 MSc. Zoology; Department of Zoology, Bahauddin
Zakariya University, Multan, Punjab, Pakistan
1998-2000 BSc. Biology; Government College Dera Ghazi
Khan, Bahauddin Zakariya University, Multan,
Punjab, Pakistan
Professional Occupation
2007-2014 Lecturer in Zoology (Permanent); Kohat University
of Science and Technology (KUST), Kohat,
Pakistan
2005-2007 Lecturer in Zoology (Temporary); Kohat University
of Science and Technology (KUST), Kohat,
Pakistan

71
D. Scientific Output
Original articles
1. Khattak RM, Kasi KK, Schauer B, Kasi MD, Völzke H, Ittermann T. Epidemiology of
Crimean Congo Hemorrhagic Fever (CCHF) Across the Durand Line. 2018.
2. Khattak RM, Saira S, Schauer B, Khattak MNK, Völzke H, Ittermann T. Prevalence of
Underweight, Overweight and Obesity Among School Going Cchildren (6-12 Years)
From Pakistan and Disparity of Results Based on IOTF and CDC Cut-offs. 2017.
3. Khattak RM, Kühn J-P, Lerch MM, Ittermann T, Völzke H. Association of Thyroid
Function with Fat and Iron Contents of the Liver derived from MRI. 2017.
4. Khattak RM, Saifullah Z, Khadija G, Fayyaz A, Zaman S, Gul M, Khattak MNK,
Schauer B, Völzke H, Ittermann T. Regional Influence on Iodine Nutritional Status of
Pakistani Pregnant Women. 2017.
5. Khattak RM, Khattak MNK, Ittermann T, Völzke H. Factors affecting sustainable iodine
deficiency elimination in Pakistan: A global perspective. Journal of Epidemiology. 2017.
6. Khattak RM, Ittermann T, Nauck M, Below H, Völzke H. Monitoring the prevalence of
thyroid disorders in the adult population of Northeast Germany. Population health
metrics. 2016;14(1):39.
7. Naeem M, Khattak RM, ur Rehman M, Khattak MNK. The role of glycated hemoglobin
(HbA1c) and serum lipid profile measurements to detect cardiovascular diseases in type 2
diabetic patients. South East Asia Journal of Public Health. 2016;5(2):30-34.
8. Völzke H, Caron P, Dahl L, De Castro JJ, Erlund I, Gaberšček S, Gunnarsdottir I,
Hubalewska-Dydejczyk A, Ittermann T, Ivanova L, Khattak RM, ........... Ensuring
effective prevention of iodine deficiency disorders. Thyroid. 2016;26(2):189-196.
9. Ittermann T, Khattak RM, Nauck M, Cordova CM, Völzke H. Shift of the TSH reference
range with improved iodine supply in Northeast Germany. European journal of
endocrinology. 2015;172(3):261-267.

72
10. Jahangir M, Khattak R, Shahab M, Tauseef I, Khattak M. Prevalence of goiter and iodine
nutritional status in School-age Children of District Karak, Khyber Pakhtunkhwa,
Pakistan. Acta Endocrinologica (1841-0987). 2015;11(3).
11. Saeed S, Jahangir M, Fatima M, Shaikh R, Khattak R, Ali M, Iqbal F. PCR based
detection of Theileria lestoquardi in apparently healthy sheep and goats from two districts
in Khyber Pukhtoon Khwa (Pakistan). Tropical biomedicine. 2015;32(2):225-232.
12. Subhan F, Jahangir M, Saira S, Khattak RM, Shahab M, Haq M, Khattak MNK.
Prevalence of goiter and iodine status among 6-12 years school age children in district
Kohat, Pakistan. South East Asia Journal of Public Health. 2015;4(2):42-46.
13. Saira S, Khattak R, Rehman A, Khan A, Khattak M. Prevalence of goiter and iodine
nutritional status in 6-12 years School-age Children and pregnant women of District
Charsadda, Pakistan. Acta Endocrinologica (1841-0987). 2014;10(1).
14. Ashraf QU, Khan AU, Khattak RM, Ali M, Shaikh RS, Iqbal F. A report on the high
prevalence of Anaplasma sp. in buffaloes from two provinces in Pakistan. Ticks and tick-
borne diseases. 2013;4(5):395-398.
15. Iqbal F, Khattak R, Ozubek S, Khattak M, Rasul A, Aktas M. Application of the reverse
line blot assay for the molecular detection of Theileria and Babesia sp. in sheep and goat
blood samples from Pakistan. Iranian journal of parasitology. 2013;8(2):289.
16. Durrani S, Khan Z, Khattak RM, Andleeb M, Ali M, Hameed H, Taqddas A, Faryal M,
Kiran S, Anwar H. A comparison of the presence of Theileria ovis by PCR amplification
of their ssu rRNA gene in small ruminants from two provinces of Pakistan. Asian Pacific
Journal of Tropical Disease. 2012;2(1):43-47.
17. Khattak R, Rabib M, Khan Z, Ishaq M, Hameed H, Taqddus A, Faryal M, Durranis S,
Gillani Q, Allahyar R. A comparison of two different techniques for the detection of
blood parasite, Theileria annulata, in cattle from two districts in Khyber Pukhtoon Khwa
Province (Pakistan). Parasite: journal de la Société Française de Parasitologie.
2012;19(1):91.

73
18. Khattak RM, Ali S, Jahangir M, Khan MN, Rasul A, Iqbal F. Prevalence of ectoparasites
in wild and domesticated grey (Francolinus pondicerianus) and black partridges
(Francolinus francolinus) from Khyber Pakhtoonkhwa Province of Pakistan. Pakistan
Journal of Zoology. 2012;44(5):1239-1244.
19. Gilbert M, Oaks JL, Virani MZ, Watson RT, Ahmed S, Chaudhry M, Arshad M,
Mahmood S, Ali A, Khattak RM. The status and decline of vultures in the provinces of
Punjab and Sind, Pakistan: a 2003 update. Raptors worldwide (Eds: Chancellor, RC &
BU Meyburg) World Working Group on Birds of Prey/MME-BirdLife Hungary.
2004:221-234.
Presentations
1. Khattak RM, Khattak MNK, Ittermann T, Völzke H. Factors affecting sustainable iodine
deficiency elimination in Pakistan: A global perspective. Paper presented at: 12th Asia
Oceania Thyroid Association Congress 2017; Busan, South Korea.
Posters
1. Khattak RM, Kühn J-P, Lerch MM, Ittermann T, Völzke H. Association of Thyroid
Function with Fat and Iron Contents of Liver; MRI-based Examinations. Paper presented
at: 40th Annual Meeting of the European Thyroid Association 2017; Belgrade, Serbia.
2. Khattak RM, Saifullah Z, Khadija G, Fayyaz A, Zaman S, Gul M, Safdar F, Gul N,
Khattak MNK, Schauer B, Völzke H, Ittermann T. Regional Influence on Iodine
Nutritional Status of Pakistani Pregnant Women. Paper presented at: 12th Asia Oceania
Thyroid Association Congress 2017; Busan, South Korea.
3. Khattak RM, Ittermann T, Nauck M, Below H, Völzke H. Monitoring the Prevalence of
Thyroid Disorders in the Adult Population of Northeast Germany. Paper presented at:
39th Annual Meeting of the European Thyroid Association 2016; Copenhagen, Denmark.

74
E. Acknowledgements
My heartiest thanks to Prof. Dr. Henry Völzke for providing me the opportunity to work under
his supervision, and further increasing my research related capabilities. I am obliged to him for
providing the intellectual support in SHIP team and in the international scientific community.
Further thanks for the extending support to my family for staying in Germany and in all other
aspects.
My special thanks to Dr. Till Ittemann for his assistance throughout my stay in Institute for
Community Medicine. He has always been a beacon light throughout the research I conducted in
the Institute for Community Medicine, University Medicine Greifswald, Germany.
My gratitude to all the colleagues in the SHIP team for making my stay comfortable with their
hostile attitude.
I extend my gratitude to my family−particularly my late mom (Noor Jehan), my father (Moweez
Gul Khattak) my wife (Mumtaz Begum) my kids (Noyana Fatma, Hanzala Abdullah Khattak) all
my brothers and sisters and my friends.
I would particularly like to thank Higher Education Commission (HEC) of Pakistan for
providing funding for my stay in Germany for completion of doctoral degree. I would also like to
thank Islamia College Peshawar (Chartered University) and all our funding partners for the
different projects.