Embed Size (px)
Citation preview

7 Med Genet 1993; 30: 752-755
Epidermal mosaicism and Blaschko's lines
Celia Moss, S Larkins, M Stacey, A Blight, P A Farndon, E V Davison
AbstractTo test the hypothesis that epidermalrather than dermal mosaicism deter-mines Blaschko's lines in hypomelanosisof Ito (HI), we studied the distributionof chromosomal mosaicism in fourpatients. In two, mosaicism had notbeen detected in lymphocytes or dermalfibroblasts, but was clearly shown in epi-dermal keratinocytes; furthermore, theabnormal cell line was confined to the
Department of hypopigmented epidermis and the nor-Dermatology, mal epidermis contained only normal
Children's Hospital, cells. Negative findings in the other twoLadywood Middleway, patients might be because of mosaicismLadywood, which was undetected either because itBirmingham B16 8ET,
was submicroscopic or because it wasUK.C Moss present in melanocytes, which have not
yet been studied. These preliminary re-UenitnalCiytgenetics sults support the ideas that (1) Blaschko'sMaternity Hospital, lines represent single clones of epidermalEdgbaston, cells; (2) in patients with HI and severeBirmingham B152TGK neurological involvement mosaicism, ifS Larkins detectable, is best shown in keratino-M Stacey cytes; and (3) the cytogenetic defect inE V Davison epidermal cells may be directly respon-
Skin Culture sible for the failure of pigmentation inLaboratory, HI.Birmingham Accident (J7 Med Genet 1993;30:752-5)Hospital, Bath Row,Birmingham B15 1NA,UK. Birthmarks arising from the superficial layer ofA Blight the skin, epidermal naevi, form striking linear
West Midlands and whorled patterns. Blaschko, a 19th cen-Regional Genetic tury dermatologist, was struck not only by theServices, Birmingham strangeness of the patterns, but also by theirMaternity Hospital, constancy from one person to the next. HeEdgbaston,Birmingham B15 2TG, documented the lesions in over 100 patients,UK. transferred them to a plaster of Paris classicalP A Farndon statue, and thereby constructed the systemCorrespondence to known as Blaschko's lines.'2Dr Moss. We now recognise Blaschko's lines in manyReceived 22 April 1993. different dermatoses, but the cause of thisRevised version accepted3 June 1993. pattern remains speculative. Its constancy in
Table 1 Linear dermatoses explained on the basis of mosaicism.
Skin condition Characteristics of abnormal Cause of mosaicismclone of epidermal cells
Incontinentia pigmenti Lethal X linked dominant gene LyonisationGoltz syndromeChondrodysplasia punctata
Epidermal naevus Lethal autosomal dominant gene Half chromatid orLinear porokeratosis somatic mutationCHILD syndromeILVENProteus syndromeMcCune-Albright syndromeEpidermolytic hyperkeratosis Non-lethal autosomal dominant Half chromatid orLinear Darier's disease gene somatic mutationSegmental neurofibromatosisLinear psoriasisLinear lichen planusLinear eczema (lichen striatus)Linear dyspigmentation Chromosomal abnormality Somatic
non-disjunction
Linear dyspigmentation Normal Chimerism
different disorders suggests that it is a functionof normal skin biology rather than a pathologi-cal process. Montgomery,' in 1901, dismissedvarious anatomical candidates: Blaschko'slines do not correspond to vascular or lympha-tic territories, to dermatomes, to Voigt's lineswhich demarcate areas supplied by the majorcutaneous nerve branches, to Langer's lines ofskin tension, or to embryological body seg-ments. Montgomery concluded that they ref-lected the streams or trends of growth ofembryonic tissues. This view is still held,unproven but supported by animal studies ofmelanocyte and keratinocyte migration.45 Thisexplanation of the orientation of the lines doesnot, however, explain the patchy nature of thedifferent dermatoses following this pattern. In1965, Curth and Warburton6 suggested thatthe pigmentation following Blaschko's linesseen in the X linked disorder incontinentiapigmenti reflected functional X chromosomemosaicism (Lyonisation), the normal skincomprising cells in which the normal, paternalX chromosome is active, and the affected skincontaining cells in which the abnormal, mater-nal X chromosome is active. In 1978, Shuster7expressed the more general idea that thewhorled appearance of many naevi is "bestrelated to the developmental movement of aclone of cells" and that "susceptibility even toa common disease such as eczema may be focalwith a bizarre linear and whorled appearancein a 'clonal' pattern". Happle"'0 has developedthe hypothesis that disorders followingBlaschko's lines reflect genetic mosaicism as aresult of Lyonisation or somatic mutation.This idea has been supported by the finding ofchromosomal mosaicism in patients with lineardyspigmentation following Blaschko's lines, acondition known as hypomelanosis of Ito (HI)when associated with neurological deficit."-5All dermatoses in Blaschko's lines can now beexplained on the basis of mosaicism (table 1).This clonal hypothesis of Blaschko's lines
seems so likely to be true that little time hasbeen wasted in trying to prove it. Remarkably,however, experiments in mosaic subjects havetotally failed to show what it predicts, namelythat one skin type is composed of one cell type,and the other skin type of the other cell type.The hypothesis was first tested in three her-maphrodites, human chimeras with a mixtureof 46,XX and 46,XY cells, who had patchypigmentation with midline demarcation. Cyto-genetic studies on fibroblasts cultured fromlight and dark areas showed a mixture of bothcell types in one or both sites.'6 It was nexttested in incontinentia pigmenti: X inactiva-tion studies on fibroblasts cultured from lightand dark skin showed that the same X chromo-some was active in both sites, rather than thenormal paternal X in the normal skin and the
752
on February 22, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.752 on 1 Septem
ber 1993. Dow
nloaded from

Epidermal mosaicism and Blaschko's lines
abnormal maternal X in the pigmented skin ashad been expected. This result was attributed tothe proliferative advantage of cells containingthe normal X."7 Most recently it has beentested in patients with chromosomal mosai-cism and linear dyspigmentation. There arenow many reports of cytogenetic studies onfibroblasts cultured from light and dark skin,but hardly any show pure cultures of the twodifferent cell lines in the two different biopsies:there is almost always a mixture in one or bothbiopsies.11-15The most likely explanation for this is that
fibroblasts do not conform to Blaschko's lines.Most of the dermatoses following Blaschko'slines (table 1) affect ectodermal derivatives,namely melanocytes, keratinocytes, or epider-mal appendages. Similarly all the chimericanimal studies involve epidermal cells.4 5Therefore, we performed cytogenetic studieson cultured epidermal cells from light and darkareas of four patients with linear dyspigmen-tation, three of whom had severe neurologicaldeficit (HI). We chose to examine ker-atinocytes rather than melanocytes simplybecause they are easier to grow.
MethodsCELL CULTURE AND CHROMOSOME ANALYSISMetaphase chromosome preparations weremade from peripheral blood lymphocytes andcultured skin fibroblasts using standardmethods.For the preparation of keratinocytes for
chromosome analysis the skin biopsies werewashed in calcium and magnesium free PBSand then floated in 2 ml 0 1% trypsin solutionfor one hour at 37°C with agitation at 10minute intervals, to separate the epidermis.The epidermis was then peeled back and thekeratinocytes gently scraped from the keratinlayer, and from the epidermal side of thebasement membrane. The loose cells werecollected by washing the tissue with mediumand centrifuging the resultant cell suspension.The cell yield was placed in a 60mm petri
dish containing 5 x 105 feeder cells (Swiss3T3.J2 irradiated mouse fibroblasts) and Kmedium18 without epidermal growth factor(EGF). Mouse EGF (1Ong/ml) was added atthe first medium change (three to four days)and at all subsequent changes. Cultures wereincubated at 37°C in 10% CO2 in air.Primary cultures were subcultured after
eight days' growth. The feeder layers wereselectively removed by vigorous pipetting with0-01% EDTA before disaggregating the ker-atinocytes with 1 part trypsin:1 part EDTA.Secondary cultures were established at 105cells per 25 cm2 growth area flasks preparedas for primary culture. Before harvestingfor cytogenetics the feeder cells were againremoved and metaphases prepared usingstandard methods.
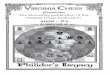
PATIENTSCase 1, an Asian female aged 3 years, had facialasymmetry, developmental delay, bilateral
sensorineural deafness, and hypopigmentedstreaks and whorls (fig 1). Previous cytogeneticstudies in lymphocytes and in fibroblasts cul-tured from light and dark skin on the arm hadbeen reported as normal with no mosaicism:a single fibroblast out of a total of 70 grownfrom dark skin showed the karyotype46,XX, - 13, + mar, but this was dismissed as acultural artefact. Further 2 mm biopsies weretaken from light and dark areas on the back forboth fibroblast and keratinocyte culture.
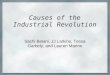
Case 2, an Asian female aged 1 year, wasdevelopmentally delayed, epileptic, andseverely visually impaired, with minimal whitestreaks on the right flank, hip, and leg (fig 2).Previous cytogenetic studies on lymphocyteswere normal. Fibroblasts from a biopsy oflight skin had failed to grow and from darkskin showed a normal karyotype. Furtherbiopsies were taken from light and dark skin onthe flanks for keratinocyte culture.
Case 3, a white male aged 13, had epilepsy,moderate learning difficulties with language, awebbed neck, bilateral talipes, and generalisedlight and dark streaks. Cytogenetic studies inlymphocytes and fibroblasts from light skin onthe arm showed a normal 46,XY karyotype,while fibroblasts from adjacent dark skinshowed a mixture of 46,XY and 45,X, 4-8%cells being abnormal. Further biopsies weretaken from light and dark skin on the back forkeratinocyte culture.
Case 4, a white male aged 13 years, wasprofoundly retarded and epileptic, with linearhypopigmented streaks. Lymphocytes had thekaryotype 46,XY with no mosaicism. Biopsieswere taken from light and dark skin on the armfor fibroblast and keratinocyte culture.These fibroblast karyotypes are summarised
in table 2.
Figure 1 Hypopigmented streaks on the anterior trunkof case 1.
753
on February 22, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.752 on 1 Septem
ber 1993. Dow
nloaded from

Moss, Larkins, Stacey, Blight, Farndon, Davison
Figure 2 Hypopigmented streaks and whorl on the right hip and flank of case 2.
Table 2 Fibroblast karyotypes.
Patient Dark skin Light skin
Cells Karyotype Cells Karyotype
No % No %
Case 1 1 1 4 46,XX,- 13,+ mar No growth(1st culture) 70 98.6 46,XX
Case 1 35 100 46,XX 2 13 3 46,XX,- 13,+mar(2nd culture)* 13 86 7 46,XX
Case 2 102 100 46,XX No growth
Case 3 119 95-2 46,XY 62 100 46,XY6 48 45,X
Case 4 26 100 46,XY 44 100 46,XY
* Skin fibroblasts were cultured from case 1 on two occasions: the first time only fibroblasts weregrown and the second time both fibroblasts and keratinocytes were grown.
Table 3 Keratinocyte karyotypes.
Patient Dark skin Light skin
Cells Karyotype Cells Karyotype
No % No %
Case 1 15 100 46,XX 4 100 46,XX,- 13,+marCase 2 15 100 46,XX 1 4 46,XX
24 96 47,XX, + 7
Case 3 100 100 46,XY 60 100 46,XYCase 4 31 100 46,XY 31 100 46,XY
ResultsCytogenetic studies on keratinocytes showedthe following. Case 1. All 15 cells examinedfrom dark skin showed a normal 46,XX karyo-type, while all four cells from light skin showedthe abnormal karyotype 46,XX, - 13, + mar,the small marker chromosome probably beinga ring 13. Fibroblasts grown from the same
skin biopsies gave the following: all 35 cellsfrom dark skin were normal, while two out of15 cells from light skin showed the abnormal-ity 46,XX,- 13,+ mar. Case 2. All 15 cellsfrom dark skin were normal (46,XX) while 24out of 25 cells from light skin showed trisomy
7, one cell being normal. Case 3. All cells fromboth dark (100 cells) and light (60 cells) skinshowed a normal 46,XY karyotype. Case 4. Allcells from both dark and light skin showed anormal 46,XY karyotype.These results are summarised in table 3.
DiscussionOur results show the following. (1) In chromo-somally mosaic patients, keratinocytes cul-tured from light or dark skin demarcated byBlaschko's lines are more likely to yield asingle cell type than are fibroblasts. Three ofthe eight successful fibroblast cultures yieldeda mixture of cells, the abnormal cell line com-prising 1 4 to 13 3% of cells examined. Onlyone of eight keratinocyte cultures yielded amixture of cells, and in that culture only asingle cell was 'out of place', having a normalkaryotype when the other 24 cells had an extrachromosome 7. This could well be because ofrandom loss in broken metaphase. These find-ings support the idea that Blaschko's linesdemarcate epidermal rather than dermalclones. This idea is also supported by findingsin the single patient where we looked at ker-atinocytes and fibroblasts from the same bi-opsy: the second skin biopsy from light skin incase 1 showed a mixture of cells in the dermis,but a pure culture in the overlying epidermis.
(2) In patients with dyspigmentation follow-ing Blaschko's lines, where chromosomalmosaicism is suspected but not definitelyshown in fibroblasts, it may be confirmed inkeratinocytes (cases 1 and 2). Clearly this ob-servation will be useful clinically. The patho-genetic significance of this finding is not yetclear: our patients do not resemble previouspatients with ring 13,'9 13q-,22' or trisomy 7,22and this might be because of a low level ofmosaicism or tissue specificity.The finding of mosaicism in keratinocytes
supports the idea that Blaschko's lines aredetermined by the epidermis, but the negativefindings in two patients require explanation.In case 4 no mosaicism was found in anytissue, but this patient's phenotype is so typi-cal of HI that it seems very likely that he ismosaic. It has been suggested that all patientswith HI are mosaic but the mosaicism may besubmicroscopic,23 and this would certainlyexplain our negative findings in this patient.The result from case 3 was unexpected: ker-atinocytes from both light and dark skinshowed a normal male karyotype, while fibro-blasts from dark skin were mosaic 46,XY/45,X. The abnormal cells cannot be dismissedas artefactual because phenotypically thepatient showed some features of Turner's syn-drome, with a webbed neck and low posteriorhairline. This finding can, however, be recon-ciled with the hypothesis that Blaschko's linesare determined by the epidermis, since kerati-nocytes are not the only cells in the epidermis:melanocytes are also present, and areobviously relevant in these patients becausethe phenomenon we are studying is pigmen-tation. In this patient, epidermal mosaicismmight be confined to melanocytes, but this has
754
..... ....
1'..
mob-'"I"It--ile,
on February 22, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.752 on 1 Septem
ber 1993. Dow
nloaded from

Epidermal mosaicism and Blaschko's lines
not yet been tested. Interestingly, case 3 wasthe most mildly affected neurologically of thepatients we studied. Embryologically, kerati-nocytes and the central nervous system havethe same ectodermal origin, while melanocytesderive later from the neural crest. We suggestthat in this patient the abnormal cell linedeveloped in the mesoderm and neural crest,largely sparing the keratinocytes and brain.We plan to test this hypothesis in future byexamining cultured melanocytes for mosai-cism.
(3) We predicted that in subjects with epi-dermal mosaicism, one skin type would showone cell line and the other skin type wouldshow the other cell line. Our results haveindeed shown this in case 1 and also in case 2with the exception of only one cell.
(4) In both patients showing epidermalmosaicism, the abnormal (pale) skin containedthe abnormal cell line. This revives the possi-bility that the cytogenetic abnormality isdirectly responsible for the failure of pigmen-tation. Previous studies in fibroblasts haveshown abnormal cells in both light and darkskin: this observation, and the fact that somany different cytogenetic abnormalities pro-duce the same appearance, has led to the ideathat the pigmentary anomaly is a non-specificresult of genetically different cells migratingtogether.23 However, this does not explain thefact that most chromosomally mosaic patientsdo not have linear dyspigmentation. Further-more, the control of pigment production, stor-age, and distribution is controlled by manygenes,24 and could probably be disturbed bymany different chromosomal rearrangementsin keratinocytes or melanocytes.
In conclusion, our limited findings supportthe idea that Blaschko's lines are determinedby epidermal rather than fibroblast clones. Wesuggest that looking for chromosomal mosai-cism is a more sensitive test for HI whencarried out in keratinocytes rather than infibroblasts alone, and in future melanocytesshould also be studied. The presence of mosai-cism in fibroblasts but not keratinocytes mightbe associated with a better prognosis neuro-logically. Finally, the cytogenetic abnormality
in the epidermis might be directly responsiblefor the failure of pigmentation in the palestreaks of hypomelanosis of Ito.
1 Blaschko A. Die Nevenverteilung in der Haut in ihrerBeziehung zu den Ekrankungen der Haut. Beilage zu denVerhandlungen der Deutschen Dermatologischen Gesell-schaft VII Congress, Breslau 1901. Table 16. Wien, Leip-zig: Braumuller, 1901.
2 Happle R. An early drawing of Blaschko's lines. BrJDermatol 1993;128:464.
3 Montgomery DW. The cause of the streaks in naevuslinearis. J Cutaneous Genitourinary Dis 1901;19:455-64.
4 Mintz B. Gene control of mammalian pigmentary differen-tiation. I. Clonal origin of melanocytes. Proc Natl AcadSci USA 1967;58:344-51.
5 Schmidt GH, Blount MA, Ponder BAJ. Immunochemicaldemonstration of the clonal organisation of chimaericmouse epidermis. Development 1987;100:534-41.
6 Curth HO, Warburton D. The genetics of incontinentiapigmenti. Arch Dermatol 1965;92:229-35.
7 Shuster S. Dermatology in internal medicine. Oxford: OxfordMedical Publications, 1978:21.
8 Happle R. Genetische Interpretation streifenformiger Hau-tanomalien. Hautarzt 1978;29:357-63.
9 Happle R. Lyonization and the lines of Blaschko. HumGenet 1985;70:200-6.
10 Happle R. Cutaneous manifestation of lethal genes. HumGenet 1986;72:280.
11 Flannery DB, Byrd JR, Freeman WE, Perlman SA. Hypo-melanosis of Ito: a cutaneous marker of chromosomalmosaicism. Am J Hum Genet 1985;37:A93.
12 Donnai D, Read AP, McKeown C, Andrews T. Hypomela-nosis of Ito: a manifestation of mosaicism or chimerism. JMed Genet 1988;25:809-18.
13 Thomas IT, Frias JL, Cantu ES, et al. Association ofpigmentary anomalies with chromosomal and geneticmosaicism and chimaerism. Am J Hum Genet1989;45: 193-205.
14 Flannery DB. Pigrnentary dysplasias, hypomelanosis of Itoand genetic mosaicism. Am J Med Genet 1990;35:18-21.
15 Ohashi H, Tsukahara M, Murano I, et al. Pigmentarydysplasias and chromosomal mosaicism: report of ninecases. AmJ Med Genet 1992;43:716-21.
16 Findlay GH, Moores PP. Pigment anomalies of the skin inhuman chimaera: their relation to systematised naevi. BrJ Dermatol 1980;103:489-98.
17 Migeon B, Axelman J, de Beur SJ, et al. Selection againstlethal alleles in females heterozygous for incontinentiapigmenti. Am J Hum Genet 1989;44:100-6.
18 O'Connor NE, Gallico GG, Compton C, et al. Grafting ofburns with cultured epithelium prepared from autologousepidermal cells. II. Intermediate term results on threepaediatric patients. In: Hunt TK, Heppenstall KB, PinesE, Rovee D, eds. Soft and hard tissue repair. Vol 2.Chapter 14. New York: Praeger, 1984:283-92.
19 Martin NJ, Harvey PH, Pearn JH. The ring chromosome13 syndrome. Hum Genet 1982;61:18-23.
20 Tranebjaerg L, Nielsen KB, Tommerup N, et al. Intersti-tial deletion 13q: further delineation of the syndrome byclinical and high-resolution chromosome analysis of fivepatients. Am J Med Genet 1988;29:739-53.
21 Brandt CA, Hertz JM, Petersen MB, et al. Ring chromo-some 13: lack of distinct syndromes based on differentbreakpoints on 13q. J7 Med Genet 1992;29:704-8.
22 Pflueger SMV, Scott CI, Moore CM. Trisomy 7 and Pottersyndrome. Clin Genet 1984;25:543-8.
23 Read AP, Donnai D. Association of pigmentary anomalieswith chromosomal and genetic mosaicism and chimaer-ism. AmJ Hum Genet 1990;47:166-7.
24 Hearing VJ. Unraveling the melanocyte. Am J Hum Genet1993;52: 1-7.
755
on February 22, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.752 on 1 Septem
ber 1993. Dow
nloaded from