Embed Size (px)
Citation preview
Journal of Voice Vol. 10, No. 1, pp. 93-105 © t996 Lippincott-Raven Publishers, Philadelphia
Episodic Paroxysmal Laryngospasm: Voice and Pulmonary Function Assessment and Management
* G r e g o r y J. Gal l ivan , t L e e H o f f m a n , and ~tK. Ho l ly Ga l l ivan
Departments of Cardiothoracic Surgery and #Medicine, ¢Tufts University School of Medicine, Boston, and *tSwallowing and Esophageal Disorders Program, Baystate Medical Center, Springfield, Massachusetts, U.S.A.
Summary: Episodic paroxysmal laryngospasm (EPL) is a sign of laryngeal dysfunction, often without a specific organic etiology, which can masquerade as asthma, vocal fold paralysis, or a functional voice disorder. The intermittent respiratory distress of EPL may precipitate an apparent upper airway obstruc- tive emergency, resulting in unnecessary endotracheal intubation, cardiopul- monary resuscitation, or tracheostomy. During 27 months, seven women and three men, ages 30--76 years, were assessed by a high diagnostic index of suspicion, an intensive history including psychosocial factors, physical exam- ination of the airways, provocative asthma testing, and swallowing studies. Videolaryngoscopy, stroboscopy, and pulmonary flow-volume loop testing were definitive. The classic appearance was paradoxic inspiratory adduction of the anterior vocal folds with a posterior diamond-shaped glottic gap. During an attack of stridor or wheezing, attenuation of the inspiratory flow rate as de- picted by the flow-volume loop suggested partial extrathoracic upper airway obstruction. Swallowing evaluation by videolaryngoscopy and videoesoph- agography may uncover gastroesophageal reflux disease. Hallmarks of man- agement include patient and family education by observation of laryngoscopic videos, a specific speech therapy program, psychotherapy, and medical treat- ment of associated disorders. Electromyography may become a valuable future adjunct. Unlike laryngeal dystonia, patients with EPL do not benefit from botulinum toxin type A. Key Words: Episodic paroxysmal laryngospasm-- Functional voice disorders--Endotracheal intubation~Cardiopulmonary re- suscitat ion--Tracheostomy--Videolaryngoscopy--Stroboscopy--Flow vol- ume loop---Extrathoracic upper airway obstruction--Videoesophagography-- Gastroesophageal reflux disease--Electromyography--Laryngeal dystonia~ Botulinum toxin type A.
Episodic paroxysmal laryngospasm (EPL) is a sign of laryngeal dysfunction, often without specific organic etiology and not uncommon is a conver- sion phenomenon. EPL can masquerade as asthma or vocal fold paralysis. Voice disorders, particu- larly diminished voice intensity during a sudden at-
Accepted November 14, 1994. Address correspondence and reprint requests to Dr. G.J.
Gallivan at 2 Medical Center Drive, Suite 204, Spring- field, MA 01107-1271, U.S.A.
This work was presented at The Voice Foundation's 23rd An- num Symposium: Care of the Professional Voice, June 1994, Philadelphia, Pennsylvania, U.S.A.
tack of upper airway obstruction, may herald EPL. The intermittent inspiratory distress of EPL may precipitate an emergency, resulting in unnecessary endotracheal intubation, cardiopulmonary resusci- tation (CPR), or tracheostomy. EPL is recognized by a pa thognomonic v ideolaryngoscopic pat tern of paradoxical inspiratory adduct ion of the anter ior two-thirds of the vocal folds, a pos te r ior d iamond- shaped glottic chink, and a t tenuat ion of the inspira- tory flow rates of the f low-volume loop indicating partial ext ra thoracic upper a i rway obst ruct ion, dur- ing an a t tack of str idor or wheezing. I t is episodic in
93
94 G. J. GALLIVAN ET AL.
that it is an event or reversible series of events com- plete in itself but forming part of a larger, uncom- mon but disturbing clinical condition. It is paroxys- mal in that it is a sudden attack or intensification of symptoms, recurring periodically.
Once the episode of EPL has commenced during inspiration, the forceful vocal fold adduction/spasm may carry over transiently into the expiratory phase of breathing in some patients. Occult gastroesoph- ageal reflux may be diagnosed by videolaryngo- scopic visualization of erythema of the arytenoids, using frame-by-frame flexible fiberoptic videolaryn- goscopic evaluation of swallowing and by videoe- sophagography. These diagnostic tools, strobos- copy, attention to specific vocal sounds and their patterns, along with a high diagnostic index of sus- picion, an intensive history including psychosocial factors, physical examination of the airways, pro- vocative asthma testing, and exclusion of organic pathology, are useful in differentiating EPL from asthma, laryngeal edema, vocal fold paralysis, and stenosing lesions of the upper airway.
HISTORICAL BACKGROUND
Jackson and Jackson (1), in 1942, defined a "mo- tor neurosis of spasm of the larynx in adults" in which there was "spasmodic closure of the glottis, the orifice of the larynx or of both." They stated this was a "not infrequent manifestation" that may be a reflex from local irritation, e.g., by instrumen- tation, irritating gases, foreign particles or agents, secretions, "impaired esophageal drainage" or even "an elongated uvula." They also cited a cen- tral or a peripheral neurological lesion as possible etiologies and stated "it is occasionally seen as the result of hysteria. In a typical case, the patient awakens at night gasping for air. He springs from the bed and frantically grasps hold of any object. He may hasten to a window and open it because of his air hunger.
Each inspiration is associated with a loud stridor; expiration is usually unobstructed because of the closing cellar-door mechanism--the tight closure of the glottic chink by the inspiratory blast----on the mechanical principle of a check valve. The greater the respiratory effort the tighter the (glottic) clo- sure. The patient's only chance of getting in enough air to survive is to breathe very gently and slowly. In a few moments the spasm relaxes and the patient is able to breathe more freely, though he may have a brassy cough and a somewhat hoarse voice. In
some cases the attacks occur during the daytime and a sudden seizure may cause the patient to fall in the street, the spasm (continuing) so long that the patient becomes unconscious. In other cases the relaxation will come just before unconsciousness supervenes. If opportunity is afforded for a laryn- goscopic examination during a spasm, the diagnosis is promptly and conclusively made. For the attack the best thing is a proper psychic preparation for the patient. He must be made to feel there is no danger and that the harder he tries to inspirate, the less air he will get."
EPL has been well documented in the psychiat- ric, neurological, pulmonary, and otolaryngological literature, but has suffered from a lack of consensus of nomenclature. During the past 20 years, more than a dozen names have been coined. In 1974, Patterson et al. (2) described Mtinchausen's stridor as a nonorganic laryngeal obstruction. In 1982, Downing et al. (3) used a physiological approach to diagnose factitious asthma. Christopher et al. (4) noted vocal cord dysfunction presenting as asthma in 1983. Spastic vocal cord adduction, laryngeal spasm mimicking bronchial asthma (5), stridor caused by vocal cord malfunction associated with emotional factors (6), episodic laryngeal dyskinesia (7), and terms such as variable, paradoxical, and psychogenic vocal cord dysfunction masquerading as wheezing, exercise-induced asthma, stridor, or pulmonary disorders were documented in the de- cade from 1978 to 1988 (8-13).
Rogers and Stell (13), in 1978, stated that epi- sodes of dysphonia were known to be associated with functional conditions, often initiated by mild infections. They described two patients who pre- sented with stridor caused by approximation of the vocal folds during inspiration on indirect laryn- goscopy. First, a 36-year-old neurotic, divorced woman with hoarseness, noisy breathing, and throat tightness had a childhood history of asthma and edematous vocal folds. Second, an immature, emotional 19-year-old student nurse, having diffi- culty coping with working in an operating theater, developed an upper respiratory infection, a bovine cough with noisy breathing, and bilateral vocal fold edema. A speech therapist helped her to become symptom free within 2 days. They stated that the diagnosis of paradoxical vocal fold movement mer- its consideration when stridor is found in an other- wise healthy patient and that the condition may eas- ily be misdiagnosed as bronchospasm.
Causes of functional laryngeal or upper airway
Journal of Voice, Vol. 10, No. 1, 1996
EPISODIC PAROXYSMAL LAR YNGOSPASM 95
obstruction viewed as a psychogenic or somatiza- tion disorder were reported from 1981 to 1992 (14- 18), although Aronson et al. (19) had described psy- chiatric symptoms in functional dysphonia and aphonia in 1966. Psychogenic stridor, or emotional laryngospasm, was described by Arnold in 1973 (20). In 1981, Appelblatt and Baker (14) discussed cases of hysterical aphonia with tightly adducted vocal folds during spasms, but without signs of re- spiratory tract obstruction. They stated that func- tional upper airway obstruction may be difficult to diagnose initially in the presence of severe respira- tory tract distress and that tracheostomy early in the course of the disorder seemed justified, if it were indicated on clinical grounds. Their reported cases were before the era of videolaryngoscopy.
In 1990, Ophir et al. (17) studied flow-volume loops in a 12-year-old girl and cited a 14-year-old girl and a 15-year-old boy with inspiratory paradox- ical vocal fold adduction during symptomatic peri- ods and normal vocal fold movement during asymp- tomatic periods. The sudden onset of symptoms in the absence of organic disease suggested hysterical laryngeal spasm induced by emotional stress as an unconscious somatic expression of an emotional conflict. They stated that the stridor is not factitious and that the term of Miinchausen's stridor is inap- propriate, since this appears to be a true conversion neurosis.
Nagai et al. (18) described a 15-year-old boy with functional upper airway obstruction, which he called psychogenic pharyngeal constriction, who had a flow-volume loop showing normal expiratory flows but markedly decreased inspiratory flows, in- dicating extrathoracic airway obstruction. Nagai et al. did not use videolaryngoscopy to visualize the glottis.
DIAGNOSTIC DEVELOPMENTS
Kellman and Leopold (21), in 1982, reported three cases of paradoxical vocal cord motion caus- ing stridor. One of their patients underwent trache- ostomy on two occasions before the correct diag- nosis was made. These were young female patients with recent upper respiratory infections who pho- nated weakly, could not cough, had noisy inspira- tions and stridor, or critical upper airway obstruc- tion requiring tracheostomy. They recognized that indirect laryngoscopy was pivotal, rather than di- rect laryngoscopy under general anesthesia, as the normal anatomical examination allowed for assess-
ment of vocal fold function. Although they consid- ered possible underlying brain stem abnormalities or cortical dysfunction, they postulated that the eti- ology may be functional and an awareness of the entity could prevent unnecessary tracheostomy. They noted that once medical personnel paid atten- tion to the seriousness of the problem, it was mag- nified by the patient. When the correct diagnosis of inspiratory paradoxical vocal fold motion was made, supportive therapy and psychiatric evalua- tion were effective therapy. Kellman and Leopold (21) recognized that indirect laryngoscopy may re- veal a normal larynx with normal vocal fold motion, but did not correlate this with the episodic nature of paroxysmal laryngospasm. They also mused about the potential of laryngeal electromyographic evalu- ation contributing to the clinical documentation of the disorder. They suggested endotracheal intuba- tion rather than tracheostomy, after meticulous ex- clusion of entities such as bilateral vocal fold paral- ysis, subgiottic stenoses, and tumors.
Christopher et al. (4) introduced two important technological advances by using either a flexible fi- beroptic rhinolaryngoscope, or a Hopkins-rod right- angle telescopic laryngoscope, performing laryn- goscopy during an episode of wheezing and dys- pnea and during a symptom-free period. Their findings were photographed with a 16-mm motion- picture camera running at the usual speed of 16 frames per second. Representative frames were se- lected for still reproduction with the aid of a motion- analysis projector. In addition, they introduced the concept of pulmonary function assessment. To as- sess upper airway obstruction, the maximum expi- ratory and inspiratory flow-volume loop relation- ships were determined during an episode of wheez- ing and dyspnea and during a symptom-free period. During episodes of wheezing and dyspnea, they ob- served marked limitation of maximal inspiratory flow rates in all five of their patients. The expira- tory/inspiratory ratios were uniformly >2. When their subjects were tested while asymptomatic, the flow-volume relationships and expiratory/inspi- ratory ratios were relatively normal.
Christopher et al. (4) took a careful history of the episodic nature of the symptoms and auscultation identified wheezing and stridor of variable quality, suggesting upper airway origin. They documented that during a typical episode of wheezing or stridor, each patient had almost complete adduction of the vocal folds, with a small posterior diamond-shaped glottic chink. The arytenoids maintained a lateral
Journal of Voice, Vol. 10, No. 1, 1996
96 G. J. G A L L I V A N E T AL.
position, with failure to adduct. Ventricular fold ad- duction was variable. Attempts at having the pa- tients voluntarily reproduce wheezing sounds failed to achieve the characteristic glottic cinelaryngo- scopic and still-frame motion-analysis pattern. The maximal expiratory and inspiratory flow-volume loop re la t ionships and the high exp i ra to ry / inspiratory flow ratios occurring during an episode of wheezing and dyspnea suggested the presence of a variable extrathoracic upper airway obstruction. Arterial blood gases and the alveolar-arterial oxy- gen tension gradients were normal and provocative tests for bronchial asthma were negative. They ex- panded their analysis beyond laryngological and physiological evaluations to include psychiatric and speech-pathology evaluations. Whereas psycholog- ical testing did not differentiate these patients from others with severe asthma, all five of their patients had difficulty in directly expressing anger, sadness, or fear and had various degrees of secondary gain from respiratory symptoms. They were diagnosed as having a variety of psychiatric disorders, includ- ing stress-related exacerbation of symptoms. Once the laryngeal dysfunction was identified, all their patients were evaluated by a speech/language pa- thologist.
MODERN DIAGNOSTIC TECHNIQUES
Indirect mirror laryngoscopy, flexible fiberoptic transnasal laryngoscopy and rigid telescopic laryn- goscopy, all share the problem of requiring real- time assessment of laryngeal dynamics during pa- tient examination. Motion-picture (cine) laryngos- copy with analysis of individual frames was helpful, but was expensive and cumbersome, and the diag- nosis was delayed by the time required for special film processing. In 1981, Yanagisawa et al. (22)de- scribed a simple method of videolaryngoscopy, uti- lizing a right-angle telescope and home video cam- era, which he taught the principal author in 1987. That year, Martin et al. (10) used videolaryngos- copy to show how paradoxical vocal fold closure on inspiration results in laryngeal dysfunction mas- querading as asthma. They involved an otolaryngol- ogist, pulmonologist, speech/language pathologist, and psychiatrist to achieve diagnosis and treatment and to avoid inappropriate medications and surgical procedures. In evaluating the location of respirato- ry distress, they found that many individuals pointed to the area of the larynx. Their patient pop- ulation was usually female, between ages 20 and 40
years , commonly with medical- re la ted back- grounds, and educated above the high school level. Whereas auscultation of the larynx was a poor in- dicator of vocal fold function, in severe cases of paradoxical vocal fold adduction during inspiration, stridor was heard over the larynx. Laboratory data were variable and during asymptomatic periods, lung volumes, spirometry, arterial blood gases, and chest roentgenography were usually normal. During symptomatic periods, the most helpful guide was the flow-volume loop, which showed attenuation of the inspiratory portion of the loop, and occasionally of the expiratory portion. The flow-volume loop suggested the correct diagnosis and videolaryngos- copy was the definitive study. In cases where vid- eolaryngoscopy could not be done during an acute exacerbation, Martin et al. (10) put the patient through several maneuvers, including repetitive rapid deep inspirations, panting, phonation, and stimulation with the laryngoscope below the epi- glottis to uncover the laryngeal dysfunction. During a quiescent period, the only sign suggesting the presence of vocal fold abuse was mucous stranding across the vocal folds. The classic pattern was in- spiratory adduction of the anterior two-thirds of the vocal folds with a posterior diamond-shaped glottic chink or gap.
CASE REPORTS
Case 1 A 46-year-old woman with a long-standing diag-
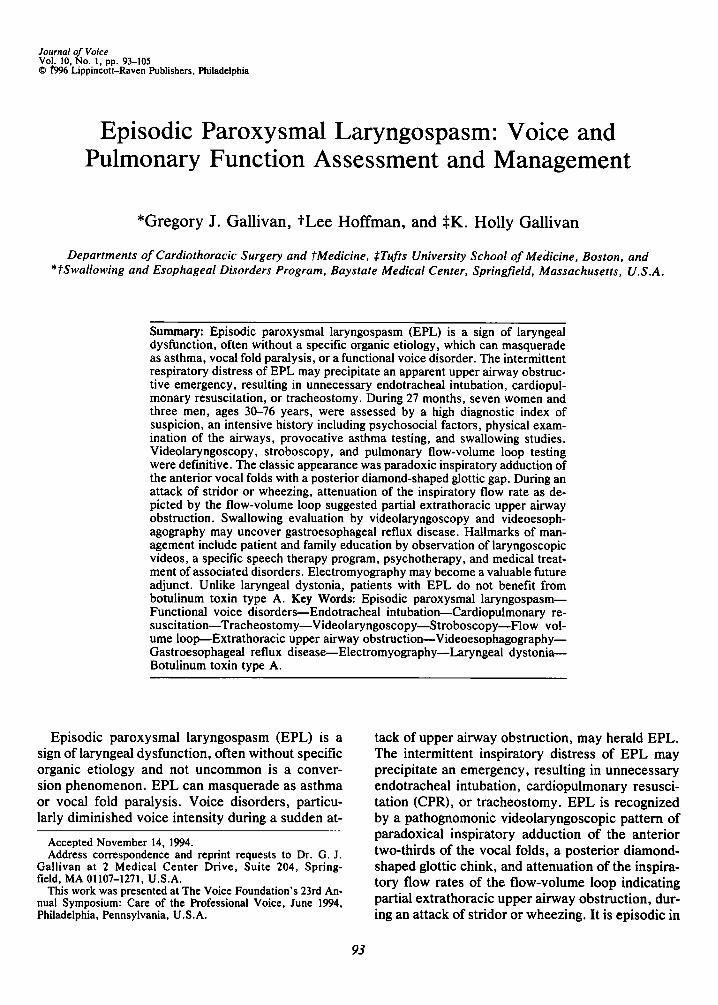
nosis of asthma treated with inhaled bronchodila- tors had many occasions of serious respiratory in- sufficiency. Two episodes of upper airway obstruc- tion resulted in her collapsing, turning blue, and being endotracheally intubated. She had some hoarseness on exposure to horses and various per- fumes. Upper airway obstructive episodes were even set off by toothbrushing. She was a school teacher described as a nervous person, and one pul- monologist felt she had psychogenic laryngospasm. Occult gastroesophageal reflux was suspected. Dur- ing videolaryngoscopy, a typical episode of EPL occurred with inspiratory crowing and stridor. In addition, a characteristic postendotracheal intuba- tion granulation tissue "key-hole" lesion, as de- scribed by Gallivan et al. was seen, (23,24), with mucous stranding posteriorly (Fig. 1). This appear- ance varies from and should not be confused with the condition of"paralysis of the interarytenoideus, and adductor muscle" nor the so-called "complete
Journal of Voice, I/ol. 10, No. 1, 1996
EPISODIC P A R O X Y S M A L LAR YNGOSPASM 97
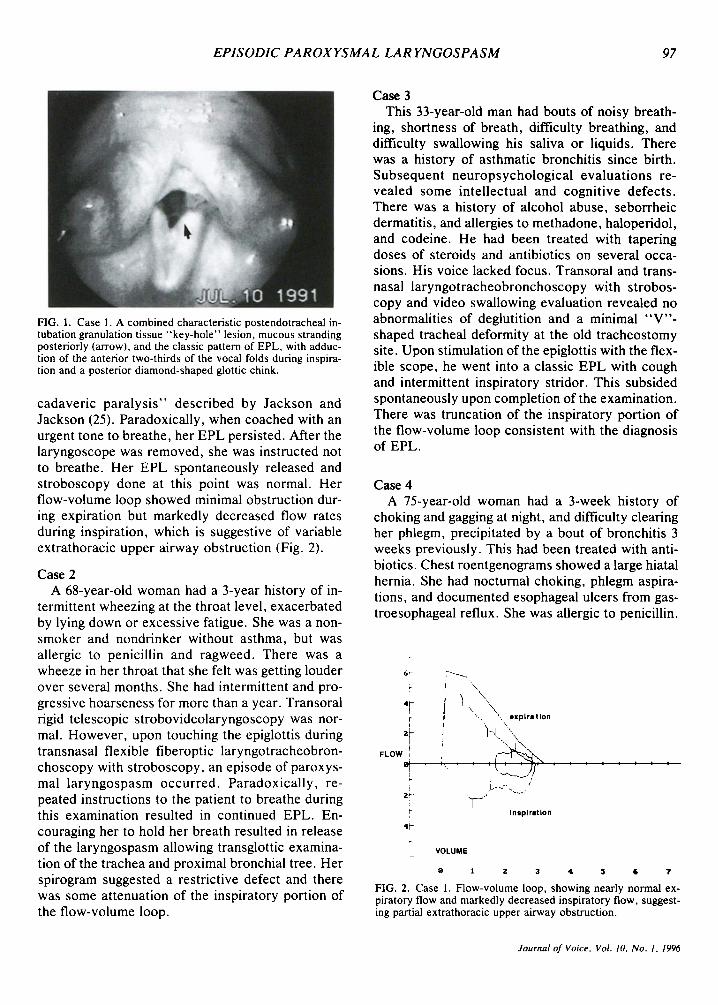
FIG. 1. Case I. A combined characteristic postendotracheal in- tubation granulation tissue "key-hole" lesion, mucous stranding posteriorly (arrow), and the classic pattern of EPL, with adduc- tion of the anterior two-thirds of the vocal folds during inspira- tion and a posterior diamond-shaped glottic chink.
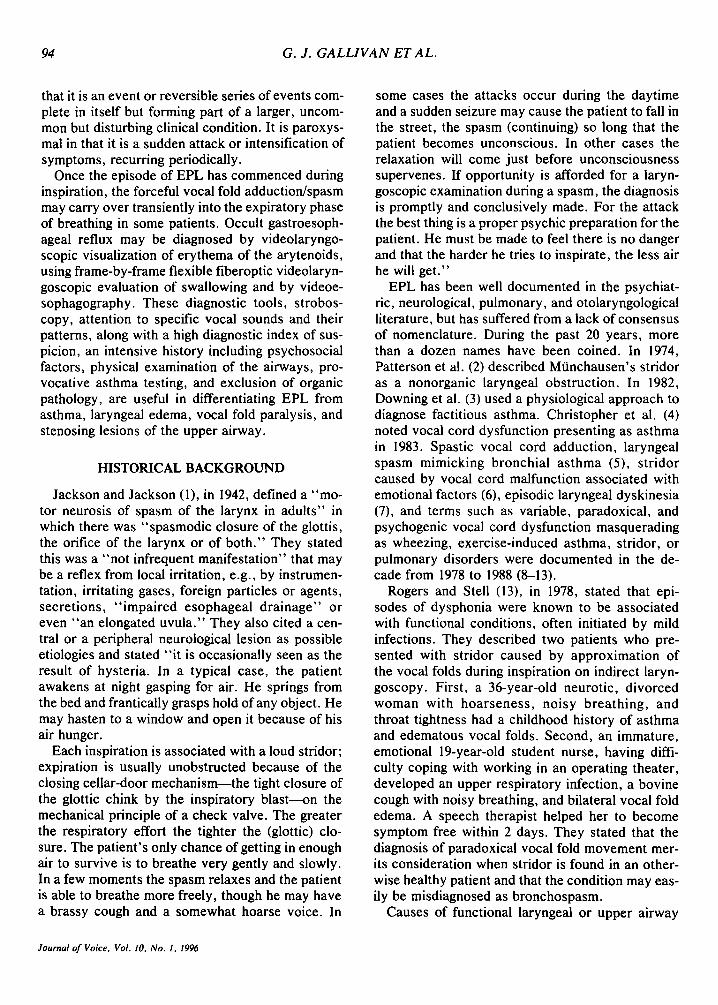
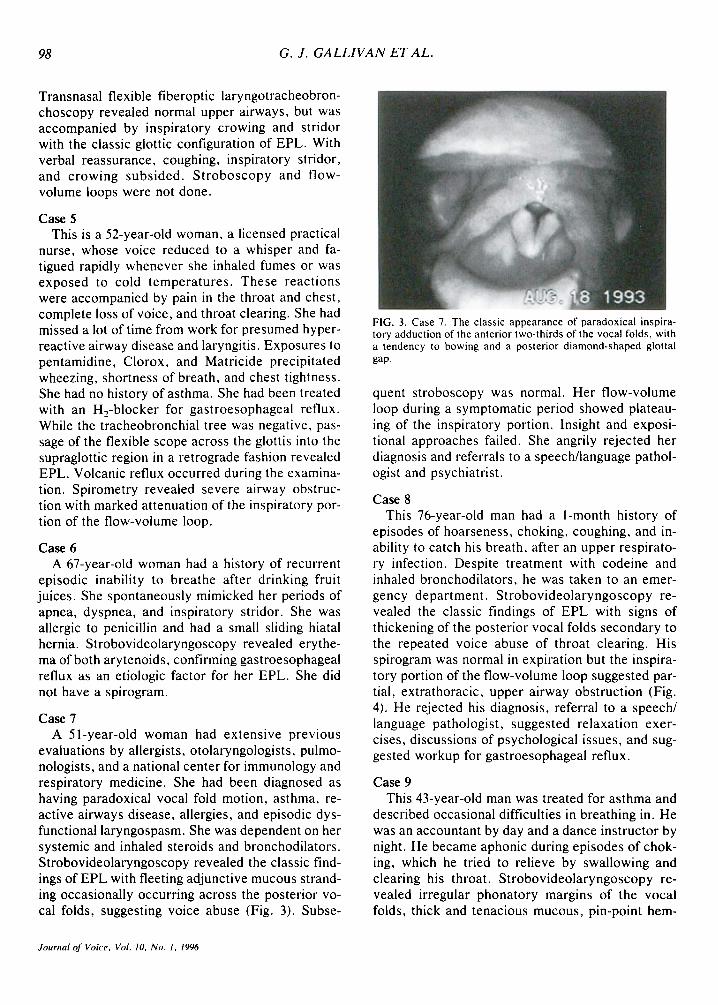
cadaveric paralysis" described by Jackson and Jackson (25). Paradoxically, when coached with an urgent tone to breathe, her EPL persisted. After the laryngoscope was removed, she was instructed not to breathe. Her EPL spontaneously released and stroboscopy done at this point was normal. Her flow-volume loop showed minimal obstruction dur- ing expiration but markedly decreased flow rates during inspiration, which is suggestive of variable extrathoracic upper airway obstruction (Fig. 2).
Case 2 A 68-year-old woman had a 3-year history of in-
termittent wheezing at the throat level, exacerbated by lying down or excessive fatigue. She was a non- smoker and nondrinker without asthma, but was allergic to penicillin and ragweed. There was a wheeze in her throat that she felt was getting louder over several months. She had intermittent and pro- gressive hoarseness for more than a year. Transoral rigid telescopic strobovideolaryngoscopy was nor- mal. However, upon touching the epiglottis during transnasal flexible fiberoptic laryngotracheobron- choscopy with stroboscopy, an episode of paroxys- mal laryngospasm occurred. Paradoxically, re- peated instructions to the patient to breathe during this examination resulted in continued EPL. En- couraging her to hold her breath resulted in release of the laryngospasm allowing transglottic examina- tion of the trachea and proximal bronchial tree. Her spirogram suggested a restrictive defect and there was some attenuation of the inspiratory portion of the flow-volume loop.
Case 3 This 33-year-old man had bouts of noisy breath-
ing, shortness of breath, difficulty breathing, and difficulty swallowing his saliva or liquids. There was a history of asthmatic bronchitis since birth. Subsequent neuropsychological evaluations re- vealed some intellectual and cognitive defects. There was a history of alcohol abuse, seborrheic dermatitis, and allergies to methadone, haloperidol, and codeine. He had been treated with tapering doses of steroids and antibiotics on several occa- sions. His voice lacked focus. Transoral and trans- nasal laryngotracheobronchoscopy with strobos- copy and video swallowing evaluation revealed no abnormalities of deglutition and a minimal "V"- shaped tracheal deformity at the old tracheostomy site. Upon stimulation of the epiglottis with the flex- ible scope, he went into a classic EPL with cough and intermittent inspiratory stridor. This subsided spontaneously upon completion of the examination. There was truncation of the inspiratory portion of the flow-volume loop consistent with the diagnosis of EPL.
Case 4 A 75-year-old woman had a 3-week history of
choking and gagging at night, and difficulty clearing her phlegm, precipitated by a bout of bronchitis 3 weeks previously. This had been treated with anti- biotics. Chest roentgenograms showed a large hiatal hernia. She had nocturnal choking, phlegm aspira- tions, and documented esophageal ulcers from gas- troesophageal reflux. She was allergic to penicillin.
6 ~
"F
2~ F L O W I
i 2 ~
4~
\ ,
"- , , , . expiration
' . ] - ~
Ineplratlon
V O L U M E
0 I 2 3 4 S • ?
FIG. 2. Case 1. Flow-volume loop, showing nearly normal ex- piratory flow and markedly decreased inspiratory flow, suggest- ing partial extrathoracic upper airway obstruction.
Journal of Voice, Vol. 10, No. 1, 1996
98 G. J. G A L L I V A N ET AL.
Transnasal flexible fiberoptic laryngotracheobron- choscopy revealed normal upper airways, but was accompanied by inspiratory crowing and stridor with the classic glottic configuration of EPL. With verbal reassurance, coughing, inspiratory stridor, and crowing subsided. S t roboscopy and flow- volume loops were not done.
Case 5 This is a 52-year-old woman, a licensed practical
nurse, whose voice reduced to a whisper and fa- tigued rapidly whenever she inhaled fumes or was exposed to cold temperatures. These reactions were accompanied by pain in the throat and chest, complete loss of voice, and throat clearing. She had missed a lot of time from work for presumed hyper- reactive airway disease and laryngitis. Exposures to pentamidine, Clorox, and Matricide precipitated wheezing, shortness of breath, and chest tightness. She had no history of asthma. She had been treated with an H2-blocker for gastroesophageal reflux. While the tracheobronchial tree was negative, pas- sage of the flexible scope across the glottis into the supraglottic region in a retrograde fashion revealed EPL. Volcanic reflux occurred during the examina- tion. Spirometry revealed severe airway obstruc- tion with marked attenuation of the inspiratory por- tion of the flow-volume loop.
Case 6 A 67-year-old woman had a history of recurrent
episodic inability to breathe after drinking fruit juices. She spontaneously mimicked her periods of apnea, dyspnea, and inspiratory stridor. She was allergic to penicillin and had a small sliding hiatal hernia. Strobovideolaryngoscopy revealed erythe- ma of both arytenoids, confirming gastroesophageal reflux as an etiologic factor for her EPL. She did not have a spirogram.
Case 7 A 51-year-old woman had extensive previous
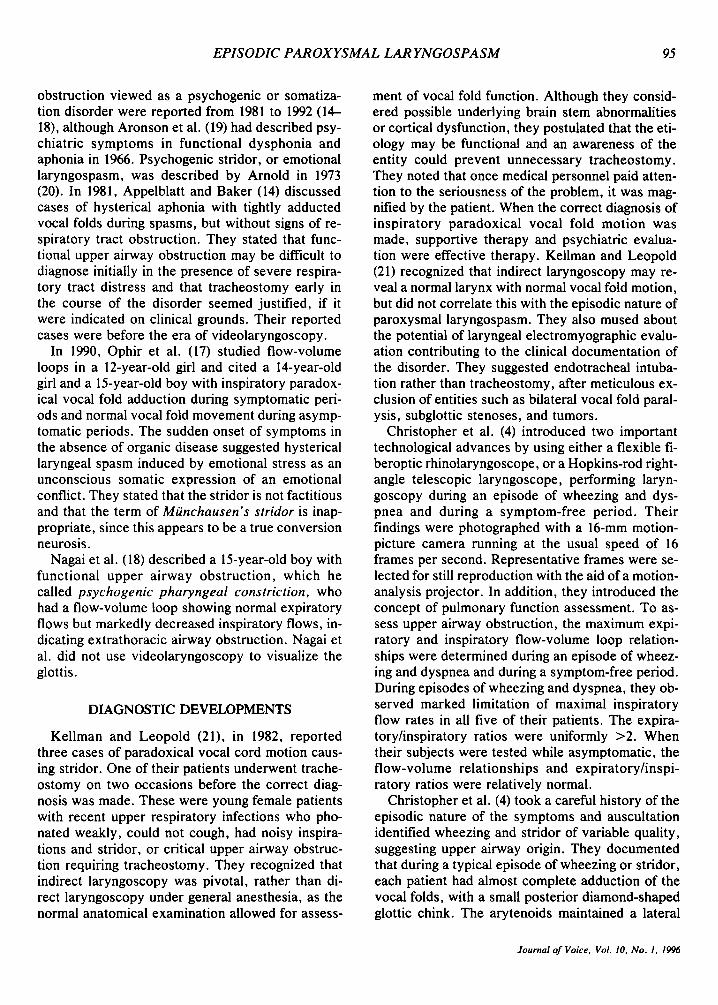
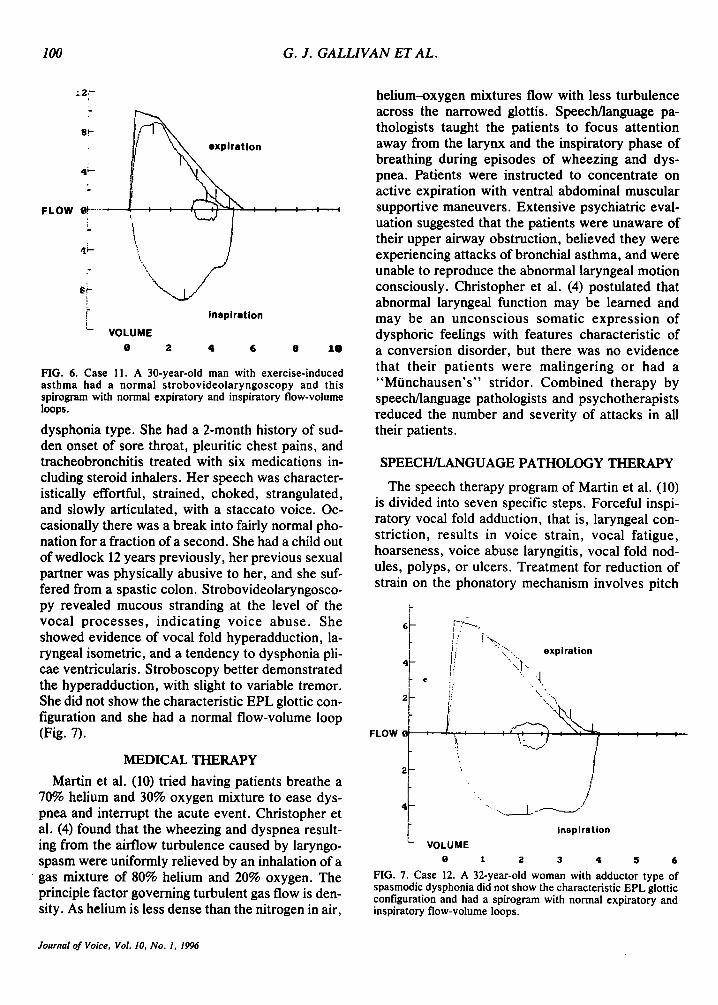
evaluations by allergists, otolaryngologists, pulmo- nologists, and a national center for immunology and respiratory medicine. She had been diagnosed as having paradoxical vocal fold motion, asthma, re- active airways disease, allergies, and episodic dys- functional laryngospasm. She was dependent on her systemic and inhaled steroids and bronchodilators. Strobovideolaryngoscopy revealed the classic find- ings of EPL with fleeting adjunctive mucous strand- ing occasionally occurring across the posterior vo- cal folds, suggesting voice abuse (Fig. 3). Subse-
FIG. 3. Case 7. The classic appearance of paradoxical inspira- tory adduction of the anterior two-thirds of the vocal folds, with a tendency to bowing and a posterior diamond-shaped glottal gap.
quent stroboscopy was normal. Her flow-volume loop during a symptomatic period showed plateau- ing of the inspiratory portion. Insight and exposi- tional approaches failed. She angrily rejected her diagnosis and referrals to a speech/language pathol- ogist and psychiatrist.
Case 8 This 76-year-old man had a l-month history of
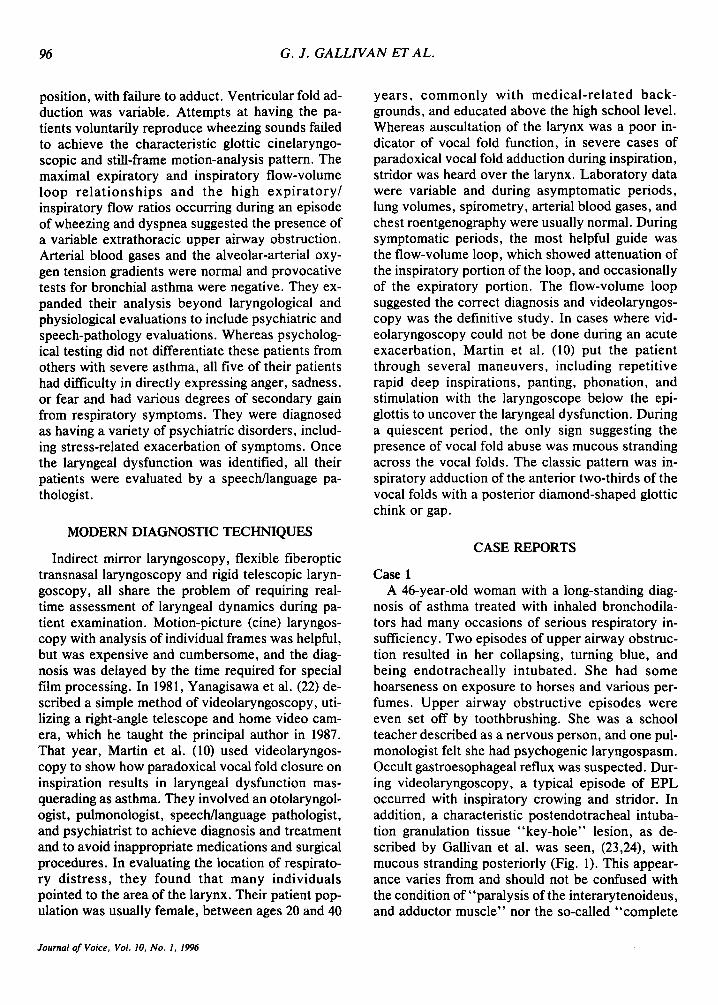
episodes of hoarseness, choking, coughing, and in- ability to catch his breath, after an upper respirato- ry infection. Despite treatment with codeine and inhaled bronchodilators, he was taken to an emer- gency department. Strobovideolaryngoscopy re- vealed the classic findings of EPL with signs of thickening of the posterior vocal folds secondary to the repeated voice abuse of throat clearing. His spirogram was normal in expiration but the inspira- tory portion of the flow-volume loop suggested par- tial, extrathoracic, upper airway obstruction (Fig. 4). He rejected his diagnosis, referral to a speech/ language pathologist, suggested relaxation exer- cises, discussions of psychological issues, and sug- gested workup for gastroesophageal reflux.
Case 9 This 43-year-old man was treated for asthma and
described occasional difficulties in breathing in. He was an accountant by day and a dance instructor by night. He became aphonic during episodes of chok- ing, which he tried to relieve by swallowing and clearing his throat. Strobovideolaryngoscopy re- vealed irregular phonatory margins of the vocal folds, thick and tenacious mucous, pin-point hem-
Journal o f Voice, Vol. I0. No. 1, 1996

EPISODIC PAROXYSMAL LAR YNGOSPASM 99
n
4- i/: ~ expiration
J z -
Inspiration 4~
VOLUME
• I. 2 3 4 5 6 ? il
FIG. 4. Case 8. Flow-volume loop with attenuation of the inspi- ratory flow rate portion suggesting partial extrathoracic upper airway obstruction.
orrhages in the dorsal aspect of the anterior third of the left vocal fold, and EPL. Mucosal waves showed some phase dyssymmetry only during the beginning or end of phonatory tasks, The expiratory portion of his spirogram was normal, but the inspi- ratory portion of the flow-volume loop suggested partial, extra-thoracic, upper airway obstruction (Fig. 5). He accepted speech/language pathology therapy.
Case 10 This 53-year-old woman was referred as an emer-
gency case by an otolaryngologist because of inspi- ratory stridor with paradoxical vocal fold adduc- tion. She had several attacks in rapid sequence, with severe difficulties breathing, coughing, whis- pering and strained voice, flailing her arms, turning "white as a ghost," and almost passing out, during three emergency department visits on one evening. Her daughter, a hospital employee, was particularly intrusive and disruptive to all care providers. The patient had been treated with steroids and antibiot- ics and had a history of Crohn's disease. During repeated bouts of EPL she jumped around in her bed, patted and pounded her face and chest, and progressed to inspiratory and expiratory stridor, auscultated only at the laryngeal level. When atten- tion was momentarily deflected from this patient by another event in the emergency department, the pa- tient's EPL transformed to dysphonic rapid stutter- ing, rhythmic spastic and monosyllabic speech pat- terns, aphonia arrests, and then resolved spontane- ously. Further history revealed an extremely ill and dependent husband, a precipitous fall from afflu- ence to poverty, and stressful familial interrelation- ships. There had been no antecedent history of
asthma or chronic obstructive pulmonary disease. Spirometry was uninterpretable because of the pa- tient's difficulties in cooperating with the maneu- vers required. Videolaryngoscopy revealed the classic findings of EPL. Insight and expositional techniques resulted in a series of disruptive reac- tions by the patient and her daughter, prolonging inpatient hospitalization and delaying appropriate outpatient therapy.
Case 11 In contrast, a 30-year-old man is a representative
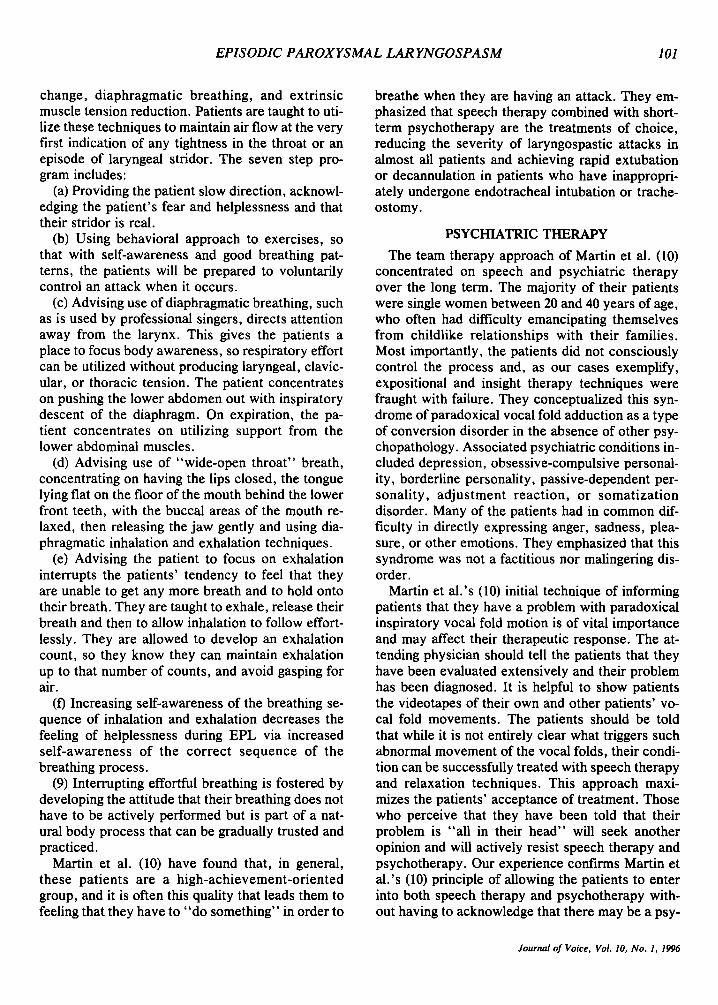
case without EPL in whom the differential diagno- sis was exercise-induced asthma versus laryngo- spasm. He was asthmatic until the age of 5, had a symptom-free interval, and had no voice abnormal- ities. During aerobic exercise, he developed wheez- ing, tightness and choking at the neck level, re- lieved by stopping all activity, resting, or using his albuterol inhaler. He also had episodes of intermit- tent transient cervical dysphagia. He had a normal strobovideolaryngoscopy, before and after he was aerobically exercised by running up and down two flights of stairs. His spirogram with flow-volume loops were normal (Fig. 6).
Case 12 Again in contrast, this 32-year-old woman is a
representative case, without EPL, who had a laryn- geal dystonia of the adductor spasmodic or spastic
I
;
41-
FLOW • i
1 4!-
i
i - t
;
i'~-...~- - .
i..,,,.\ i. \ ' "~' expiration " i '\
t~ ,,
P
inspiration
V O L U M E
• 2 4 6 8 18
FIG. 5. Case 9. Flow-volume loop showing normal expiratory portion and attenuated inspiratory portion suggesting partial ex- trathoracic upper airway obstruction.
Journal of Voice, Vol. 10, No. 1, 1996
100 G. J. GALLIVAN ET AL.
" . 2 r -
8!-
FLOW e, i" .... I I I ' L J /
4:'- :
: . J L I
r" Inspirat ion !_ VOLUME
• ~- 4 6 I 1 I
FIG. 6. Case 11. A 30-year-old man with exerc ise- induced a s t h m a had a no r m a l s t r o b o v i d e o l a r y n g o s c o p y and this spirogram with normal expiratory and inspiratory flow-volume loops.
dysphonia type. She had a 2-month history of sud- den onset of sore throat, pleuritic chest pains, and tracheobronchitis treated with six medications in- cluding steroid inhalers. Her speech was character- istically effortful, strained, choked, strangulated, and slowly articulated, with a staccato voice. Oc- casionally there was a break into fairly normal pho- nation for a fraction of a second. She had a child out of wedlock 12 years previously, her previous sexual partner was physically abusive to her, and she suf- fered from a spastic colon. Strobovideolaryngosco- py revealed mucous stranding at the level of the vocal processes , indicating voice abuse. She showed evidence of vocal fold hyperadduction, la- ryngeal isometric, and a tendency to dysphonia pli- cae ventricularis. Stroboscopy better demonstrated the hyperadduction, with slight to variable tremor. She did not show the characteristic EPL glottic con- figuration and she had a normal flow-volume loop (Fig. 7).
MEDICAL THERAPY
Martin et al. (10) tried having patients breathe a 70% helium and 30% oxygen mixture to ease dys- pnea and interrupt the acute event. Christopher et al. (4) found that the wheezing and dyspnea result- ing from the airflow turbulence caused by laryngo- spasm were uniformly relieved by an inhalation of a gas mixture of 80% helium and 20% oxygen. The principle factor governing turbulent gas flow is den- sity. As helium is less dense than the nitrogen in air,
helium--oxygen mixtures flow with less turbulence across the narrowed glottis. Speech/language pa- thologists taught the patients to focus attention away from the larynx and the inspiratory phase of breathing during episodes of wheezing and dys- pnea. Patients were instructed to concentrate on active expiration with ventral abdominal muscular supportive maneuvers. Extensive psychiatric eval- uation suggested that the patients were unaware of their upper airway obstruction, believed they were experiencing attacks of bronchial asthma, and were unable to reproduce the abnormal laryngeal motion consciously. Christopher et al. (4) postulated that abnormal laryngeal function may be learned and may be an unconscious somatic expression of dysphoric feelings with features characteristic of a conversion disorder, but there was no evidence that their patients were malingering or had a "Mtinchausen's" stridor. Combined therapy by speech/language pathologists and psychotherapists reduced the number and severity of attacks in all their patients.
SPEECH/LANGUAGE PATHOLOGY THERAPY
The speech therapy program of Martin et al. (10) is divided into seven specific steps. Forceful inspi- ratory vocal fold adduction, that is, laryngeal con- striction, results in voice strain, vocal fatigue, hoarseness, voice abuse laryngitis, vocal fold nod- ules, polyps, or ulcers. Treatment for reduction of strain on the phonatory mechanism involves pitch
t
;' " - expiration
I- ! \" """ 4 i "\I-- '!
I " ii " ,
i
2t ' ' I . . . .
~ " ~: " / . . . . . .
" I
t ' I !
L Inspiration VOLUME
0 I 2 3 4 5 6
FIG. 7. Case 12. A 32-year-old woman with adductor type of spasmodic dysphonia did not show the characteristic EPL glottic configuration and had a spirogram with normal expiratory and inspiratory flow-volume loops.
FLOW
Journal of Voice, Vol. 10, No. 1o 1996
EPISODIC PAROXYSMAL LAR YNGOSPASM 101
change, diaphragmatic breathing, and extrinsic muscle tension reduction. Patients are taught to uti- lize these techniques to maintain air flow at the very first indication of any tightness in the throat or an episode of laryngeal stridor. The seven step pro- gram includes:
(a) Providing the patient slow direction, acknowl- edging the patient's fear and helplessness and that their stridor is real.
(b) Using behavioral approach to exercises, so that with self-awareness and good breathing pat- terns, the patients will be prepared to voluntarily control an attack when it occurs.
(c) Advising use of diaphragmatic breathing, such as is used by professional singers, directs attention away from the larynx. This gives the patients a place to focus body awareness, so respiratory effort can be utilized without producing laryngeal, clavic- ular, or thoracic tension. The patient concentrates on pushing the lower abdomen out with inspiratory descent of the diaphragm. On expiration, the pa- tient concentrates on utilizing support from the lower abdominal muscles.
(d) Advising use of "wide-open throat" breath, concentrating on having the lips closed, the tongue lying flat on the floor of the mouth behind the lower front teeth, with the buccal areas of the mouth re- laxed, then releasing the jaw gently and using dia- phragmatic inhalation and exhalation techniques.
(e) Advising the patient to focus on exhalation interrupts the patients' tendency to feel that they are unable to get any more breath and to hold onto their breath. They are taught to exhale, release their breath and then to allow inhalation to follow effort- lessly. They are allowed to develop an exhalation count, so they know they can maintain exhalation up to that number of counts, and avoid gasping for air.
(f) Increasing self-awareness of the breathing se- quence of inhalation and exhalation decreases the feeling of helplessness during EPL via increased self-awareness of the correct sequence of the breathing process.
(9) Interrupting effortful breathing is fostered by developing the attitude that their breathing does not have to be actively performed but is part of a nat- ural body process that can be gradually trusted and practiced.
Martin et al. (10) have found that, in general, these patients are a high-achievement-oriented group, and it is often this quality that leads them to feeling that they have to "do something" in order to
breathe when they are having an attack. They em- phasized that speech therapy combined with short- term psychotherapy are the treatments of choice, reducing the severity of laryngospastic attacks in almost all patients and achieving rapid extubation or decannulation in patients who have inappropri- ately undergone endotracheal intubation or trache- ostomy.
PSYCHIATRIC THERAPY
The team therapy approach of Martin et al. (10) concentrated on speech and psychiatric therapy over the long term. The majority of their patients were single women between 20 and 40 years of age, who often had difficulty emancipating themselves from childlike relationships with their families. Most importantly, the patients did not consciously control the process and, as our cases exemplify, expositional and insight therapy techniques were fraught with failure. They conceptualized this syn- drome of paradoxical vocal fold adduction as a type of conversion disorder in the absence of other psy- chopathology. Associated psychiatric conditions in- cluded depression, obsessive-compulsive personal- ity, borderline personality, passive-dependent per- sonality, adjustment reaction, or somatization disorder. Many of the patients had in common dif- ficulty in directly expressing anger, sadness, plea- sure, or other emotions. They emphasized that this syndrome was not a factitious nor malingering dis- order.
Martin et al.'s (10) initial technique of informing patients that they have a problem with paradoxical inspiratory vocal fold motion is of vital importance and may affect their therapeutic response. The at- tending physician should tell the patients that they have been evaluated extensively and their problem has been diagnosed. It is helpful to show patients the videotapes of their own and other patients' vo- cal fold movements. The patients should be told that while it is not entirely clear what triggers such abnormal movement of the vocal folds, their condi- tion can be successfully treated with speech therapy and relaxation techniques. This approach maxi- mizes the patients' acceptance of treatment. Those who perceive that they have been told that their problem is "all in their head" will seek another opinion and will actively resist speech therapy and psychotherapy. Our experience confirms Martin et al.'s (10) principle of allowing the patients to enter into both speech therapy and psychotherapy with- out having to acknowledge that there may be a psy-
Journal of Voice, Vol. 10, No. 1, 1996

102 G. J. GALLIVAN ET AL.
chiatric cause for the condition. The initial aim of psychotherapy is to allow the patients to retain many of their psychiatric symptoms without need- ing to utilize EPL as a coping syndrome. Psycho- therapy includes relaxation exercises and support- ive therapy with alleviation of patients' fears and fantasies concerning their health or dying. Changes in the health care plan, including discontinuation of steroids in patients misdiagnosed as asthmatics, must be discussed in detail. Education about health care options and side-effects must be provided and active support given for the positive changes the patient makes. It is useful to deal with this in a limited paradigm and brief psychotherapy format, rather than in long-term insight-oriented dynamic therapy. Patients resistant to individual psychother- apy may benefit from expansion of that treatment to the entire family, focusing on issues of emancipa- tion from the home and the intensity of family dy- namics associated with the illness.
DISCUSSION
EPL versus asthma To establish EPL as an entity, it is necessary to
differentiate its diagnosis and treatment from other disorders. Brown et al. (II) presented a solitary case of a depressed woman with psychogenic vocal fold dysfunction who had long been misdiagnosed as an asthmatic. O'Halloran (26), in 1990, indepen- dently documented that when the vocal folds ap- proximate during inspiration, severe subjective dys- pnea may occur, without evidence of hypoxia, or abnormality in the alveolar-arterial oxygen gradi- ent. He found that provocative asthma tests with methacholine were negative in his group of predom- inantly female patients with paradoxical vocal fold motion, many of whom had an affiliation with the medical profession and had psychological difficul- ties.
Caraon and O'Toole (27), in 1991, described a 14-year-old boy with deteriorating asthma and marked stridor whose paradoxical fold adduction throughout the respiratory cycle responded to psy- chotherapy and hypnotherapy.
Isolated case reports from the literature identify- ing vocal fold dysfunction presenting as asthma were documented by Lim in 1991 (28) and by Fields et al. in 1992 (29). Craig et al. (30), in 1991, docu- mented paradoxical fold dysfunction masquerading as asthma during wartime. Corren and Newman (31), in 1992, and Sokal, in 1993 (32) emphasized history, pulmonary function tests, and direct visu-
alization of the larynx during an acute attack to dif- ferentiate the vocal fold dysfunction of EPL from asthma. Schmidt (33) described functional laryngos- pasm, stated "not all wheezing is asthma" and uti- lized laryngoscopy and pulmonary function tests.
Magnenat and Junod (34), in 1991, presented five cases that they termed to be episodic laryngeal dys- kinesia. They made the definitive diagnosis by ex- cluding organic pathology, visualizing the laryngeal spasm, and inspecting flow-volume loops, thereby differentiating the reversible and recurrent entity of EPL from bronchial asthma, laryngeal edema, and stenosing lesions of the upper airways. They em- phasized that the diagnostic criteria were important in avoiding too aggressive an approach in these pa- tients.
Gastroesophageal reflux disease (GERD) Kaufman (35) suggested that we don't yet know
the aerodigestive manifestations of gastroesoph- ageal reflux. Psychosomatic response to stress may be associated with an increased incidence of GERD. It is known that GERD can cause aerodi- gestive, particularly asthmatic and laryngopharyn- geal symptoms and signs in patients who do not have a history of pyrosis or regurgitation, and who may have dysphonia, hoarseness, cervical dyspha- gia, globus pharyngeus, asthma, chronic throat clearing, and chronic cough.
In several of our EPL cases in whom dysphagia has been one of the significant complaints, transna- sal flexible fiberoptic videolaryngoscopic evalua- tion of swallowing, utilizing special effects tech- niques, including 28 to 30 frames-per-second slow motion and freeze-frame, forward and reverse stop motion techniques, visualized supraglottic and glot- tic function, as well as laryngeal excursion with deglutition (swallowing). A relationship between EPL and GERD was suggested by the usual video- laryngoscopic criteria of cherry-red arytenoids and by cineradiography and other routine evaluations by our Swallowing and Esophageal Disorders Pro- gram, the details of which are beyond the scope of the present paper.
Psychosomatic/somatization disorder Starkman and Appelblatt (15) explored the tem-
poral association of stressful environmental stimuli in the initiation of symptoms, as well as the evi- dence of serious underlying psychiatric distur- bances. Features were similar to those found in pa- t ients with asthma, in whom conflicts of ten stemmed from exaggerated dependency needs and
.Journal of Voice, Vol. 10, No. I, 1996
EPISODIC P A R O X Y S M A L L A R Y N G O S P A S M 103
fears of separation. Patients were resistant to psy- chological exploration and guarded about describ- ing ongoing family difficulties. EPL occurred, in some cases, not as an isolated or pure conversion symptom, but rather in the context of a more per- vasive psychiatric disturbance, such as panic disor- der and a borderline personality disorder. Upon learning that laryngoscopy revealed no organic dis- ease, anger, agitation, and resistive behavior re- suited. Laryngospasm could be viewed as a behav- ioral response to ward off dysphoric affect.
In describing functional upper airway obstruction as a somatization disorder, Sim et al. (16) suspected an upper airway lesion due to the presence of inspi- ratory stridor and the maximal intensity of the wheezing sound heard over the larynx in their case report of a 30-year-old woman. She experienced re- current stridor refractory to therapeutic doses of prednisone, hydroxyzine, and cimetidine. During a documented attack, the maximum expiratory and inspiratory flow-volume relationship and the high expiratory/inspiratory ratio suggested the presence of variable extrathoracic airway obstruction. Direct laryngoscopy showed paradoxical vocal fold adduc- tion during inspiration. The psychiatric evaluation disclosed dependent behavior and high levels of anxiety, which were considered to be triggering her functional laryngeal obstruction. They emphasized the typical history involving paroxysms of stridor or wheezing, which could be induced by bizarre trig- gers and were refractory to standard therapies, such as high doses of steroids. Episodes usually occurred suddenly rather than developing over an extended period of time. Their flow-volume loops showed the normal curves during asymptomatic periods with an expiratory/inspiratory ratio of 1.13. Marked attenu- ation of inspiratory flow loops occurred during symptomatic periods, with expiratory to inspiratory ratios ranging from 3.12 to 5.18. Sim et al.'s pa- tient's laryngeal dysfunction may have symbolized the subconscious somatic expression of her dyspho- ric feelings, with features characteristic of a conver- sion disorder. Psychological intervention was di- rected at anxiety control, assisted by biofeedback, and then externalizing emotional fear or anger, rather than succumbing to a "choking-off" internal- ization mechanism, which may be identified with psychosomatic upper airway dysfunction.
Treatment alternatives Insight therapy is usually not beneficial, as pa-
tients may feel a conscious sense of shame about
the disorder, fears of confiding, fears of rejection, and struggles between attachment and interdepen- dence (36). Counseling, education, relaxation tech- niques, and oral asthma therapy used as a placebo have all been successful treatment modalities (37). It may be worthwhile to explain to the patient the role of precipitating psychological factors, muscle tension, and anticipatory anxiety in the production of the disorder. The interaction and additive effects of organic and psychosocial factors may also be re- viewed as part of patient preparation. Hypnotic suggestion may be of value in some cases. Proper understanding of the misuse of voluntary muscula- ture in patients with psychological conflicts enables the treating psychiatrist to collaborate more readily with both the speech/language pathologist and the laryngologist (38).
In presenting two patients with EPL triggered during bronchoscopy, Pitchenik (39) utilized a pant- ing maneuver, which was successful in relieving 25 to 30 recurrent attacks of functional laryngeal ob- struction. He suggested that panting may be an ef- fective emergency measure for relief of EPL in those patients on whom videolaryngoscopic and flow-volume loop documentation has made the di- agnosis. We have found this maneuver to be suc- cessful in some patients.
ELECTROMYOGRAPHY (EMG) OF FUNCTIONAL VOICE DISORDERS
EMG is an objective method available to study laryngeal muscle activity, as pointed out in 1994 by Gould and Korovin (40). EMG provides informa- tion about the electrical activity resulting from con- traction of muscles or motor units. These studies help determine which laryngeal muscles are being used during different respiratory and phonation conditions. An EMG can tell an investigator wheth- er a muscle is operating, when a muscle starts and stops contracting, whether paired muscles fire in synchrony, and to what extent a muscle is contract- ing. Needle electrodes can be placed into the crico- thyroid and thyroarytenoid muscles, while the lat- eral and poster ior cr icoarytenoid muscles are reached via a transoral approach. Surface elec- trodes have also been used. Extensions of such use of the EMG could eventually improve diagnosis and prognosis in evaluating functional laryngeal defi- cits.
Hirano (41), in 1981, cited the 1965 work of Sram and Kalvodov,-I in which they reported their elec-
Journal of Voice, Vol. 10, No. 1, 1996
104 G. J. GALLIVAN ET AL.
tromyographic findings in patients with psy- chogenic aphonia and in those with spastic dyspho- Ilia. The vocalis muscles showed irregular activities during normal and deep breathing. In psychogenic aphonia, there was no consistent picture of the pat- tern and duration of interference potentials during attempted phonation. The potentials either de- creased, disappeared, or temporarily increased. In spastic dysphonia, an increase in tension of the vo- calis muscle was found at rest as well as during phonation.
Hirano (41) documented electromyograms of the laryngeal muscles of a patient with psychogenic dysphonia. While her larynx appeared normal dur- ing respiration under observation with a laryngeal mirror, when she attempted to phonate, the poste- rior part of her glottis was not completely closed. EMG revealed that the posterior cricoarytenoid was active during phonation as well as during inspi- ration. The cricothyroid and the adductor muscles showed normal patterns of activity. Incomplete glottic closure during phonation, he postulated, could be attributed to the neutralization of the ac- tivity of the adductor muscles as a result of the contraction of the posterior cricoarytenoid muscle. Electromyographic studies may become an impor- tant tool in EPL in the future.
LARYNGEAL DYSTONIA
Blitzer and Brin (42) described laryngeal dystonia as a neurological disorder of central motor process- ing characterized by action-induced spasms of the vocal folds that produce a clinical voice syndrome often termed spasmodic or spastic dysphonia, with subclassifications of adductor, abductor, and mixed types. The adductor patients have uncontrolled spasms during phonation characterized by a stran- gulated, strained voice pattern with breaks, vocal tremor, harshness, and grunts, whereas the abduc- tor types have whispered dysphonic breaks and a breathy voice. The laryngeal dystonia patients al- most never have the characteristics of EPL.
Blitzer and Brin (43) emphasized that the patient with a dystonic larynx should be put through vocal tasks to look for tremor and hyperadduciton, which are often completely missed on mirror indirect la- ryngoscopy. On videolaryngoscopy, hyperadduc- tion produced a slightly open posterior commissure (laryngeal isometric) or caused closure of the ven- tricular folds or narrowing of the anteroposterior dimension of the glottis, because of tipping of the
arytenoids anteriorly or complete apposition of the arytenoids against the petiole of the epiglottis. They found that strobovideolaryngoscopy may be useful in defining tremor and better demonstrating the hy- peradduction.
Strobovideolaryngoscopic examination on pa- tients with abductor dystonia revealed a synchro- nous and untimely abduction of the vocal folds ex- posing an extremely wide glottal gap. These abduc- tor spasms were triggered by consonant sounds, particularly when the consonants were in the initial position of words, the patients were under stress or using the telephone. The abductor spasmodic dys- phonia patients often have a normal laugh, normal yawn, normal humming, and occasionally a normal singing voice (43).
The third category of patients with compensatory abductor dysphonia voluntarily produced a breathy voice by not contracting their vocal folds in order to prevent the spasms in the broken speech pattern of adductor dystonia. There was an even rarer entity, compensatory adductor dysphonia, in which the pa- tients tried to prevent the breathiness of abductor dystonia by tightly contracting their vocal folds (43).
The National Institutes of Health Consensus De- velopment Conference Consensus Statement from 1990 suggested that botulinum toxin was effective therapy for laryngeal dystonia, including adductor spasmodic dysphonia, abductor spasmodic dyspho- nia, as well as stuttering and vocal tremor (44).
Grillone et al. (45) have described adductor laryn- geal breathing dystonia (ALBD) as a rare disorder characterized by inspiratory stridor, normal voice, cough, dysphagia, and paradoxical, involuntary, ac- tion-induced adduction spasms of the vocal folds on inspiration. They stated that while the diagnosis may be confused with other disorders characterized by airway noise or cough, such as asthma, GERD, or "psychogenic stridor" (EPL), the diagnosis of ALBD is further supported by the finding of dysto- nias involving other segments of the body and an associated respiratory and diaphragmatic dysrhyth- mia. Speech therapy, psychotherapy, and pharma- cotherapy have all had limited success in treating ALBD, but botulinum toxin type A bilateral thy- roarytenoid injections were successfully used in seven patients. The diagnosis needs to be precise before giving therapy.
We encourage the future application of laryngeal EMG in patients who have EPL. Recognizing that laryngeal dystonia patients almost never have EPL,
Journal of Voice, Vol. 10, No. 1, 1996
E P I S O D I C P A R O X Y S M A L L A R Y N G O S P A S M 105
pat ien ts with E P L are no t necessa r i ly cand ida te s for b o t u l i n u m toxin type A and can be effect ively t rea ted by speech / l anguage pa tho logy and psychia t - ric t echn iques .
Acknowledgment: We are deeply indebted to Helen K. GaUivan and Laurie H. Dagesse for their steadfast sup- port, understanding, and assistance in developing, pro- ducing, and editing this article.
R E F E R E N C E S
1. Jackson C, Jackson CL. Motor neuroses of the larynx. In: Diseases and injuries of the larynx-...-a textbook for students
tomatology in functional dysphonia and aphonia. J Speech Hear Dis 1966;31:115-27.
20. Arnold GE. Disorders of laryngeal function. In: Paparella MM, Shumrick DA, eds. Otolaryngology. Philadelphia: W.B. Sanders, 1973;3:631.
21. Kellman RM, Leopold DA. Paradoxical vocal cord motion: an important cause of stridor. Laryngoscope 1982;92:58--60.
22. Yanagisawa E, Casuccio JR, Suzvi N. Videolaryngnscopy using a rigid telescope and video home system color camera: a useful procedure. Ann Otol Rhinol Laryngol 1981 ;90:346--50.
23. Gallivan G J, Dawson JA, Robbins LD. Critical care perspec- five: videolaryngoscopy after endotracheal intubation: im- plication for voice. Voice 1989;3:76--80.
24. Gallivan GJ, Dawson JA, Opfell "AP. Videolaryngnscopy af- ter endotracheal intubation: part II. A critical care perspec- tive of lesions affecting voice. Voice 1990;4(2): 159--64.
25. Jackson C, Jackson CL. Adductor paralysis of the larynx. In: Diseases and injuries of the larynx--a textbook for stu- dents and practitioners. New York: The MacMillan Com- pany, 1942:305-14.
26. O'Halloran MT. Masqueraders in clinical allergy: laryngeal dysfunction causing dyspnea. Ann Allergy 1990;65:351--6.
27. Caraon P, O'Toole C. Vocal cord dysfunction presenting as asthma. Irish Medical Journal 1991 ;84:98-9.
28. Lira TK. Vocal cord dysfunction presenting as bronchial asthma: the association with abnormal thoraco-abdominal wall motion. Singapore Med J 1991 ;32:208--10.
29. Fields CL, Roy TM, Ossorio MA. Variable vocal cord dys- function: an asthma variant. South Med J 1992;85:422--4.
30. Craig T, Sitz K, Squire E, Smith L, Carpenter G. Vocal cord dysfunction during wartime. Military Medicine 1991;157: 614--6.
31. Corren J, Newman KB. Vocal cord dysfunction mimicking bronchial asthma. Postgrad Med 1992;92:153--6.
32. Sokol W. Vocal cord dysfunction presenting as asthma. West J Med 1993;158:614-5.
33. Schmidt M. Not all wheezing is asthma: on functional laryn- gospasm. Pneumonologie 1993;47:439--42.
34. Magnenat JL, Junod AF. Episodic laryngeal dyskinesia: a functional cause of stridor. Rev Mal Respir 1991;8:95-9.
35. Kaufman JA. Aerodigestive manifestations of gastroesoph- ageal reflux: what we don't yet know. Chest 1993;104: 1321-2.
36. Vachon L. Respiratory disorders. In: Kaplan HI, Sadock B J, ed. Comprehensive textbook of psychiatry. 5th ed. Bal- timore: Williams & Wilkins, 1992:1207-9.
37. Meitzer EO, Orgel HA, Kemp JP, Welch MJ, Ostrom NK, Park SM, Kearns DB. Vocal cord dysfunction in a child with asthma. J Asthma 1991 ;28:141-5.
38. Nichol H, Morrison MD, Rammage LA. Interdisciplinary approach to functional voice disorders: The psychiatrist's role. Otolaryngol Head Neck Surg 1993;108:643-7.
39. Pitchenik AE. Functional laryngeal obstruction relieved by panting. Chest 1991 ;100:1465-7.
40. Gould WJ, Korovin GS. The G. Paul Moore lecture: Labora- tory Advances for Voice Measurements. Voice 1994;8:8-17.
41. Hirano M. Clinical examination of voice. New York: Springer-Verlag, 1981:21-2.
42. Blitzer A, Brin MF. Laryngeal dystonia: a series with botu- linum toxin therapy. Ann Otol Rhinol Laryngol 1991;100: 85-9.
43. Blitzer A, Brin MF. The dystonic larynx. Voice 1992;6: 294-7.
44. Clinical use of botulinum toxin (Reprinted from NIH Cons- ens Dev Conf. Consens Statement 1990 (Nov 12-14);8(8).
45. Grillone GA, Blitzer A, Brin MF, Annino DJ Jr, Saint- Hilalre M-H. Treatment of adductor laryngeal breathing dys- tonia with botulinum toxin type A. Laryngoscope 1994;104: 30-2.
Journal of Voice,.Vol. 10, No. 1, 1996





























