Embed Size (px)
Citation preview

6/11/2019
1/26
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e
Chapter 279: Neck and Back Pain David Della-Giustina; Je�rey S. Dubin; William Frohna
EPIDEMIOLOGY
Low back pain alone accounts for approximately 3% of all ED visits in the United States.1 Nearly one third of
ED back pain patients receive x-rays, and 10% undergo CT or MRI imaging.2 Analysis of the 2010 GlobalBurden of Disease study reveals a point prevalence of 5% for low back pain and 9% for neck pain. Back pain is
the number one cause of disability in the United States; neck pain is number four.3,4
RISK FACTORS FOR SERIOUS CAUSES OF NECK AND BACK PAIN
There are many causes of neck and back pain, including trauma and biomechanical injuries, degeneration,inflammation (arthritides), infection (e.g., discitis, meningitis, and epidural abscess), infiltration (e.g.,metastatic cancer and spinal cord tumors), and compression (e.g., epidural hematoma and abscess). In manycases of atraumatic neck and back pain, no specific cause can be identified. However, due to the high volumeof ED patients with neck and back pain, clinicians can develop an indi�erence to this complaint andpotentially overlook serious causes. Take care to perform a systematic evaluation based on risk factors in thehistory and physical examination, and let findings guide diagnostic testing and management (Table 279-1).Consider spinal anatomy while focusing on the presence or absence of neurologic signs to identifypathologic causes and prevent complications.

6/11/2019
2/26
TABLE 279-1
Risk Factors for Serious Causes of Neck and Back Pain
Risk Factors Concern
Historical Risk Factors
Pain >6 weeks Tumor, infection
Age <18, >50 Congenital anomaly, tumor, infection
Major trauma Fracture
Minor trauma in elderly or rheumatologic disease Fracture
History of cancer Tumor
Fever and rigors Infection
Weight loss Tumor, infection
Injection drug use Infection
Immunocompromised Infection
Night pain Tumor, infection
Unremitting pain, even when supine Tumor, infection
Incontinence Epidural compression
Saddle anesthesia Epidural compression
Severe/progressive neurologic deficit Epidural compression
Anticoagulants and coagulopathy Epidural compression
Physical Risk Factors
Fever Infection
Patient writhing in pain Infection, vascular cause

6/11/2019
3/26
Risk Factors Concern
Unexpected anal sphincter laxity Epidural compression
Perianal/perineal sensory loss Epidural compression
Major motor weakness/gait disturbance Nerve root or epidural compression
Positive straight leg raise test Herniated disk
Radiculopathy and myelopathy are identified through pattern recognition of the motor and dermatomeinnervations and their associated spinal level (see Figure 164-1 and Tables 164-1 and 164-2 in chapter titled"Neurologic Examination").
CLINICAL FEATURES OF NECK PAIN
In general, it is helpful to classify patients with neck pain into two groups: those with uncomplicated neckpain arising mainly from the joints and associated ligaments and muscles of the neck, and those with neckpain and radiculopathy (signs and symptoms attribuTable to a single nerve root) and/or myelopathy (signs orsymptoms due to a spinal cord lesion, stenosis, or compression).
HISTORY IN PATIENTS WITH NECK PAIN
Ask about the onset, duration, and location of the neck pain; recent or remote trauma; associated symptoms;sti�ness; deformity; neurologic complaints (e.g., weakness, changes in sensation, gait, or vision);constitutional symptoms such as fever, anorexia, and weight loss; and comorbid conditions such as arthritis,cancer, and infections. See Table 279-1 for clues to serious pathology to investigate in the history.Rheumatoid arthritis, ankylosing spondylitis, and psoriatic spondyloarthropathy may involve the C1-C2 joint,damage the transverse ligament, and erode the odontoid process, yielding instability of the atlantoaxialjoint. Subluxation may occur spontaneously or following a trivial injury. Morning sti�ness may signifyarthritic joints. Identify precipitating and palliative factors, maneuvers, or activities. Inquire about priorepisodes of neck pain, past diagnostic studies, and treatment. Determine the character of pain and itsdistribution. Patients with radiculopathy o�en complain of sharp, burning, intense pain that radiates to thetrapezius, periscapular area, or down the arm. Weakness or paresthesias may develop weeks a�er painonset. Patients with myelopathy may have neck pain that progresses insidiously and may complain ofclumsy hands, gait disturbances, and sexual or bladder dysfunction. Table 279-2 summarizes importantdi�erences in symptoms between uncomplicated mechanical neck pain and neck pain associated withradiculopathy or myelopathy.

6/11/2019
4/26
*Patient in either pain category is not expected to have all, or majority, of listed signs.
TABLE 279-2
Di�erentiating Cervical Radiculopathy from Uncomplicated Musculoskeletal Neck Pain
Factors Favoring Cervical Radiculopathy or
Myelopathy*
Factors Favoring Uncomplicated Musculoskeletal
Neck Pain*
Pain from the neck radiates down the arm in
dermatome pattern.
Tenderness of involved muscles, examiner may find
a focal point of tenderness.
Sensory changes along dermatome distribution. Atrophy or thinning of shoulder muscles (may
occur a�er rotator cu� injury).
Pushing down on top of head, with neck in extension
(chin up) and head leaning toward symptomatic side
elicits pain, typically toward or down the arm (positive
Spurling's sign); 90% specific, 45% sensitive.
Pain increases with shoulder abduction on the side
of neck pain (increased pain could derive from
rotator cu�–related pain; radicular pain may
decrease with this maneuver).
Pain may worsen with Valsalva, which increases
intrathecal pressure.
Repetitive movement of arm or shoulder at work or
play; may be new activity.
Flex neck forward until chin meets chest or pain stops
movement. An electric shock sensation radiating
down spine into both arms is a positive result
(Lhermitte's sign). Occasionally, paresthesias occur.
History of recent injury or recent event of awkward
position (such as neck or head position during
sleep in an unfamiliar setting) or awkward standing
posture to accommodate a special situation.
Depressed reflexes or, uncommonly, increased
reflexes (see also Table 279-3).
Pain is accompanied by "sti�ness" of involved
muscle group.
PHYSICAL EXAMINATION IN PATIENTS WITH NECK PAIN
Begin with a general assessment of the patient, noting evidence of weight loss, pallor, adenopathy, and
abnormalities of posture, movement, and facial expression.5 Pain may cause splinting of the head on theshoulders during position change. Assess active and passive movement, including rotation (chin toshoulder), lateral flexion (ear to shoulder), and flexion-extension (chin down, then up). Most mechanicalcauses of neck pain result in asymmetric lesions and asymmetrically limited or painful movements, whereasinflammatory or neoplastic disorders are typically more widespread, with pain and movement restriction
being more symmetric.5 When localized ipsilateral neck pain is felt toward the side of head movement,

6/11/2019
5/26
suspect facet (zygapophyseal) joint irritability. Examine for Spurling's sign (see Table 279-2). The abductionrelief sign, performed by having the patient place the hand of the a�ected upper extremity on the top of hisor her head to obtain relief, may indicate so� disk protrusion causing radicular pain. When neck pain occurson the side away from head movement, suspect a ligamentous or muscular source.
Palpate the posterior cervical triangle, the supraclavicular fossa, carotid sheaths, and the anterior neck. C5-C6 root lesions o�en elicit tenderness over the brachial plexus at Erb's point, 2 to 3 cm above the clavicle,midway up the posterior border of the sternocleidomastoid muscle in the posterior triangle of the neck. A C8-T1 root lesion may cause tenderness over the ulnar nerve at the elbow.
Pathology in the lymph nodes, salivary glands, or thyroid gland may cause neck pain. A bruit over the carotidmay signal cerebral insu�iciency; a bruit over the subclavian arteries may be associated with thoracic outletor vascular steal syndrome. Examine the temporal artery for tenderness, because temporal arteritis may bethe cause of neck and shoulder pain (see also chapter 165, "Headache").
Sensory symptoms of pain or dysesthesias are di�icult to evaluate, particularly when motor signs are absent,which is o�en the case in cervical spinal radiculopathies. The discrete separation of the motor and sensoryroots at the cervical neural foramina can explain motor sparing despite severe sensory symptoms. Forexample, C7 root irritability without motor weakness can present as aching at the medial to middle scapularborder; aching in the myotome distribution to the chest, axilla, or triceps; or numbness or tingling in themiddle finger.
Early detection of cervical spinal myelopathies requires a complete neurologic examination. Hyperreflexia, apositive Babinski's sign, clonus, gait disturbance, sexual or bladder dysfunction, lower extremity weakness,impaired fine hand movement, and upper and lower extremity spasticity may signal myelopathy. Examine forLhermitte's sign (Table 279-2), which is indicative of possible cord compression. Ho�man's sign indicates anupper motor neuron lesion and is performed by flicking the tip of the middle finger as the hand is relaxed in aneutral position. A positive (abnormal) response is flexion of the thumb and index finger in a pinchingmotion.

6/11/2019
6/26
TABLE 279-3
Signs and Symptoms of Cervical Radiculopathy
Disk
Space
Cervical
RootPain Complaint
Sensory
Abnormality
Motor
WeaknessAltered Reflex
C1-C2 C2 Neck, scalp Scalp
C4-C5 C5 Neck, shoulder, upper arm Shoulder Infraspinatus,
deltoid,
biceps
Reduced
biceps reflex
C5-C6 C6 Neck, shoulder, upper medial,
scapular area, proximal forearm,
thumb, index finger
Thumb and
index finger,
lateral
forearm
Deltoid,
biceps,
pronator
teres, wrist
extensors
Reduced
biceps and
brachioradialis
reflex
C6-C7 C7 Neck, posterior arm, dorsum
proximal forearm, chest, medial
third of scapula, middle finger
Middle
finger,
forearm
Triceps,
pronator
teres
Reduced
triceps reflex
C7-T1 C8 Neck, posterior arm, ulnar side of
forearm, medial inferior scapular
border, medial hand, ring, and
little fingers
Ring and
little fingers
Triceps, flexor
carpi ulnaris,
hand
intrinsics
Reduced
triceps reflex
Table 279-3 summarizes the sensory, motor, and reflex findings in cervical radiculopathy. This informationshould be used to determine the level of motor and sensory involvement and to compare findings in thea�ected and una�ected sides. Bilateral or multilevel involvement usually implies serious pathology.
DIAGNOSIS OF NECK PAIN
Laboratory testing is rarely helpful, unless considering infection. See the "Epidural Compression Syndrome,""Transverse Myelitis," and "Spinal Infection" sections later in this chapter, as well as chapter 246, "Neck andUpper Airway."
The need for imaging studies depends on the clinical condition suspected and the duration of neck pain.Acute (days to weeks), uncomplicated, nonradicular, nonmyelopathic, atraumatic neck pain typically
requires no imaging because the cause is likely benign and the treatment is conservative.5 Obtain three-view

6/11/2019
7/26
cervical spine films in patients with chronic (weeks to months) neck pain with or without a history of trauma,
those with neck pain and a prior history of malignancy or remote neck surgery,5 and those with neck painand preexisting spinal disorders such as rheumatoid arthritis, ankylosing spondylitis, and psoriaticspondyloarthropathy. Flexion-extension films may be useful if instability is suspected, especially in patients
with rheumatoid arthritis or other inflammatory arthritides.6 Patients with normal radiographs, patients withradiographic evidence of degenerative changes without neck instability, or patients with radiographic
evidence of previous trauma and no neurologic signs or symptoms require no further imaging.5 MRI isindicated for patients with chronic neck pain with neurologic signs or symptoms regardless of the plain
radiographic findings.5 MRI is also indicated when plain radiographs reveal bone or disk margin destruction,
if there is cervical instability, and (with intravenous contrast) if epidural abscess or malignancy is suspected.5
CT myelography is recommended when contraindications to MRI exist.
DIFFERENTIAL DIAGNOSES OF NECK PAIN
Mechanical Neck Disorders
Mechanical neck disorders are also called hyperextension strain, acceleration-deceleration injury,hyperextension-hyperflexion injury, neck strain, neck sprain, and whiplash. The most common precipitatingevents are motor vehicle collisions, falls, sports injuries, and work-related injuries (see chapter 258, "SpineTrauma" for discussion of acute injury). Strain injury, caused by an awkward position during sleep orprolonged abnormal head-neck positions during work or recreation, is another cause.
Cervical Disk Herniations
Cervical disk herniations occur as the nucleus pulposus protrudes through the posterior annulus fibrosis,producing an acute radiculopathy or, occasionally, a myelopathy. Protrusions are usually confined by theposterior longitudinal ligament but can occasionally extrude through this ligament as free fragments. Directposterior ruptures, although infrequent, can produce progressive myelopathy, whereas the more commonposterolateral herniations can cause acute cervical radiculopathy. The levels of most frequent involvementare C5-C6 (C6 root) and C6-C7 (C7 root).
The symptoms of an acute cervical disk prolapse include neck pain, headache, pain distributed to theshoulder and along the medial scapular border, dermatome pain, and dysesthesia in the spinal rootdistribution to the shoulder and arm. Motor signs include fasciculations, atrophy and weakness in thedermatome distribution of the spinal root, loss of deep tendon reflexes, and, with cervical myelopathy, lowerextremity hyperreflexia, Babinski's sign, and in rare cases, loss of sphincter control. Cervical hyperextensionand lateral flexion to the symptomatic side (Spurling's sign; see Table 279-2) may replicate the symptoms, ascan a Valsalva maneuver, whereas manual cervical distraction in flexion alleviates them. A thorough physicalexamination, including strength, sensory, and reflex testing, may delineate the level of root involvement (seeTable 279-3). MRI is necessary for diagnosis.

6/11/2019
8/26
Cervical Spondylosis and Stenosis
Cervical spondylosis (or degenerative disk disease or osteoarthritis) is a progressive, degenerative conditionresulting in a loss of cervical flexibility, neck pain, occipital neuralgia, radicular pain, or occasionallyprogressive myelopathy. There is progressive degeneration of the disks, ligaments, facet joints(zygapophyseal joints), and uncovertebral joints (joints of Luschka). From a radiographic standpoint, cervicalspondylosis may be diagnosed if any one of three findings is present: osteophytes, disk space narrowing, orfacet disease. However, there is a high prevalence of cervical spondylosis in asymptomatic individuals, andcare must be taken in ascribing painful syndromes to findings on imaging. Degenerative disk diseasepredisposes a patient to progressive osteoarthrosis of the cervical spine, joint instability, and incongruousjoint motion during neck movement. Spondylosis most commonly occurs at the C5-C6 and C6-C7 levels.
Osteophytic spurs can encroach posteriorly on the spinal canal, producing cervical myelopathy; laterally onthe intervertebral foramen, producing cervical radiculopathy; and anteriorly on the esophagus, producingdysphagia. Spurious osteophytes may also produce Horner's syndrome, vertebrobasilar symptoms, severeradicular symptoms without associated neck pain, painless upper extremity myotome weakness, and chestpain mimicking angina. Neurologic findings (radiculopathy or myelopathy) may be gradual in onset unlessthere is a history of recent trauma.
The combination of a congenitally narrowed spinal canal, further compromised by a vertebral osteophyticbar anteriorly and a buckling ligamentum flavum posteriorly, increases the risk of myelopathy secondary tocervical spinal stenosis as the diameter of the spinal canal is reduced to less than 13 mm.
Cancer of the Cervical Spine
Consider metastatic cancer in the di�erential diagnosis of chronic neck pain, especially unremitting nightpain. Lung, breast, and prostate cancers and lymphoma and multiple myeloma may involve the cervicalspine. Although most cases of epidural cord compression occur in the thoracic spine, involvement of thecervical spine and multiple levels are not unusual. Myelopathy, which is commonly caused by disk ordegenerative disease, is rarely caused by metastatic tumors. Plain films have inadequate sensitivity (10% to17% false-negative rate) in detecting spinal metastases but may reveal destruction of the vertebral bodies,lytic lesions of the pedicles, and pathologic compression fractures. MRI is the standard for the detection ofspinal epidural metastatic disease and cord compression, and cancer patients with radiographic evidence of
bone or disk margin destruction should undergo MRI.5
Cervical Myofascial Pain Syndrome
Myofascial pain syndrome is a cause of chronic neck pain and is o�en confused with radiculopathy.Myofascial pain symptoms may present or exacerbate acutely, especially a�er trauma. Psychological distressand specific personality traits are risk factors. Typically, patients complain of pain in the neck, scapula, andshoulder with or without nondermatomal radiation into the upper extremity. Tender spots, "trigger points,"may be evident on palpation of the head, neck, shoulder, and scapular region. Neurologic examination is

6/11/2019
9/26
normal. Because radiographic cervical spine abnormalities develop with age in the asymptomaticpopulation, radiographic findings cannot be relied upon to verify the source of neck pain or upper extremitysymptoms. Imaging reveals either nonspecific degenerative or disk changes that do not correlate with theclinically suspected site.
Other Conditions
Epidural abscess, osteomyelitis, and transverse myelitis are infectious and inflammatory causes of neck pain(see related sections later in this chapter). Cervical spinal epidural hematoma o�en presents as neck painfollowed by symptoms and signs of cord compression (see later section on epidural compression syndrome)and should be considered in the patient taking anticoagulants or in the patient with a bleeding diathesis.Pain from ischemic heart disease may radiate into the neck and shoulder. Peripheral nerve involvement, suchas carpal tunnel syndrome, may present as a C6-C7 sensory radiculopathy, whereas multiple sclerosis,amyotrophic lateral sclerosis, subacute combined degeneration, and syrinx are in the di�erential ofmyelopathy.
TREATMENT AND DISPOSITION OF PATIENTS WITH NECK PAIN
Treatment issues can be divided into three categories: neck pain, neck and arm pain consistent withradiculopathy, and myelopathy. There is little evidence-based science to support many of the commonlyrecommended conservative treatment modalities (e.g., physiotherapy, acupuncture, electrotherapy,
manipulation, traction, thermotherapy, medicinal and injection therapies, exercises).7,8,9,10,11 Individualpatients may indeed benefit from one or more of these therapies.
TREATMENT OF UNCOMPLICATED NECK PAIN
Most cases of neck pain without clear underlying pathology will improve with minimal intervention. Thepatient should be advised to "act as usual" and avoid activities that produce pain. Initial medications mayinclude nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, and for significant pain, a shortcourse of oral opiates; no NSAID, muscle relaxant, or opiate is clearly superior to another in its class.Encourage follow-up with the primary physician to assess the need for physical or manual therapies oradditional medications.
Patients with acute neck pain following an acceleration-deceleration (whiplash) injury may benefit from asimilar pharmacologic regimen as that described earlier. In a Danish study of 458 patients, immobilizationwith a semi-rigid collar, advice to "act as usual," and active mobilization had similar e�ects in terms of
preventing long-lasting pain and disability.12 A so� collar reduces range of motion of the neck less than 20%
and provides little immobilization or neck support.13 If a so� collar is given, it should be used for no morethan 10 days. Spinal manipulation therapy or home exercises a�er two 60-minute physical therapy sessions
may each be more e�ective than medication therapy for short- and long-term pain relief.14

6/11/2019
10/26
Therapy for neck pain from myofascial pain syndrome should address both muscular tension andpsychobehavioral issues. See chapter 38, "Chronic Pain" for further discussion including recommendationsfor alternative therapies.
TREATMENT OF CERVICAL RADICULOPATHY
In the absence of myelopathy, first-line treatment is conservative activity modification to prevent symptomexacerbation or injury and oral medications. Immobilization with a so� or hard cervical collar is controversialwithout clear evidence for or against its use. Encourage follow-up with a primary physician for possiblereferral to a neurosurgical or orthopedic spine specialist, an electrodiagnostic evaluation, and additionalrehabilitation interventions. Oral medications may include NSAIDs, opioid analgesics, and muscle relaxants.A 7- to 10-day course of oral steroids (e.g., methylprednisolone or prednisone) is commonly prescribed foracute radiculopathy, but steroid e�icacy has been shown in only small low-quality studies of low back pain.Epidural steroid injections may be e�ective for chronic cervical radiculopathy when other treatments havefailed. If the symptoms and signs of acute cervical root compression fail to respond to conservativetreatment, or if they recur, and if imaging demonstrates concordant findings, surgery may be recommended.Indications for hospital admission include progressive upper extremity weakness, especially in the C7distribution; acute or progressive symptoms or signs of myelopathy; and finally, in a small subset of patients,intracTable radicular pain unresponsive to treatment.
TREATMENT OF CERVICAL MYELOPATHY
Treatment decisions for patients with symptoms and signs of cord compression should be made inconjunction with specialists. Cervical spondylotic myelopathy causes the greatest degree of impairment anddisability in the continuum of spondylosis. Also, myelopathy is the most common cause of spasticparaparesis in patients older than 55 years of age, thus paralleling the time course of spondylosis. Thepatient with myelopathy should be referred to a neurosurgeon or orthopedic spine surgeon to discuss thepossibility of decompressive surgery. Additional therapeutic considerations (e.g., steroids and radiation inspinal epidural metastases) will depend on the time course of symptoms and signs and etiology but shouldbe addressed in conjunction with a neurosurgeon.
CLINICAL FEATURES OF THORACIC AND LUMBAR PAIN SYNDROMES
Back pain is categorized based on the duration of symptoms: acute back pain lasts <6 weeks, subacute pain
lasts between 6 and 12 weeks, and chronic pain continues beyond 12 weeks.15 Pain lasting >6 weeks is anindicator of more serious disease, since most episodes of nonspecific back pain (80% to 90%) resolve within6 weeks. Risk factors for serious causes of back and neck pain are listed in Table 279-1; specific historicalfactors that help to identify benign verses serious causes of back pain are listed in the following sections.
HISTORICAL RISK FACTORS IN BACK PAIN
Patient Age

6/11/2019
11/26
In patients <18 years old and >50 years old, back pain is more likely to be caused by tumor or infection thanin the 18- to 50-year-old age group. Patients <18 years old also have a higher incidence of congenital andbony abnormalities such as spondylolysis, spondylolisthesis, and Scheuermann's kyphosis. Patients >50years old are more prone to fractures (age >65 years is more specific for fracture), spinal stenosis, and intra-abdominal processes such as an abdominal aortic aneurysm.
Pain Location and Radiation
Pain that originates from muscular, ligamentous, vertebral, or disk disease without nerve involvement islocated primarily in the back, possibly with radiation into the buttocks or thighs. Sciatica, radicular back pain
in the distribution of a lumbar or sacral nerve root, is o�en accompanied by sensory or motor deficits.15
Sciatica occurs in only 1% of patients with back pain and is associated with disk herniation or nerve rootimpingement below the L3 nerve root. Ninety-five percent of herniated disks occur at the L4-L5 or the L5-S1
lumbar disk spaces, impinging on the L5 or S1 nerve roots, respectively.15
Trauma
History of major trauma is a risk factor for fracture in all patients. In the elderly, minor trauma, such as fallingfrom standing or from sitting in a chair, may cause fracture due to associated osteoporosis. Risk factors forosteoporosis increase the incidence of compression fractures (i.e., female sex, steroid use, alcoholism).
Systemic Complaints
Systemic symptoms such as fever, chills, night sweats, malaise, and an undesired weight loss suggestinfection, systemic rheumatologic disease, or malignancy. These symptoms are more concerning forinfection if the patient has any of the following risk factors: recent bacterial infection (including urinary tractinfection, pneumonia, and especially skin abscesses), recent GU or GI procedure, immunocompromised
status, injection drug use, alcoholism, renal failure, or diabetes.16,17,18 Injection drug use is a substantial riskfactor for spinal infection, so assume that back pain in a patient who is an injection drug user is due to spinalinfection until proven otherwise.
A rupturing abdominal aortic aneurysm is the most immediately life-threatening extraspinal cause of backpain. Other potential causes of pain referred to the back include pancreatitis, a posterior lower lobepneumonia, nephrolithiasis, and renal infarct.
Pain Features
A dull, aching pain that generally worsens with movement but improves with rest and lying still is the typicaldescription of benign back pain. Symptoms suggestive of tumor and infection include pain that occurs atnight and o�en awakens the patient from sleep or that is unrelenting despite appropriate use of analgesics
and rest.15,19 Pain worsened by coughing, Valsalva maneuver, or sitting and that is relieved by lying in thesupine position suggests herniation. Spinal stenosis is associated with bilateral sciatic pain that is worsened

6/11/2019
12/26
by activities such as walking, prolonged standing, and back extension and is relieved by rest and forwardflexion. In the authors' experience, night pain and unrelenting pain are worrisome symptoms that should bespecifically queried as part of the history, because these symptoms are risk factors for serious disease andsuch queries are o�en omitted in history taking.
Neurologic Deficit by History
Neurologic complaints such as paresthesias, numbness, weakness, and gait disturbances must be furtheraddressed in the history and delineated in the physical examination to determine whether the symptomsinvolve single or multiple nerve roots. Bowel or bladder incontinence is a serious symptom that raisesconcern for an epidural compression syndrome, such as spinal cord compression, cauda equina syndrome,or conus medullaris syndrome. If a patient has back pain and has a history of urinary incontinence (acute orchronic), but an otherwise completely normal history and evaluation, measure the postvoid residual volumewith bedside US or by catheterization if US findings are in doubt. A large postvoid residual volume (e.g., >100mL) indicates overflow incontinence, which, when combined with the presence of low back pain, suggests
neurologic compromise and an epidural compression syndrome.15,20
Past Medical History
History of cancer is a risk factor because back pain is the initial symptom in the majority of those with spinal
metastases.20 Malignant neoplasm is the most common systemic disease a�ecting the spine. Most patientswith this diagnosis are >50 years old. However, only one third of patients diagnosed with spinal malignancyhave a known history of cancer. Thus, symptoms such as unremitting pain, night pain, and weight lossrequire further diagnostic testing.
PHYSICAL EXAMINATION RISK FACTORS IN BACK PAIN
Although fever is a marker of infection, sensitivity for infection is low, varying from 27% for tuberculousosteomyelitis to 50% for pyogenic osteomyelitis, 60% to 70% for pyogenic discitis, and 66% to 83% for spinal
epidural abscess.16,19 Careful history, examination, and possibly diagnostic testing are needed for patientswith back pain and fever. In patients with severe or excessive pain, consider acute spinal infection orabdominal aortic aneurysm. Examine the abdomen, listen for bruits, and palpate for masses, tenderness,and an enlarged aorta.
Examine the back for signs of erythema, warmth, skin abscesses, furuncles, and purulent drainage, whichsuggest an underlying spinal infection. Contusion and swelling suggest trauma. Palpate the back and percussthe vertebral bodies. Consider fracture or bacterial infection if there is point tenderness to vertebralpercussion. Perform straight leg raise testing. With the patient lying supine, li� each leg separately toapproximately 70 degrees in an attempt to produce radicular pain. A positive straight leg raise test causes aradicular pain radiating below the knee of the a�ected leg. This pain is worsened by ankle dorsiflexion andimproved with ankle plantar flexion or decreasing leg elevation. Reproduction of the patient's back pain or

6/11/2019
13/26
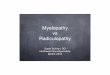
pain in the gluteal or hamstring area when the leg is raised is not a positive result. The straight leg raise testcan be easily replicated with the patient in the seated position with similar leg extension and footdorsiflexion (Figure 279-1). Straight leg raise testing is a screening examination for a herniated disk. One thirdof those with positive straight leg raising test and a negative sitting knee extension test have an MRI-proven
herniated disk.21 A positive straight leg raise test is 68% to 80% sensitive for a L4-L5 or L5-S1 herniated
disk.21 Radicular pain down the a�ected leg when li�ing the asymptomatic leg is called a positive crossedstraight leg raise test. A positive result is highly specific but insensitive for nerve root compression by aherniated disk.
FIGURE 279-1.
Sitting knee extension test. With the patient sitting on a table, both hip and knees flexed at 90 degrees, slowlyextend the knee as if evaluating the patella or bottom of the foot. This maneuver stretches nerve roots asmuch as a moderate degree of supine straight leg raising.
Neurologic Examination For Back Pain
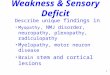
The neurologic examination is directed to detecting deficits in each of the specific spinal nerve roots.Sensation may be tested by using light touch initially, followed more formally by pinprick, temperature,proprioception, and vibration testing if there are any questions regarding diminished sensation. Next assessstrength, with a focus on those muscle groups innervated by individual nerve roots (Figure 279-2).Individually test the ankle dorsiflexors (L4), extensor hallucis longus (great toe dorsiflexion) (L5), and ankleplantar flexors (S1/S2). Finally, evaluate the patellar (L3-L4), Achilles (S1), and Babinski's reflexes. There is noeasily obtainable reflex for the L5 nerve root.
FIGURE 279-2.
Testing for lumbar nerve root compromise.

6/11/2019
14/26
It is not necessary to perform a digital rectal examination on all patients with back pain. However, performrectal examination in patients with neurologic complaints or findings on physical examination and thosewith risk factors for serious disease. Evaluate rectal sphincter tone and perianal sensation and the presenceof prostatic and rectal masses. Poor rectal tone in association with back pain and saddle anesthesia indicatesan epidural compression syndrome.
DIAGNOSIS OF BACK PAIN SYNDROMES
For most patients, no testing is required. However, laboratory testing is indicated in the ED if there is concernfor infection, tumor, or rheumatologic causes of the back pain. Order a CBC, erythrocyte sedimentation rate,and urinalysis. With infection, the WBC count may be normal or elevated. However, the erythrocyte

6/11/2019
15/26
sedimentation rate is typically elevated (>20 mm/h), even in immunocompromised patients, with a
sensitivity of 90% to 98% for spine infection.16,19,22 The erythrocyte sedimentation rate will also be elevated
in patients with a rheumatologic or neoplastic disease of the spine.15 The C-reactive protein will also be
elevated with acute spinal infection.15,19 Obtain a urinalysis to identify urinary tract infection or renal diseasecausing pain referred to the back.
IMAGING
Plain spinal radiographs can be considered when one suspects fracture, tumor, or infection, but sensitivity isonly 83% for tumor and very poor for infection. Anteroposterior and lateral views are su�icient. The coned-down L5-S1 and oblique views rarely add clinically useful information while more than doubling gonadalradiation exposure and cost.
CT scanning is most useful for evaluating vertebral fractures, the facet joints, and the posterior elements ofthe spine. It shows good detail of the vertebral bodies but has poor resolution of the spinal canal and spinalcord in comparison with MRI. CT may be useful if MRI is unavailable or unsuitable, but CT myelography is thebest substitute for conditions such as epidural abscess or cord compression when MRI is unavailable.
MRI provides the best resolution for lesions in the vertebral bodies, spinal canal, and spinal cord, and for diskdisease. MRI is also the standard study in cases of suspected spinal infection, neoplasm, and epiduralcompression syndromes. MRI is also used to determine progression of neoplastic processes of the spine anddisk disease and for continued back pain for 6 to 8 weeks.
DIFFERENTIAL DIAGNOSIS AND MANAGEMENT OF BACK PAINSYNDROMES
ACUTE NONSPECIFIC BACK PAIN
Nonspecific back pain is a symptom complex that has countless names, including back strain/sprain,mechanical back pain, and lumbago. However, because strain and/or sprain have no histopathologicfindings, a more accurate term to use is idiopathic or nonspecific back pain. Nonspecific back pain is theauthors' choice of term, especially because most patients will never be given a more precise diagnosis.
Diagnosis is clinical. The pain is mild to moderate and is aggravated with movement and relieved with rest.Although the typical mechanism is usually minor exertion or li�ing, the patient may not recall anyremarkable etiology. There are no risk factors for serious disease on the history and physical examination, orif any risk factors are present, the diagnostic evaluation is normal.
Treatment focuses on restriction of activity, analgesia, manipulation, and other physical modalities. Monitorsymptoms for 4 to 6 weeks before embarking on further diagnostics. In 80% to 90% of patients, symptoms
will resolve on their own within this time period.15 Watchful waiting avoids wasting time and money and

6/11/2019
16/26
eliminates exposure to unnecessary radiation. This course of action should be discussed with patientsbecause they may expect diagnostic testing.
Patients who resume their normal activities to the furthest extent tolerable recover more rapidly than those
on 2 or 7 days of bed rest or those who perform back-mobilizing exercises.23 Thus, patients should continue
daily activities using pain as the limiting factor.15 Withhold exercise programs until the acute painful episodehas resolved or improved significantly.
Medication is a combination of acetaminophen and NSAIDs. Acetaminophen is an excellent first-line agent,
and there is little evidence that NSAIDs are more e�ective for symptomatic relief.24,25 Most NSAIDs areequally e�icacious for back pain. However, there are significant di�erences in the side e�ect profiles andtoxicity. In one review, ibuprofen was the least toxic of the 12 NSAIDs studied, particularly with regard toupper GI bleeding. Because there is a linear relationship between dose and toxicity, the lowest dose possibleshould be used in patients at risk. In patients at risk for GI bleeding, the addition of a proton pump inhibitor
or misoprostol can reduce the risk.25
We recommend using acetaminophen in combination with NSAIDs or as the sole initial agent when treatingpatients at higher risk for adverse e�ects of NSAIDs (the elderly and those with renal disease or peptic ulcers).One regimen is acetaminophen, 650 to 975 milligrams every 4 to 6 hours (do not exceed 4 grams in a 24-hourperiod), either alone or in conjunction with ibuprofen, 800 milligrams three times daily, or naproxen, 250 to500 milligrams twice daily. If there is a concern for GI bleeding, then add a proton pump inhibitor such asomeprazole, 20 milligrams once daily.
Opioid analgesics should be o�ered to patients with moderate to severe pain, but for a limited (1 week)
duration, as they are only e�ective in the short term.15,24,26 When prescribing opioid analgesic combinationsthat include acetaminophen, warn patients not to combine them with other acetaminophen products.
Muscle relaxants are useful for treating back pain.26 Muscle relaxants, such as diazepam, 5 to 10 milligramsevery 6 to 8 hours, and methocarbamol, 1000 to 1500 milligrams four times a day, are e�ective. Althoughtheir e�icacy appears equal to NSAIDs, there are no studies comparing muscle relaxants alone with NSAIDs inthe treatment of nonspecific low back pain. Additionally, there does not appear to be any additional pain
relief or synergistic benefit when these medications are used in combination.27 Corticosteroids takensystemically or injected locally or into the epidural space have no role in the treatment of nonspecific back
pain.15,28
Manipulative therapy, while not generally an ED treatment, is one of the more controversial treatmentoptions for back pain. Clinical outcome of manipulation is no better than standard medical therapy
according to a Cochrane review,29 but is not harmful.15
Other physical modalities include traction, diathermy, cutaneous laser treatment, exercise, US treatment,and transcutaneous electrical nerve stimulation. None of these have any proven e�icacy in the treatment of

6/11/2019
17/26
acute low back symptoms. The application of heat or ice may provide temporary symptomatic relief in some
patients, with evidence favoring heat.15
CHRONIC NONSPECIFIC BACK PAIN
There is a higher concern for serious disease in patients with ongoing or intermittent symptoms for a timeperiod of months to years. The best approach is to review the previous evaluations for completeness and tobe sure that abnormalities were not overlooked. If the evaluation has been incomplete, then considercompleting it in the ED at that visit, or facilitate referral for an outpatient evaluation, with urgency guided bythe severity of symptoms. If the evaluation has been thorough but negative, then treat as described fornonspecific back pain. If opioid analgesics are needed, prescribe them for only a very limited time. Chronic
back pain is a di�icult condition to manage, and benefit of medications is small.15,24,26,30 Furtherinformation on the management of chronic back pain can be found in chapter 38.
LOW BACK PAIN WITH SCIATICA
Although sciatica only a�ects a very small proportion of all patients with back pain, it is present in the vastmajority of patients with a symptomatic herniated disk. Although disk herniation is the most common causeof sciatica, anything that compresses or impinges on the spinal nerve roots, cauda equina, or spinal cord cancause sciatica. Other important etiologies to consider in the ED include intraspinal tumor or infection,foraminal stenosis, extraspinal plexus compression, piriformis syndrome (see chapter 281, "Hip and KneePain"), and lumbar canal stenosis (spinal stenosis).
DISK HERNIATION
Diagnosis is suspected clinically and confirmed with nonurgent MRI (urgent MRI only in the setting ofsuspected spinal cord compression). Patients who present with sciatica due to a herniated disk generallycomplain more about the radicular symptoms than about back pain. Because the vast majority of diskherniations occur at the L4-L5 (L5 nerve root) or L5-S1 (S1 nerve root) level, the radicular pain extends belowthe knee in the dermatomal distribution of that nerve root. A small proportion (o�en the elderly) have diskherniation at the L2-L3 (L3 nerve root) and L3-L4 (L4 nerve root) levels. The physical examination generallydemonstrates localization of pain and a neurologic deficit in a unilateral single nerve root, usually L5 or S1,and frequently includes a positive result on straight leg raise testing.
If the patient has no risk factors in the history and physical examination for serious disease other than
sciatica, treat conservatively and do not perform any diagnostic tests in the ED.15 If the patient has ademonstrable neurologic deficit, consider obtaining plain radiographs to look for other possible causes forsymptoms such as tumor, fracture, spondylolisthesis, and infection. Guidelines recommend imaging (MRIpreferred) in patients with severe or progressive neurologic deficits and those with serious underlying
conditions suspected based on history or physical examination.15 If the symptoms have not progressedrapidly or the symptoms are not severe, the MRI can be ordered routinely or urgently rather than emergently.

6/11/2019
18/26
Treatment is as for nonspecific back pain. Routine daily activity is as good as 2 weeks of bed rest in terms of
intensity of pain, distress associated with symptoms, and functional status.23 Recommendations for
analgesic (acetaminophen, NSAID, and opiates) and muscle relaxant therapy remain the same.31 NSAIDs areless e�ective in treating the symptoms of a herniated disk than they are in treating nonspecific back pain.
Corticosteroid therapy for herniated disk has limited benefit. Specifically, epidural corticosteroid injectionprovides a minor reduction in leg pain and sensory deficits in comparison with placebo. However, theimprovement in symptoms is not associated with any significant functional benefit, and it does not reducethe need for surgery. Although epidural steroid injection is not an ED procedure, it o�ers an alternative forthe moderately to severely symptomatic patient in follow-up. Although oral steroids are used widely, theyappear to have little measurable benefit in patients with sciatica.
Manipulation is not recommended for the routine management of symptoms from herniated disk.29 Localapplication of heat or ice may provide temporary relief.
Most patients with a herniated disk may be treated and monitored by their primary care physician withoutspecialist referral. Most patients ultimately improve with nonsurgical therapy, with over half recovering in 6weeks. Most spine surgeons agree that surgery is appropriate only when all three of the following criteria aremet: definitive evidence of herniation on imaging study; corresponding clinical picture and neurologicdeficit; and conservative treatment for 4 to 6 weeks that fails to produce improvement.
Emergency decompressive surgery is required only in patients with acute epidural compression syndromes.Patients who underwent surgery had improved function and fewer symptoms at 1 and 2 yearspostoperatively, compared with those treated conservatively; however, by 4 and 10 years postoperatively,
both groups had comparable results.32,33
SPINAL STENOSIS
Spinal stenosis is a narrowing of any part of the lumbar spine, including the spinal canal, nerve root canal,and intervertebral foramina, which may occur at single or multiple spinal levels. Degenerative disease causesnarrowing and compression of vascular and neural structures. It is a cause of chronic back pain, with orwithout associated sciatica. The symptoms, which usually begin in the sixth decade, include low back painthat is aggravated by prolonged standing and spinal extension and is relieved by rest and forward flexion.Typically, symptomatic patients present with low back and lower extremity pain while walking that issymptomatically similar to vascular claudication. This symptom is termed neurogenic claudication orpseudoclaudication to distinguish it from vascular claudication. Neurogenic claudication is relieved with rest
and forward flexing the spine and worsened by extending the spine.34 Physical examination findings areo�en absent. The diagnosis is made principally by history with confirmation by CT scan or MRI. Symptomatictreatment is the same as chronic back pain with primary care follow-up.
ANKYLOSING SPONDYLITIS

6/11/2019
19/26
Ankylosing spondylitis is an autoimmune arthritis that primarily a�ects the spine and pelvis. It is associatedwith human leukocyte antigen B-27, trauma, and infection. It most commonly occurs in patients <40 yearsold with a 3:1 male predilection. Patients complain of awakening with low back pain and sti�ness thatimproves throughout the day with mild activity. The diagnosis is suspected by history and physical exam inindividuals with symptoms longer than 3 months in duration and is confirmed by imaging and laboratorytests. Radiographic studies demonstrate sacroiliitis and squaring of the vertebral bodies, the so-calledbamboo spine. Patients can be treated symptomatically with NSAIDs and should be referred to arheumatologist for diagnostic confirmation and further management.
EPIDURAL COMPRESSION SYNDROME
Epidural compression syndrome is a collective term encompassing spinal cord compression, cauda equinasyndrome, and conus medullaris syndrome.
Although the diagnosis of a complete epidural compression is obvious, the challenge is diagnosis in patientswith early signs and symptoms. The initial di�erential diagnosis is broad and includes most conditions thatcause weakness, sensory changes, or autonomic dysfunction of the lower extremities. The history andphysical examination should narrow the di�erential diagnosis to a compressive lesion of the spinal cord orcauda equina.
Possible causes of epidural compression include spinal canal hemorrhage with hematoma, tumors of thespine or epidural space, spinal canal infections including spinal epidural abscess, and massive midline diskherniation. Transverse myelitis is a noncompressive condition that may present clinically like a compressivelesion of the spinal cord.
The history usually includes back pain with associated neurologic deficits. Specifically, it may includeperianal sensory loss, fecal incontinence or urinary incontinence with or without retention, and sciatica inone or both legs. The duration of symptoms does not di�erentiate these syndromes from benign causes ofback pain. In one small study, urinary retention of >500 mL alone or in combination with two of the followingcharacteristics—bilateral sciatica, subjective urinary retention, or rectal incontinence symptoms—is the most
important predictor of MRI-confirmed cauda compressions.35 Also, a history of malignancy and a rapidprogression of neurologic symptoms, especially bilateral symptoms, increase the likelihood of compression.
The physical examination findings vary depending on the level of compression and the amount and area ofthe spinal cord or cauda equina that is compressed. The most common finding in cauda equina syndrome isurinary retention with or without overflow incontinence, with a sensitivity of 90% and a specificity of about
95%.35 Other common findings for epidural compression include weakness or sti�ness in the lowerextremities, paresthesias or sensory deficits, gait di�iculty, and abnormal results on straight leg raise
testing.36 The most common sensory deficit occurs over the buttocks, posterosuperior thighs, and perinealregions and is commonly called saddle anesthesia. Anal sphincter tone is decreased in 60% to 80% of cases.

6/11/2019
20/26
When one clinically suspects epidural compression, especially due to tumor, treat the patient with
dexamethasone, 10 milligrams IV, before obtaining any confirmatory tests.36 A�er the patient has receiveddexamethasone, obtain an emergent MRI of the spine. If investigating the possibility of epidural compressiondue to neoplasm, obtain an MRI of the entire spine because 10% of patients with vertebral metastases have
additional silent epidural metastases that would be missed by a localized imaging study.36 The presence oftumors remote from the symptomatic site may change patient management. Additionally, the neurologicexamination may falsely localize the spinal lesion(s) and limited regional MRI may not detect the lesion. Ifone suspects a pure cauda equina syndrome from a herniated disk, then it is reasonable to obtain an MRIlocalized to the lumbosacral spine.
The functional clinical outcome for epidural compression from tumor depends on patient symptoms atpresentation. Patients who cannot walk before treatment rarely walk again. Those who are too weak to walkwithout assistance but who are not paraplegic have a 50% chance of walking again. Those who are able to
walk when treatment begins are likely to remain ambulatory.36 Of those patients who require a catheter forurinary retention before treatment, 82% will continue to require the urinary catheter a�er treatment. Thepresence of cord compresion is an indication for urgent consultation with a spine surgeon for decompression
and/or radiation therapy for a tumor mass, determined by MRI findings.37,38
TRANSVERSE MYELITIS
Transverse myelitis is an inflammatory disorder that involves a complete transverse section of the spinalcord. It usually presents with neck or back pain in association with neurologic complaints and findings onphysical examination, depending on the level of the spinal cord that is involved. The typical clinicalsyndrome involves bilateral motor, sensory, and autonomic disturbances that may progress over a period of
days to weeks. Fecal and urinary retention and incontinence are common.39 Transverse myelitis may resultfrom viral infection, a�er vaccination, or as part of a systemic disease such as systemic lupus erythematosus,cancer, or, more commonly, multiple sclerosis. The most important issue regarding transverse myelitis isrecognition of the potential for a compressive lesion of the spinal cord and managing the patient as outlinedunder epidural compression syndromes. The MRI may demonstrate lesions of the spinal cord, but MRI
findings may lag the clinical presentation, especially early in the disease process.38 In those situations wherethe patient has definite neurologic findings that are consistent with epidural compression but has a normalMRI, transverse myelitis is one of the primary working diagnoses. In such cases, consult a neurologist foradmission and consider performing a lumbar puncture to assist in the diagnosis. The spinal fluid most
commonly demonstrates lymphocytosis and elevated protein.38 Treatment includes corticosteroids and
plasma exchange at the direction of a neurologist.38
SPINAL INFECTION
Spinal infections, such as vertebral osteomyelitis, discitis, and spinal epidural abscess, are uncommon but
serious causes of back pain. Unfortunately, these infections are commonly missed on first assessment.19,22

6/11/2019
21/26
Risk factors for infection include the following: immunocompromised states (diabetes, HIV infection, andorgan transplant recipients), alcoholism, recent invasive procedures, spinal implants and devices, injection
drug use, and skin abscesses.16,19,22
Vertebral Osteomyelitis
Patients with vertebral osteomyelitis usually have had prolonged symptoms, and in many cases, pain has
been present for >3 months.19,40 On physical examination, about half have fever and vertebral body
tenderness to percussion.19,40 The WBC may be normal, but the erythrocyte sedimentation rate and C-
reactive protein are almost always elevated, although this is nonspecific.16,17,19,40 Blood cultures arepositive in approximately 40% of cases of vertebral osteomyelitis and should be routinely drawn as part ofthe management. In osteomyelitis, plain radiographs are normal until the bone demineralizes, which cantake from 2 to 8 weeks. The most common radiographic abnormalities with vertebral osteomyelitis are bony
destruction, irregularity of vertebral end plates, and disk space narrowing.19 See the section on osteomyelitisin chapter 281 for further discussion.
Discitis
In patients with discitis, >90% present with a complaint of unremitting back or neck pain, which awakens
them at night and is relieved by neither rest nor analgesics.19 Fever is present in 60% to 70% of patients,
whereas the percentage of patients with neurologic deficits is highly variable, from 10% to 50%.19 Elevationin the erythrocyte sedimentation rate occurs in >90% of patients, whereas elevated WBC count occurs in less
than half of patients.19
Spinal Epidural Abscess
The classic triad of symptoms suggesting spinal epidural abscess is severe back pain, fever, and neurologic
deficits, but the triad occurs in only 8% to 13% of patients.22 Spinal epidural abscess is commonly found in
association with vertebral osteomyelitis and discitis, in 62% and 38% of cases, respectively.16,22 Risk factors98% sensitive for epidural abscess include injection drug use, immunocompromise, alcohol abuse, recentspine procedure, distant site of infection, diabetes, indwelling catheter, recent spine fracture, chronic renal
failure, and cancer.22 Erythrocyte sedimentation rate is elevated (>20 mm/h) in >95% of patients,16,17,22 and
the C-reactive protein is elevated in >90% of patients.19 For all spinal infections, contrast-enhanced MRI is thegold standard imaging study. For detailed discussion, see chapter 174, "Central Nervous System and SpinalInfections."
Treatment of Spinal Infections
Epidural abscess requires antibiotics and emergent evaluation and treatment by a spine surgeon. Thetreatment for discitis is long-term antibiotics, with surgery reserved for those with spinal cord compression

6/11/2019
22/26
1.
2.
3.
4.
5.
6.
7.
8.
or biomechanical instability. The treatment for vertebral osteomyelitis is primarily medical, consisting of 6weeks of IV antibiotics followed by a 4- to 8-week course of oral antibiotics. For vertebral osteomyelitis,consult with a spine surgeon before antibiotic administration, because antibiotics may result in negativeculture results from a bone biopsy. However, do not withhold antibiotics unless specifically directed by thespine surgeon. Empiric antibiotic therapy should be directed against Staphylococcus aureus. Parenteralpiperacillin-tazobactam, 3.375 grams IV, and vancomycin, 1 gram IV, or similar agents with broad-spectrum
coverage can be given until culture results are available.17,18 The remainder of treatment is symptomatic.
REFERENCES
Waterman BR, Belmont PJ Jr, Schoenfeld AJ: Low back pain in the United States: incidence and riskfactors for presentation in the emergency setting. Spine J 12: 63, 2012.
[PubMed: 21978519]
Friedman BW, Chilstrom M, Bijur PE, Gallagher EJ: Diagnostic testing and treatment of low back pain inUnited States emergency departments: a national perspective. Spine 35: E1406, 2010.
[PubMed: 21030902]
Hoy D, March L, Brooks P et al.: The global burden of low back pain: estimates from the Global Burden ofDisease 2010 study. Ann Rheum Dis 73: 975, 2014.
[PubMed: 24665117]
Hoy D, March L, Woolf A et al.: The global burden of neck pain: estimates from the Global Burden ofDisease 2010 study. Ann Rheum Dis 73: 1309, 2014.
[PubMed: 24482302]
http://www.acr.org (American College of Radiology: ACR appropriateness criteria: chronic neck pain, 2013.)Accessed Januray 4, 2015.
Soderman T, Olerud C, Shalabi A et al.: Static and dynamic CT imaging of the cervical spine in patientswith rheumatoid arthritis. Skeletal Radiol 44: 241, 2015
[PubMed: 25227660]
Kroeling P, Gross A, Graham N et al. Electrotherapy for neck pain. Cochrane Database Syst Rev 8:CD004251, 2013.
[PubMed: 23979926]
Peloso P, Gross A, Haines T et al.: Medicinal and injection therapies for mechanical neck disorders.Cochrane Database Syst Rev 3: CD000319, 2007.
[PubMed: 17636629]

6/11/2019
23/26
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Kay TM, Gross A, Goldsmith CH et al.: Exercises for mechanical neck disorders. Cochrane Database SystRev 8: CD004250, 2012.
[PubMed: 22895940]
Verhagen AP, Scholten-Peeters GG, van Wijngaarden S, de Bie RA, Bierma-Zeinstra SM: Conservativetreatments for whiplash. Cochrane Database Syst Rev 2: CD003338, 2007.
[PubMed: 17443525]
Gross AR, Peloso PM, Galway E et al.: Physician-delivered injection therapies for mechanical neckdisorders: a systematic review update (non-oral, non-intravenous pharmacological interventions for neckpain). Open Orthop J 7: 562, 2013.
[PubMed: 24155806]
Kongsted A, Qerama E, Kasch H et al.: Neck collar, "act-as-usual" or active mobilization for whiplashinjury? A randomized parallel-group trial. Spine 32: 618, 2007.
[PubMed: 17413465]
Whitcro� KL, Massouh L, Amirfeyz R, Bannister GC: A comparison of neck movement in the so� cervicalcollar and rigid cervical brace in healthy subjects. J Manipulative Physiol Ther 34: 119, 2011.
[PubMed: 21334544]
Bronfort G, Evans R, Anderson AV, Svendsen KH, Bracha Y, Grimm RH: Spinal manipulation,medication, or home exercise with advice for acute and subacute neck pain: a randomized trial. Ann InternMed 156: 1, 2012.
[PubMed: 22213489]
Chou R, Qaseem A, Snow V et al.: Diagnosis and treatment of low back pain: a joint clinical practiceguideline from the American College of Physicians and the American Pain Society. Ann Intern Med 147: 478,2007.
[PubMed: 17909209]
Darouiche RO: Spinal epidural abscess. New Engl J Med 355: 2012, 2006. [PubMed: 17093252]
Pradilla G, Ardila GP, Hsu W, Rigamonti D: Epidural abscesses of the CNS. Lancet Neurol 8: 292, 2009. [PubMed: 19233039]
Tompkins M, Panuncialman I, Lucas P, Palumbo M: Spinal epidural abscess. J Emerg Med 39: 384, 2010. [PubMed: 20060254]

6/11/2019
24/26
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
Cottle L, Riordan T: Infectious spondylodiscitis. J Infect 56: 401, 2008. [PubMed: 18442854]
McCurdy MT, Shanholtz CB: Oncologic emergencies. Crit Care Med 40: 2212, 2012. [PubMed: 22584756]
Rabin A, Gerszten PC, Karausky P, Bunker CH, Potter DM, Welch WC: The sensitivity of the seatedstraight-leg raise test compared with the supine straight-leg raise test in patients presenting with magneticresonance imaging evidence of lumbar nerve root compression. Arch Phys Med Rehab 88: 840, 2007.
[PubMed: 17601462]
Davis DP, Wold RM, Patel RJ et al.: The clinical presentation and impact of diagnostic delays onemergency department patients with spinal epidural abscess. J Emerg Med 26: 285, 2004.
[PubMed: 15028325]
Dahm KT, Brurberg KG, Jamtvedt G, Hagen KB: Advice to rest in bed versus advice to stay active foracute low-back pain and sciatica. Cochrane Database Syst Rev 6: CD007612, 2010.
[PubMed: 20556780]
Chou R, Hu�man LH, American Pain Society, American College of Physicians: Medications for acute andchronic low back pain: a review of the evidence for an American Pain Society/American College of Physiciansclinical practice guideline. Ann Intern Medi 147: 505, 2007.
[PubMed: 17909211]
Kuritzky L, Samraj GP: Nonsteroidal anti-inflammatory drugs in the treatment of low back pain. J PainRes 5: 579, 2012.
[PubMed: 23271922]
Martell BA, O'Connor PG, Kerns RD et al.: Systematic review: opioid treatment for chronic back pain:prevalence, e�icacy, and association with addiction. Ann Intern Med 146: 116, 2007.
[PubMed: 17227935]
Roelofs PD, Deyo RA, Koes BW, Scholten RJ, van Tulder MW: Nonsteroidal anti-inflammatory drugs forlow back pain: an updated Cochrane review. Spine 33: 1766, 2008.
[PubMed: 18580547]
Friedman BW, Holden L, Esses D et al.: Parenteral corticosteroids for emergency department patientswith non-radicular low back pain. J Emerg Med 31: 365, 2006.
[PubMed: 17046475]

6/11/2019
25/26
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
Rubinstein SM, Terwee CB, Assendel� WJ, de Boer MR, van Tulder MW: Spinal manipulative therapy foracute low back pain: an update of the cochrane review. Spine 38: E158, 2013.
[PubMed: 23169072]
Chaparro LE, Furlan AD, Deshpande A, Mailis-Gagnon A, Atlas S, Turk DC: Opioids compared to placeboor other treatments for chronic low back pain: an update of the Cochrane Review. Spine 39: 556, 2014.
[PubMed: 24480962]
Pinto RZ, Maher CG, Ferreira ML et al.: Drugs for relief of pain in patients with sciatica: systematic reviewand meta-analysis. BMJ 344: e497, 2012.
[PubMed: 22331277]
Jacobs WC, van Tulder M, Arts M et al.: Surgery versus conservative management of sciatica due to alumbar herniated disc: a systematic review. Eur Spine J 20: 513, 2011.
[PubMed: 20949289]
Hahne AJ, Ford JJ, McMeeken JM: Conservative management of lumbar disc herniation with associatedradiculopathy: a systematic review. Spine 35: E488, 2010.
[PubMed: 20421859]
Markman JD, Gaud KG: Lumbar spinal stenosis in older adults: current understanding and futuredirections. Clin Geriat Med 24: 369, 2008.
[PubMed: 18387461]
Domen PM, Hofman PA, van Santbrink H, Weber WE: Predictive value of clinical characteristics inpatients with suspected cauda equina syndrome. Eur J Neurol 16: 416, 2009.
[PubMed: 19490073]
Cole JS, Patchell RA: Metastatic epidural spinal cord compression. Lancet Neurol 7: 459, 2008. [PubMed: 18420159]
Penas-Prado M, Loghin ME: Spinal cord compression in cancer patients: review of diagnosis andtreatment. Curr Oncol Rep 10: 78, 2008.
[PubMed: 18366964]
Loblaw DA, Mitera G, Ford M, Laperriere NJ: A 2011 updated systematic review and clinical practiceguideline for the management of malignant extradural spinal cord compression. Int J Radiat Oncol Biol Phys84: 312, 2012.
[PubMed: 22420969]

6/11/2019
26/26
39.
40.
Beh SC, Greenberg BM, Frohman T, Frohman EM: Transverse myelitis. Neurol Clin 31: 79, 2013. [PubMed: 23186897]
Murillo O, Roset A, Sobrino B et al.: Streptococcal vertebral osteomyelitis: multiple faces of the samedisease. Clin Micro Infect 20: 33, 2014.
[PubMed: 23889700]
McGraw HillCopyright © McGraw-Hill Education
All rights reserved. Your IP address is 75.148.241.33
Terms of Use • Privacy Policy • Notice • Accessibility
Access Provided by: Brookdale University Medical CenterSilverchair