Embed Size (px)
Citation preview

E
RMNa
b
c
d
e
f
a
AA
KHAEMM
1
dafm(so(
t(skc
B
(
1h
Respiratory Physiology & Neurobiology 186 (2013) 146– 154
Contents lists available at SciVerse ScienceDirect
Respiratory Physiology & Neurobiology
j o ur nal homep age : www.elsev ier .com/ locate / resphys io l
po deficiency alters cardiac adaptation to chronic hypoxia
aja El Hasnaoui-Saadania,∗, Dominique Marchanta, Aurélien Pichona, Brigitte Escoubetb,e,f,ylène Pezetb, Denise Hilfiker-Kleinerc, Melanie Hochc, Isabelle Phama, Patricia Quidua,icolas Voiturona, Clément Journéb, Jean-Paul Richaleta, Fabrice Favreta,d
Université Paris 13, Sorbonne Paris Cité, EA2363 «Réponses cellulaires et fonctionnelles à l’hypoxie», 93017 Bobigny, FranceUniversité Paris-Diderot, Centre d’Exploration Fonctionnelle – Imagerie – IFR02 75018 Paris, FranceDepartment of Cardiology and Angiology, Medical School Hannover, 30625 Hannover, GermanyUniversité de Strasbourg, Faculté de Médecine, EA3072 «Mitochondrie, Stress Oxydant et Protection Musculaire», 67000 Strasbourg, FranceInserm UMR 872, Centre de Recherche des Cordeliers, 75006 Paris, FranceAssistance Publique – Hôpitaux de Paris, Hôpital Bichat, 75018 Paris, France
r t i c l e i n f o
rticle history:ccepted 8 January 2013
eywords:ypoxianemiarythropoietin
a b s t r a c t
The involvement of erythropoietin in cardiac adaptation to acute and chronic (CHx) hypoxia was inves-tigated in erythropoietin deficient transgenic (Epo-TAgh) and wild-type (WT) mice. Left (LV) and rightventricular functions were assessed by echocardiography and hemodynamics. HIF-1�, VEGF and Epopathways were explored through RT-PCR, ELISA, Western blot and immunocytochemistry. Epo geneand protein were expressed in cardiomyocytes of WT mice in normoxia and hypoxia. Increase in bloodhemoglobin, angiogenesis and functional cardiac adaptation occurred in CHx in WT mice, allowing a
yocardial vascularisationyocardial contractility
normal oxygen delivery (O2T). Epo deficiency induced LV hypertrophy, increased cardiac output (CO)and angiogenesis, but O2T remained lower than in WT mice. In CHx Epo-TAgh mice, LV hypertrophy,CO and O2T decreased. HIF-1� and Epo receptor pathways were depressed, suggesting that Epo-TAgh
mice could not adapt to CHx despite activation of cardioprotective pathways (increased P-STAT-5/STAT-5). HIF/Epo pathway is activated in the heart of WT mice in hypoxia. Chronic hypoxia induced cardiac
ere a
adaptive responses that w. Introduction
Exposure to intermittent and chronic hypoxia has been shown toevelop coronary vasculature, decrease infarction size, and provide
more efficient metabolism and a better post-ischemic cardiacunctional recovery (Anderson and Honigman, 2011). Part of the
echanisms involved are mediated via the hypoxia inducible factorHIF-1�), a transcription factor which increases the gene expres-ion of erythropoietin (Epo) as well as other factors implied inxygen homeostasis such as vascular endothelial growth factorVEGF) (Cassavaugh and Lounsbury, 2011).
Epo is a circulating glycoprotein hormone that controls ery-hropoiesis by stimulating the proliferation of erythroid precursorsJelkmann, 1992; Mole and Ratcliffe, 2008). Tissue-specific expres-
ion of the Epo gene is tightly controlled and in the adult organism,idneys produce around 90% of circulating Epo (Jelkmann, 1992). Inomparison to kidneys, sensitive mRNA assays demonstrated low∗ Corresponding author at: EA2363 UFR SMBH, 74 rue Marcel Cachin, 93017obigny Cedex, France. Tel.: +33 1 48388876; fax: +33 1 48388924.
E-mail addresses: [email protected], [email protected]. El Hasnaoui-Saadani).
569-9048/$ – see front matter © 2013 Elsevier B.V. All rights reserved.ttp://dx.doi.org/10.1016/j.resp.2013.01.003
ltered with Epo deficiency, failing to maintain oxygen delivery to tissues.© 2013 Elsevier B.V. All rights reserved.
levels of Epo mRNA in the brain from neurons and astrocytes, testis,lung and spleen (Jelkmann, 1992; Marti, 2004). More recently, somereports showed that heart could be an additional Epo productivetissue (Bin-Jaliah et al., 2010; Cai and Semenza, 2004), in particularthat cardiac tissue reveals Epo gene and protein expression (Hochet al., 2011; Miro-Murillo et al., 2011). Through specific bindingto its receptor (EpoR), Epo triggers intracellular signaling eventsthat depend on the activation of Jak2 tyrosine kinase (Koury andBondurant, 1992). The exploration of these pathways revealed thatEpo is also an angiogenic as well as an anti-apoptotic factor asdescribed respectively in the brain (Digicaylioglu and Lipton, 2001)and the heart (Kertesz et al., 2004; Marzo et al., 2008). Indeed, injec-tion of Epo promoted the differentiation of progenitor cardiac cellsinto endothelial cells (Hoch et al., 2011).
Angiogenesis is also a major component of the physiologicalresponse to hypoxia as it allows an increased blood supply and sub-sequent oxygen and nutrient delivery to oxygen deficient tissues.Under hypoxic conditions, angiogenesis is primarily driven by HIF-dependent transcription of VEGF (Forsythe et al., 1996; Levy et al.,
1998).Our model of erythropoietin-SV40 T antigen (Epo-TAgh) trans-genic mice presents a targeted disruption in the 5′ untranslatedregion of the Epo gene that severely reduces its expression (Binley

hysio
eAcvccb
ioeEfdetaaE
2
2
wbRl
2
FwWthEMCpNmw1Ath
2
2
tcn(Bfr5fflac
R. El Hasnaoui-Saadani et al. / Respiratory P
t al., 2002; Maxwell et al., 1993) and then induces chronic anemia.s previously demonstrated, these Epo-TAgh mice can survive inhronic hypoxia (14 days at 4500 m), in part through an increase inentilation and probably a higher cardiac output with a significantardiac hypertrophy (Macarlupu et al., 2006a,b). We also evidencederebrovascular adaptations to chronic anemia and hypoxia in therain of these mice (El Hasnaoui-Saadani et al., 2009).
The objectives of the present study were therefore (1) to ver-fy the expression of Epo in the heart, (2) to assess the effectsf hypoxia on the Epo pathways in the heart, (3) to assess theffect of Epo-deficiency (using our Epo-TAgh mutant mice) on thepo pathways in the heart, (4) and finally to determine if heartunction is maintained in chronic hypoxia despite chronic Epoeficiency. We explored myocardial contractile function throughchocardiography and catheterization, and angiogenesis throughhe HIF-1�/VEGF pathway. The initiation of cardioprotective mech-nisms was estimated through EpoR/P-STAT5 signalization as wells by a change in the P-STAT5/STAT5 ratio in response to chronicpo deficiency and/or hypoxia.
. Methods
.1. Ethics statement
All the experimental procedures were performed in agreementith the Guide for the Care and Use of Laboratory Animals published
y the National Institutes of Health (NIH Publication No. 85-23,evised 1996) and were approved by the French “Ministère de
’Agriculture” Guidelines (authorization number A-93-008-01).
.2. Animal model and experimental groups
Male Wild-Type (WT) F1 BL6/CBA (Charles River, L’Arbresle,rance) and male Epo deficient SV-40T antigen (Epo-TAgh) miceere randomly divided into six groups: normoxic wild-type (NxT); normoxic Epo-TAgh (Nx Epo-TAgh); acute hypoxic wild-
ype (AHx WT); acute hypoxic Epo-TAgh (AHx Epo-TAgh); chronicypoxic wild-type (CHx WT); and chronic hypoxic Epo-TAgh (CHxpo-TAgh). At the moment of dissection all mice were 8 week old.ice undergoing AHx were housed for 48 h and mice undergoing
Hx housed for 14 days in a hypoxic chamber connected to a gasump where air circulated at a pressure of 420 mm Hg (∼4500 m).ormoxic groups were kept in a normobaric normoxic environ-ent (760 mm Hg) outside the hypobaric chamber. All animalsere housed in standard conditions (temperature 20–23 ◦C with a
2 h light:12 h dark cycle) and had free access to tap water and food.t the end of each experiment, intra cardiac blood samples were
aken for hemoglobin measurement (OSM 3, Radiometer, Copen-agen, Denmark).
.3. Physiological measurements
.3.1. EchocardiographyMice underwent echocardiography under isoflurane light anes-
hesia (0.75–1% in oxygen), before and after acclimatization tohronic hypoxia (Nx WT, Nx Epo-TAgh, CHx WT and CHx Epo-TAgh
= 6 per group), using a PowerVision 6000, SSA 370A apparatusToshiba, Tokyo, Japan) equipped with a 14-MHz linear probe.riefly, the heart was visualized in the long axis parasternal view
or M-mode left ventricle (LV) dimension measurement and poste-ior wall pulse wave tissue Doppler measurement. An apical 4- to-chamber view was obtained from the subcostal view for diastolic
unction assessment with pulse wave spectral LV inflow and out-ow and for pulse wave tissue Doppler measurement of the mitralnnulus velocities (Parlakian et al., 2005). Cardiac output was cal-ulated as stroke volume x heart rate and indexed to body weight.logy & Neurobiology 186 (2013) 146– 154 147
Stroke volume was calculated from the LV volumes from paraster-nal view and TM measurement. Oxygen transport was calculatedas cardiac output x arterial oxygen content.
2.3.2. Hemodynamic measurementsIn brief, mice (Nx WT, Nx Epo-TAgh, CHx WT and CHx Epo-TAgh
n = 6 per group) were sedated with isoflurane anesthesia (1.0–1.5%in oxygen). After right thoracotomy, a 2-French micromanometer-tipped catheter (Millar Instruments Inc., Houston, TX) was placedin the right ventricular (RV) cavity through the apex. The RV pres-sure (peak systolic, end-diastolic and developed pressures), andits maximal and minimal derivatives (dP/dtmax and dP/dtmin) wererecorded with a IOX 1.8.9.4. software (Emka-technologies, Paris,France). All data are reported as the means for 15 steady-statecardiac cycles.
2.3.3. Systolic arterial blood pressure in awake miceArterial systolic blood pressure (BP) and heart rate were
measured by the tail-cuff plethysmography method in trained con-scious mice (Nx WT, Nx Epo-TAgh, CHx WT and CHx Epo-TAgh
n = 6 per group) placed in a warming restrainer (Marty Technologie,Phymep, Paris, France). Tail-cuff pressure detected by a pressuretransducer (SP844; SensoNorasa, Oslo, Norway) and tail arterialpulsations detected by a piezoelectric pulse sensor were amplifiedby a signal amplifier Qazap 92204-02 (Bionic Instruments, Phymep,Paris, France). Signals were processed and displayed by meansof a PowerLab/4SP program (ADInstruments, Colorado Springs,CO). Arterial blood pressure was defined as the tail-cuff inflationpressure at which the waveform was extinguished. For all mice,measurements were repeated for 3 days, between 10 a.m. and 1p.m. Each day, approximately ten consecutive inflation cycles wereperformed, and final blood pressure was calculated by averagingsuccessful readings. Heart rate, computerized on-line, was readduring stable resting phases preceding inflation cycles (Le Menuetet al., 2001).
2.4. Biological measurements
2.4.1. Real-time RT-PCRmRNAs were extracted from total hearts of mice (Nx, AHx and
CHx; n = 6 in each group) by using the TRI-Reagent (Invitrogen,Carlsbad, CA, USA). cDNAs were synthesized from 5 �g of mRNAwith the SuperScript III First-Strand Synthesis System (Invitrogen,Carlsbad, CA, USA). Finally, real-time PCR was performed to quan-tify the expression of HIF-1�, VEGF, Epo and EpoR mRNA in theexperimental samples, using the Light Cycler FastStart DNA Mas-ter SYBR Green I (Roche Biochemicals, Stockholm, Sweden). Theprimers sequences and RT-PCR parameters used in this study aredescribed in Table 1. The PCR products of Epo gene were then loadedin agarose gel 2%, purified and sequenced (Millegen, Toulouse,France).
2.4.2. Plasma and heart Epo immunoassayThe quantitative determination of mouse Epo concentration
([Epo]) in plasma and heart extracts from Nx WT, Nx Epo-TAgh,AHx WT, AHx Epo-TAgh, CHx WT and CHx Epo-TAgh mice (n = 6per group) were assayed by Enzyme-Linked Immunosorbent assay(ELISA) using the Quantikine Mouse Epo Immunoassay (R&Dsystems Europe, Abingdon, UK). Plasma collection and assay pro-cedure were carried out following the manufacturer’s instructions.Because nothing is known about Epo concentration in the heart,we did not separate the ventricles and samples were homogenized
in a very low quantity of ice cold PBS to ensure a sufficient pro-tein quantity for the detection by the kit. The concentration of Epo(pg/mL) detected in each sample was compared to the Epo standardcurve. Finally, data were expressed in pg/mL for plasma, and as the
148 R. El Hasnaoui-Saadani et al. / Respiratory Physiology & Neurobiology 186 (2013) 146– 154
Table 1Sequence and hybridization temperature (Tm) of specific primers.
Gene name Forward 5′–3′ Reverse 5′–3′ Tm Amplicon size bps Genbank accession number
HIF 1� AGCCCTAGATGGCTTTGTGA TATCGAGGCTGTGTCGACTG 62 ◦C 467 NM 010431VEGF GCCAGCACATAGAGAGAATGAGC CAAGGCTCACAGTGATTTTCTGG 63 ◦C 97 M95200
CCCC ◦
TACAGGCCG
rm
2
Aw15((2dShtd
2
Wea(btTfi6Snadun4o
2
ErhpwpSopkdw
2
T
Epo AACGTCCCACCCTGCTGCTTTT TGTACAGCTTCAGTTTEpoR GCTCCGGGATGGACTTCA GAGCCTGGTGCAGGC�-Actin AGAGGGAAATCGTGCGTGAC CAATAGTGATGACCT
atio of the quantity of Epo (in pg) to the total protein content (ing) in the hearts.
.4.3. Determination of active HIF-1˛Nuclear extracts from total heart of Nx WT, Nx Epo-Tgh, AHx WT,
Hx Epo-TAgh, CHx WT and CHx Epo-TAgh mice (n = 6 per group)ere obtained by using a lysis buffer A (10 mM HEPES (pH 7.9),
.5 mM MgCl2, 10 mM KCl, 0.5 mM DTT, 0.1% NP-40, 2 mM Na3VO4, mM NaF, and antiproteinase cocktail). Samples were centrifuged5000 × g, 5 min, 4 ◦C) and pellets were submitted to a lysis buffer B20 mM HEPES (pH 7.9), 1.5 mM MgCl2, 420 mM NaCl, 0.5 mM DTT,5% glycerol, 2 mM Na3VO4, 5 mM NaF and antiprotease coktail) asescribed in the protocol of DuoSet IC Mouse active HIF-1 ̨ (R&Dystem, Europe, Abingdon, UK). The determination of active HIF1-˛as been carried out as described by the manufacturer (R&D Sys-em, Europe, Abingdon, UK). Results are expressed as mean opticalensity (OD) per 100 �g of total nuclear proteins.
.4.4. Western blot analysisHeart samples (n = 5 per group) from Nx WT, Nx Epo-Tgh, AHx
T, AHx Epo-TAgh, CHx WT and CHx Epo-TAgh mice were homog-nized in an ice-cold lysis buffer (62.5 mM Tris–HCl, pH 6.8, 2% SDSnd 10% glycerol) supplemented with a protease inhibitor cocktailSigma–Aldrich). 50 �g of protein of each sample were separatedy electrophoresis on 10% SDS-polyacrylamide gel and transferredo PVDF membrane. Membranes were placed in 5% BSA/TBS-0.5%ween 20 for 2 h to block nonspecific binding, and then incubatedrst with primary antibodies (EpoR: Santa Cruz Biotechnology #sc-97; STAT-5a: Santa Cruz Biotechnology #sc-136081, P-STAT-5a:anta Cruz Biotechnology #sc-10185, �-actin: Santa Cruz Biotech-ology #sc-47778) and in a second time with an anti-rabbit IgGntibody-horseradish peroxidase conjugate. All antibodies wereiluted in blocking buffer. Immunodetection was accomplishedsing ECL Western blot analysis kit detection (Santa Cruz Biotech-ology, Santa Cruz, CA). Densitometric analysis, using ImagePro Plus.1 software, were done to quantify the specific protein expressionf each sample compared to internal control (�-actin).
.4.5. ImmunohistochemistryFour mice per group (Nx WT, Nx Epo-TAgh, CHx WT and CHx
po-TAgh) were killed by cervical dislocation, hearts were removed,insed in PBS to remove blood and postfixed in 4% paraformalde-yde, prior an embedding in paraffin. Immunolocalization wereerformed on six-micrometer transversal heart. Antigen retrievalas done in 1× boiled citrate. Sections were incubated with arimary antibody (HIF 1�: Novus biological # NB100-105; VEGF:anta Cruz Biotechnology #sc-507; Epo: Santa Cruz Biotechnol-gy #sc-7956). The negative Controls were performed by omittingrimary antibody. Sections were then labeled using a detectionit (ChemMate; Dako) with biotinylated secondary antibody andiaminobenzidine (DAB) as the substrate. Computerized imagesere captured at a magnification of 40× using Zeiss image analyzer.
.4.6. Capillary densityThree mice per experimental group were used (Nx WT, Nx Epo-
Agh, CHx WT, CHx Epo-TAgh). The analysis of capillary density in
CGGA 60 C 534 NM 007942T 60 ◦C 86 NM 010149T 62 ◦C 138 NM 007393
the heart was performed using Caveolin-1 antibody (Santa CruzBiotechnology #sc-894) on nine transversal sections per mouseincluding sections for negative controls. Pictures were taken at 40×lens, and the number of Caveolin-positive capillaries was deter-mined using a grid. The area of this grid at 40× lens was 0.065 mm2.The Caveolin positive capillaries inside the grid area as well as thenumber of cardiac fibers were counted in three regions per slide.In addition, the capillaries/fibers ratio was also calculated. Theseimmunohistochemical parameters were essentially measured inthe left ventricle because of the small size of the right ventricle.The obtained values from three mice per group were averaged,and results were expressed as the mean number of capillaries permm2 ± SEM.
2.5. Statistical analysis
Two-way analysis of variance was carried out to study the effectof anemia and or hypoxia and Newman–Keuls test was used forpost hoc test. A Student t-test was exceptionally used for Epo assaysince four measurements in Epo-TAgh group were under detec-tion threshold of the ELISA assay, making impossible to performa two-way ANOVA. The statistical analyses were performed usingStatistica software (StartSoft, Tulsa, OK). All values are expressed asmean ± SD unless otherwise specified. Differences were consideredto be significant when P ≤ 0.05.
3. Results
3.1. Animal characteristics
Body weight, hemoglobin and plasma [Epo] are summarized inTable 2. Body weight was similar in all groups with or withouthypoxia. In Nx Epo-TAgh mice, mean plasma [Epo] was 58% lowerthan in Nx WT group. AHx increased Epo by 294% in WT and by 101%in Epo-TAgh mice. After CHx, plasma [Epo] has returned to basalvalues in both groups. [Hemoglobin] was dramatically reduced inNx Epo-TAgh when compared to Nx WT mice and increased in CHxonly in WT mice.
3.2. Epo mRNA and protein expression in cardiac tissue
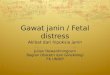
Transcripts encoding Epo were detected in whole heart mRNA ofNx WT mice and the amplified products were sequenced to ensuretheir identity. The time course pattern of Epo gene expression inWT mice showed that cardiac Epo mRNA was over expressed afterAHx, while they returned to Nx values after CHx (Fig. 1A). CardiacEpo protein concentration in WT mice showed similar time coursepatterns (Fig. 1B). Immunohistochemical studies confirmed a dif-fuse pattern of distribution in the myocardium of WT mice in Nxand showed an increased staining after AHx (Fig. 1D pictures 1–4).Rare cardiomyocytes showed positive staining to Epo protein in
their cytoplasm in Nx WT, while they were more frequent afterAHx (Fig. 1D picture 2). In Epo-TAgh mice, no signal was detectedby real time RT-PCR. Cardiac Epo protein concentration was 2–7-fold lower than in their respective WT counterparts (Fig. 3A) and
R. El Hasnaoui-Saadani et al. / Respiratory Physiology & Neurobiology 186 (2013) 146– 154 149
Table 2Body weight, plasma hemoglobin and Epo concentration in wild-type (WT) and Epo-Tagh mice in normoxia (Nx), acute hypoxia for 48 h (AHx) and chronic hypoxia for 14days (CHx).
WT Epo-TAgh
Nx AHx CHx Nx AHx CHx
Body weight (g) 28.0 ± 1.9 24.5 ± 1.1 26.7 ± 0.5 25.9 ± 0.4 26.2 ± 1.5 24.8 ± 0.3[Hemoglobin] (g/dL) 17.1 ± 0.3 16.9 ± 0.4 19.2 ± 0.5* 6.7 ± 0.5$ 6.1 ± 0.2$ 7.1 ± 0.5$
[Epo] (pg/mL) 152 ± 8 599 ± 74* 123 ± 19# 88 ± 6$ 177 ± 31*,$ 78 ± 5$
Values are mean ± SEM. n = 6 in each group except for [Epo] in Epo-TAgh in AHx and CHx where n = 4.
di
3
msc(
1eVi
Fdc(
* P < 0.05 from corresponding Nx group.# P < 0.01 from corresponding AHx group.$ P < 0.05 from corresponding WT group.
id not increase after Hx. In addition, no signal was detected bymmunohistochemistry.
.3. Effect of hypoxia in the heart of WT mice
No change was observed in LV or in RV weight after CHx in WTice. Acclimatized WT mice did not develop pulmonary hyperten-
ion as shown by end systolic pressure in RV (Table 3). Moreover,ardiac output (CO) and O2T were maintained after CHx in WT miceTable 4).
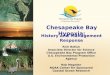
The AHx WT mice demonstrated an increase in cardiac HIF-
� and VEGF protein expressions (Fig. 2B and D). After CHx, thexpression of HIF-1� protein remained elevated (Fig. 2B), whileEGF declined (Fig. 2D). These results were associated with anncreased density of HIF-1� (Fig. 2F, picture 3) and VEGF positive
ig. 1. Epo mRNA (A) and protein (B) in the heart of WT mice in normoxia (Nx), followinemonstrated bands at 534 bps and the time course pattern of Epo mRNA expression. (ircles) and diffuse cytoplasmic distribution (arrows) in the cardiomyocytes of Nx WT micpicture 3) while negative control showed no signal (picture 4). Values are expressed as m
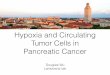
immuno-staining (Fig. 2F, picture 7) after CHx when comparedwith Nx WT animals (Fig. 2F, pictures 1 and 5). Caveolin-positivecapillaries (+67%, Fig. 2E and F, pictures 9 and 11) as well as the cap-illary/fiber ratio were also increased in the heart of CHx WT mice.Furthermore, EpoR protein as well as the P-STAT-5/STAT-5 ratioincreased in response to CHx (Fig. 3C and F).
3.4. Effect of chronic Epo deficiency in the heart of Epo-TAgh mice
Epo deficiency induced a cardiac hypertrophy (Table 3, +37% forLV + S/BW and +63% for RVW/BW). RV systolic function, evaluated
by RV dP/dt max, was unchanged by chronic Epo deficiency and nopulmonary hypertension developed in Epo-TAgh mice, as demon-strated by RV ESP (Table 3). On the contrary, Epo deficiency wasassociated with LV dilatation (16% increase in LV EDD, Table 4).g 48 h (AHx) and 14 days (CHx) of hypoxia. (C) Representative agarose gels of EpoD) Immunohistochemical staining for Epo protein around endothelial cells (blacke (picture 1) and after AHx (picture 2). Positive control has been assayed on kidneyean ± SEM. *vs. Nx; #CHx vs. AHx.

150 R. El Hasnaoui-Saadani et al. / Respiratory Physiology & Neurobiology 186 (2013) 146– 154
Table 3Body weight, heart weight and right ventricular function in WT and Epo-Tagh mice in normoxia (Nx) and after chronic hypoxia (CHx).
Wild Type Epo-Tagh
Nx CHx Nx CHx
Body weight (g) 25.8 ± 1.9 26.0 ± 1.3 28.2 ± 3.6 24.3 ± 0.3LV + S/BW (mg/g) 4.0 ± 1.0 3.7 ± 0.5 5.6 ± 1.1* 4.9 ± 0.6@,&
RVW/BW (mg/g) 0.74 ± 0.03 0.78 ± 0.08 1.21 ± 0.14* 1.11 ± 0.07@,&
RV ESP (mmHg) 23 ± 4 26 ± 3 27 ± 8 28 ± 5RV dP/dtmax (mmHg/s) 1948 ± 654 2348 ± 526 1723 ± 856 1834 ± 274Heart rate (bpm) 485 ± 41 449 ± 60 453 ± 55 421 ± 40
L eightN esult
SSwbfw(
e1apopo(ctw
3
w−rfda
TE
Lcam
V + S: left ventricular weight including septum; RVW: right ventricular free wall wx-Wild Type; &CHxEpo-TAgh vs. NxEpo-TAgh; @CHxEpo-TAgh vs. CHx-Wild Type.R
ystolic LV function was normal or even increased (Sa andpw) as well as diastolic function (Ea and Epw), although EFas unchanged. Cardiac output was increased in Epo-TAgh mice
ecause of increased in stroke volume (+87% for CO/BW, +68%or SV/BW). In spite of this adaptation, oxygen delivery (O2T/BW)as reduced in Nx Epo-TAgh mice, as compared with WT controls
−25%).Chronic Epo deficiency was also associated with increased
xpression of HIF-1� and VEGF proteins (Fig. 2B and D) in Nx. HIF-� and VEGF immuno-staining, as indicated by arrows, were rarend essentially localized around vessels in Nx WT hearts (Fig. 2F,ictures 1 and 5), while Nx Epo-TAgh mice showed numerous areasf positive staining (Fig. 2F, pictures 2 and 6). In addition, Caveolin-ositive capillaries (Fig. 2F, pictures 9 and 10, +98%), the numberf cardiac fibers (Fig. 2E, +51%), as well as the capillary/fiber ratioFig. 2E, +32%) were increased in the heart in response to Epo defi-iency. A significant rise above Nx WT group was also observed inhe protein expression of EpoR, while the P-STAT-5/STAT-5 ratioas unchanged in Nx Epo-TAgh mice (Fig. 3C–F).
.5. Effect of chronic hypoxia in Epo deficient mice
In Epo-TAgh mice exposed to CHx the hypertrophic responseas altered in LV and RV as compared to Nx Epo-TAgh mice (Table 3,12% for LV + S/BW and −8% for RVW/BW). However, this response
emained higher than in chronically hypoxic WT counterparts. RVunction was not affected by CHx in Epo-TAgh mice (Table 3). LVilatation was reduced in CHx Epo-TAgh mice (−9% in LV EDD)nd associated with a mild alteration of LV function (−32% in Spw)
able 4chocardiographic characteristics of WT and Epo-Tagh mice in normoxia (Nx) and after c
Wild Type
Nx CHx
Heart rate (bpm) 500 ± 27 52Aorta diameter (mm) 1.42 ± 0.06 1.3LV EDD (mm) 4.04 ± 0.35 3.7LV ESD (mm) 2.12 ± 0.26 2.1EF (%) 85 ± 6 8Vcfc (circ/s) 2.99 ± 0.39 3.0Sa (cm/s) 2.99 ± 0.32 3.1Spw (cm/s) 3.18 ± 0.47 3.6IVRT (ms) 17 ± 3 1Ea (cm/s) 4.74 ± 0.56 4.4Epw (cm/s) 5.11 ± 1.00 4.9E/Ea 23 ± 3 2SV/BW (�L/g) 1.9 ± 1.9 1.CO/BW (mLmin−1g−1) 0.94 ± 14 0.8Systolic BP (mmHg) 96.7 ± 8.5 97.O2T/BW (ml O2min−1g−1) 21.2 ± 3.2 22.
V EDD: left ventricular end diastolic diameter; LV ESD: left ventricular end systolic diaorrected for ejection time; IVRT: isovolumic relaxation time; Sa: systolic velocity of mitnnulus; Epw: diastolic velocity of posterior wall; BP: blood pressure; CO: cardiac outputean ± SD. * vs. NX-Wild Type; &CHxEpo-TAgh vs. NxEpo-TAgh; @CHxEpo-TAgh vs. CHx-W
; ESP: end-systolic pressure. dP/dtmax: maximal derivative of the RV pressure. * vs.s are shown as mean ± SD. n = 6 in each group.
compared to Nx Epo-TAgh mice, without LV global dysfunction (nonsignificant 5% decrease in EF). CO was reduced after CHx in Epo-TAgh mice (−20%) compared to Nx Epo-TAgh, although significantlyhigher than in CHx WT mice. It was associated with a decrease instroke volume and systolic blood pressure (Table 4, −15%). O2T/BWwas further reduced in CHx when compared to Nx Epo-TAgh mice(Table 4, −16%).
HIF-1� protein was increased after AHx and returned to controlvalues after CHx (Fig. 2B) when compared to Nx Epo-TAgh mice.VEGF protein expression was significantly lower in CHx (Fig. 2D).Moreover, HIF-1� and VEGF protein expressions were also lowerin CHx Epo-TAgh mice, as compared with CHx WT, while thecapillary/fiber ratio was not affected by CHx in Epo-TAgh mice.The P-STAT-5/STAT-5 ratio was enhanced only following CHx inEpo-TAgh mice although it remained lower than in CHx WT mice(Fig. 3F).
4. Discussion
In this study, we showed that (1) Epo gene and protein areexpressed in cardiomyocytes of WT mice, (2) angiogenesis andfunctional cardiac adaptation occurred in WT mice exposed tochronic hypoxia, (3) cardiac hypertrophy, increased cardiac out-put and angiogenesis occurred in Epo-TAgh mice, with activationof the HIF1� pathway, (4) finally, these adaptation processes were
altered in Epo-TAgh mice in chronic hypoxia.We confirmed in vivo an increased cardiac Epo expression inresponse to acute hypoxia in WT mice. Although circulating and tis-sue Epo is decreased in Epo-TAgh mice under normoxia, its effects
hronic hypoxia (CHx).
Epo-TAgh
Nx CHx
4 ± 11 548 ± 46 501 ± 384 ± 0.08 1.40 ± 0.13 1.43 ± 0.104 ± 0.37 4.70 ± 0.20* 4.31 ± 0.18&,@
5 ± 0.23 2.51 ± 0.36* 2.51 ± 0.28@
1 ± 6 84 ± 6 80 ± 52 ± 0.44 3.23 ± 0.44 2.78 ± 0.277 ± 0.85 3.40 ± 0.72 3.19 ± 0.530 ± 1.17 4.39 ± 0.69* 2.99 ± 0.51&
6 ± 2 15 ± 2 17 ± 49 ± 1.04 5.73 ± 1.15* 5.31 ± 0.72@
3 ± 0.66 6.11 ± 1.08 5.39 ± 0.813 ± 7 22 ± 2 22 ± 37 ± 4.8 3.2 ± 6.8* 2.8 ± 4.2&,@
7 ± 0.24 1.76 ± 0.43* 1.40 ± 0.26&,@
9 ± 7.7 94.2 ± 5.8 80.2 ± 5.2&,@
0 ± 6.0 16.0 ± 3.9* 13.5 ± 2.5@
meter; EF: ejection fraction; Vcfc: velocity of shortening of circumferential fibersral annulus; Spw: systolic velocity of posterior wall, Ea: diastolic velocity of mitral; SV: stroke volume; O2T: oxygen transport; BW: body weight.Results are shown as
ild Type. n = 6 in each group.

R. El Hasnaoui-Saadani et al. / Respiratory Physiology & Neurobiology 186 (2013) 146– 154 151
Fig. 2. HIF-1 � (A) and VEGF mRNA (C) and their protein level (respectively B, and D) in the heart of wild-type (WT) and Epo-TAgh mice in normoxia (Nx), following48 h (AHx,) and 14 days (CHx) of hypoxia. (E) The caveolin-immunoreactive vessels, the number of cardiomyocytes and the capillary/fiber ratio were also quantified. (F)I d cavc . Nx Ep
cdiV
mmunohistochemical staining for HIF-1� (pictures 1–4), VEGF (pictures 5–8), anaveolin positive capillaries. Values are expressed as mean ± SEM. *vs. Nx WT; & vs
ould be partially rescued by upregulation of EpoR pathways. Theecreased oxygen delivery in Epo-TAgh mice resulted in an increase
n CO as well as angiogenesis through activation of the HIF-1� andEGF pathway. Epo-TAgh mice survive in CHx despite a limitation
eolin (pictures 9–12). Arrows indicate HIF-1� and VEGF-positive cells as well aso-TAgh; #CHx vs. AHx; @ CHx Epo-TAgh vs. CHx WT. P ≤ 0.05.
in LV hypertrophy and function with a decrease in CO associ-ated with a fall in oxygen delivery. Moreover, HIF-1� and EpoRpathways were depressed in CHx Epo-TAgh mice, although theincreased P-STAT-5/STAT-5 ratio suggests the activation of defense

152 R. El Hasnaoui-Saadani et al. / Respiratory Physiology & Neurobiology 186 (2013) 146– 154
Fig. 3. Epo, EpoR, STAT-5, and P-STAT-5 in the heart of WT and Epo-TAgh mice in normoxia (Nx) following 48 h (AHx) and 14 days of hypoxia (CHx). EpoR mRNA (A) andp /STATi n ± SE@
mcmctcacHs
rotein level (B); STAT-5 (D) and P-STAT-5 (E) protein expressions; the ratio P-STAT5mmunoreactive bands at 60 and 90 kDa, respectively. Values are expressed as meaCHx Epo-TAgh vs. CHx WT. P ≤ 0.05.
echanisms against both constraints. Using our hypoxia/Epo defi-iency model, we could manipulate separately arterial PO2 (noteasured but assumed to be low in hypoxia) and arterial O2
ontent. However, it is important to note that our model ofransgenic mice combine the effects of chronic anemia (low O2ontent) and the effects of chronic EPO deficiency. To differenti-
te the respective effect of each constraint is rather difficult sincehronic anemia itself is a consequence of chronic Epo deficiency.owever, it could be speculated from the activation of HIF/VEGFystems (see Fig. 2B and D) that it is the reduction in tissue O2
5 (F). Representative Western blot of EpoR, STAT-5 and P-STAT-5 (G) demonstratedM. *vs. Nx WT; and vs. Nx Epo-TAgh; #CHx vs. AHx; � AHx Epo-TAgh vs. AHx WT;
delivery (and therefore chronic anemia) that triggers the observedadaptations.
4.1. Expression of Epo in the cardiomyocytes
Some reports have suggested cardiac expression of Epo pro-
tein in mice (Cai et al., 2003) as well as in rats (Bin-Jaliah et al.,2010). A more recent study showed a cardiac Epo gene expressioninduced by inactivation of Vhl gene in adult mice (Miro-Murilloet al., 2011). Moreover, in a recent study, we found Epo transcripts
hysio
ietoihtcedrdhicatts
4
segIaiaaCtata
Tt2CgLCcCciTctcVrppmtSctbtabs
R. El Hasnaoui-Saadani et al. / Respiratory P
n Nx WT mouse hearts (Hoch et al., 2011). We also showed Epoxpression in isolated cardiomyocytes from Nx WT hearts and cul-ured neonatal rat cardiomyocytes (Hoch et al., 2011). In line withur recent study, we confirmed an Epo mRNA expression in Nxn the heart of WT mice that was increased in acute and chronicypoxia. Our immunocytochemical studies confirmed an Epo pro-ein localization around capillaries and in the cytoplasm of someardiomyocytes (Hoch et al., 2011) suggesting that cardiomyocytesxpress Epo. The lack of positive signal in Epo-TAgh mice is in accor-ance with the down-expression of Epo gene in these mice andeinforces our results. Lastly, it should be noted that we did notetect Epo in the Epo-TAgh mice neither by RT-PCR nor by immuno-istochemistry but we found a residual expression of Epo protein
n total heart of Epo-TAgh mice. This result should be taken withaution since it is probably due to the high sensitivity of the ELISAssay and also to the high quantity of total protein loaded duringhe experiment. Since the heart was not perfused, a residual sys-emic Epo could react with the Epo antibody; however total heartamples have been rinsed in PBS before assays.
.2. Cardiac function in hypoxic mice
In the present study, all parameters of cardiac function are pre-erved when comparing WT mice under Nx and CHx conditions. Asxpected, systolic blood pressure, pulmonary pressure, CO and oxy-en delivery were not affected by 14 days of hypoxia in WT mice.n addition, CHx WT mice responded by increasing plasma Epond blood hemoglobin resulting in a rise in oxygen carrying capac-ty. As previously described (Ray et al., 2000) we also evidencedn improved myocardial angiogenesis in the adult heart associ-ted with the activation of HIF-1�/VEGF pathway in response toHx. Increased EpoR and P-STAT-5/STAT-5 ratio suggests an activa-ion of cardioprotective pathways implying HIF-1� and Epo. Thesedaptive responses contribute to the preservation of cardiac func-ion and protect the heart against hypoxic insults to maintain andequate tissue oxygen supply.
As previously described, [Epo] is reduced by 50% in Nx Epo-Agh mice (Macarlupu et al., 2006a,b). It has been already shownhat anemia induces right and LV hypertrophy (Macarlupu et al.,006a; Naito et al., 2009; Olivetti et al., 1989a,b) and increasesO, offsetting the fall in arterial oxygen content to maintain oxy-en delivery. Our echocardiographic data confirm compensatoryV hypertrophy, higher myocardial chamber volumes, and a higherO which could be explained by an increase in preload withouthange in LV afterload as depicted by unchanged blood pressure.ardiac hypertrophy associated with an increase in the number ofardiomyocytes might be a consequence of the chronic increasen CO (Olivetti et al., 1992). Although CO was increased in Epo-Agh mice, oxygen delivery remained lower than in controls. Thisould induce the stabilization of HIF-1� as already described inhe brain in acute (McLaren et al., 2007; Rakusan et al., 2001) andhronic anemia (El Hasnaoui-Saadani et al., 2009), and promoteEGF-induced angiogenesis as shown in Nx Epo-TAgh mice with aise in the capillary/fiber ratio, thus optimizing oxygen diffusion asreviously described in the brain (LaManna et al., 2004). Epo/EpoRathway is known to be involved in the transcription of target genesainly involved in the inhibition of apoptosis and cell prolifera-
ion (Lopez et al., 2011) through the phosphorylation of Jak2 andTAT-5. Because of unchanged P-STAT-5/STAT-5 ratio, we could notonfirm the activation of this cardioprotective pathway in responseo chronic Epo deficiency, in contrast with what occurred in therain of these mice (El Hasnaoui-Saadani et al., 2009). In addition
o its angiogenic function, VEGF may also activate pathways associ-ted with the NO synthesis and thus induce vasodilation, improvinglood supply to cardiac cells (Schoch et al., 2002). Thus, we demon-trated that chronic Epo deficiency induced a cardiac angiogenesislogy & Neurobiology 186 (2013) 146– 154 153
probably mediated by HIF-1�/VEGF and EpoR pathways, whichcould have synergic effects in cardioprotection and oxygen supplyoptimization, in order to limit the consequences of chronic anemiaon cardiac cells.
4.3. Combined effects of Epo deficiency and hypoxia
We investigated for the first time the effects of both chronicEpo deficiency and hypoxia in the heart of Epo-TAgh mice. Whenchronic hypoxia was added to Epo deficiency, cardiac hypertrophywas reduced and CO could not catch up with the oxygen demand.Systolic blood pressure did not increase indicating that systemicafterload was not responsible for the decrease in CO. Moreover, CHxdid not significantly affect RV hemodynamics, and Epo-TAgh micedid not develop pulmonary hypertension. Therefore, the decreasein CO was not the consequence of RV failure. In CHx Epo-TAgh
mice, LV hypertrophy developed but was lower than that of Nxanemic mice, which could account for the decrease in CO and O2delivery. Furthermore, our data showed a mild alteration of dia-stolic and systolic LV function suggesting that altered myocardialfunction in CHx Epo-TAgh mice could participate in the failureof cardiac adaptation to CHx. Although hypoxia or Epo-deficiencyresults in an over expression of HIF-1�, VEGF, Epo and EpoR, wedid not observe a synergic effect of these combined constraintson the heart of CHx Epo-TAgh mice, except for P-STAT-5/STAT-5ratio. However, this ratio was lower in CHx Epo-TAgh than in CHxWT mice, suggesting that activation of the cardioprotective path-ways downstream the Epo/EpoR system may represent a limitingstep. The depression of the HIF-1�/VEGF pathway was not asso-ciated with a fall in the capillary density, probably because of thetime scale of the hypoxic constraint in our experimental setting (14days). As we found a decrease in LV hypertrophy and functional LVadaptation, a depressed HIF-1�/VEGF pathway as well as a reducedoxygen delivery, our results suggest that cardiac adaptive mecha-nisms that take place with chronic Epo deficiency and hypoxia mayrequire extensive Epo effects (angiogenesis, cardioprotection) onthe heart. On the other hand, our previous results in Epo-TAgh micedemonstrate that high levels of Epo are not necessary for survivalin chronic moderate hypoxia (Macarlupu et al., 2006a,b). Similarly,the pika (Ochotona curzoniae) a lagomorph with low Hb (10 g/dL)is adapted to high altitude and does not develop RV hypertrophy(Ge et al., 1998). Interestingly, this mammal presents a high venti-latory response to hypoxia (Pichon et al., 2009), similarly to whatwas previously shown in our Epo-TAgh model (Macarlupu et al.,2006a,b), favoring the acclimatization process to chronic hypoxia.
4.4. Perspective and significance
The present study provides a series of interesting results aboutcardiac adaptations to chronic Epo deficiency. Indeed, we showedan altered cardiac hypertrophic response in Epo-TAgh mice afterchronic hypoxia. As cardiac hypertrophy was already developedin normoxic Epo-TAgh mice before submitting animals to chronichypoxia, we hypothesized a probable decrease in ventricular massby cell death. We did not exclude a partial reversal of car-diomyocytes hypertrophy but more investigations are necessary.Moreover, our results allowed us to speculate that Epo could bereleased by the cardiomyocytes and that this source of Epo may beimportant for cardiac adaptation to hypoxia. Finally, further inves-tigations are necessary to assess the benefit of cardiac Epo in heartfailure.
Acknowledgements
This work was supported by “Agence Nationale de la Recherche”No. ANR-08-GENOPAT-029.

1 hysio
E
R
A
B
B
C
C
C
D
E
F
G
H
J
K
K
L
L
L
L
myocardium: implications for myocardial angiogenesis. Molecular and Cellular
54 R. El Hasnaoui-Saadani et al. / Respiratory P
We wish to thank Stéphane Chambris, Sonia Varela, Moniquetienne and Clément Lourdes for their skillful technical assistance.
eferences
nderson, J.D., Honigman, B., 2011. The effect of altitude-induced hypoxia on heartdisease: do acute, intermittent, and chronic exposures provide cardioprotec-tion? High Altitude Medicine and Biology 12, 45–55.
in-Jaliah, I., Ammar, H.I., Mikhailidis, D.P., Dallak, M.A., Al-Hashem, F.H., Haidara,M.A., Yassin, H.Z., Bahnasi, A.A., Rashed, L.A., Isenovic, E.R., 2010. Cardiac adap-tive responses after hypoxia in an experimental model. Angiology 61, 145–156.
inley, K., Askham, Z., Iqball, S., Spearman, H., Martin, L., de Alwis, M., Thrasher,A.J., Ali, R.R., Maxwell, P.H., Kingsman, S., Naylor, S., 2002. Long-term reversal ofchronic anemia using a hypoxia-regulated erythropoietin gene therapy. Blood100, 2406–2413.
ai, Z., Manalo, D.J., Wei, G., Rodriguez, E.R., Fox-Talbot, K., Lu, H., Zweier, J.L.,Semenza, G.L., 2003. Hearts from rodents exposed to intermittent hypoxia orerythropoietin are protected against ischemia-reperfusion injury. Circulation108, 79–85.
ai, Z., Semenza, G.L., 2004. Phosphatidylinositol-3-kinase signaling isrequired for erythropoietin-mediated acute protection against myocardialischemia/reperfusion injury. Circulation 109, 2050–2053.
assavaugh, J., Lounsbury, K.M., 2011. Hypoxia-mediated biological control. Journalof Cellular Biochemistry 112, 735–744.
igicaylioglu, M., Lipton, S.A., 2001. Erythropoietin-mediated neuroprotectioninvolves cross-talk between Jak2 and NF-kappaB signalling cascades. Nature412, 641–647.
l Hasnaoui-Saadani, R., Pichon, A., Marchant, D., Olivier, P., Launay, T., Quidu, P.,Beaudry, M., Duvallet, A., Richalet, J.P., Favret, F., 2009. Cerebral adaptations tochronic anemia in a model of erythropoietin-deficient mice exposed to hypoxia.American Journal of Physiology. Regulatory, Integrative and Comparative Phys-iology 296, R801–R811.
orsythe, J.A., Jiang, B.H., Iyer, N.V., Agani, F., Leung, S.W., Koos, R.D., Semenza, G.L.,1996. Activation of vascular endothelial growth factor gene transcription byhypoxia-inducible factor 1. Molecular and Cellular Biology 16, 4604–4613.
e, R.L., Kubo, K., Kobayashi, T., Sekiguchi, M., Honda, T., 1998. Blunted hypoxicpulmonary vasoconstrictive response in the rodent Ochotona curzoniae (pika)at high altitude. American Journal of Physiology 274, H1792–H1799.
och, M., Fischer, P., Stapel, B., Missol-Kolka, E., Sekkali, B., Scherr, M., Favret, F.,Braun, T., Eder, M., Schuster-Gossler, K., Gossler, A., Hilfiker, A., Balligand, J.L.,Drexler, H., Hilfiker-Kleiner, D., 2011. Erythropoietin preserves the endothe-lial differentiation capacity of cardiac progenitor cells and reduces heart failureduring anticancer therapies. Cell Stem Cell 9, 131–143.
elkmann, W., 1992. Erythropoietin: structure, control of production, and function.Physiological Reviews 72, 449–489.
ertesz, N., Wu, J., Chen, T.H., Sucov, H.M., Wu, H., 2004. The role of erythropoietinin regulating angiogenesis. Developmental Biology 276, 101–110.
oury, M.J., Bondurant, M.C., 1992. The molecular mechanism of erythropoietinaction. European Journal of Biochemistry 210, 649–663.
aManna, J.C., Chavez, J.C., Pichiule, P., 2004. Structural and functional adaptation tohypoxia in the rat brain. Journal of Experimental Biology 207, 3163–3169.
e Menuet, D., Isnard, R., Bichara, M., Viengchareun, S., Muffat-Joly, M., Walker, F.,Zennaro, M.C., Lombes, M., 2001. Alteration of cardiac and renal functions intransgenic mice overexpressing human mineralocorticoid receptor. Journal ofBiological Chemistry 276, 38911–38920.
evy, N.S., Chung, S., Furneaux, H., Levy, A.P., 1998. Hypoxic stabilization of vascularendothelial growth factor mRNA by the RNA-binding protein HuR. Journal of
Biological Chemistry 273, 6417–6423.opez, T.V., Lappin, T.R., Maxwell, P., Shi, Z., Lopez-Marure, R., Aguilar, C., Rocha-Zavaleta, L., 2011. Autocrine/paracrine erythropoietin signalling promotesJAK/STAT-dependent proliferation of human cervical cancer cells. InternationalJournal of Cancer 129, 2566–2576.
logy & Neurobiology 186 (2013) 146– 154
Macarlupu, J.L., Buvry, A., Morel, O.E., Leon-Velarde, F., Richalet, J.P., Favret, F.,2006a. Characterisation of the ventilatory response to hypoxia in a modelof transgenic anemic mice. Respiratory Physiology and Neurobiology 150,19–26.
Macarlupu, J.L., Buvry, A., Morel, O.E., Leon-Velarde, F., Richalet, J.P., Favret, F.,2006b. Time course of ventilatory acclimatisation to hypoxia in a modelof anemic transgenic mice. Respiratory Physiology and Neurobiology 153,14–22.
Marti, H.H., 2004. Erythropoietin and the hypoxic brain. Journal of ExperimentalBiology 207, 3233–3242.
Marzo, F., Lavorgna, A., Coluzzi, G., Santucci, E., Tarantino, F., Rio, T., Conti, E., Autore,C., Agati, L., Andreotti, F., 2008. Erythropoietin in heart and vessels: focus ontranscription and signalling pathways. Journal of Thrombosis and Thrombolysis26, 183–187.
Maxwell, P.H., Osmond, M.K., Pugh, C.W., Heryet, A., Nicholls, L.G., Tan, C.C., Doe,B.G., Ferguson, D.J., Johnson, M.H., Ratcliffe, P.J., 1993. Identification of the renalerythropoietin-producing cells using transgenic mice. Kidney International 44,1149–1162.
McLaren, A.T., Marsden, P.A., Mazer, C.D., Baker, A.J., Stewart, D.J., Tsui, A.K., Li, X.,Yucel, Y., Robb, M., Boyd, S.R., Liu, E., Yu, J., Hare, G.M., 2007. Increased expressionof HIF-1alpha, nNOS, and VEGF in the cerebral cortex of anemic rats. AmericanJournal of Physiology. Regulatory Integrative and Comparative Physiology 292,R403–R414.
Miro-Murillo, M., Elorza, A., Soro-Arnaiz, I., Albacete-Albacete, L., Ordonez, A., Balsa,E., Vara-Vega, A., Vazquez, S., Fuertes, E., Fernandez-Criado, C., Landazuri, M.O.,Aragones, J., 2011. Acute Vhl gene inactivation induces cardiac HIF-dependenterythropoietin gene expression. PLoS ONE 6, e22589.
Mole, D.R., Ratcliffe, P.J., 2008. Cellular oxygen sensing in health and disease. Pedi-atric Nephrology 23, 681–694.
Naito, Y., Tsujino, T., Matsumoto, M., Sakoda, T., Ohyanagi, M., Masuyama, T., 2009.Adaptive response of the heart to long-term anemia induced by iron defi-ciency. American Journal of Physiology. Heart and Circulatory Physiology 296,H585–H593.
Olivetti, G., Lagrasta, C., Quaini, F., Ricci, R., Moccia, G., Capasso, J.M., Anversa, P.,1989a. Capillary growth in anemia-induced ventricular wall remodeling in therat heart. Circulation Research 65, 1182–1192.
Olivetti, G., Lagrasta, C., Ricci, R., Sonnenblick, E.H., Capasso, J.M., Anversa, P., 1989b.Long-term pressure-induced cardiac hypertrophy: capillary and mast cell pro-liferation. American Journal of Physiology 257, H1766–H1772.
Olivetti, G., Quaini, F., Lagrasta, C., Ricci, R., Tiberti, G., Capasso, J.M., Anversa, P., 1992.Myocyte cellular hypertrophy and hyperplasia contribute to ventricular wallremodeling in anemia-induced cardiac hypertrophy in rats. American Journal ofPathology 141, 227–239.
Parlakian, A., Charvet, C., Escoubet, B., Mericskay, M., Molkentin, J.D., Gary-Bobo,G., De Windt, L.J., Ludosky, M.A., Paulin, D., Daegelen, D., Tuil, D., Li, Z., 2005.Temporally controlled onset of dilated cardiomyopathy through disruption ofthe SRF gene in adult heart. Circulation 112, 2930–2939.
Pichon, A., Zhenzhong, B., Favret, F., Jin, G., Shufeng, H., Marchant, D., Richalet, J.P., Ge,R.L., 2009. Long-term ventilatory adaptation and ventilatory response to hypoxiain plateau pika (Ochotona curzoniae): role of nNOS and dopamine. AmericanJournal Physiology. Regulatory Integrative and Comparative Physiology 297,R978–R987.
Rakusan, K., Cicutti, N., Kolar, F., 2001. Effect of anemia on cardiac function, microvas-cular structure, and capillary hematocrit in rat hearts. American Journal ofPhysiology. Heart Circulatory Physiology 280, H1407–H1414.
Ray, P.S., Estrada-Hernandez, T., Sasaki, H., Zhu, L., Maulik, N., 2000. Early effectsof hypoxia/reoxygenation on VEGF, ang-1, ang-2 and their receptors in the rat
Biochemistry 213, 145–153.Schoch, H.J., Fischer, S., Marti, H.H., 2002. Hypoxia-induced vascular endothe-
lial growth factor expression causes vascular leakage in the brain. Brain 125,2549–2557.