Embed Size (px)
Citation preview

ClassifiCation and epidemiology
Epidemiology of tobacco, alcohol and drug usemichael farrell
e Jane marshall
Abstracttobacco, alcohol and drug use are very common in the general popula-
tion. population studies indicate that 30% of adults smoke tobacco,
88% of adults consume alcohol on a regular basis and nearly half the
population drink more than twice a week (48%), and 21% of men and
12% of women drink four or more times a week. nearly 1 in 4 smokers
(24%) had used drugs in the past year, compared with 1 in 20 (5%)
non-smokers. similarly, those with a high aUdit score were more likely
to have ever used drugs: 19% of those with an aUdit score below 8
reported drug use in the past year, compared with 47% of those with
a score greater than 8. nearly 1 in 4 of the english population (25%)
reported ever using cannabis. the next most common drug reported was
amphetamine, with 7% saying they had used it at some time. lifetime
prevalence rates for ecstasy, cocaine or lsd were all 4%. Crack cocaine,
heroin and non-prescribed methadone were used by less than 1% of the
population. in 1993, 5% of the population reported using any drug in
the past year, but by 2000 this had risen to 12%. it is estimated 20%
of the population are nicotine dependent, 4–7% are alcohol dependent
and 4% are drug dependent. Being dependent on any drug was related
to smoking and drinking, with heavy smokers having a 12-fold increase
in the odds of dependence, and those scoring 16 or more on the aUdit
having a sixfold increase in the risk of drug dependence. these beha-
viours are associated with significant added mental and physical health
problems.
Keywords addiction; alcohol; drugs; tobacco
A number of major surveys of psychiatric morbidity have included questions about tobacco, alcohol and drug use. In North America the first major study was the Epidemiological Catchment Area Study.1 This study has been broadly replicated
Michael Farrell MRCP MRCPsych is a Reader in Addiction Psychiatry at
the National Addiction Centre, Institute of Psychiatry, King’s College
London, UK, and Consultant Psychiatrist at the South London and
Maudsley NHS Trust. His research interests include health services-
related research and social and psychiatric epidemiology. Conflicts of
interest: none declared.
E Jane Marshall MRCPI MRCPsych is Senior Lecturer in the Addictions at
the National Addiction Centre, Institute of Psychiatry, London, UK, and
Consultant Psychiatrist at the South London and Maudsley NHS Trust.
Her research interests include treatment outcome and quality of life
studies in alcohol use disorders. Conflicts of interest: none declared.
psyCHiatRy 5:12 42
in many countries, initially by the National Comorbidity Study,2 and subsequent studies using the same instruments have been done in Europe and Central and South America.
In the UK a programme of national psychiatric morbidity surveys has been under way over the past decade.3 This has included two national household surveys (in 1993 and 2000), a survey of the homeless and a survey of prisoners. The more recent household survey included a 12-month follow-up com-ponent. Some of the key findings of these different surveys in relation to tobacco, alcohol and other drug use are described in this contribution.
The benefits of population studies
Large-scale population studies, whether cross-sectional or longi-tudinal, are important because they allow researchers to: • understand the prevalence of problems in the community • develop estimates of incidence and prevalence of different
disorders • look at how people with different disorders access help for
their problems.After anxiety and depression, disorders of substance dependence are among the most common mental health disorders. Yet in spite of their high occurrence and significant public health burden, they are also the conditions for which patients are least likely to be undergoing current treatment or to have access to help.
Tobacco, alcohol and drug dependence are heterogeneous conditions that vary significantly across the lifespan. There are also significant sex differences in the prevalence of alcohol and drug dependence. One of the functions of population-based sur-veys is to delineate the extent of the harm associated with the consumption of and dependence on these substances. Many of the problems and harms are hidden and often there is a lack of awareness of the large scale of problems, and the burden on the health service and the criminal justice system, associated with these disorders.
Findings from the National Survey of Psychiatric Morbidity, 20004
SmokingThirty percent of adults aged 16–74 years reported current smok-ing, 23% were ex-regular smokers and 47% had never smoked regularly. Men were more likely than women to report ‘heavy smoking’ (11% compared with 7%). The 20–24-year age group reported the highest rates of smoking (44%); this figure decreased with age, with only 14% of those in the 70–74-year age range reporting smoking behaviour. The proportion of women who reported ‘never smoking’ was substantially higher in the older age groups, indicating the trend for increased smoking rates among young women.
AlcoholAround 1 in 8 people (12%) reported not having any alcoholic drinks in the past year. Women were more likely than men to be non-drinkers (14% compared with 9%). Nearly half the pop-ulation drank more than twice a week (48%), and 21% of men and 12% of women drank four or more times a week. Over-all, men were more likely to drink, to drink more often and to
7 © 2006 published by elsevier ltd.

ClassifiCation and epidemiology
drink more heavily on each occasion than women. When asked about drinking more than six drinks per drinking session, 2% of the population declared this as a daily occurrence and 17% declared it as a weekly occurrence. This pattern of binge drink-ing and drunkenness has become an issue of major concern in the UK and in many parts of Europe. In addition, recent work reports a very marked rise in the incidence and prevalence of alcohol-related liver disease, with rates higher in the UK than in other parts of Europe. In Scotland the cirrhosis rates have doubled and in England they have increased by two-thirds in the recent past.5
Alcohol dependence: the World Health Organization Alcohol Use Disorders Identification Test (AUDIT) scale is a continu-ous measure of increasing levels of alcohol problems along physical, psychological and social domains. A score of 8 or more, out of a maximum of 40, on this 10-item scale is indica-tive of hazardous drinking. Overall, a quarter of respondents (26%) scored more than 8; 4% scored 16 or more, which indicates more severe alcohol problems and probable alcohol dependence. Scores were highest in the youngest age groups and declined progressively with age. Scores were consistently higher in the white group than in the ethnic minority groups. In the national psychiatric morbidity survey hazardous drink-ing was associated with over half of all incidents involving injury. Antisocial personality disorder conveyed an attribut-able risk of 24% of respondents reporting victim injuries, but screening positive for psychosis conveyed an attributable risk of only 1.2%.6
The Severity of Alcohol Dependence Questionnaire (SADQ) was used to measure alcohol-dependence; overall 7% were rated as alcohol-dependent. Men were more likely to show signs of dependence than women, and the younger age group was more likely to show signs of dependence than the older age group. However, all cases rated as severe dependence were among people aged between 30 and 65 years.7
Drug useCannabis accounts for the bulk of self-reported illicit drug use in the UK population. Nearly 1 in 4 respondents (25%) reported ever using cannabis. The next most common drug reported was amphetamine, with 7% saying they had used it at some time. Lifetime prevalence rates for ecstasy, cocaine or LSD were all 4%. Crack cocaine, heroin and non-prescribed methadone were used by less than 1% of the population. In 1993, 5% of the popu-lation reported using any drug in the past year, but by 2000 this had risen to 12%, indicating a substantial shift in patterns of ‘ever use’ among the younger population. Men were more likely than women to report ever, past-year or past-month use.
Drug dependence: the prevalence of dependence on any drug was 4% for the total population. Rates were highest in the younger group and significantly declined with age. Three per-cent of drug dependence in the population was accounted for by cannabis dependence, and the other 1% was accounted for by a range of other drugs. Men were more likely than women to be dependent on all types of drugs, with the exception of tranquil-lizers. Regarding injecting drug use, 0.4% reported having ever injected and 0.2% reported having injected regularly.
psyCHiatRy 5:12 42
Interactions between smoking, drinking and drug-takingFor all ages and for both sexes, smokers were twice as likely to have ever used drugs compared with non-smokers. Nearly 1 in 4 smokers (24%) had used drugs in the past year, com-pared with 1 in 20 (5%) non-smokers. Similarly, those with a high AUDIT score were more likely to have ever used drugs: 19% of those with an AUDIT score below 8 reported drug use in the past year compared with 47% of those with a score greater than 8.
Being dependent on any drug was related to smoking and drinking, with heavy smokers having a 12-fold increase in the odds of dependence, and those scoring 16 or more on the AUDIT having a sixfold increase in the risk of drug dependence.
Relationship between substance use and mental health disordersThe prevalence of smoking, drinking and drug use and dependence was greater for people with mental health disorders than for those without. High scores on the Clinical Interview Schedule – Revised (CIS-R) had a stronger relationship with smoking than they did for measures of drinking and drug use. People with antisocial personality disorder showed very high levels of use of and dependence on tobacco, alcohol and drugs.
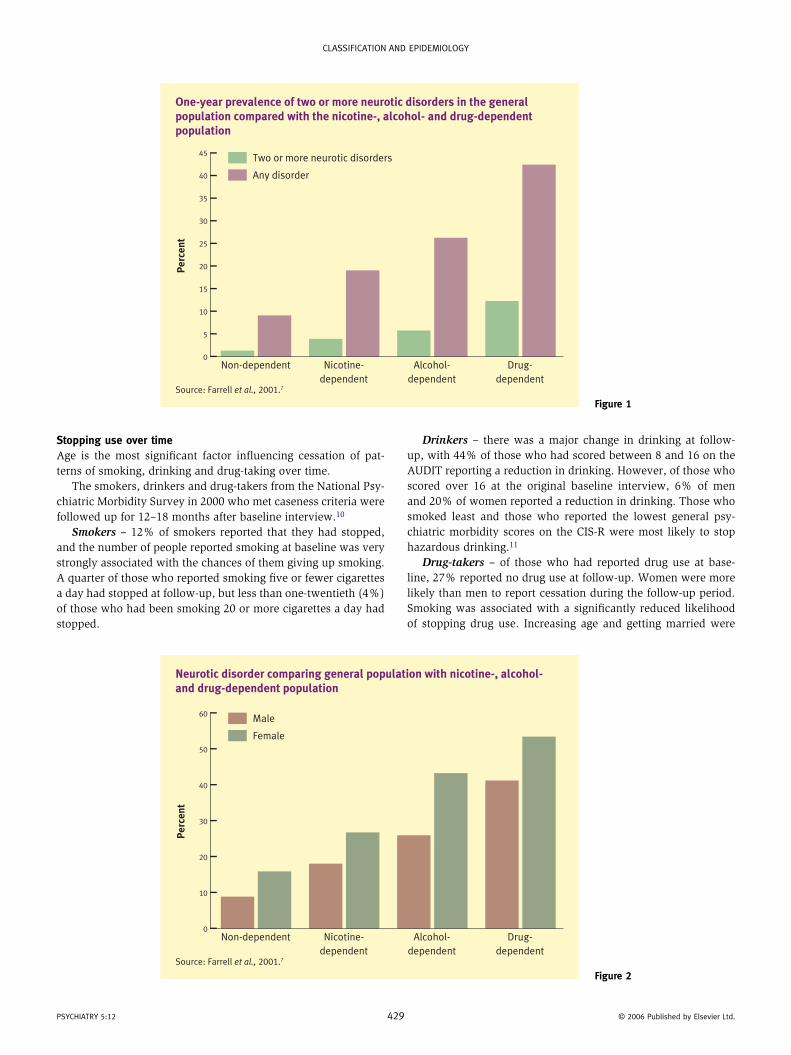
There is a consistent relationship between smoking, alcohol dependence, drug dependence and psychiatric disorder. Farrell et al. reported that nicotine, alcohol and drug dependence were associated with significantly higher rates of non-psychotic dis-orders (see Figures 1 and 2).7 The rates almost doubled from tobacco to alcohol, and doubled again from alcohol dependence to drug dependence.
The prevalence in the general population differs significantly from that in mental health services (see Marshall, 20008), in prisons and among the homeless. Both prison populations and the homeless report very high rates of smoking – approximately 80% – with high rates of heavy smoking. Over half of these popu-lations, in a range of surveys, report alcohol or drug dependence. These are associated with high rates of co-occurring disorders.9
Service useSubstance dependence not only adds to the individual health burden, both physical and psychological, but adds to the bur-den of services overall. Heavy smokers are more likely to con-sult their doctors about physical health problems and are also more likely to have used community services for a mental or emotional problem than non-smokers. The patterns of service use are more complex for those who are alcohol dependent, with many not showing any difference in service use from those who are not dependent. However, this group are more at risk of accidents and traumatic events, and in earlier life heavier drinking is associated with a significantly increased risk of mortality. Some of these data are accounted for by the fact that men between the ages of 20 and 35 account for most of the hazardous drinking, but overall are low users of health services. People who are dependent on drugs other than cannabis – primarily opioids – report higher rates of service use, with a higher likelihood of being in contact with treatment services, are more likely to have spoken to a GP about their problem in the past year, and more likely to have used other community services.
8 © 2006 published by elsevier ltd.
ClassifiCation and epidemiology
One-year prevalence of two or more neurotic disorders in the general population compared with the nicotine-, alcohol- and drug-dependent population
Source: Farrell et al., 2001.7
Pe
rce
nt
Non-dependent Nicotine-
dependent
Alcohol-
dependent
Drug-
dependent
45
0
Two or more neurotic disorders
Any disorder40
35
30
20
10
5
25
15
Figure 1
Stopping use over timeAge is the most significant factor influencing cessation of pat-terns of smoking, drinking and drug-taking over time.
The smokers, drinkers and drug-takers from the National Psy-chiatric Morbidity Survey in 2000 who met caseness criteria were followed up for 12–18 months after baseline interview.10
Smokers – 12% of smokers reported that they had stopped, and the number of people reported smoking at baseline was very strongly associated with the chances of them giving up smoking. A quarter of those who reported smoking five or fewer cigarettes a day had stopped at follow-up, but less than one-twentieth (4%) of those who had been smoking 20 or more cigarettes a day had stopped.
psyCHiatRy 5:12 42
Drinkers – there was a major change in drinking at follow-up, with 44% of those who had scored between 8 and 16 on the AUDIT reporting a reduction in drinking. However, of those who scored over 16 at the original baseline interview, 6% of men and 20% of women reported a reduction in drinking. Those who smoked least and those who reported the lowest general psy-chiatric morbidity scores on the CIS-R were most likely to stop hazardous drinking.11
Drug-takers – of those who had reported drug use at base-line, 27% reported no drug use at follow-up. Women were more likely than men to report cessation during the follow-up period. Smoking was associated with a significantly reduced likelihood of stopping drug use. Increasing age and getting married were
Neurotic disorder comparing general population with nicotine-, alcohol- and drug-dependent population
Source: Farrell et al., 2001.7
Pe
rce
nt
Non-dependent Nicotine-
dependent
Alcohol-
dependent
Drug-
dependent
60
0
Male
Female50
40
30
20
10
Figure 2
9 © 2006 published by elsevier ltd.

ClassifiCation and epidemiology
associated with an increased likelihood of cessation. Lack of social support was also significantly associated with reduced likelihood of cessation.
Conclusion
Nicotine is the commonest drug of dependence used in the gen-eral population, followed by alcohol. However, rates of cannabis use and dependence rose dramatically over the past decade but may be levelling out now. Other drugs, such as psychostimu-lants, amphetamines, cocaine and opioids, are less frequently used but are associated with an increased health burden to the individual and to the community.
New drugs such as methamphetamine ‘Ice’ are spreading in the USA and the Asia Pacific region but have yet to arrive in Europe to any major extent. The level of substance involve-ment is significantly correlated across the different substances but is also correlated with rates of other psychiatric morbidity. The nature of this relationship is complex but there is now a very consistent body of evidence to support the view that heavy substance involvement is associated with an increased mental health burden and decreased likelihood of change and recovery. More severe conditions are more resistant to change and are more likely to occur in combination with other disor-ders, which further complicates management. A new additional problem has been the growth of new technologies for gambling and it is predicted that the prevalence of gambling problems is set to surge. Individuals who are drug- and alcohol-involved appear to be also at increased risk of developing gambling problems. ◆
REFERENCES
1 Regier da, farmer me, Rae ds, et al. Comorbidity of
mental disorders with alcohol and other drug abuse: results
psyCHiatRy 5:12 4
from the epidemiology Catchment area study. JAMA 1990; 264:
2511–18.
2 Kessler RC, Crum Rm, Warner la. lifetime co-occurrence of dsm-iii-R
alcohol abuse and dependence with other psychiatric disorders
in the national Comorbidity study. Arch Gen Psychiatry 1997; 54: 313–21.
3 Jenkins R, lewis g, Bebbington p, et al. the national psychiatric
morbidity survey – initial findings from the Household survey.
Psychol Med 1997; 27: 775–90.
4 Coulthard m, farrell m, singleton n, meltzer H. tobacco, alcohol and
drug use and mental health: national statistics. london: stationery
office, 2002. also available at: http://www.statistics.gov.uk (accessed
14 sep 2006).
5 leon david a, mcCambridge J. liver cirrhosis mortality rates in
Britain from 1950 to 2002, an analysis of routine data. Lancet 2006;
367: 52–56.
6 Coid J, yang m, Roberts a, et al. Violence and psychiatric morbidity
in the national household population of Britain: public health
implications. Br J Psychiatry 2006; 189: 12–19.
7 farrell m, Howes s, Bebbington p, et al. nicotine, alcohol and drug
dependence, and psychiatric comorbidity – results of a national
household survey. Br J Psychiatry 2001; 179: 432–37.
8 marshall eJ. alcohol dependence and alcohol problems. in: gelder mg,
lópez-ibor Jr. JJ, andreasen nC, eds. new oxford textbook of psychiatry.
oxford: oxford University press, 2000.
9 farrell m, Howes s, taylor C, et al. substance misuse and psychiatric
comorbidity: an overview of the opCs psychiatric morbidity survey.
Int Rev Psychiatry 2003; 15: 43–49.
10 singleton n, lewis g, eds. Better or worse: a longitudinal survey
of the mental health of adults living in private households in great
Britain. london: stationery office, 2003. also available at:
http://www.statistics.gov.uk (accessed 14 sep 2006).
11 farrell m. tobacco, alcohol and drug use and cessation of use at
follow up. in: singleton n, lewis g, eds. Better or worse: a
longitudinal study of the mental health of adults living in private
households in great Britain. london: stationery office, 2003.
30 © 2006 published by elsevier ltd.





























