Embed Size (px)
Citation preview

Meriem Bensalem-Owen, MD
University of Kentucky
EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG
MONITORING

DISCLOSURES
Received grants for sponsored research as investigator from:
• UCB
• Eisai
• Upsher-Smith Laboratories
Speaker bureau:
• Sunovion
OBJECTIVES
• To review the principles of video-EEG monitoring in the pre-surgical evaluation of drug resistant epilepsy patients.
• To outline the limitations of non-invasive video-EEG monitoring.
• To discuss the importance of safety during monitoring.
INTRODUCTION
• VEM is the most indispensable initial step in the evaluation and identification of the epileptogenic zone in order to determine candidacy for surgical treatment.
• The epileptogenic zone being defined as the area generating seizures, and whose removal/disconnection is necessary for seizure freedom.
Lüders HO. Epilepsy Surgery 3rd Ed. 2009
HISTORICAL PERSPECTIVE
• In 1935, about a year after Berger’s findings on interictal EEG activity, Penfield recognized the great potential of the EEG to define better the epileptogenic zone.
• In the 1970s, Dreifus, Penry and Porter aided in the development of the video-EEG system.
Penry JK, Porter RJ, Dreifuss FE. Simultaneous recording of absence seizures with video tape and electroencephalography. A study of 374 seizures in 48 patients. Brain 1974;98(3):427-440.

BASIC PRINCIPLES OF VEM
• Valuable tool for the diagnosis, localization and lateralization of seizures.
• In the surgical evaluation, it helps correlate ictal EEG with seizure semiology.
• Activation techniques:
1.AED withdrawal
2.Sleep deprivation
• Special strategies: additional electrodes and tailored seizure examination.
• Creation of an environment where seizures can be safely captured.

CHALLENGES & LIMITATIONS OF VEM
• The EEG can only support a diagnosis of epilepsy that is clinically based.
• Temporal relationship between the clinical and EEG findings may vary.
• Time constraint (cost, patient comfort...)
• How many seizures are necessary for localization of the epileptogenic zone?
• Co-existent epileptic and non-epileptic events in pre-surgical candidates.
• Effects of anticonvulsant withdrawal on seizure semiology and EEG.
• Safety issues.

TEMPORAL RELATIONSHIP BETWEEN CLINICAL & EEG FINDINGS
• In temporal lobe seizures the clinical onset almost always precedes the EEG, often by several seconds.
• Auras will often not show up in the scalp-sphenoidal EEG.
• In approximately 30% of cases auras may be reflected by suppression of ongoing activity, changes in the heart rate, or, occasionally, some rhythmic or semi-rhythmic periodic activity on the sphenoidal and anterotemporal electrodes.
Williamson et al. Characteristics of medial temporal lobe epilepsy: II. Interictal and ictal scalp electroencephalography, neuropsychological testing, neuroimaging, surgical results, and pathology. Ann Neurol 1993;34:781-787.
Devinsky et al. Clinical and electroencephalographic features of simple partial seizures. Neurology 1988; 38:1347-1352.

AURAS: FREQUENTLY CONSIDERED AS THE BEST INDICATOR OF THE EPILPTOGENIC ZONE
• The symptomatology of the aura usually correlates with seizure onset.
• Up to 90% of patients with temporal lobe epilepsy report experiencing auras, however, auras are frequently lacking during monitoring or are not remembered.
• Seizures arising from silent cortex produce auras at a distance from the epileptogenic zone
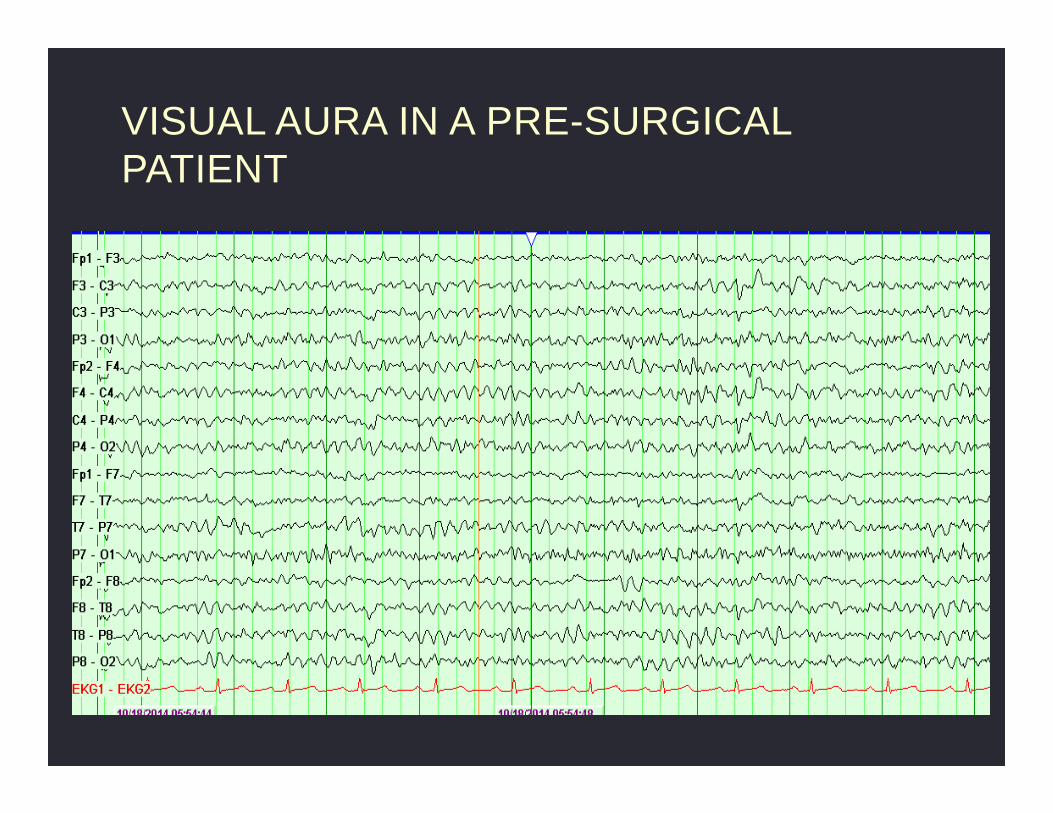
VISUAL AURA IN A PRE-SURGICAL PATIENT
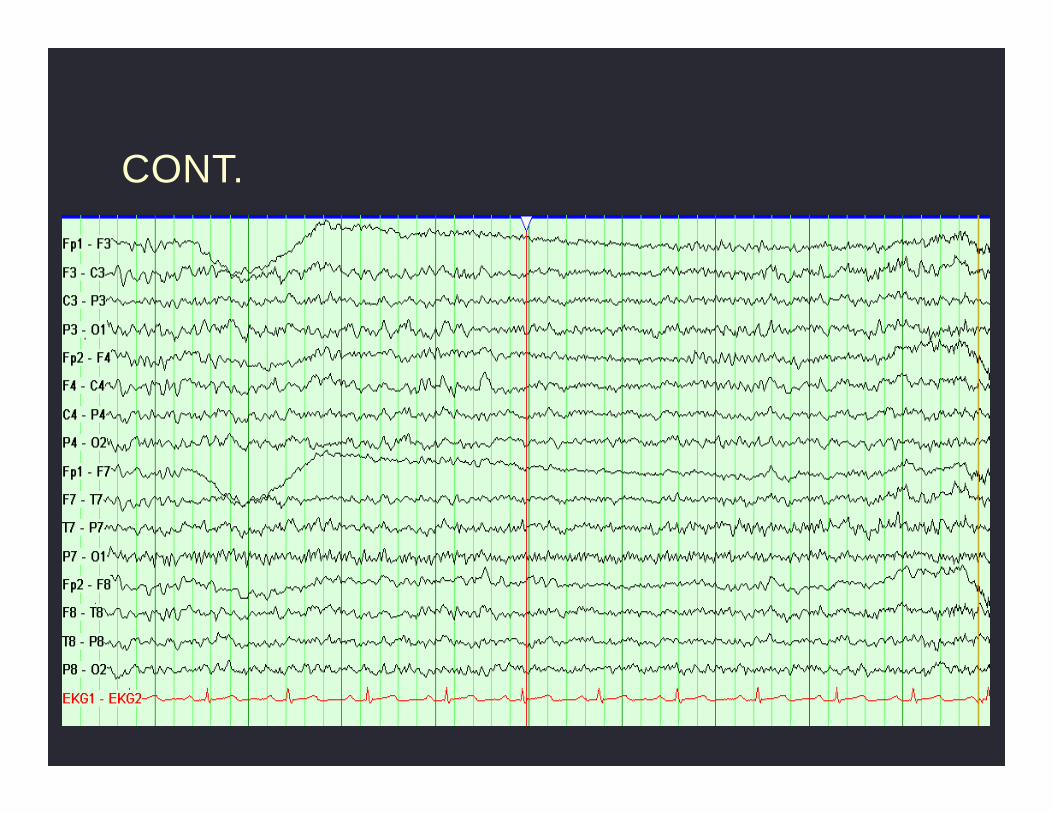
CONT.
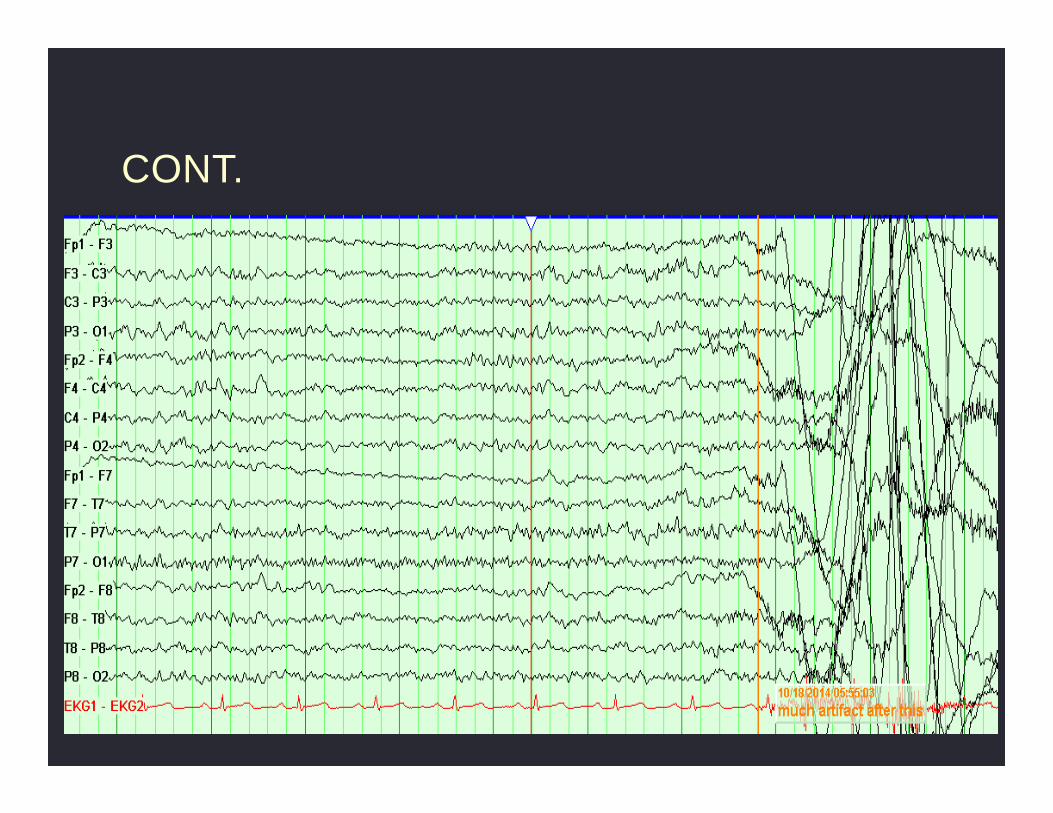
CONT.
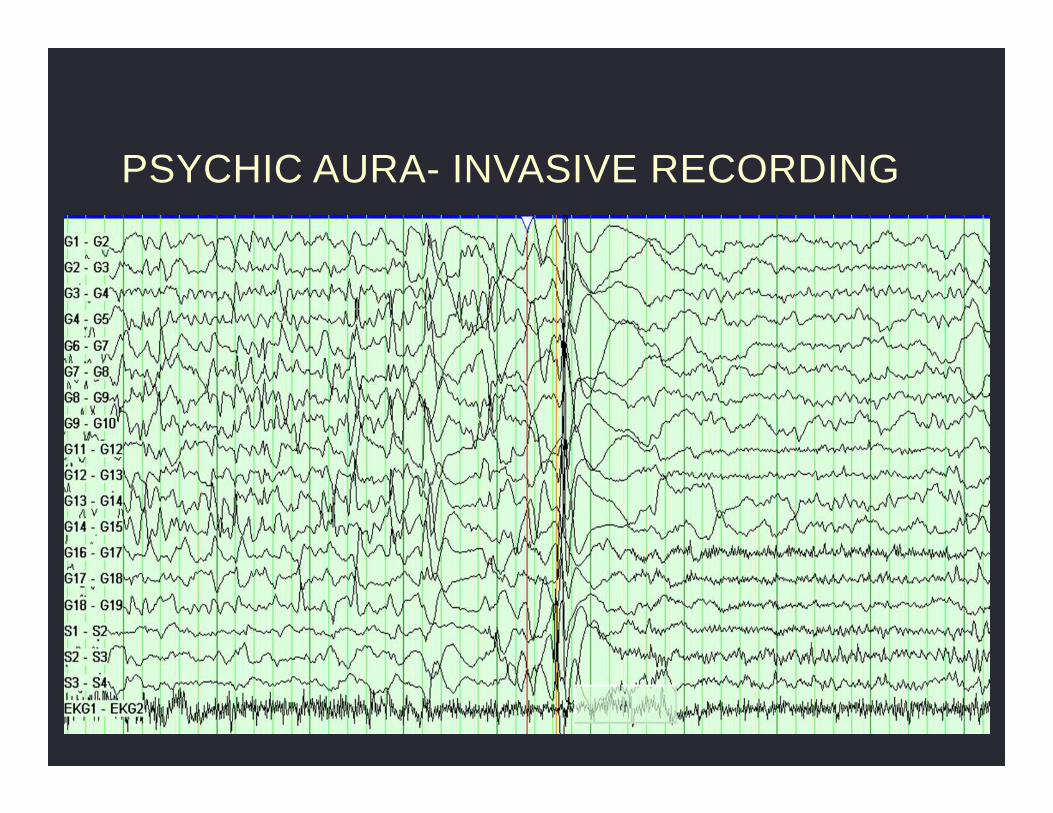
PSYCHIC AURA- INVASIVE RECORDING

CONT.

CONT.
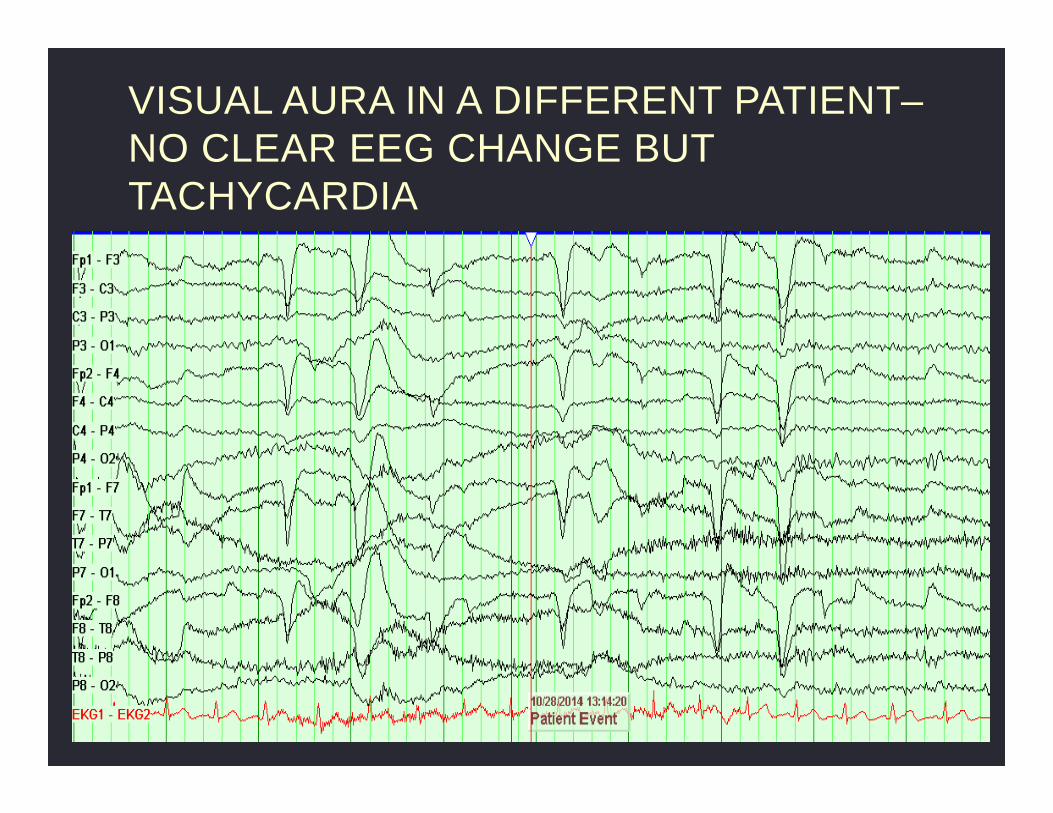
VISUAL AURA IN A DIFFERENT PATIENT–NO CLEAR EEG CHANGE BUT TACHYCARDIA

CONT.

FIRST SEIZURE RECORDED DURING PRE-SURGICAL EVALUATION ASSOCIATED WITH ASYSTOLE

CONT.

HOW MANY SEIZURES ARE NECESSARY FOR LOCALIZATION OF THE EPILEPTOGENIC ZONE? • There is no consensus.
• Mathematical models suggest the need for at least 5 concordant seizures to achieve a 95% level of confidence of unilaterally or at least 4 such seizures in patients with strictly unilateral interictal spikes.
• The first seizure, usually captured within 2 days of recording and especially when well localized, has proven to be a good predictor of the final outcome of the study.
• The total duration of noninvasive VEM and the number of seizures to be captured should depend on the individual patient history.
• Patient comfort, cost of the procedure and the use of available resources should be considered.
Blume D. Prevalence of bilateral partial seizure foci and implications for electroencephalographic telemetry monitoring and epilepsy surgery. Electroencephalogr Clin Neurophysiol 1994;91:329-336.

CO-EXISTENCE OF EPILEPTIC AND NON-EPILEPTIC SEIZURES IN A PRE-SURGICAL CANDIDATE
•Video

SAME PATIENT
•Video

ATYPICAL EVENT (DE NOVO NES) DURING THE PRE-SURGICAL EVALUATION
•Video
ANTICONVULSANT WITHDRAWAL
• Antiepileptic drugs (AEDs) are often withdrawn in order to record several seizures over a short time that a patient is typically kept in the unit (2-7 days).
• No universal standard AED withdraw protocol.
• AEDs levels?
• Knowledge of the pharmacology of AEDs can help maximize the information in the least possible time.
• Several assumptions underlie this approach:
1. Acute withdrawal reliably leads to increased seizure frequency occurring within a short time after discontinuation
2. Seizures recorded are clinically similar to a patient’s habitual seizures
3. Withdrawal is safe for the patient
CHALLENGES OF AEDS WITHDRAWAL
• The risk of increased seizures is not the same for all AEDs.
• Risk of bilateral convulsive seizures at times in patients who never had them or haven't had them for years.
• Atypical seizures can be recorded.
• Effects of AED withdrawal on EEG characteristics?
• Complications such as status epilepticus and behavioral changes, even though rare, can occur.
Spencer et al. Ictal effects of anticonvulsant medication withdrawal in epilepsy patients. Epilepsia 1981;22:297-307

FIRST SECONDARILY GTC SEIZURE EXPERIENCED DURING VEM ASSOCIATED WITH COMPRESSIVE FRACTURE
•VIDEO
SLOW VS. RAPID AED WITHDRAWAL?
• Di Gennaro et al. study in 54 patients undergoing pre-surgical VEM (total of 190 seizures recorded) :
� 11% patients had 4-h clusters
� 39% patients had 24-h clusters
� 26% sGTCS
� No status epilepticus
� 3 patients had epileptic falls with no significant injuries
� Mean time to first seizure was 3.3 days
� Time to conclude video-EEG monitoring averaged 6 days.
Di Gennaro G et al. Seizure clusters and adverse events during pre-surgical video-EEG monitoring with
a slow anti-epileptic drug (AED) taper. Clin Neurophysiol. 2012 Mar;123(3):486-468.

SLOW VS. RAPID AED WITHDRAWAL?
• The complication rate in one study including 158 patients who had rapid withdrawal of AEDs over 24hr was of 5.06%.
• Complications were characterized largely by musculoskeletal pain secondary to clinical seizures.
• No mortality observed.
• 2.5% of patients received emergency-room admission for seizure clustering in the first month following VEM.
Rizvi SA et al. Is rapid withdrawal of anti-epileptic drug therapy during video EEG monitoring safe and efficacious? Epilepsy Res. 2014 May;108(4):755-764.

LIMITATIONS OF NONINVASIVE VEM EVALUATION
• The electrical signals generated by the brain:
1. are small
2. their recording is subject to numerous distorting factors
3. they must compete for recognition with larger electrical potentials in the same environment
• Artifact (muscle and movement) can occur at the most critical points of the recording, i.e. seizure onset.
• Blume and Lemieux found scalp potentials to be 1/5 to 1/6 that recorded on the cortex.
• Both ictal and interictal recordings may yield ambiguous data when epiletogenesis arises from “occult” surfaces (mesial or inferior surfaces).
Blume WT, Lemieux JF. Morphology of spikes recorded simultaneously by subdural and scalp electrodes. In: Engel J Jr et al, eds. Fundamental mechanisms of human brain function. New York: Raven Press, 1987:171-185.
WHEN EEG, CLINICAL SEMIOLOGY AND IMAGING ARE DISCORDANT
•Video
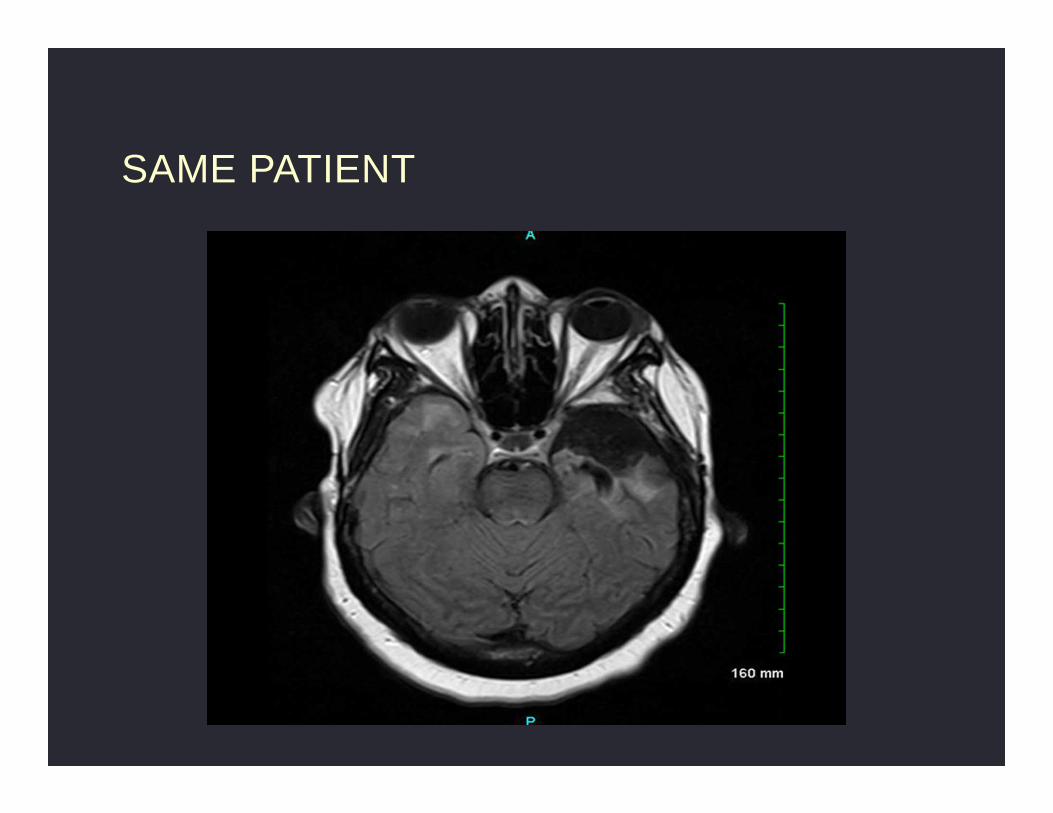
SAME PATIENT

FRONTAL LOBE SEIZURE, NON-LESIONAL MRI AND INCONCLUSIVE EEG

SAME PATIENT - SAFETY ISSUES!
•Video
SAFETY DURING VEM
• Admissions for VEM result in the induction of seizures rather than minimizing and/or treating symptoms which can lead to an increased risk to patient safety.
• Report of serious adverse events (SAEs) vary.
• SAEs affect about 10% of patients.
• SUDEP and near-SUDEP, were encountered by more than 10% of European and Australian EMUs.
• In US-based EMUs 3% of patients suffer a death within a 1-year duration census.
Rheims S, Ryvlin P. Patients' safety in the epilepsy monitoring unit: time for revising practices. Curr Opin Neurol. 2014 Apr;27(2):213-218

SAFETY DURING VEM
• In a recent study, Sauro et al. found that the number of adverse events was low at 4.9%.
• In the study Dobesberger et al. 9% of 507 consecutive patients had adverse events:
� 5% have psychiatric complications (postictal psychosis, aggression, panic attacks)
� 4% injuries (fractures, ecchymosis…)
� 3% status epilepticus
Sauro KM et al. Quality indicators in an epilepsy monitoring unit. Epilepsy Behav. 2014 Apr;33:7-11.
Dobesberger J et al. Video-EEG monitoring: safety and adverse events in 507 consecutive patients. Epilepsia. 2011; 52(3), 443-452.
SAFETY- POSTICTAL AGITATION DURING PRESURGICAL VEM
•Video

STRATEGIES TO PROMOTE SAFETY
• Staff education
• Safe environment (patient room and bathroom)
• Preadmission screening (history!)
• Development of appropriate guidelines
� Seizure provocation techniques
� Seizure precautions
� AED withdraw protocols/tailoring to patient’s history
� Seizure response protocols and rescue medications
� Postictal aggression and psychosis
� Safe discharge practices
CONCLUSIONS
• VEM is the most indispensable initial step in the evaluation and identification of the epileptogenic zone.
• There are several challenges and limitations encountered during pre-surgical scalp video-EEG evaluation.
• Maintaining a safe environment during VEM is essential to delivering the best possible care and to mitigating undesirable outcomes.








![WONOEP appraisal: Imaging biomarkers in epilepsy...recent advances in identifying the irritative zone (e.g., scalp and intracranial electroencephalography–functional MRI [EEG-fMRI])](https://img.pdfslide.net/doc/110x75/6055314f35bedc66711e5aef/wonoep-appraisal-imaging-biomarkers-in-epilepsy-recent-advances-in-identifying.jpg)